Neutrophil/Lymphocyte Ratio as Predictor of Anastomotic Leak after Gastric Cancer Surgery


 ,
,  ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
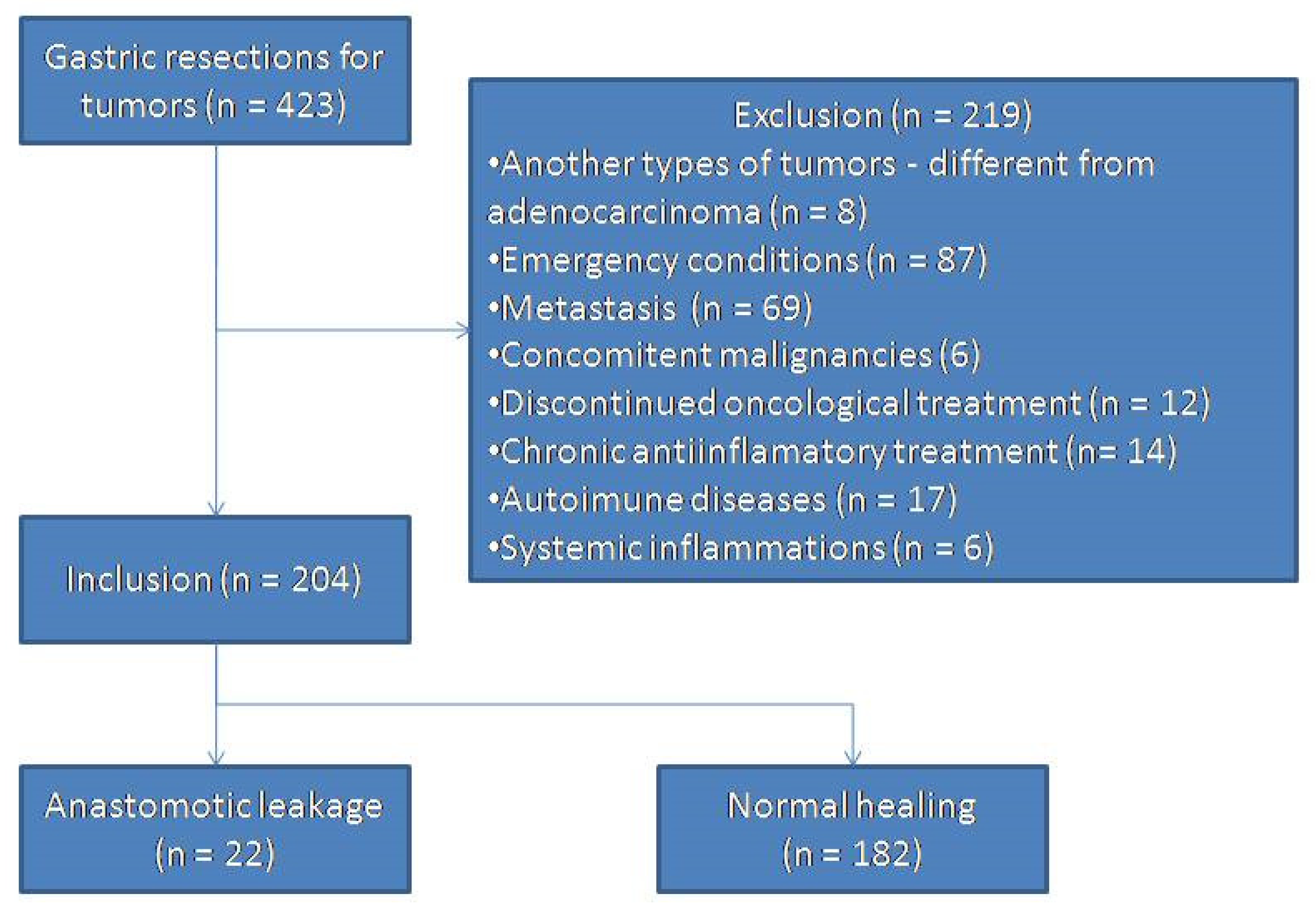
2.1. Inclusion and Exclusion Criteria
2.2. Study Design
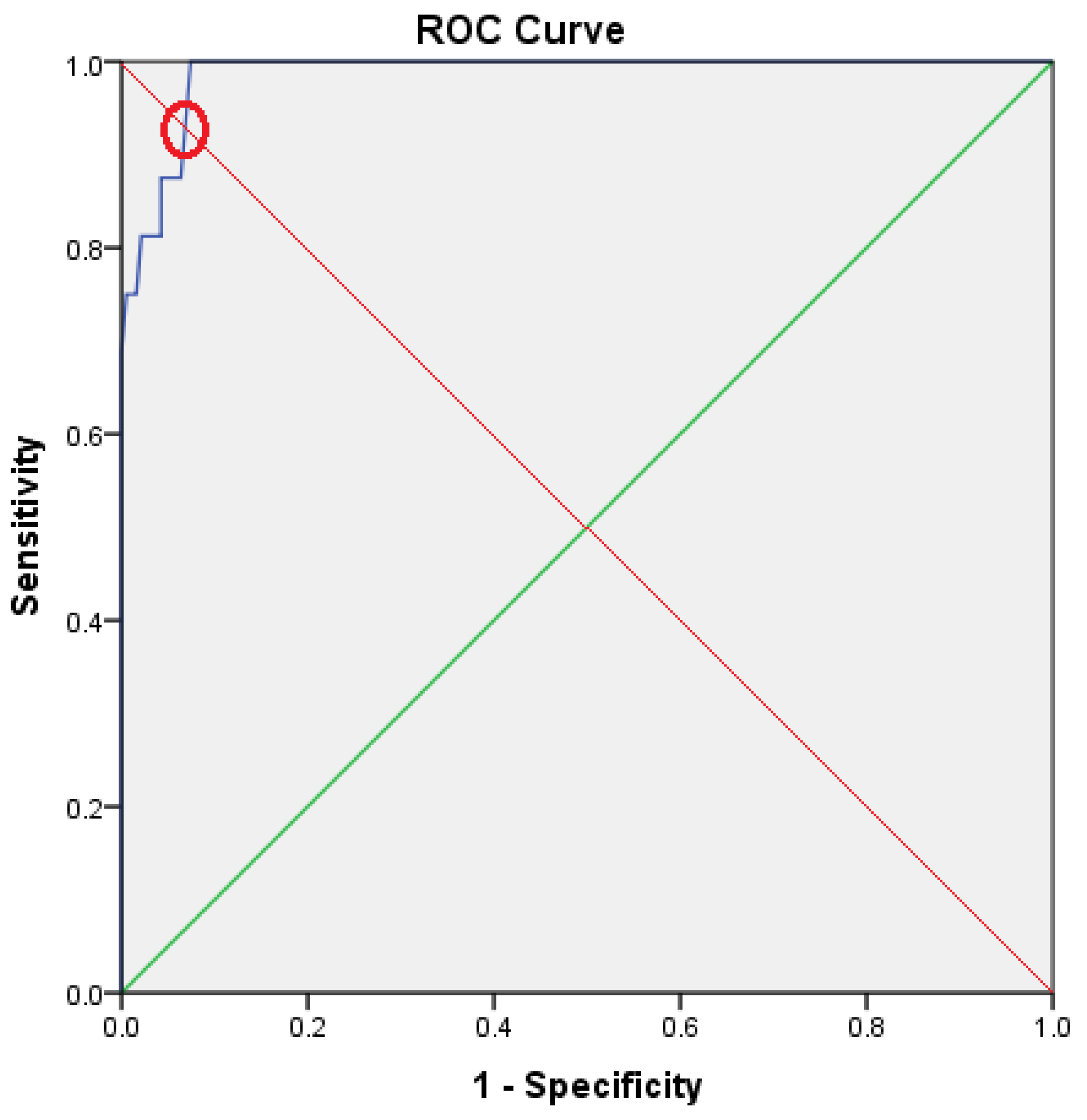
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Deguchi, Y.; Fukagawa, T.; Morita, S.; Ohashi, M.; Saka, M.; Katai, H. Identification of risk factors for esophagojejunal anastomotic leakage after gastric surgery. World J. Surg. 2012, 36, 1617–1622. [Google Scholar] [CrossRef] [PubMed]
- Tsuei, B.J.; Schwartz, R.W. Management of the difficult duodenum. Curr. Surg. 2004, 61, 166–171. [Google Scholar] [CrossRef] [PubMed]
- Rădulescu, D.; Cârţu, D.; Georgescu, E.; Georgescu, I.; Șurlin, V.; Marinescu, D. Anastomotic leakage and fistula after gastric andesophageal cancer surgery—A literature review. J. Surg. 2020, 16, 13–22. [Google Scholar]
- Shrikhande, S.V.; Barreto, S.G.; Shetty, G.; Suradkar, K.; Bodhankar, Y.D.; Shah, S.B.; Goel, M. Post-operative abdominal drainage following major upper gastrointestinal surgery: Single drain versus two drains. J. Cancer Res. Ther. 2013, 9, 267–271. [Google Scholar] [CrossRef]
- Ackland, G.L.; Minto, G.; Clark, M.; Whittle, J.; Stephens, R.C.M.; Owen, T.; Prabhu, P.; del Arroyo, A.G. autonomic regulation of systemic inflammation in humans: A multicenter, blinded observational cohort study. Brain Behav. Immun. 2018, 67, 47–53. [Google Scholar] [CrossRef]
- Vidal, A.C.; Howard, L.E.; de Hoedt, A.; Cooperberg, M.R.; Kane, C.J.; Aronson, W.J.; Terris, M.K.; Amling, C.L.; Taioli, E.; Fowke, J.H.; et al. Neutrophil, lymphocyte and platelet counts, and risk of prostate cancer outcomes in white and black men: Results from the search database. Cancer Causes Control. 2018, 29, 581–588. [Google Scholar] [CrossRef]
- Kumarasamy, C.; Sabarimurugan, S.; Madurantakam, R.; Lakhotiya, K.; Samiappan, S.; Baxi, S.; Nachimuthu, R.; Gothandam, K.M.; Jayaraj, R. Prognostic significance of blood inflammatory biomarkers NLR, PLR, and LMR in cancer—A protocol for systematic review and meta-analysis. Medicine 2019, 98, E14834. [Google Scholar] [CrossRef]
- Iadecola, C.; Cho, S.; Feuerstein, G.Z.; Hallenbeck, J. Chapter 45: Cerebral ischemia and inflammation. In Stroke, 4th ed.; Churchill Livingstone: New York, NY, USA, 2004; pp. 883–893. [Google Scholar]
- Frangogiannis, N.G.; Smith, C.W.; Entman, M.L. The inflammatory response in myocardial infarction. Cardiovasc. Res. 2002, 53, 31–47. [Google Scholar] [CrossRef]
- Schwartz, M.; Moalem, G. Beneficial immune activity after CNS injury: Prospects for vaccination. J. Neuroimmunol. 2001, 113, 185–192. [Google Scholar] [CrossRef]
- Dirican, N.; Karakaya, Y.A.; Gunes, S.; Daloglu, F.T.; Dirican, A. Association of intratumoral tumor infiltrating lymphocytes and neutrophil-to-lymphocyte ratio are an independent prognostic factor in non-small cell lung cancer. Clin. Respir.J. 2017, 11, 789–796. [Google Scholar] [CrossRef]
- Hasegawa, S.; Eguchi, H.; Tomokuni, A.; Tomimaru, Y.; Asaoka, T.; Wada, H.; Hama, N.; Kawamoto, K.; Kobayashi, S.; Konnno, M.; et al. Pre-treatment neutrophil to lymphocyte ratio as a predictive marker for pathological response to preoperative chemoradiotherapy in pancreatic cancer. Oncol. Lett. 2016, 11, 1560–1566. [Google Scholar] [CrossRef] [PubMed]
- Nagasaki, T.; Akiyoshi, T.; Fujimoto, Y.; Konishi, T.; Nagayama, S.; Fukunaga, Y.; Ueno, M. Prognostic impact of neutrophil-tolymphocyte ratio in patients with advanced low rectal cancer treated with preoperative chemoradiotherapy. Dig. Surg. 2015, 32, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Imtiaz, F.; Shafique, K.; Mirza, S.S.; Ayoob, Z.; Vart, P.; Rao, S. Neutrophil lymphocyte ratio as a measure of systemic inflammation in prevalent chronic diseases in Asian population. Int. Arch. Med. 2012, 5. [Google Scholar] [CrossRef]
- Bhat, T.; Teli, S.; Rijal, J.; Bhat, H.; Raza, M.; Khoueiry, G.; Meghani, M.; Akhtar, M.; Costantino, T. Neutrophil to lymphocyte ratio and cardiovascular diseases: A review. Expert Rev. Cardiovasc. Ther. 2013, 11, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Balkwill, F.; Mantovani, A. Inflammation and cancer: Back to Virchow? Lancet 2001, 357, 539–545. [Google Scholar] [CrossRef]
- Roxburgh, C.S.D.; Mcmillan, D.C. Role of systemic inflammatory response in predicting survival in patients with primary operable cancer. Future Oncol. 2010, 6, 149–163. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Allavena, P.; Sica, A.; Balkwill, F. Cancer-related inflammation. Nature 2008, 454, 436–444. [Google Scholar] [CrossRef]
- Zahorec, R. Ratio of neutrophil to lymphocyte counts—Rapid and simple parameter of systemic inflammation and stress in critically ill. Bratisl. Lek. Listy. 2001, 102, 5–14. [Google Scholar]
- Li, M.X.; Liu, X.M.; Zhang, X.F.; Zhang, J.F.; Wang, W.L.; Zhu, Y.; Dong, J.; Cheng, J.-W.; Ma, L.; Lv, T. Prognostic role of neutrophil-to-lymphocyte ratio in colorectal cancer: A systematic review and meta-analysis. Int. J. Cancer 2014, 134, 2403–2413. [Google Scholar] [CrossRef]
- Guthrie, G.J.; Charles, K.A.; Roxburgh, C.S.; Horgan, P.G.; Mcmillan, D.C.; Clarke, S.J. the systemic inflammation-based neutrophil-lymphocyte ratio: Experience in patients with cancer. Crit. Rev. Oncol. Hematol. 2013, 88, 218–230. [Google Scholar] [CrossRef]
- Miyamoto, R.; Inagawa, S.; Sano, N.; Tadano, S.; Adachi, S.; Yamamoto, M. The neutrophil-to-lymphocyte ratio (NLR) predicts short-term and long-term outcomes in gastric cancer patients. Eur. J. Surg. Oncol. 2018, 44, 607–612. [Google Scholar] [CrossRef] [PubMed]
- Malietzis, G.; Giacometti, M.; Askari, A.; Nachiappan, S.; Kennedy, R.H.; Faiz, O.D.; Aziz, O.; Jenkins, J.T. A preoperative neutrophil to lymphocyte ratio of 3 predicts disease-free survival after curative elective colorectal cancer surgery. Ann. Sur. 2014, 260, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Oh, S.Y.; Kim, S.H.; Lee, J.H.; Kim, M.C.; Kim, K.H.; Kim, H.J. Prognostic significance of neutrophil lymphocyte ratio and platelet lymphocyte ratio in advanced gastric cancer patients treated with Folfox chemotherapy. BMC Cancer 2013, 13, 350. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.G.; Li, P.; Tang, D.; Chen, J.; Wang, D.R. Impact of postoperative complications on long-term survival after radical resection for gastric cancer. World J. Gastroenterol. 2013, 19, 4060e5. [Google Scholar] [CrossRef]
- Kubota, T.; Hiki, N.; Nunobe, S.; Kumagai, K.; Aikou, S.; Watanabe, R.; Sano, T.; Yamaguchi, T. Significance of the inflammation-based glasgow prognostic score for short- and long-term outcomes after curative resection of gastric cancer. J. Gastrointest. Surg. 2012, 16, 2037–2044. [Google Scholar] [CrossRef]
- Moyer, R.A.; Wendt, M.K.; Johanesen, P.A.; Turner, J.R.; Dwinell, M.B. Rho activation regulates CXCL 12 chemokine stimulated actin rearrangement and restitution in model intestinal epithelia. Lab. Investig. 2007, 87, 807–817. [Google Scholar] [CrossRef]
- Broughton, G.; Janis, J.E.; Attinger, C.E. The basic science of wound healing. Plast. Reconstr. Surg. 2006, 117 (Suppl. 7), 12–34. [Google Scholar] [CrossRef]
- Velnar, T.; Bailey, T.; Smrkolj, V. The wound healing process: An overview of the cellular and molecular mechanisms. J. Int. Med. Res. 2009, 37, 1528–1542. [Google Scholar] [CrossRef]
- Tymen, S.D.; Rojas, I.G.; Zhou, X.; Fang, Z.J.; Zhao, Y.; Marucha, P.T. restraint stress alters neutrophil and macrophage phenotypes during wound healing. Brain Behav. Immun. 2013, 28, 207–217. [Google Scholar] [CrossRef] [Green Version]
- Singh, S.; Young, A.; McNaught, C.E. The physiology of wound healing. Surgery 2017, 35, 473–477. [Google Scholar] [CrossRef]
- Wang, W.T.; Lee, S.S.; Wang, Y.C.; Lai, Y.W.; Kuo, Y.R.; Tang Chen, Y.B.; Liu, Y.S.; Wu, Y.C. Impaired cutaneous T-cell attracting chemokine elevation and adipose-derived stromal cell migration in a high-glucose environment cause poor diabetic wound healing. Kaohsiung J. Med. Sci. 2018, 34, 539–546. [Google Scholar] [CrossRef]
- Nathan, C. Points of control in inflammation. Nature 2002, 420, 846–852. [Google Scholar] [CrossRef]
- Noy, R.; Pollard, J.W. Tumor-associated macrophages: From mechanisms to therapy. Immunity 2014, 41, 49–61. [Google Scholar] [CrossRef] [Green Version]
- Van Verschuer, V.M.; Hooning, M.J.; van Baare-Georgieva, R.D.; Hollestelle, A.; Timmermans, A.M.; Koppert, L.B.; Verhoog, L.C.; Martens, J.W.M.; Seynaeve, C.; van Deurzen, C.H.M. Tumor-associated inflammation as a potential prognostic tool in Brca1/2-associated breast cancer. Hum. Pathol. 2015, 46, 182–190. [Google Scholar] [CrossRef]
- Koh, C.H.; Bhoo-Pathy, N.; Ng, K.L.; Jabir, R.S.; Tan, G.H.; See, M.H.; Jamaris, S.; Taib, N.A. Utility of pre-treatment neutrophil-lymphocyte ratio and platelet-lymphocyte ratio as prognostic factors in breast cancer. Br. J. Cancer 2015, 113, 150–158. [Google Scholar] [CrossRef]
- Krenn-Pilko, S.; Langsenlehner, U.; Stojakovic, T.; Pichler, M.; Gerger, A.; Kapp, K.S.; Langsenlehner, T. The elevated preoperative derived neutrophil-to-lymphocyte ratio predicts poor clinical outcome in breast cancer patients. Tumor Biol. 2016, 37, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Hu, K.; Lou, L.; Ye, J.; Zhang, S. Prognostic role of the neutrophil-lymphocyte ratio in renal cell carcinoma: A metaanalysis. BMJ Open 2015, 5, E006404. [Google Scholar] [CrossRef]
- De Martino, M.; Pantuck, A.J.; Hofbauer, S.; Waldert, M.; Shariat, S.F.; Belldegrun, A.S.; Klatte, T. Prognostic impact of preoperative neutrophil-to-lymphocyte ratio in localized nonclear cell renal cell carcinoma. J. Urol. 2013, 190, 1999–2004. [Google Scholar] [CrossRef] [PubMed]
- He, J.R.; Shen, G.P.; Ren, Z.F.; Qin, H.; Cui, C.; Zhang, Y.; Zheng, Y.-X.; Jia, W.-H. Pretreatment levels of peripheral neutrophils and lymphocytes as independent prognostic factors in patients with nasopharyngeal carcinoma. Head Neck 2012, 34, 1769–1776. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.; Ye, X.; He, C.; Zhang, B.; Zhang, Y. Pretreatment neutrophil-to-lymphocyte ratio as predictor of survival for patients with metastatic nasopharyngeal carcinoma. Head Neck 2015, 37, 69–75. [Google Scholar] [CrossRef]
- Haddad, C.R.; Guo, L.; Clarke, S.; Guminski, A.; Back, M.; Eade, T. Neutrophil-to-lymphocyte ratio in head and neck cancer. J. Med. Imaging RadiatOncol. 2015, 59, 514–519. [Google Scholar] [CrossRef] [PubMed]
- Walker, P.A.; Kunjuraman, B.; Bartolo, D.C.C. Neutrophil-to-lymphocyte ratio predicts anastomotic dehiscence. ANZ J. Surg. 2018. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.J.; Gao, C.Q.; Wang, G.C.; Wang, Y.C.; Lu, X.Z.; Han, G.S. The clinical values of neutrophil-to-lymphocyte ratio as an early predictor of anastomotic leak in postoperative rectal cancer patients. Zhonghua Zhong Liu Za Zhi 2020, 42, 70–73. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Total, Mean Value ± Standard Deviation (Extreme Values) | High NLR (n = 22) | Low NLR (n = 182) | p-Value | |
|---|---|---|---|---|
| Age | 67.75 ± 9.73 (32, 91) | 63.50±13.82 | 68.27 ± 9.03 | 0.128 |
| Gender % | 0.579 | |||
| Male | 128 | 15 | 113 | |
| Female | 76 | 7 | 69 | |
| Fistula | <0.001 * | |||
| Yes | 22 | 14 | 4 | |
| No | 182 | 8 | 174 | |
| Stage | 0.060 | |||
| I | 24 | 1 | 23 | |
| II | 65 | 4 | 61 | |
| III | 94 | 8 | 86 | |
| IV | 21 | 6 | 16 | |
| Platelets × 103/μL | 268.82 ± 110.17 (51, 611) | 236.18 ± 93.88 | 272.76 ± 111.55 | 0.142 |
| Leukocites × 103/μL | 8.05 ± 2.66 (4.01, 22.13) | 9.46 ± 4.35 | 7.88 ± 2.33 | 0.108 |
| Hemoglobin g/dL | 11.87 ± 2.45 (4.7, 16.63) | 11.21 ± 2.26 | 11.95 ± 2.47 | 0.185 |
| Serum total proteins g/dL | 6.44 ± 0.66 (4.02, 8.10) | 6.52 ± 0.58 | 6.44 ± 0.67 | 0.566 |
| Death | 6 | 5 | 1 | 0.025 * |
| Stage | N | Mean | Std. Deviation | 95% Confidence Interval for Mean | Minimum | Maximum | |
|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||||
| I | 24 | 2.52 | 0.94 | 2.1303 | 2.9291 | 1.97 | 6.72 |
| II | 65 | 2.67 | 0.90 | 2.4464 | 2.8961 | 2.00 | 6.39 |
| III | 94 | 2.61 | 1.01 | 2.4101 | 2.8276 | 1.49 | 9.75 |
| IV | 21 | 3.45 | 2.13 | 2.4784 | 4.4244 | 1.61 | 7.80 |
| Total | 204 | 2.71 | 1.16 | 2.5502 | 2.8713 | 1.49 | 9.75 |
| Anastomotic Dehiscence (n = 16) | Normal Anastomotic Healing (n= 188) | p-Value | |
|---|---|---|---|
| Age | 64.56 ± 14.90 | 68.03±9.17 | 0.702 |
| Gender % | 0.272 | ||
| Male | 12 | 128 | |
| Female | 4 | 60 | |
| NLR | 5.83 ± 1.68 | 2.44 ± 0.51 | <0.001 * |
| Stage | |||
| I | 1 | 23 | 0.006 * |
| II | 4 | 60 | |
| III | 6 | 88 | |
| IV | 5 | 17 | |
| Platelets × 103/μL | 255.14 ± 105.22 | 287.98 ± 115.95 | 0.148 |
| Leukocites × 103/μL | 9.06 ± 4.19 | 7.96 ± 2.48 | 0.316 |
| Hemoglobin g/dL | 11.76 ± 2.40 | 11.88 ± 2.46 | 0.854 |
| Total serum proteins g/dL | 6.64 ± 0.67 | 6.43 ± 0.66 | 0.225 |
| Death | 4 | 2 | 0.049 * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Radulescu, D.; Baleanu, V.D.; Padureanu, V.; Radulescu, P.M.; Bordu, S.; Patrascu, S.; Socea, B.; Bacalbasa, N.; Surlin, M.V.; Georgescu, I.; et al. Neutrophil/Lymphocyte Ratio as Predictor of Anastomotic Leak after Gastric Cancer Surgery. Diagnostics 2020, 10, 799. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10100799
Radulescu D, Baleanu VD, Padureanu V, Radulescu PM, Bordu S, Patrascu S, Socea B, Bacalbasa N, Surlin MV, Georgescu I, et al. Neutrophil/Lymphocyte Ratio as Predictor of Anastomotic Leak after Gastric Cancer Surgery. Diagnostics. 2020; 10(10):799. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10100799
Chicago/Turabian StyleRadulescu, Dumitru, Vlad Dumitru Baleanu, Vlad Padureanu, Patricia Mihaela Radulescu, Silviu Bordu, Stefan Patrascu, Bogdan Socea, Nicolae Bacalbasa, Marin Valeriu Surlin, Ion Georgescu, and et al. 2020. "Neutrophil/Lymphocyte Ratio as Predictor of Anastomotic Leak after Gastric Cancer Surgery" Diagnostics 10, no. 10: 799. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10100799