Nuclear Expression Loss of SSBP2 Is Associated with Poor Prognostic Factors in Colorectal Adenocarcinoma

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
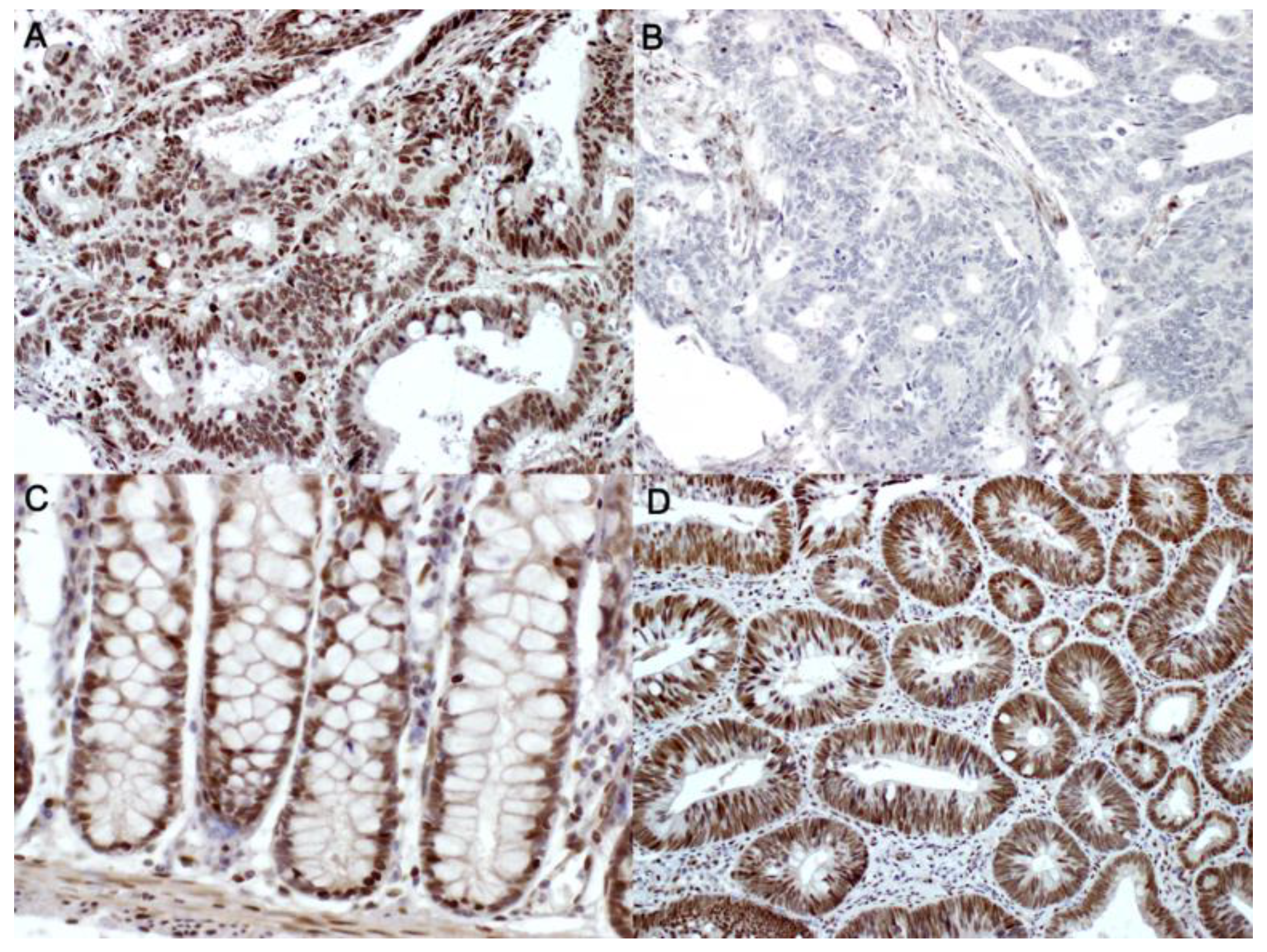
2.2. Immunohistochemical Stainings and Interpretation
2.3. Statistical Analyses
3. Results
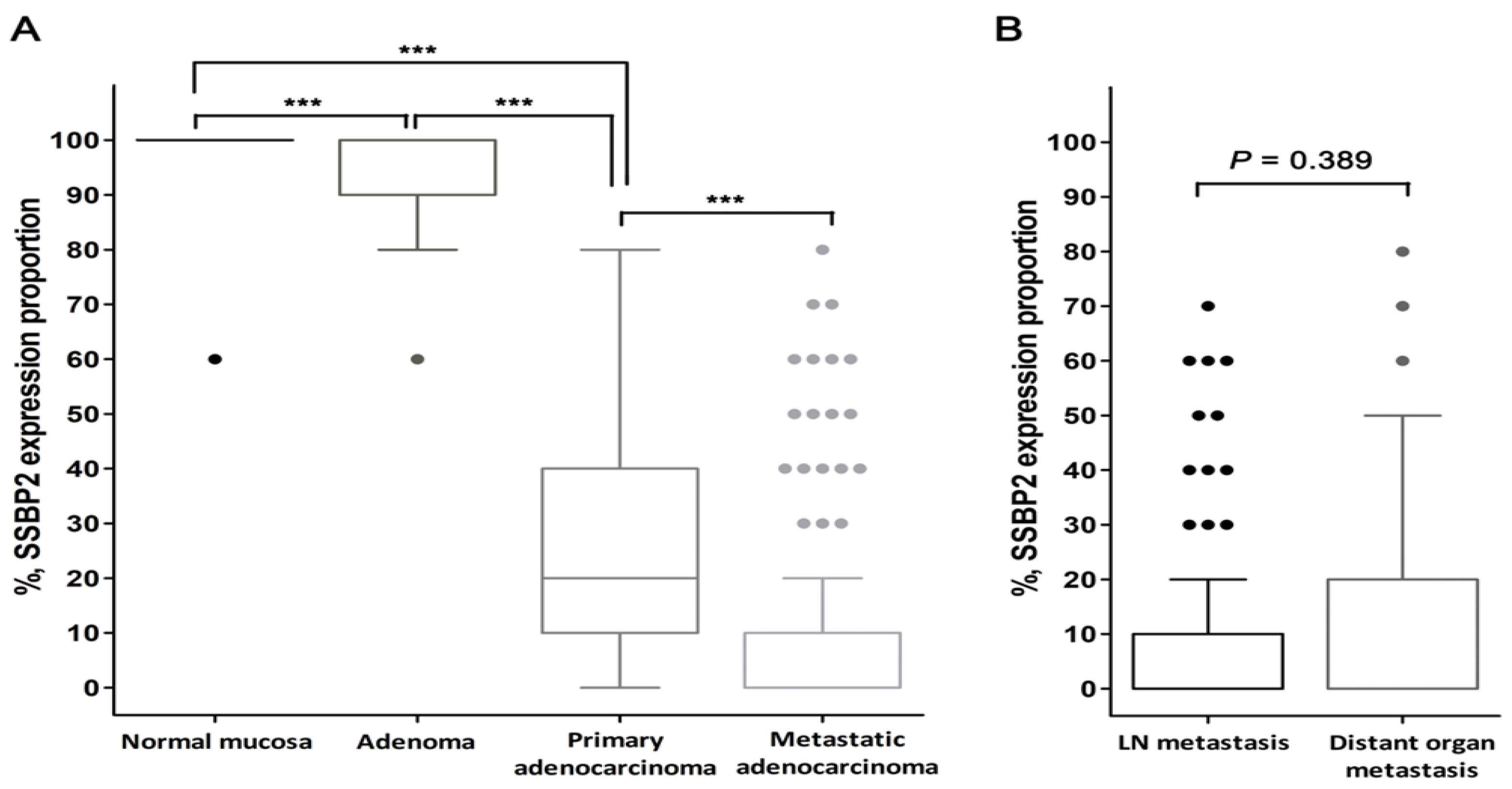
3.1. Patient Characteristics and SSBP2 Expression
3.2. Correlation between SSBP2 Expression and Clinicopathological Features
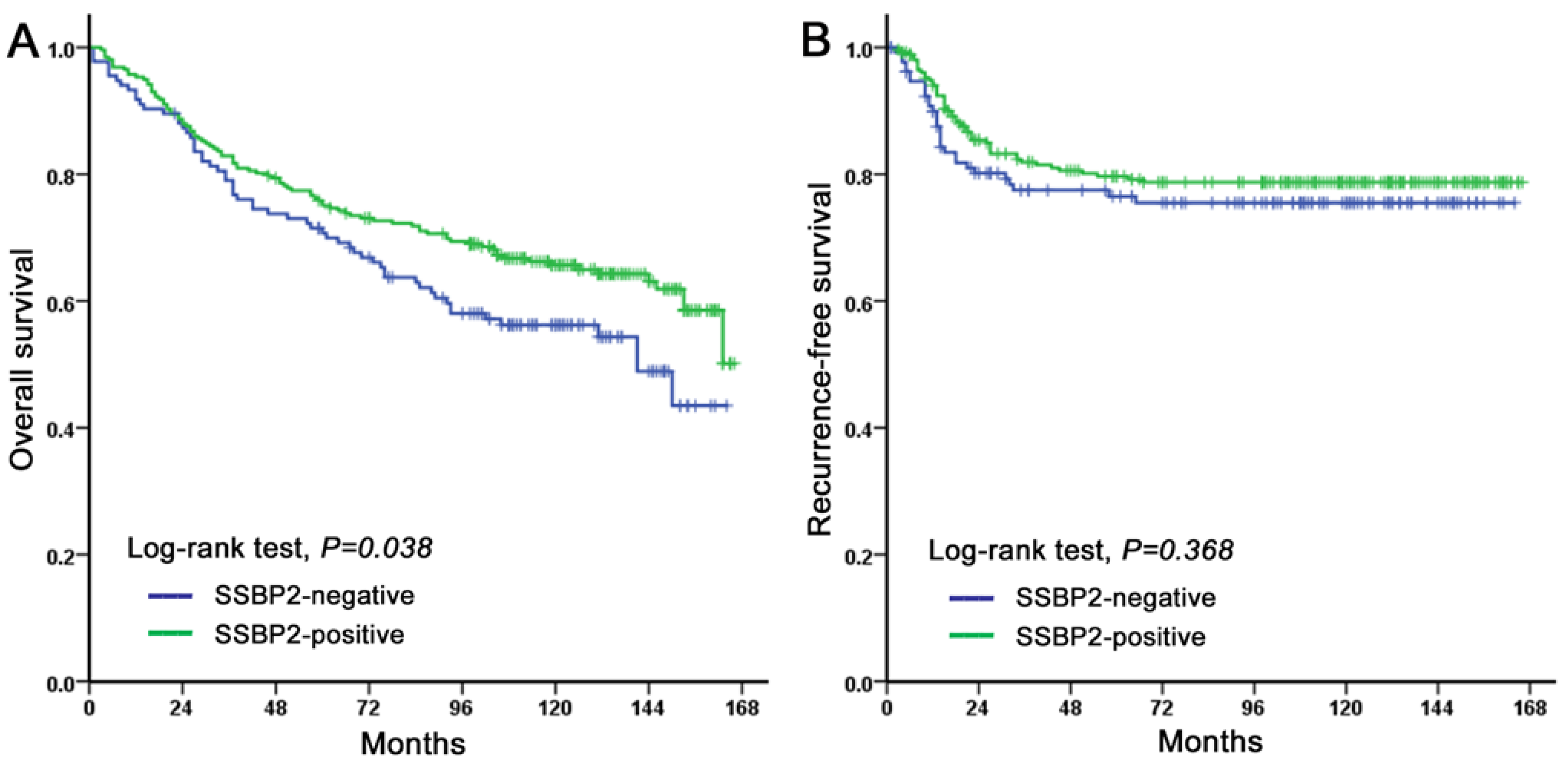
3.3. Prognostic Significance of SSBP2 Expression
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Availability of Data and Materials
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Muller, M.F.; Ibrahim, A.E.; Arends, M.J. Molecular pathological classification of colorectal cancer. Virchows Arch. Int. J. Pathol. 2016, 469, 125–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poulogiannis, G.; Ichimura, K.; Hamoudi, R.A.; Luo, F.; Leung, S.Y.; Yuen, S.T.; Harrison, D.J.; Wyllie, A.H.; Arends, M.J. Prognostic relevance of DNA copy number changes in colorectal cancer. J. Pathol. 2010, 220, 338–347. [Google Scholar] [CrossRef] [PubMed]
- Arends, M.J. Pathways of colorectal carcinogenesis. Appl. Immunohistochem Mol. Morphol. 2013, 21, 97–102. [Google Scholar]
- Markowitz, S.D.; Bertagnolli, M.M. Molecular origins of cancer: Molecular basis of colorectal cancer. N. Engl. J. Med. 2009, 361, 2449–2460. [Google Scholar] [CrossRef] [Green Version]
- Jones, P.A.; Baylin, S.B. The fundamental role of epigenetic events in cancer. Nat. Rev. Genet. 2002, 3, 415–428. [Google Scholar] [CrossRef]
- Hoque, M.O.; Kim, M.S.; Ostrow, K.L.; Liu, J.; Wisman, G.B.; Park, H.L.; Poeta, M.L.; Jeronimo, C.; Henrique, R.; Lendvai, A.; et al. Genome-wide promoter analysis uncovers portions of the cancer methylome. Cancer Res. 2008, 68, 2661–2670. [Google Scholar] [CrossRef] [Green Version]
- Powell, S.M.; Zilz, N.; Beazer-Barclay, Y.; Bryan, T.M.; Hamilton, S.R.; Thibodeau, S.N.; Vogelstein, B.; Kinzler, K.W. APC mutations occur early during colorectal tumorigenesis. Nature 1992, 359, 235–237. [Google Scholar] [CrossRef]
- Esteller, M.; Sparks, A.; Toyota, M.; Sanchez-Cespedes, M.; Capella, G.; Peinado, M.A.; Gonzalez, S.; Tarafa, G.; Sidransky, D.; Meltzer, S.J.; et al. Analysis of adenomatous polyposis coli promoter hypermethylation in human cancer. Cancer Res. 2000, 60, 4366–4371. [Google Scholar]
- Evrard, C.; Tachon, G.; Randrian, V.; Karayan-Tapon, L.; Tougeron, D. Microsatellite Instability: Diagnosis, Heterogeneity, Discordance, and Clinical Impact in Colorectal Cancer. Cancers (Basel) 2019, 11, 1567. [Google Scholar] [CrossRef] [Green Version]
- Sinicrope, F.A.; Sargent, D.J. Molecular pathways: Microsatellite instability in colorectal cancer: Prognostic, predictive, and therapeutic implications. Clin. Cancer Res. 2012, 18, 1506–1512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tougeron, D.; Mouillet, G.; Trouilloud, I.; Lecomte, T.; Coriat, R.; Aparicio, T.; Des Guetz, G.; Lecaille, C.; Artru, P.; Sickersen, G.; et al. Efficacy of Adjuvant Chemotherapy in Colon Cancer With Microsatellite Instability: A Large Multicenter AGEO Study. J. Natl. Cancer Inst. 2016, 108. [Google Scholar] [CrossRef] [PubMed]
- Sargent, D.J.; Marsoni, S.; Monges, G.; Thibodeau, S.N.; Labianca, R.; Hamilton, S.R.; French, A.J.; Kabat, B.; Foster, N.R.; Torri, V.; et al. Defective mismatch repair as a predictive marker for lack of efficacy of fluorouracil-based adjuvant therapy in colon cancer. J. Clin. Oncol. 2010, 28, 3219–3226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jover, R.; Zapater, P.; Castells, A.; Llor, X.; Andreu, M.; Cubiella, J.; Pinol, V.; Xicola, R.M.; Bujanda, L.; Rene, J.M.; et al. Mismatch repair status in the prediction of benefit from adjuvant fluorouracil chemotherapy in colorectal cancer. Gut 2006, 55, 848–855. [Google Scholar] [CrossRef] [Green Version]
- Barbalan, A.; Nicolaescu, A.C.; Magaran, A.V.; Mercut, R.; Balasoiu, M.; Bancescu, G.; Serbanescu, M.S.; Lazar, O.F.; Saftoiu, A. Immunohistochemistry predictive markers for primary colorectal cancer tumors: Where are we and where are we going? Rom. J. Morphol. Embryol. 2018, 59, 29–42. [Google Scholar]
- Castro, P.; Liang, H.; Liang, J.C.; Nagarajan, L. A novel, evolutionarily conserved gene family with putative sequence-specific single-stranded DNA-binding activity. Genomics 2002, 80, 78–85. [Google Scholar] [CrossRef]
- Fairman, J.; Wang, R.Y.; Liang, H.; Zhao, L.; Saltman, D.; Liang, J.C.; Nagarajan, L. Translocations and deletions of 5q13.1 in myelodysplasia and acute myelogenous leukemia: Evidence for a novel critical locus. Blood 1996, 88, 2259–2266. [Google Scholar] [CrossRef]
- Huang, Y.; Chang, X.; Lee, J.; Cho, Y.G.; Zhong, X.; Park, I.S.; Liu, J.W.; Califano, J.A.; Ratovitski, E.A.; Sidransky, D.; et al. Cigarette smoke induces promoter methylation of single-stranded DNA-binding protein 2 in human esophageal squamous cell carcinoma. Int. J. Cancer 2011, 128, 2261–2273. [Google Scholar] [CrossRef]
- Liang, H.; Samanta, S.; Nagarajan, L. SSBP2, a candidate tumor suppressor gene, induces growth arrest and differentiation of myeloid leukemia cells. Oncogene 2005, 24, 2625–2634. [Google Scholar] [CrossRef] [Green Version]
- Kagohara, L.T.; Schussel, J.L.; Subbannayya, T.; Sahasrabuddhe, N.; Lebron, C.; Brait, M.; Maldonado, L.; Valle, B.L.; Pirini, F.; Jahuira, M.; et al. Global and gene-specific DNA methylation pattern discriminates cholecystitis from gallbladder cancer patients in Chile. Future Oncol. 2015, 11, 233–249. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.W.; Nagpal, J.K.; Sun, W.; Lee, J.; Kim, M.S.; Ostrow, K.L.; Zhou, S.; Jeronimo, C.; Henrique, R.; Van Criekinge, W.; et al. ssDNA-binding protein 2 is frequently hypermethylated and suppresses cell growth in human prostate cancer. Clin. Cancer Res. 2008, 14, 3754–3760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maldonado, L.; Brait, M.; Loyo, M.; Sullenberger, L.; Wang, K.; Peskoe, S.B.; Rosenbaum, E.; Howard, R.; Toubaji, A.; Albadine, R.; et al. GSTP1 promoter methylation is associated with recurrence in early stage prostate cancer. J. Urol. 2014, 192, 1542–1548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, W.L.; Weng, X.T.; Wang, J.L.; Lin, Y.K.; Liu, T.W.; Zhou, Q.Y.; Hu, Y.; Pan, Y.; Chen, X.L. Association Between c-Myc and Colorectal Cancer Prognosis: A Meta-Analysis. Front. Physiol. 2018, 9, 1549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michailidi, C.; Soudry, E.; Brait, M.; Maldonado, L.; Jaffe, A.; Ili-Gangas, C.; Brebi-Mieville, P.; Perez, J.; Kim, M.S.; Zhong, X.; et al. Genome-wide and gene-specific epigenomic platforms for hepatocellular carcinoma biomarker development trials. Gastroenterol. Res. Pr. 2014, 2014, 597164. [Google Scholar] [CrossRef]
- Brait, M.; Banerjee, M.; Maldonado, L.; Ooki, A.; Loyo, M.; Guida, E.; Izumchenko, E.; Mangold, L.; Humphreys, E.; Rosenbaum, E.; et al. Promoter methylation of MCAM, ERalpha and ERbeta in serum of early stage prostate cancer patients. Oncotarget 2017, 8, 15431–15440. [Google Scholar] [CrossRef] [Green Version]
- Andersen, C.L.; Christensen, L.L.; Thorsen, K.; Schepeler, T.; Sorensen, F.B.; Verspaget, H.W.; Simon, R.; Kruhoffer, M.; Aaltonen, L.A.; Laurberg, S.; et al. Dysregulation of the transcription factors SOX4, CBFB and SMARCC1 correlates with outcome of colorectal cancer. Br. J. Cancer 2009, 100, 511–523. [Google Scholar] [CrossRef] [Green Version]
- Shannon, N.B.; Tan, J.W.; Tan, H.L.; Wang, W.; Chen, Y.; Lim, H.J.; Tan, Q.X.; Hendrikson, J.; Ng, W.H.; Loo, L.Y.; et al. A set of molecular markers predicts chemosensitivity to Mitomycin-C following cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for colorectal peritoneal metastasis. Sci. Rep. 2019, 9, 10572. [Google Scholar] [CrossRef] [Green Version]
- Perilli, L.; Tessarollo, S.; Albertoni, L.; Curtarello, M.; Pasto, A.; Brunetti, E.; Fassan, M.; Rugge, M.; Indraccolo, S.; Amadori, A.; et al. Silencing of miR-182 is associated with modulation of tumorigenesis through apoptosis induction in an experimental model of colorectal cancer. BMC Cancer 2019, 19, 821. [Google Scholar] [CrossRef] [Green Version]
- Amin, M.B.; Edge, S.; Greene, F.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. AJCC Cancer Staging Manual, 8th ed.; Springer: New York, NY, USA, 2017. [Google Scholar]
- Zlobec, I.; Steele, R.; Michel, R.P.; Compton, C.C.; Lugli, A.; Jass, J.R. Scoring of p53, VEGF, Bcl-2 and APAF-1 immunohistochemistry and interobserver reliability in colorectal cancer. Mod. Pathol. 2006, 19, 1236–1242. [Google Scholar] [CrossRef] [Green Version]
- Zlobec, I.; Vuong, T.; Compton, C.C. The predictive value of apoptosis protease-activating factor 1 in rectal tumors treated with preoperative, high-dose-rate brachytherapy. Cancer 2006, 106, 284–286. [Google Scholar] [CrossRef]
- Rosati, G.; Chiacchio, R.; Reggiardo, G.; De Sanctis, D.; Manzione, L. Thymidylate synthase expression, p53, bcl-2, Ki-67 and p27 in colorectal cancer: Relationships with tumor recurrence and survival. Tumour Biol. J. Int. Soc. Oncodevelopmental Biol. Med. 2004, 25, 258–263. [Google Scholar] [CrossRef] [PubMed]
- Galizia, G.; Lieto, E.; Ferraraccio, F.; Orditura, M.; De Vita, F.; Castellano, P.; Imperatore, V.; Romano, C.; Ciardiello, F.; Agostini, B.; et al. Determination of molecular marker expression can predict clinical outcome in colon carcinomas. Clin. Cancer Res. 2004, 10, 3490–3499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okonkwo, A.; Musunuri, S.; Talamonti, M.; Benson, A., 3rd; Small, W., Jr.; Stryker, S.J.; Rao, M.S. Molecular markers and prediction of response to chemoradiation in rectal cancer. Oncol. Rep. 2001, 8, 497–500. [Google Scholar] [CrossRef]
- Giatromanolaki, A.; Stathopoulos, G.P.; Tsiompanou, E.; Papadimitriou, C.; Georgoulias, V.; Gatter, K.C.; Harris, A.L.; Koukourakis, M.I. Combined role of tumor angiogenesis, bcl-2, and p53 expression in the prognosis of patients with colorectal carcinoma. Cancer 1999, 86, 1421–1430. [Google Scholar] [CrossRef]
- Ahmed, H. Promoter Methylation in Prostate Cancer and its Application for the Early Detection of Prostate Cancer Using Serum and Urine Samples. Biomark Cancer 2010, 2010, 17–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brait, M.; Maldonado, L.; Noordhuis, M.G.; Begum, S.; Loyo, M.; Poeta, M.L.; Barbosa, A.; Fazio, V.M.; Angioli, R.; Rabitti, C.; et al. Association of promoter methylation of VGF and PGP9.5 with ovarian cancer progression. PLoS ONE 2013, 8, e70878. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| SSBP2 Nuclear Expression | Normal Mucosa (n = 48) | Adenoma (n = 47) | Primary Adenocarcinoma (n = 391) | Metastatic Carcinoma (n = 131) | p-Value |
|---|---|---|---|---|---|
| Positive | 48 (100.0 %) | 47 (100.0 %) | 257 (65.7 %) | 31 (23.7%) | <0.001 a |
| Negative | 0 (0.0%) | 0 (0.0 %) | 134 (34.3 %) | 100 (76.3%) | |
| Positive cell proportion, % (Mean ± SD) | 99.17 ± 5.77 | 94.47 ± 7.96 | 25.38 ± 20.80 | 9.92 ± 18.46 | <0.001 b |
| Parameters | SSBP2-Negative (n = 134) | SSBP2-Positive (n = 257) | p-Value |
|---|---|---|---|
| Age | 0.507 | ||
| <65 years | 72 (35.8%) | 129 (64.2%) | |
| ≥65 years | 62 (32.6%) | 128 (67.4%) | |
| Sex | 0.924 | ||
| Male | 82 (34.5%) | 156 (65.5%) | |
| Female | 52 (34.0%) | 101 (66.0%) | |
| Tumor location | 0.062 | ||
| Right side | 19 (24.1%) | 60 (75.9%) | |
| Transverse and Left side | 13 (30.2%) | 30 (69.8%) | |
| Rectosigmoid | 102 (37.9%) | 167 (62.1%) | |
| Histologic grade | 0.061 | ||
| G1 (well differentiated) | 7 (24.1%) | 22 (75.9%) | |
| G2 (moderately differentiated) | 55 (30.1%) | 128 (69.9%) | |
| G3 (poorly differentiated) | 72 (40.2%) | 107 (59.8%) | |
| Lymphatic invasion | 0.116 | ||
| Absent | 54 (30.2%) | 125 (69.8%) | |
| Present | 80 (37.7%) | 132 (62.3%) | |
| Vascular invasion | 0.005 | ||
| Absent | 98 (31.0%) | 218 (69.0%) | |
| Present | 36 (48.0%) | 39 (52.0%) | |
| Perineural invasion | 0.123 | ||
| Absent | 62 (30.7%) | 140 (69.3%) | |
| Present | 72 (38.1%) | 117 (61.9%) | |
| Tumor budding | 0.795 | ||
| Absent/Low/intermediate-grade (0∼9 buds/×200) | 79 (33.3%) | 155 (66.2%) | |
| High-grade (≥10 buds/×200) | 55 (35.0%) | 102 (65.0%) | |
| T category | 0.045 | ||
| pT1 and pT2 | 18 (24.3%) | 56 (75.7%) | |
| pT3 and pT4 | 116 (36.6%) | 201 (63.4%) | |
| Nodal status | 0.119 | ||
| Negative | 51 (30.0%) | 119 (70.0%) | |
| Positive | 83 (37.6%) | 138 (62.4%) | |
| Stage * | 0.119 | ||
| I | 13 (22.8%) | 44 (77.2%) | |
| II | 37 (33.3%) | 74 (66.7%) | |
| III | 72 (36.4%) | 126 (63.6%) | |
| IV | 12 (48.0%) | 13 (52.0%) |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| Variables | HR | 95% CI | p-Value | HR | 95% CI | p-Value |
| SSBP2 (positive vs. negative) | 1.406 | 1.017–1.944 | 0.038 | 1.190 | 0.850–1.666 | 0.311 |
| Age (<65 vs. ≥65) | 2.810 | 1.996–3.956 | <0.001 | 3.196 | 2.261–4.518 | <0.001 |
| Sex (Female vs. Male) | 1.508 | 1.076–2.114 | 0.017 | 1.643 | 1.167–2.312 | 0.004 |
| pT category (1,2 vs. 3,4) | 1.036 | 1.013-1.060 | 0.002 | 1.015 | 0.991-1.041 | 0.225 |
| Nodal status (negative vs. positive) | 1.046 | 1.017-1.075 | 0.002 | 0.975 | 0.889-1.070 | 0.597 |
| Stage * (I, II vs. III, IV) | 1.025 | 1.010-1.041 | 0.001 | |||
| Histological grade (1,2 vs. 3) | 1.664 | 1.210-2.289 | 0.002 | 1.384 | 0.975–1.964 | 0.069 |
| Lymphatic invasion (absent vs. present) | 1.769 | 1.273–2.456 | 0.001 | 1.571 | 0.520–4.749 | 0.424 |
| Vascular invasion (absent vs. present) | 2.768 | 1.964–3.901 | <0.001 | 2.220 | 1.520–3.244 | <0.001 |
| Perineural invasion (absent vs. present) | 1.805 | 1.308–2.491 | <0.001 | 1.244 | 0.845–1.831 | 0.268 |
| Tumor budding (Absent/Low/intermediate vs. High) | 1.452 | 1.058-1.993 | 0.021 | 1.102 | 0.777–1.562 | 0.586 |
Publisher's Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chung, Y.; Kim, H.; Bang, S.; Jang, K.; Paik, S.S.; Shin, S.-J. Nuclear Expression Loss of SSBP2 Is Associated with Poor Prognostic Factors in Colorectal Adenocarcinoma. Diagnostics 2020, 10, 1097. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10121097
Chung Y, Kim H, Bang S, Jang K, Paik SS, Shin S-J. Nuclear Expression Loss of SSBP2 Is Associated with Poor Prognostic Factors in Colorectal Adenocarcinoma. Diagnostics. 2020; 10(12):1097. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10121097
Chicago/Turabian StyleChung, Yumin, Hyunsung Kim, Seongsik Bang, Kiseok Jang, Seung Sam Paik, and Su-Jin Shin. 2020. "Nuclear Expression Loss of SSBP2 Is Associated with Poor Prognostic Factors in Colorectal Adenocarcinoma" Diagnostics 10, no. 12: 1097. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10121097