Biomarkers for Inner Ear Disorders: Scoping Review on the Role of Biomarkers in Hearing and Balance Disorders

 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Databases
2.2. Study Eligibility, Inclusion, and Exclusion Criteria
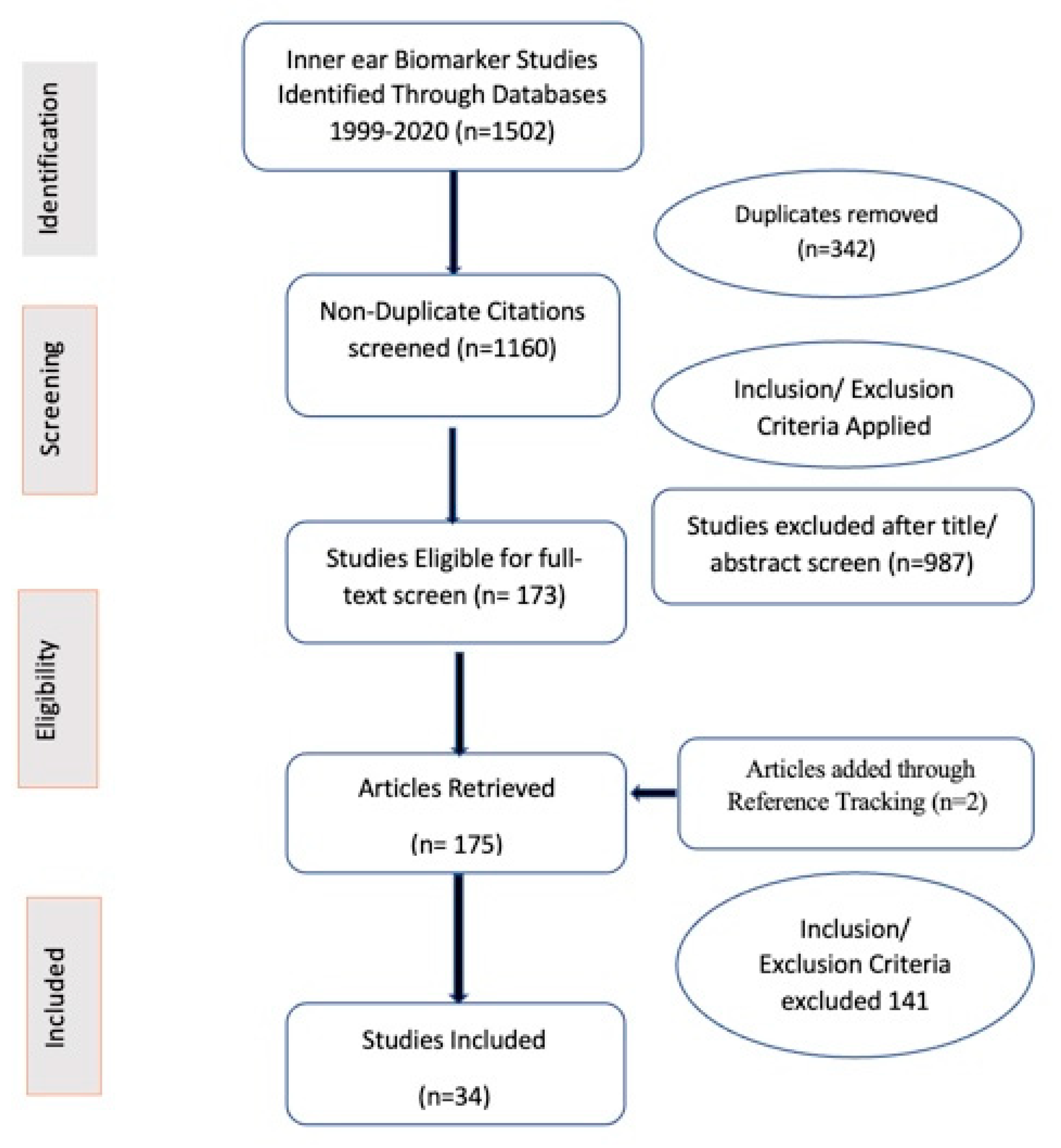
2.3. Screening Process
2.4. Data Extraction and Analysis
3. Results
3.1. Included Studies
3.2. Biomarker Classification
3.2.1. Molecular Biomarkers [Table 1 and 3]
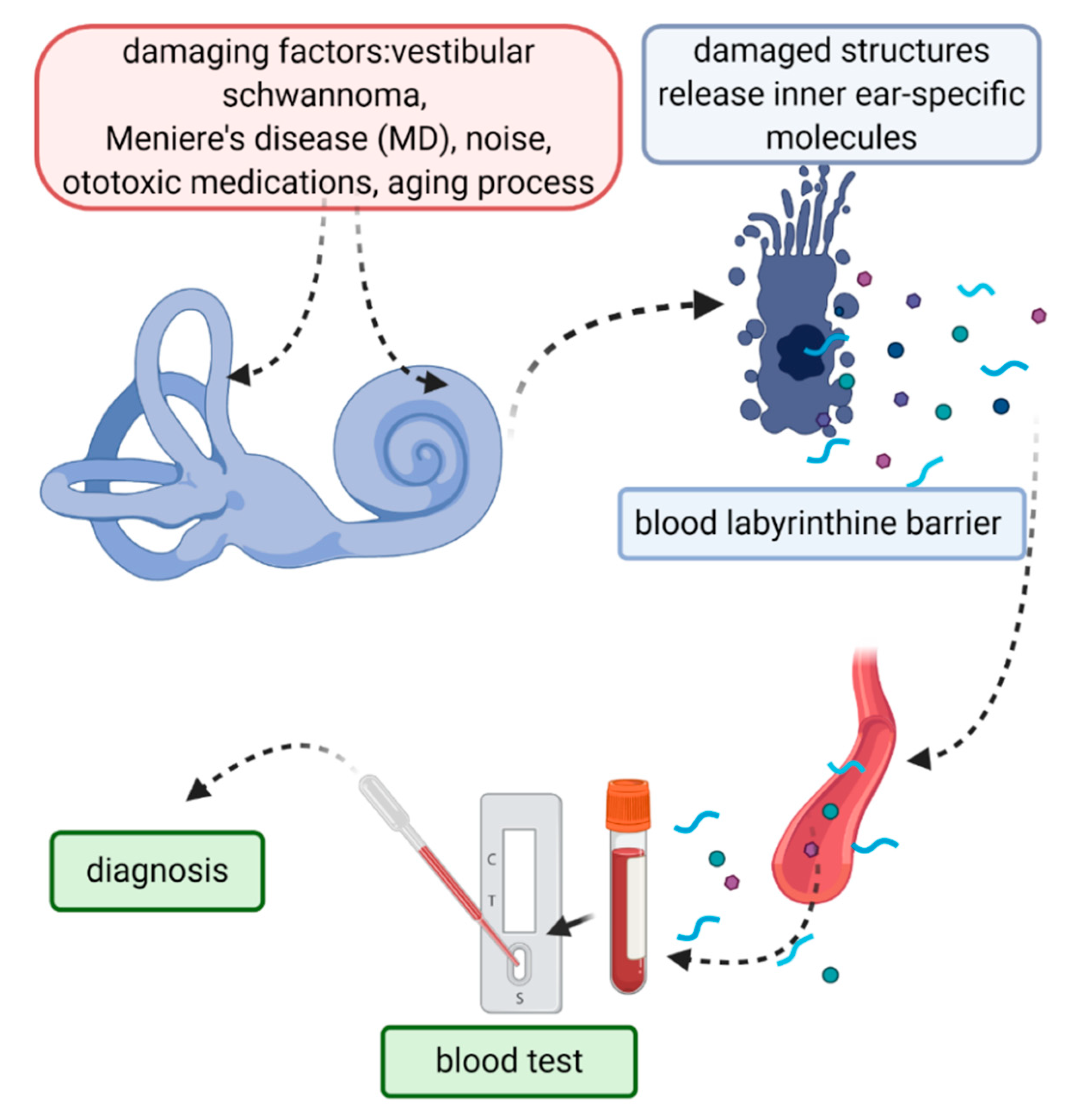
Inner Ear-Specific Protein Biomarkers that Can Be Detected in Peripheral Blood, Plasma, or Serum
Protein Biomarkers
Biomarkers of Inflammation
Antibody Biomarkers
Other Biomarkers
Inner-Ear-Specific Biomarkers Detected in the Perilymph or Inner Ear Structures
Biomarkers of Oxidative Stress [Damage]
Other Biomarkers
3.2.2. Functional Biomarkers [Tables 2 and 3]
4. Discussion
4.1. Study Limitations
4.2. Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Paone, J.F.; Phillip Waalkes, T.; Robinson Baker, R.; Shaper, J.H. Serum UDP-galactosyl transferase as a potential biomarker for breast carcinoma. J. Surg. Oncol. 1980, 15, 59–66. [Google Scholar] [CrossRef]
- McCarthy, J.F.; Shugart, L.R. Biomarkers of Environmental Contamination; Lewis Publisher: Boca Raton, FL, USA, 1990. [Google Scholar]
- Council, N.R. Committee on biological markers. Environ. Health Perspect. 1987, 74, 3–9. [Google Scholar]
- Depledge, M.H.; Fossi, M.C. The role of biomarkers in environmental assessment (2). Invertebrates. Ecotoxicology 1994, 3, 161–172. [Google Scholar] [CrossRef] [PubMed]
- Pardon, A.; Aubert, V.; Bart, P. Biomarkers in clinical immunology. Rev. Med. Suisse 2013, 9, 1982, 1984–1986, 1988. [Google Scholar] [PubMed]
- Garg, P.; Morris, P.; Fazlanie, A.L.; Vijayan, S.; Dancso, B.; Dastidar, A.G.; Plein, S.; Mueller, C.; Haaf, P. Cardiac biomarkers of acute coronary syndrome: From history to high-sensitivity cardiac troponin. Intern. Emerg. Med. 2017, 12, 147–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCabe, B.F. Autoimmune sensorineural hearing loss. Ann. Otol. Rhinol. Laryngol. 1979, 88, 585–589. [Google Scholar] [CrossRef] [PubMed]
- Parham, K.; Sacks, D.; Bixby, C.; Fall, P. Inner ear protein as a biomarker in circulation? Otolaryngol. Head Neck Surg. 2014, 151, 1038–1040. [Google Scholar] [CrossRef]
- Wong, E.H.C.; Dong, Y.Y.; Coray, M.; Cortada, M.; Levano, S.; Schmidt, A.; Brand, Y.; Bodmer, D.; Muller, L. Inner ear exosomes and their potential use as biomarkers. PLoS ONE 2018, 13, e0198029. [Google Scholar] [CrossRef] [Green Version]
- Fugazzola, L.; Cerutti, N.; Mannavola, D.; Crino, A.; Cassio, A.; Gasparoni, P.; Vannucchi, G.; Beck-Peccoz, P. Differential diagnosis between Pendred and pseudo-Pendred syndromes: Clinical, radiologic, and molecular studies. Pediatric Res. 2002, 51, 479–484. [Google Scholar] [CrossRef] [Green Version]
- Schmitt, H.; Roemer, A.; Zeilinger, C.; Salcher, R.; Durisin, M.; Staecker, H.; Lenarz, T.; Warnecke, A. Heat Shock Proteins in Human Perilymph: Implications for Cochlear Implantation. Otol. Neurotol. 2018, 39, 37–44. [Google Scholar] [CrossRef]
- Mijovic, T.; Zeitouni, A.; Colmegna, I. Autoimmune sensorineural hearing loss: The otology-rheumatology interface. Rheumatology (Oxford) 2013, 52, 780–789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Satoh, H.; Billings, P.; Firestein, G.S.; Harris, J.P.; Keithley, E.M. Transforming growth factor beta expression during an inner ear immune response. Ann. Otol. Rhinol. Laryngol. 2006, 115, 81–88. [Google Scholar] [CrossRef]
- Satoh, H.; Firestein, G.S.; Billings, P.B.; Harris, J.P.; Keithley, E.M. Proinflammatory cytokine expression in the endolymphatic sac during inner ear inflammation. J. Assoc. Res. Otolaryngol. 2003, 4, 139–147. [Google Scholar] [CrossRef] [Green Version]
- Merchant, S.N.; Durand, M.L.; Adams, J.C. Sudden deafness: Is it viral? ORL J. Otorhinolaryngol. Relat. Spec. 2008, 70, 52–62. [Google Scholar] [CrossRef] [Green Version]
- Pyykko, I.; Zou, J. Do viruses cause inner ear disturbances? ORL J. Otorhinolaryngol. Relat. Spec. 2008, 70, 32–41. [Google Scholar] [CrossRef]
- Livingston, G.; Sommerlad, A.; Orgeta, V.; Costafreda, S.G.; Huntley, J.; Ames, D.; Ballard, C.; Banerjee, S.; Burns, A.; Cohen-Mansfield, J.; et al. Dementia prevention, intervention, and care. Lancet 2017, 390, 2673–2734. [Google Scholar] [CrossRef] [Green Version]
- Howick, J.; Chalmers, I.; Glasziou, P.; Greenhalgh, T.; Heneghan, C.; Liberati, A.; Moschetti, I.; Phillips, B.; Thornton, H. Explanation of the 2011 Oxford Centre for Evidence-Based Medicine (OCEBM) Levels of Evidence (Background Document). (2011). 2018, Oxford Centre for Evidence-Based Medicine. Available online: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/ocebm-levels-of-evidence (accessed on 21 July 2019).
- Mulry, E.; Parham, K. Inner Ear Proteins as Potential Biomarkers. Otol. Neurotol. 2020, 41, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Deans, M.R.; Peterson, J.M.; Wong, G.W. Mammalian Otolin: A multimeric glycoprotein specific to the inner ear that interacts with otoconial matrix protein Otoconin-90 and Cerebellin-1. PLoS ONE 2010, 5, e12765. [Google Scholar] [CrossRef] [PubMed]
- Doğan, M.; Şahin, M.; Kurtulmuş, Y. Otolin-1, as a Potential Marker for Inner Ear Trauma after Mastoidectomy. J. Int. Adv. Otol. 2019, 15, 200–203. [Google Scholar] [CrossRef]
- Sacks, D.; Parham, K. Preliminary Report on the Investigation of the Association between BPPV and Osteoporosis Using Biomarkers. Otol. Neurotol. 2015, 36, 1532–1536. [Google Scholar] [CrossRef]
- Parham, K. Prestin as a biochemical marker for early detection of acquired sensorineural hearing loss. Med. Hypotheses 2015, 85, 130–133. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.; Xuan, X.; Zhou, Z.; Yuan, Y.; Xue, F. A Preliminary Report on the Investigation of Prestin as a Biomarker for Idiopathic Sudden Sensorineural Hearing Loss. Ear Nose Throat J. 2019, 99, 528–531. [Google Scholar] [CrossRef] [PubMed]
- Beck, K.; Gambee, J.E.; Bohan, C.A.; Bächinger, H.P. The C-terminal domain of cartilage matrix protein assembles into a triple-stranded alpha-helical coiled-coil structure. J. Mol. Biol. 1996, 256, 909–923. [Google Scholar] [CrossRef] [PubMed]
- Arnaud, L.; Mathian, A.; Haroche, J.; Gorochov, G.; Amoura, Z. Pathogenesis of relapsing polychondritis: A 2013 update. Autoimmun. Rev. 2014, 13, 90–95. [Google Scholar] [CrossRef]
- Ruckenstein, M.J.; Prasthoffer, A.; Bigelow, D.C.; Von Feldt, J.M.; Kolasinski, S.L. Immunologic and serologic testing in patients with Ménière’s disease. Otol. Neurotol. 2002, 23, 517–520; discussion 520-1. [Google Scholar] [CrossRef]
- Hajas, A.; Szodoray, P.; Barath, S.; Sipka, S.; Rezes, S.; Zeher, M.; Sziklai, I.; Szegedi, G.; Bodolay, E. Sensorineural hearing loss in patients with mixed connective tissue disease: Immunological markers and cytokine levels. J. Rheumatol. 2009, 36, 1930–1936. [Google Scholar] [CrossRef]
- Bovo, R.; Aimoni, C.; Martini, A. Immune-mediated inner ear disease. Acta Otolaryngol. 2006, 126, 1012–1021. [Google Scholar] [CrossRef]
- Lee, J.M.; Kim, J.Y.; Bok, J.; Kim, K.S.; Choi, J.Y.; Kim, S.H. Identification of evidence for autoimmune pathology of bilateral sudden sensorineural hearing loss using proteomic analysis. Clin. Immunol. 2017, 183, 24–35. [Google Scholar] [CrossRef]
- Hoffman, R.W.; Maldonado, M.E. Immune pathogenesis of mixed connective tissue disease: A short analytical review. Clin. Immunol. 2008, 128, 8–17. [Google Scholar] [CrossRef]
- Maldonado, M.E.; Perez, M.; Pignac-Kobinger, J.; Marx, E.T.; Tozman, E.M.; Greidinger, E.L.; Hoffman, R.W. Clinical and immunologic manifestations of mixed connective tissue disease in a Miami population compared to a Midwestern US Caucasian population. J. Rheumatol. 2008, 35, 429–437. [Google Scholar]
- Greidinger, E.L.; Hoffman, R.W. Autoantibodies in the pathogenesis of mixed connective tissue disease. Rheum. Dis. Clin. 2005, 31, 437–450. [Google Scholar] [CrossRef] [PubMed]
- Alawieh, A.; Mondello, S.; Kobeissy, F.; Shibbani, K.; Bassim, M. Proteomics studies in inner ear disorders: Pathophysiology and biomarkers. Expert Rev. Proteom. 2015, 12, 185–196. [Google Scholar] [CrossRef] [PubMed]
- Chiarella, G.; Saccomanno, M.; Scumaci, D.; Gaspari, M.; Faniello, M.C.; Quaresima, B.; Di Domenico, M.; Ricciardi, C.; Petrolo, C.; Cassandro, C.; et al. Proteomics in Ménière disease. J. Cell. Physiol. 2012, 227, 308–312. [Google Scholar] [CrossRef] [PubMed]
- Yukawa, K.; Hagiwara, A.; Ogawa, Y.; Nishiyama, N.; Shimizu, S.; Kawaguchi, S.; Nakamura, M.; Ito, H.; Tomiyama, S.; Suzuki, M. Bilateral progressive hearing loss and vestibular dysfunction with inner ear antibodies. Auris Nasus Larynx 2010, 37, 223–228. [Google Scholar] [CrossRef]
- Harris, J.P.; Sharp, P.A. Inner ear autoantibodies in patients with rapidly progressive sensorineural hearing loss. Laryngoscope 1990, 100, 516–524. [Google Scholar] [CrossRef]
- Haase, G.M.; Prasad, K.N. Oxidative damage and inflammation biomarkers: Strategy in hearing disorders. Otol. Neurotol. 2016, 37, e303–e308. [Google Scholar] [CrossRef]
- Süslü, N.; Yilmaz, T.; Gürsel, B. Utility of anti-HSP 70, TNF-alpha, ESR, antinuclear antibody, and antiphospholipid antibodies in the diagnosis and treatment of sudden sensorineural hearing loss. Laryngoscope 2009, 119, 341–346. [Google Scholar] [CrossRef]
- Yehudai, D.; Shoenfeld, Y.; Toubi, E. The autoimmune characteristics of progressive or sudden sensorineural hearing loss. Autoimmunity 2006, 39, 153–158. [Google Scholar] [CrossRef]
- Betancur, J.F.; Londoño, A.; Estrada, V.E.; Puerta, S.L.; Osorno, S.M.; Loaiza, A.; Carmona, J.A.; Gómez-Puerta, J.A. Uncommon patterns of antinuclear antibodies recognizing mitotic spindle apparatus antigens and clinical associations. Medicine (Baltimore) 2018, 97, e11727. [Google Scholar] [CrossRef]
- Berti, E.; Vannucci, G.; Lunardi, C.; Bianchi, B.; Bason, C.; Puccetti, A.; Giani, T.; Pagnini, I.; Cimaz, R.; Simonini, G. Identification of autoantibodies against inner ear antigens in a cohort of children with idiopathic sensorineural hearing loss. Autoimmunity 2013, 46, 525–530. [Google Scholar] [CrossRef]
- Vogt, B.A.; Wyatt, R.J.; Burke, B.A.; Simonton, S.C.; Kashtan, C.E. Inherited factor H deficiency and collagen type III glomerulopathy. Pediatr. Nephrol. 1995, 9, 11–15. [Google Scholar] [CrossRef] [PubMed]
- Ying, L.; Katz, Y.; Schlesinger, M.; Carmi, R.; Shalev, H.; Haider, N.; Beck, G.; Sheffield, V.C.; Landau, D. Complement factor H gene mutation associated with autosomal recessive atypical hemolytic uremic syndrome. Am. J. Hum. Genet. 1999, 65, 1538–1546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, M.; Atmaca-Sonmez, P.; Othman, M.; Branham, K.E.; Khanna, R.; Wade, M.S.; Li, Y.; Liang, L.; Zareparsi, S.; Swaroop, A.; et al. CFH haplotypes without the Y402H coding variant show strong association with susceptibility to age-related macular degeneration. Nat. Genet. 2006, 38, 1049–1054. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Närkiö-Mäkelä, M.; Hellwage, J.; Tahkokallio, O.; Meri, S. Complement-regulator factor H and related proteins in otitis media with effusion. Clin. Immunol. 2001, 100, 118–126. [Google Scholar] [CrossRef]
- Toubi, E.; Ben-David, J.; Kessel, A.; Halas, K.; Sabo, E.; Luntz, M. Immune-mediated disorders associated with idiopathic sudden sensorineural hearing loss. Ann. Otol. Rhinol. Laryngol. 2004, 113, 445–449. [Google Scholar] [CrossRef]
- Procaccio, V.; Salazar, G.; Ono, S.; Styers, M.L.; Gearing, M.; Davila, A.; Jimenez, R.; Juncos, J.; Gutekunst, C.A.; Meroni, G.; et al. A mutation of beta -actin that alters depolymerization dynamics is associated with autosomal dominant developmental malformations, deafness, and dystonia. Am. J. Hum. Genet. 2006, 78, 947–960. [Google Scholar] [CrossRef] [Green Version]
- Accetturo, M.; Creanza, T.M.; Santoro, C.; Tria, G.; Giordano, A.; Battagliero, S.; Vaccina, A.; Scioscia, G.; Leo, P. Finding new genes for non-syndromic hearing loss through an in silico prioritization study. PLoS ONE 2010, 5, e12742. [Google Scholar] [CrossRef]
- Aoki, M.; Asai, M.; Nishihori, T.; Mizuta, K.; Ito, Y.; Ando, K. The relevance of an elevation in the plasma vasopressin levels to the pathogenesis of Meniere’s attack. J. Neuroendocrinol. 2007, 19, 901–906. [Google Scholar] [CrossRef]
- Kumagami, H.; Loewenheim, H.; Beitz, E.; Wild, K.; Schwartz, H.; Yamashita, K.; Schultz, J.; Paysan, J.; Zenner, H.P.; Ruppersberg, J.P. The effect of anti-diuretic hormone on the endolymphatic sac of the inner ear. Pflügers Arch. 1998, 436, 970–975. [Google Scholar] [CrossRef]
- Takeda, T.; Takeda, S.; Kitano, H.; Okada, T.; Kakigi, A. Endolymphatic hydrops induced by chronic administration of vasopressin. Hear. Res. 2000, 140, 1–6. [Google Scholar] [CrossRef]
- Lee, W.M.; Galbraith, R.M. The extracellular actin-scavenger system and actin toxicity. N. Engl. J. Med. 1992, 326, 1335–1341. [Google Scholar] [PubMed]
- Gasparri, C.; Curcio, A.; Torella, D.; Gaspari, M.; Celi, V.; Salituri, F.; Boncompagni, D.; Torella, M.; Gulletta, E.; Cuda, G.; et al. Proteomics reveals high levels of vitamin D binding protein in myocardial infarction. Front. Biosci. 2010, 2, 796–804. [Google Scholar]
- Rüttiger, L.; Zimmermann, U.; Knipper, M. Biomarkers for Hearing Dysfunction: Facts and Outlook. ORL J. Otorhinolaryngol. Relat. Spec. 2017, 79, 93–111. [Google Scholar] [CrossRef] [PubMed]
- Serra-Millas, M. Are the changes in the peripheral brain-derived neurotrophic factor levels due to platelet activation? World J. Psychiatry 2016, 6, 84–101. [Google Scholar] [CrossRef]
- Radka, S.F.; Holst, P.A.; Fritsche, M.; Altar, C.A. Presence of brain-derived neurotrophic factor in brain and human and rat but not mouse serum detected by a sensitive and specific immunoassay. Brain Res. 1996, 709, 122–301. [Google Scholar] [CrossRef]
- de Kok, Y.J.; Bom, S.J.; Brunt, T.M.; Kemperman, M.H.; van Beusekom, E.; van der Velde-Visser, S.D.; Robertson, N.G.; Morton, C.C.; Huygen, P.L.; Verhagen, W.I.; et al. A Pro51Ser mutation in the COCH gene is associated with late onset autosomal dominant progressive sensorineural hearing loss with vestibular defects. Hum. Mol. Genet. 1999, 8, 361–366. [Google Scholar] [CrossRef] [Green Version]
- Ikezono, T.; Matsumura, T.; Matsuda, H.; Shikaze, S.; Saitoh, S.; Shindo, S.; Hasegawa, S.; Oh, S.H.; Hagiwara, Y.; Ogawa, Y.; et al. The diagnostic performance of a novel ELISA for human CTP (Cochlin-tomoprotein) to detect perilymph leakage. PLoS ONE 2018, 13, e0191498. [Google Scholar] [CrossRef] [Green Version]
- Calzada, A.P.; Lopez, I.A.; Beltran Parrazal, L.; Ishiyama, A.; Ishiyama, G. Cochlin expression in vestibular endorgans obtained from patients with Meniere’s disease. Cell Tissue Res. 2012, 350, 373–384. [Google Scholar] [CrossRef] [Green Version]
- Pathak, S.; Hatam, L.J.; Bonagura, V.; Vambutas, A. Innate immune recognition of molds and homology to the inner ear protein, cochlin, in patients with autoimmune inner ear disease. J. Clin. Immunol. 2013, 33, 1204–1215. [Google Scholar] [CrossRef] [Green Version]
- Decourt, B.; Hillman, D.; Bouleau, Y.; Dulon, D.; Hafidi, A. Is otospiralin inner ear specific? Evidence for its expression in mouse brain. Int. J. Dev. Neurosci. 2009, 27, 87–96. [Google Scholar] [CrossRef]
- Robertson, N.G.; Resendes, B.L.; Lin, J.S.; Lee, C.; Aster, J.C.; Adams, J.C.; Morton, C.C. Inner ear localization of mRNA and protein products of COCH, mutated in the sensorineural deafness and vestibular disorder, DFNA9. Hum. Mol. Genet. 2001, 10, 2493–2500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yin, Y.; Henzl, M.T.; Lorber, B.; Nakazawa, T.; Thomas, T.T.; Jiang, F.; Langer, R.; Benowitz, L.I. Oncomodulin is a macrophage-derived signal for axon regeneration in retinal ganglion cells. Nat. Neurosci. 2006, 9, 843–852. [Google Scholar] [CrossRef]
- Sakaguchi, N.; Henzl, M.T.; Thalmann, I.; Thalmann, R.; Schulte, B.A. Oncomodulin is expressed exclusively by outer hair cells in the organ of Corti. J. Histochem. Cytochem. 1998, 46, 29–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, H.-C.; Ren, Y.; Lysaght, A.C.; Kao, S.Y.; Stankovic, K.M. Proteome of normal human perilymph and perilymph from people with disabling vertigo. PLoS ONE 2019, 14, e0218292. [Google Scholar] [CrossRef] [PubMed]
- Pennisi, R.; Ascenzi, P.; di Masi, A. Hsp90: A New Player in DNA Repair? Biomolecules 2015, 5, 2589–2618. [Google Scholar] [CrossRef] [Green Version]
- Jókay, I.; Papp, Z.; Soós, G.; Sziklai, I.; Dezsö, B. The effect of chronic otitis media on the immunoreactivity of human inner ear. Eur. Arch. 2001, 258, 529–532. [Google Scholar] [CrossRef]
- Choi, S.H.; Choi, C.H. Noise-Induced Neural Degeneration and Therapeutic Effect of Antioxidant Drugs. J. Audiol. Otol. 2015, 19, 111–119. [Google Scholar] [CrossRef] [Green Version]
- Pall, M.L.; Bedient, S.A. The NO/ONOO- cycle as the etiological mechanism of tinnitus. Int. Tinnitus J. 2007, 13, 99–104. [Google Scholar]
- Szczepek, A.J.; Haupt, H.; Klapp, B.F.; Olze, H.; Mazurek, B. Biological correlates of tinnitus-related distress: An exploratory study. Hear. Res. 2014, 318, 23–30. [Google Scholar] [CrossRef]
- Hoshino, T.; Tabuchi, K.; Nishimura, B.; Tanaka, S.; Nakayama, M.; Ishii, T.; Warabi, E.; Yanagawa, T.; Shimizu, R.; Yamamoto, M.; et al. Protective role of Nrf2 in age-related hearing loss and gentamicin ototoxicity. Biochem. Biophys. Res. Commun. 2011, 415, 94–98. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.J.; So, H.S.; Lee, J.H.; Park, C.; Lee, J.B.; Youn, M.J.; Kim, S.J.; Yang, S.H.; Lee, K.M.; Kwon, K.B.; et al. Role of proinflammatory cytokines in cisplatin-induced vestibular hair cell damage. Head Neck J. Sci. Spec. Head Neck 2008, 30, 1445–1456. [Google Scholar] [CrossRef] [PubMed]
- Evans, P.; Halliwell, B. Free radicals and hearing. Cause, consequence, and criteria. Ann. N. Y. Acad. Sci. 1999, 884, 19–40. [Google Scholar] [CrossRef] [PubMed]
- Okano, T. Immune system of the inner ear as a novel therapeutic target for sensorineural hearing loss. Front. Pharmacol. 2014, 5, 205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Archibald, D.J.; Neff, B.A.; Voss, S.G.; Splinter, P.L.; Driscoll, C.L.; Link, M.J.; Dong, H.; Kwon, E.D. B7-H1 expression in vestibular schwannomas. Otol. Neurotol. 2010, 31, 991–997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edvardsson Rasmussen, J.; Laurell, G.; Rask-Andersen, H.; Bergquist, J.; Eriksson, P.O. The proteome of perilymph in patients with vestibular schwannoma. A possibility to identify biomarkers for tumor associated hearing loss? PLoS ONE 2018, 13, e0198442. [Google Scholar] [CrossRef] [PubMed]
- Hansen, M.R.; Linthicum, F.H., Jr. Expression of neuregulin and activation of erbB receptors in vestibular schwannomas: Possible autocrine loop stimulation. Otol. Neurotol. 2004, 25, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Barozzi, S.; Ginocchio, D.; Socci, M.; Alpini, D.; Cesarani, A. Audiovestibular disorders as autoimmune reaction in patients with melanoma. Med. Hypotheses 2015, 85, 336–338. [Google Scholar] [CrossRef]
- Campbell, J.D.; Cardon, G.; Sharma, A. Clinical Application of the P1 Cortical Auditory Evoked Potential Biomarker in Children with Sensorineural Hearing Loss and Auditory Neuropathy Spectrum Disorder. Semin. Hear. 2011, 32, 147–155. [Google Scholar] [CrossRef] [Green Version]
- Mostafa, I.; Shabana, M.I.; El Shennawy, A.M.; Weheiba, H.M. Assessing the applications of cortical auditory evoked potentials as a biomarker in children with hearing aids. Egypt. J. Otolaryngol. 2014, 30, 38–42. [Google Scholar]
- Counter, S.A.; Buchanan, L.H. Neuro-ototoxicity in andean adults with chronic lead and noise exposure. J. Occup. Environ. Med. 2002, 44, 30–38. [Google Scholar] [CrossRef]
- Deshpande, A.K.; Tan, L.; Lu, L.J.; Altaye, M.; Holland, S.K. fMRI as a Preimplant Objective Tool to Predict Postimplant Oral Language Outcomes in Children with Cochlear Implants. Ear Hear. 2016, 37, e263–e272. [Google Scholar] [CrossRef] [PubMed]
- Dewey, R.S.; Hall, D.A.; Guest, H.; Prendergast, G.; Plack, C.J.; Francis, S.T. The Physiological Bases of Hidden Noise-Induced Hearing Loss: Protocol for a Functional Neuroimaging Study. JMIR Res. Protoc. 2018, 7, e79. [Google Scholar] [CrossRef] [PubMed]
- Gilley, P.M.; Sharma, A.; Dorman, M.F. Cortical reorganization in children with cochlear implants. Brain Res. 2008, 1239, 56–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quaranta, A.; Portalatini, P.; Henderson, D. Temporary and permanent threshold shift: An overview. Scand Audiol. Suppl. 1998, 48, 75–86. [Google Scholar]
- Feuerstein, A.; Herbst, A.; Wallner, P. Another biomarker of susceptibility to noiseinduced hearing loss. Biomonitoring 2014, 1. [Google Scholar] [CrossRef]
- Moshammer, H.; Kundi, M.; Wallner, P.; Herbst, A.; Feuerstein, A.; Hutter, H.P. Early prognosis of noise-induced hearing loss. Occup. Environ. Med. 2015, 72, 85–89. [Google Scholar] [CrossRef]
- Kemp, D. Otoacoustic Emissions in Perspective, Otoacoustic Emissions: Clinical Applications; Robinette, M.S., Glattke, T.J., Eds.; Thieme: New York, NY, USA, 1997. [Google Scholar]
- Garrett, A.; Heibert, D.; Lithgow, B. Electrovestibulography: The “DC” potential used to separate Meniere’s disease and Benign Paroxysmal Positional Vertigo. In Proceedings of the 2007 29th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Lyon, France, 23–26 August 2007. [Google Scholar]
- Lithgow, B.J.; Heibert, D. EVestG signals: Feature selection. In Proceedings of the 2009 4th International IEEE/EMBS Conference on Neural Engineering, Antalya, Turkey, 29 April–2 May 2019; pp. 618–621. [Google Scholar]
- Kim, S.H.; Kim, J.Y.; Lee, H.J.; Gi, M.; Kim, B.G.; Choi, J.Y. Autoimmunity as a candidate for the etiopathogenesis of Meniere’s disease: Detection of autoimmune reactions and diagnostic biomarker candidate. PLoS ONE 2014, 9, e111039. [Google Scholar] [CrossRef] [Green Version]
- Dimitrijevic, A.; Alsamri, J.; John, M.S.; Purcell, D.; George, S.; Zeng, F.G. Human Envelope Following Responses to Amplitude Modulation: Effects of Aging and Modulation Depth. Ear Hear. 2016, 37, e322–e335. [Google Scholar] [CrossRef] [Green Version]
- Coffey, E.B.; Herholz, S.C.; Chepesiuk, A.M.; Baillet, S.; Zatorre, R.J. Cortical contributions to the auditory frequency-following response revealed by MEG. Nat. Commun. 2016, 7, 11070. [Google Scholar] [CrossRef]
- Stokroos, R.J.; Albers, F.W.; Krikke, A.P.; Casselman, J.W. Magnetic resonance imaging of the inner ear in patients with idiopathic sudden sensorineural hearing loss. Eur. Arch. Otorhinolaryngol. 1998, 255, 433–436. [Google Scholar] [CrossRef]
- Tebo, A.E.; Szankasi, P.; Hillman, T.A.; Litwin, C.M.; Hill, H.R. Antibody reactivity to heat shock protein 70 and inner ear-specific proteins in patients with idiopathic sensorineural hearing loss. Clin. Exp. Immunol. 2006, 146, 427–432. [Google Scholar] [CrossRef] [PubMed]
- Ballesteros, F.; Alobid, I.; Tassies, D.; Reverter, J.C.; Scharf, R.E.; Guilemany, J.M.; Bernal-Sprekelsen, M. Is there an overlap between sudden neurosensorial hearing loss and cardiovascular risk factors? Audiol. Neurootol. 2009, 14, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Micheel, C.M.; Ball, J.R. (Eds.) Institute of Medicine Committee on Qualification of, B. and D. Surrogate Endpoints in Chronic, in Evaluation of Biomarkers and Surrogate Endpoints in Chronic Disease; National Academies Press (US) Copyright 2010 by the National Academy of Sciences: Washington, DC, USA, 2010. [Google Scholar]
- Chang, K.W. Genetics of Hearing Loss—Nonsyndromic. Otolaryngol. Clin. N. Am. 2015, 48, 1063–1072. [Google Scholar] [CrossRef]
- Matsuoka, A.J.; Harris, J.P. Autoimmune inner ear disease: A retrospective review of forty-seven patients. Audiol. Neurootol. 2013, 18, 228–239. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author | Year | Study Type | Level of Evidence | Met Objectives | Biomarker | Key Source | Category | Ref. |
|---|---|---|---|---|---|---|---|---|
| Archibald et al. | 2010 | Blind retrospective chart review | 3b | Yes | B7-H1 expression in lymphocytes | Fresh frozen vestibular schwannoma Tissue | Diagnostic | [76] |
| Edvardsson Rasmussen et al. | 2018 | Observational | 4 | Yes | Alpha-2-HS-Glycoprotein | Perilymph aspirated through round window membrane | Prognostic | [77] |
| Schmitt et al. * | 2018 | Observational | 3b | Partially | Heat shock proteins | Perilymph & Cochl.T | Diagnostic | [11] |
| Lee et al. ** | 2017 | Observational | 1b | Yes | Autoimmunity; elevated sera CRP & ESR in addition to many other proteins specific for autoimmune inner ear disease, or sudden SNHL | Blood | Diagnostic | [30] |
| Kim et al. *** | 2014 | Prospective correlational | 3b | partially | Neuro-immunology antigens involved in immune reactions | Endolymphatic sac luminal fluid from 3 patients & peripheral blood from 10 patients | Diagnostic | [92] |
| Betancur et al. | 2018 | Prospective correlational | 1b | Yes | Anti-centrosome antibodies, MSA-2 CENTP-F/MSA-3, Nu-MA/MSA-1 | Serum | Diagnostic | [41] |
| Hajas et al. **** | 2009 | Prospective correlational | 2b | Partially | T cell count, IgG antibodies Anti-endothelial cell antibodies [AECA]; High levels of anti- U1RNP, IgG type aCL & AECA | Plasma & Serum | Diagnostic | [28] |
| Ikezono et al. | 2018 | Prospective correlational cohort | 2b | Yes | Perilymph specific protein Cochlin-tomoprotein [CTP] | MEL [Middle ear lavage] & Peripheral blood [Plasma & Serum | Diagnostic | [59] |
| Berti et al. ***** | 2013 | Observational study | 3b | No | Inner ear autoantibodies | Serum | Prognostic | [42] |
| Sacks & Parham | 2015 | Prospective pilot clinical trial | 2b | No | Otolin-1 | Serum | Diagnostic | [22] |
| Haase & Prasad ****** | 2016 | Research guidance papers | 1a | Yes | Biomarkers of oxidative stress; Biomarkers of inflammation | Peripheral blood | Diagnostic | [38] |
| Aoki et al. | 2007 | Retrospective cohort | 2b | No | Plasma osmolality; plasma Vasopressin levels | Plasma | Diagnostic | [50] |
| Parham et al. | 2014 | Retrospective controlled cohort | 3b | No | Otolin-1 | Serum | Diagnostic | [8] |
| Jókay et al. | 2001 | Retrospective observational | 2b | Yes | Staining for 27E10 in chronic otitis media | Temporal bones from autopsies | Pathogenic | [68] |
| Hansen & Linthicum | 2004 | Retrospective observational | 4 | Yes | ERB2 & E3, Neuregulin | Pathological specimens of vestibular schwannoma | Diagnostic | [78] |
| Chiarella et al. | 2012 | Cohort | 2b | Partially | Beta 2 glycoprotein, beta actin, complement factor-H, vit. D binding protein | Plasma | Diagnostic | [35] |
| Author | Year | Study Type | Level of Evidence | Met Objectives | BioMarker | Category | Ref |
|---|---|---|---|---|---|---|---|
| Mostafa et al. | 2014 | Correlational cohort | 1b | Partially | P1 CAEP | Diagnostic | [81] |
| Dimitrijevic | 2016 | Correlational thesis | 2b | No | Envelope following response | Diagnostic/Prognostic | [93] |
| Counter & Buchanan | 2002 | Correlational | 2b | No | Brainstem auditory evoked responses | Diagnostic | [82] |
| Campbell | 2011 | Descriptive | 4 | No | P1 component of the cortical auditory evoked potential | Treatment | [80] |
| Dewey et al. | 2018 | Observational | 1b | No | Regions of Interest (ROIs) on fMRI | Diagnostic | [84] |
| Brainstem auditory evoked responses | Diagnostic | ||||||
| Feuerstein et al. | 2015 | Observational | 5 | No | Temporal Threshold Shift (TTS) | Predictive | [88] |
| Moshammer et al. | 2015 | Pre- and post, correlational | 1c | Yes | Temporal Threshold Shift (TTS) | Diagnostic | [88] |
| Coffey et al. | 2016 | Prospective observational | 2b | Yes | Auditory Frequency Following Response (FFR) | Diagnostic | [94] |
| Choi et al. | 2017 | Secondary analysis of a double-blinded randomized clinical trial | 2b | Yes | Electrode impedance fluctuations | Prognostic | [69] |
| Deshpande et al. * | 2016 | Prospective correlational | 1b | Yes | Preoperative fMRI activation in angular, cingulate gyri and prefrontal cortex | Predictive | [83] |
| Author | Year | Level of Evidence | Met Objectives | BioMarker | Key Source | Classification | Category | |
|---|---|---|---|---|---|---|---|---|
| Evans & Halliwell | 1999 | 2a | Yes | Reactive oxygen and nitrogen species | Review of intracellular & extracellular antioxidants | Molecular | Pathophysiology/Therapeutic | [74] |
| Arnaud et al. * | 2014 | 2a | Partially | CII Ab & cell immunity in relapsing polychondritis | Review of immunity in serum | Molecular | Pathogenic model | [26] |
| Matrilin-1 in relapsing polychondritis | Review of immunity in serum | Molecular | Pathogenic model | |||||
| Okano ** | 2014 | 5 | Too broad | Immune markers | Review of immunity in serum | Molecular | Pathophysiology/Therapeutic | [75] |
| Alawieh et al. *** | 2015 | 1a | Yes | Biomarkers of inflammation | Review of immunity in plasma | Molecular | Diagnostic | [34] |
| Barozzi et al. | 2015 | 2a | No | Inner ear melanocytes | Review of aggregated inner ear melanocytes papers | Molecular | Diagnostic | [79] |
| Rüttiger et al. **** | 2017 | 5 | Yes | Overview of both functional & molecular [e.g., BDNF] | Evoked potentials + Aggregated IHCs & OHCs biomarkers in animal & human studies | Functional and Molecular | Diagnostic/Pathognomonic | [55] |
| Mulry & Parham | 2020 | 2a | Yes | Inner ear/preclinical models: (Otoconin 90/95, Otogelin, Otoancorin, Cochlin, α-tectorin, β-tectorin.) Vestibular biomarkers: Cochlin & Otolin- | Review of aggregated data of proteins specific to the inner ear, some of which could be detected outside the inner ear | Molecular | Diagnostic | [19] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gomaa, N.A.; Jimoh, Z.; Campbell, S.; Zenke, J.K.; Szczepek, A.J. Biomarkers for Inner Ear Disorders: Scoping Review on the Role of Biomarkers in Hearing and Balance Disorders. Diagnostics 2021, 11, 42. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11010042
Gomaa NA, Jimoh Z, Campbell S, Zenke JK, Szczepek AJ. Biomarkers for Inner Ear Disorders: Scoping Review on the Role of Biomarkers in Hearing and Balance Disorders. Diagnostics. 2021; 11(1):42. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11010042
Chicago/Turabian StyleGomaa, Nahla A., Zaharadeen Jimoh, Sandra Campbell, Julianna K. Zenke, and Agnieszka J. Szczepek. 2021. "Biomarkers for Inner Ear Disorders: Scoping Review on the Role of Biomarkers in Hearing and Balance Disorders" Diagnostics 11, no. 1: 42. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11010042