
Is the 1-Minute Sit-To-Stand Test a Good Tool to Evaluate Exertional Oxygen Desaturation in Chronic Obstructive Pulmonary Disease?

Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Study Design
2.3. Outcome Measurements
2.3.1. Six-Minute Walking Test (6MWT)
2.3.2. One-Minute Sit-to-Stand Test (1STST)
2.4. Statistical Analysis
3. Results
3.1. Participants
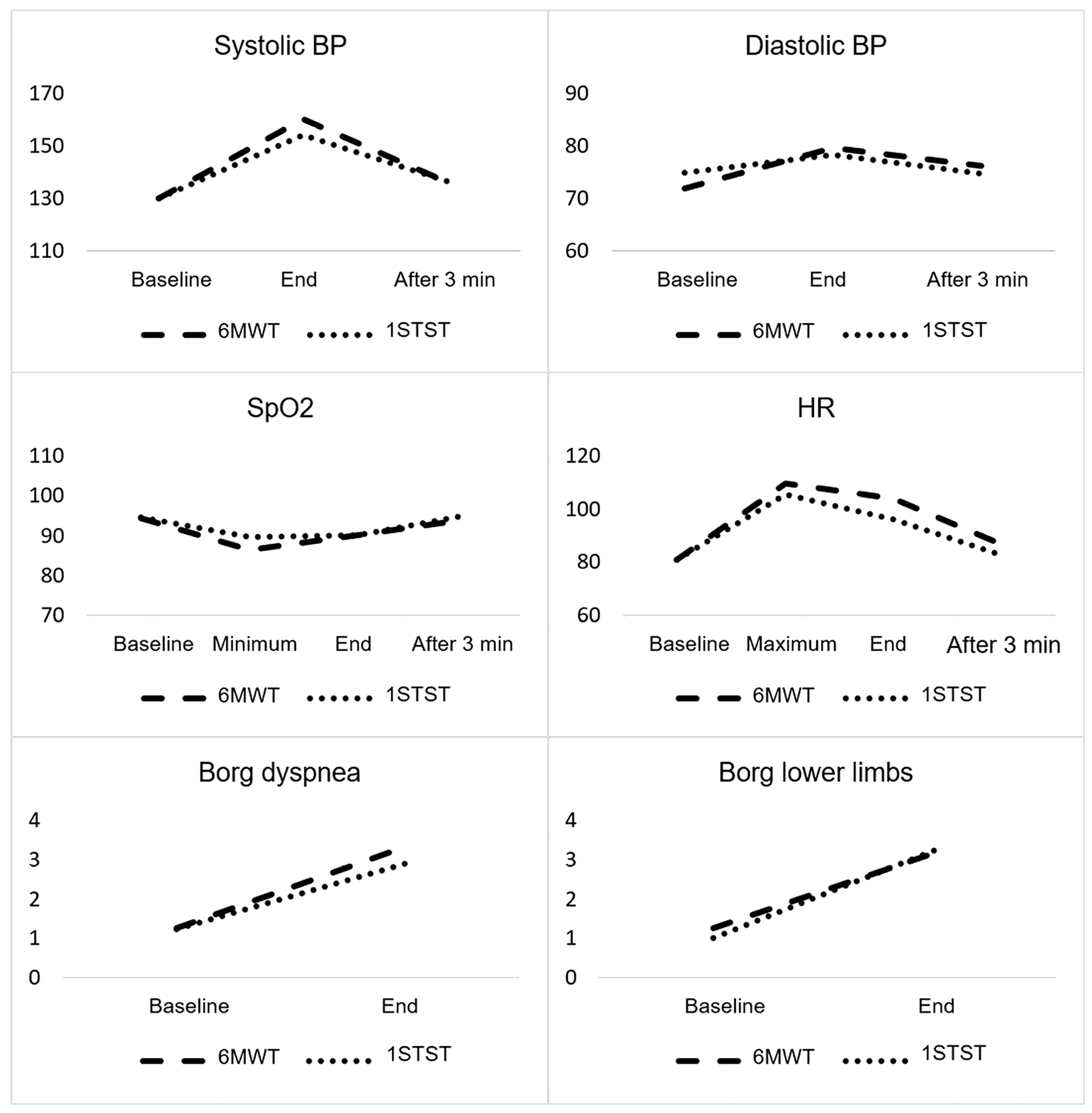
3.2. Comparison of Exercise Capacity and Cardiorespiratory Parameters between the 1STST and the 6MWT
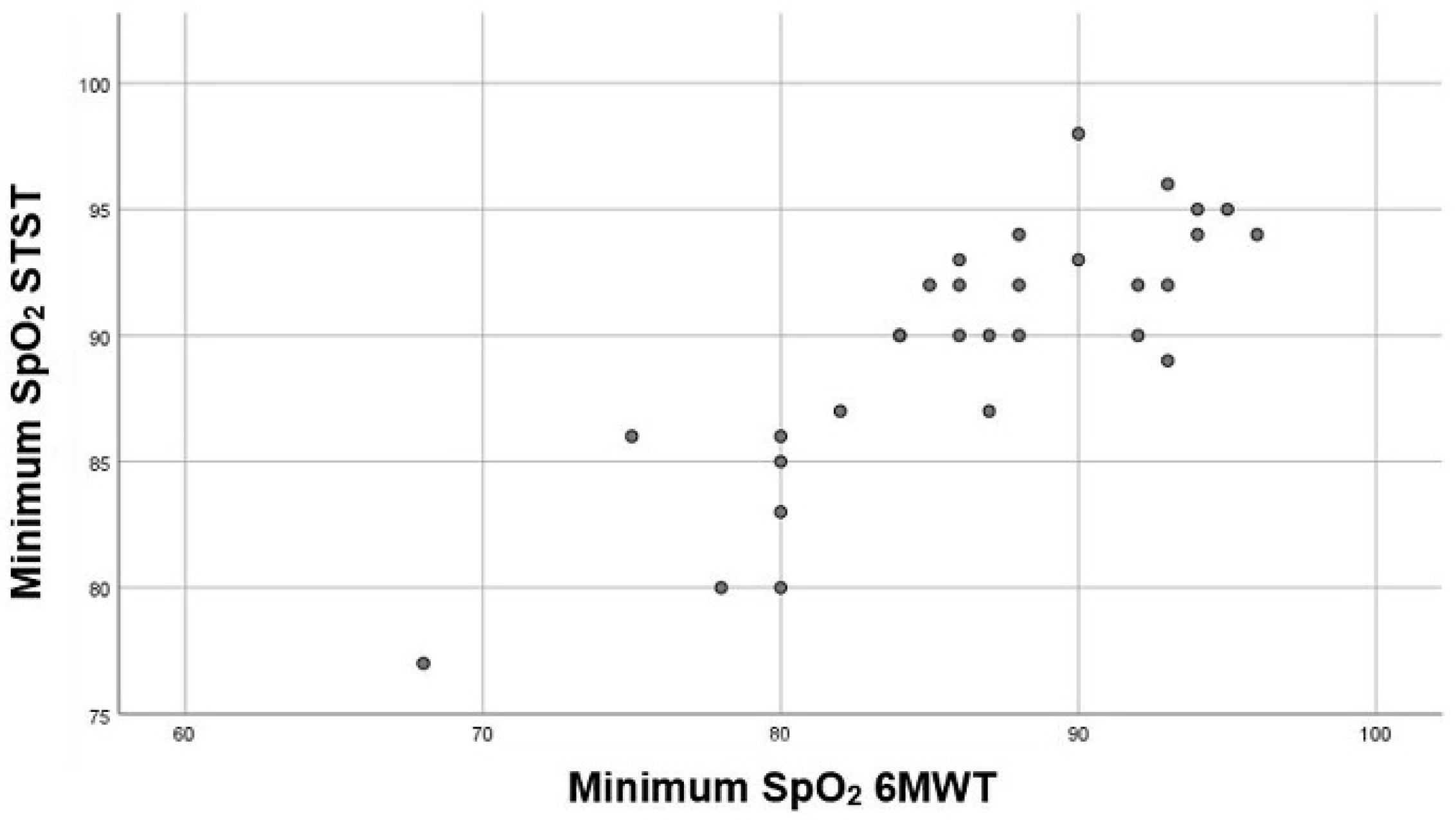
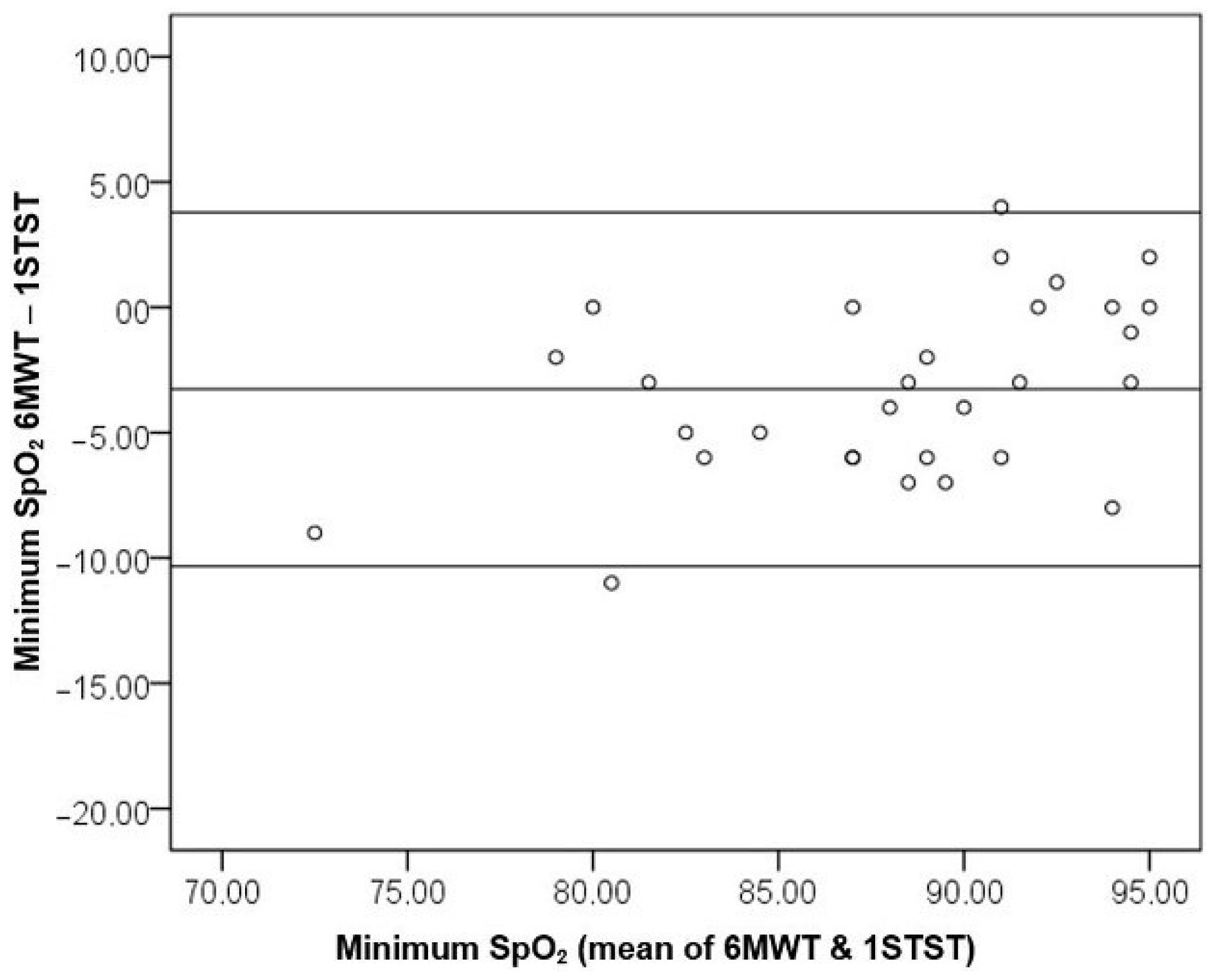
3.3. Comparison of Oxygen Desaturation between the 1STST and 6MWT
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Global Initiative for Chronic Obstructive Lung Disease—Global Initiative for Chronic Obstructive Lung Disease—GOLD. Available online: https://goldcopd.org/ (accessed on 25 December 2020).
- Waatevik, M.; Johannessen, A.; Real, F.G.; Aanerud, M.; Hardie, J.A.; Bakke, P.S.; Eagan, T.M.L. Oxygen Desaturation in 6-Min Walk Test is a Risk Factor for Adverse Outcomes in COPD. Eur. Respir. J. 2016, 48, 82–91. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, I.; Guimarães, M.J.; van Zeller, M.; Menezes, F.; Moita, J.; Simão, P. Clinical and Molecular Markers in COPD. Pulmonology 2018, 24, 250–259. [Google Scholar] [CrossRef] [PubMed]
- Holland, A.E.; Spruit, M.A.; Troosters, T.; Puhan, M.A.; Pepin, V.; Saey, D.; McCormack, M.C.; Carlin, B.W.; Sciurba, F.C.; Pitta, F.; et al. An Official European Respiratory Society/American Thoracic Society Technical Standard: Field Walking Tests in Chronic Respiratory Disease. Eur. Respir. J. 2014, 44, 1428–1446. [Google Scholar] [CrossRef] [PubMed]
- Csuka, M.; McCarty, D.J. Simple Method for Measurement of Lower Extremity Muscle Strength. Am. J. Med. 1985, 78, 77–81. [Google Scholar] [CrossRef]
- Jones, S.E.; Kon, S.S.C.; Canavan, J.L.; Patel, M.S.; Clark, A.L.; Nolan, C.M.; Polkey, M.I.; Man, W.D.C. The Five-Repetition Sit-to-Stand Test as a Functional Outcome Measure in COPD. Thorax 2013, 68, 1015–1020. [Google Scholar] [CrossRef] [Green Version]
- Vaidya, T.; Chambellan, A.; de Bisschop, C. Sit-to-Stand Tests for COPD: A Literature Review. Respir. Med. 2017, 128, 70–77. [Google Scholar] [CrossRef] [Green Version]
- Morita, A.A.; Bisca, G.W.; Machado, F.V.C.; Hernandes, N.A.; Pitta, F.; Probst, V.S. Best Protocol for the Sit-to-Stand Test in Subjects with Copd. Respir. Care 2018, 63, 1040–1049. [Google Scholar] [CrossRef]
- Chorin, F.; Cornu, C.; Beaune, B.; Frère, J.; Rahmani, A. Sit to Stand in Elderly Fallers vs Non-Fallers: New Insights from Force Platform and Electromyography Data. Aging Clin. Exp. Res. 2016, 28, 871–879. [Google Scholar] [CrossRef]
- Puhan, M.A.; Siebeling, L.; Zoller, M.; Muggensturm, P.; ter Riet, G. Simple Functional Performance Tests and Mortality in COPD. Eur. Respir. J. 2013, 42, 956–963. [Google Scholar] [CrossRef] [Green Version]
- Ozalevli, S.; Ozden, A.; Itil, O.; Akkoclu, A. Comparison of the Sit-to-Stand Test with 6 Min Walk Test in Patients with Chronic Obstructive Pulmonary Disease. Respir. Med. 2007, 101, 286–293. [Google Scholar] [CrossRef] [Green Version]
- Meriem, M.; Cherif, J.; Toujani, S.; Ouahchi, Y.; Hmida, A.B.; Beji, M. Sit-to-Stand Test and 6-Min Walking Test Correlation in Patients with Chronic Obstructive Pulmonary Disease. Ann. Thorac. Med. 2015, 10, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Crook, S.; Büsching, G.; Schultz, K.; Lehbert, N.; Jelusic, D.; Keusch, S.; Wittmann, M.; Schuler, M.; Radtke, T.; Frey, M.; et al. A Multicentre Validation of the 1-Min Sit-to-Stand Test in Patients with COPD. Eur. Respir. J. 2017, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reychler, G.; Boucard, E.; Peran, L.; Pichon, R.; le Ber-Moy, C.; Ouksel, H.; Liistro, G.; Chambellan, A.; Beaumont, M. One Minute Sit-to-Stand Test Is an Alternative to 6MWT to Measure Functional Exercise Performance in COPD Patients. Clin. Respir. J. 2018, 12, 1247–1256. [Google Scholar] [CrossRef] [PubMed]
- Vaidya, T.; de Bisschop, C.; Beaumont, M.; Ouksel, H.; Jean, V.; Dessables, F.; Chambellan, A. Is the 1-Minute Sit-to-Stand Test a Good Tool for the Evaluation of the Impact of Pulmonary Rehabilitation? Determination of the Minimal Important Difference in COPD. Int. J. COPD 2016, 11, 2609–2616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zanini, A.; Aiello, M.; Cherubino, F.; Zampogna, E.; Azzola, A.; Chetta, A.; Spanevello, A. The One Repetition Maximum Test and the Sit-to-Stand Test in the Assessment of a Specific Pulmonary Rehabilitation Program on Peripheral Muscle Strength in COPD Patients. Int. J. COPD 2015, 10, 2423–2430. [Google Scholar] [CrossRef] [Green Version]
- Briand, J.; Behal, H.; Chenivesse, C.; Wémeau-Stervinou, L.; Wallaert, B. The 1-Minute Sit-to-Stand Test to Detect Exercise-Induced Oxygen Desaturation in Patients with Interstitial Lung Disease. Ther. Adv. Respir. Dis. 2018, 12. [Google Scholar] [CrossRef]
- Gruet, M.; Peyré-Tartaruga, L.A.; Mely, L.; Vallier, J.M. The 1-Minute Sit-to-Stand Test in Adults with Cystic Fibrosis: Correlations with Cardiopulmonary Exercise Test, 6-Minute Walk Test, and Quadriceps Strength. Respir. Care 2016, 61, 1620–1628. [Google Scholar] [CrossRef] [Green Version]
- Muza, S.R.; Silverman, M.T.; Gilmore, G.C.; Hellerstein, H.K.; Kelsen, S.G. Comparison of Scales Used to Quantitate the Sense of Effort to Breathe in Patients with Chronic Obstructive Pulmonary Disease. Am. Rev. Respir. Dis. 1990, 141, 909–913. [Google Scholar] [CrossRef]
- Waatevik, M.; Johannessen, A.; Hardie, J.A.; Bjordal, J.M.; Aukrust, P.; Bakke, P.S.; Eagan, T.M.L. Different COPD Disease Characteristics Are Related to Different Outcomes in the 6-Minute Walk Test. COPD J. Chronic Obstr. Pulm. Dis. 2012, 9, 227–234. [Google Scholar] [CrossRef]
- Golpe, R.; Pérez-de-Llano, L.A.; Méndez-Marote, L.; Veres-Racamonde, A. Prognostic Value of Walk Distance, Work, Oxygen Saturation, and Dyspnea during 6-Minute Walk Test in COPD Patients. Respir. Care 2013, 58, 1329–1334. [Google Scholar] [CrossRef] [Green Version]
- Casanova, C.; Cote, C.; Marin, J.M.; Pinto-Plata, V.; de Torres, J.P.; Aguirre-Jaíme, A.; Vassaux, C.; Celli, B.R. Distance and Oxygen Desaturation during the 6-Min Walk Test as Predictors of Long-Term Mortality in Patients with COPD. Chest 2008, 134, 746–752. [Google Scholar] [CrossRef] [PubMed]
- Gálvez-Barrón, C.; Villar-Álvarez, F.; Ribas, J.; Formiga, F.; Chivite, D.; Boixeda, R.; Iborra, C.; Rodríguez-Molinero, A. Effort Oxygen Saturation and Effort Heart Rate to Detect Exacerbations of Chronic Obstructive Pulmonary Disease or Congestive Heart Failure. J. Clin. Med. 2019, 8, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strassmann, A.; Steurer-Stey, C.; Lana, K.D.; Zoller, M.; Turk, A.J.; Suter, P.; Puhan, M.A. Population-Based Reference Values for the 1-Min Sit-to-Stand Test. Int. J. Public Health 2013, 58, 949–953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernandes, N.A.; Wouters, E.F.M.; Meijer, K.; Annegarn, J.; Pitta, F.; Spruit, M.A. Reproducibility of 6-minute walking test in patients with COPD. Eur. Respir. J. 2011, 38, 261–267. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | M/n | SD/% | Minimum | Maximum |
|---|---|---|---|---|
| Male gender | 26 | 86.7 | -- | -- |
| Smoking status Former smoker | smoker | non-smoker | 15|13|2 | 50.0|43.3|6.7 | -- | -- |
| Age (years) | 67.57 | 9.10 | 48 | 83 |
| Body mass index (BMI) (kg/m2) | 25.17 | 4.98 | 15.05 | 36.05 |
| mMRC dyspnea scale | 1.60 | 0.81 | 0 | 3 |
| BODE index | 2.70 | 1.75 | 0 | 6 |
| Forced vital capacity (FVC) (liters (L)) | 2.51 | 0.76 | 1.42 | 4.56 |
| Forced vital capacity (% predicted) | 73.05 | 15.31 | 48.00 | 107.00 |
| Forced expiratory volume in 1st second (FEV1) (L) | 1.41 | 0.52 | 0.60 | 2.78 |
| Forced expiratory volume in 1st second (% predicted) | 50.83 | 14.49 | 24.70 | 78.00 |
| Residual volume (RV) (L) | 4.47 | 1.43 | 2.66 | 9.31 |
| Residual volume (% predicted) | 191.87 | 58.32 | 106.00 | 354.00 |
| Total lung capacity (TLC) (L) | 7.09 | 1.77 | 4.87 | 12.59 |
| Total lung capacity (% predicted) | 116.37 | 19.97 | 78.90 | 172.00 |
| Diffusing capacity for carbon monoxide (DLCO) (% predicted) | 45.14 | 20.47 | 15.00 | 100.00 |
| Arterial partial pressure of oxygen (PaO2) (mmHg) | 69.80 | 13.80 | 34.00 | 91.00 |
| Arterial partial pressure of carbon dioxide (PaCO2) (mmHg) | 44.36 | 7.47 | 33.00 | 64.00 |
| 6-minute walking distance (6MWD) (meters) | 409.37 | 103.23 | 240.00 | 630.00 |
| Percentage of 6MWD (%) Baseline SpO2 6MWT (%) Minimum SpO2 6MWT (%) | 84.23 94.47 86.47 | 20.65 2.60 6.55 | 52.00 88.00 68.00 | 134.00 99.00 96.00 |
| Number of repetitions during 1STST (1STSTr) Baseline SpO2 1STST (%) SpO2 minimum 1STST (%) | 18.13 94.67 89.73 | 5.46 2.58 5.01 | 9.00 89.00 77.00 | 34.00 99.00 98.00 |
| Variable | Test | Baseline | Maximum Minimum | End | After 3 min | Variance Analysis | ||
|---|---|---|---|---|---|---|---|---|
| Evolution | Test | Interaction | ||||||
| sBP & | 6MWT | 129.93 (13.38) | -- | 160.17 (21.93) | 136.20 (17.72) | p < 0.001 * | p = 0.179 | p = 0.005 * |
| STST | 130.17 (17.38) | -- | 154.17 (23.77) | 136.33 (20.16) | ||||
| dBP & | 6MWT | 71.87 (9.70) | -- | 79.67 (10.68) | 76.27 (10.64) | p < 0.001 * | p = 0.941 | p = 0.182 |
| STST | 74.87 (11.80) | -- | 78.37 (10.68) | 74.83 (10.54) | ||||
| HR & | 6MWT | 81.03 (14.24) | 109.80 (14.24) | 104.03 (16.04) | 87.00 (12.66) | p < 0.001 * | p = 0.007 * | p = 0.126 |
| STST | 80.87 (13.69) | 105.60 (15.09) | 96.13 (14.36) | 82.60 (12.60) | ||||
| SpO2 & | 6MWT | 94.47 (2.60) | 86.47 (6.55) | 90.00 (6.80) | 94.03 (2.91) | p < 0.001 * | p = 0.020 * | p = 0.148 |
| STST | 94.67 (2.58) | 89.73 (5.01) | 90.10 (5.42) | 95.03 (2.81) | ||||
| Borg Dyspnea # | 6MWT | 1.27 (0.91) | -- | 3.33 (2.06) | -- | p < 0.001 * | p = 0.095 | p = 0.103 |
| STST | 1.23 (0.97) | -- | 2.90 (1.77) | -- | ||||
| Borg Limbs # | 6MWT | 1.27 (0.87) | -- | 3.23 (1.89) | -- | p < 0.001 * | p = 0.668 | p = 0.238 |
| STST | 1.00 (0.83) | -- | 3.30 (1.64) | -- | ||||
| Variable | Baseline | Minimum | Maximum | End | After 3 min |
|---|---|---|---|---|---|
| sBP | 0.780 | - | - | 0.870 | 0.866 |
| dBP | 0.739 | - | - | 0.754 | 0.340 |
| HR | 0.891 | - | 0.665 | 0.484 | 0.789 |
| SpO2 | 0.833 | 0.810 | - | 0.506 | 0.764 |
| Borg dyspnea | 0.942 | - | - | 0.750 | - |
| Borg limbs | 0.669 | - | - | 0.555 | - |
| Variables | ∆SpO2 ≥ 4% (1STST) | Agreement Analysis | |
|---|---|---|---|
| ∆SpO2 ≥ 4% (6MWT) | No | Yes | % total agreement = 73.3% (p = 0.018) Cohen’s kappa = 0.38 |
| No | 4 (13.3%) | 0 (0%) | |
| Yes | 8 (26.7%) | 18 (60.0%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernandes, A.L.; Neves, I.; Luís, G.; Camilo, Z.; Cabrita, B.; Dias, S.; Ferreira, J.; Simão, P. Is the 1-Minute Sit-To-Stand Test a Good Tool to Evaluate Exertional Oxygen Desaturation in Chronic Obstructive Pulmonary Disease? Diagnostics 2021, 11, 159. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11020159
Fernandes AL, Neves I, Luís G, Camilo Z, Cabrita B, Dias S, Ferreira J, Simão P. Is the 1-Minute Sit-To-Stand Test a Good Tool to Evaluate Exertional Oxygen Desaturation in Chronic Obstructive Pulmonary Disease? Diagnostics. 2021; 11(2):159. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11020159
Chicago/Turabian StyleFernandes, Ana L., Inês Neves, Graciete Luís, Zita Camilo, Bruno Cabrita, Sara Dias, Jorge Ferreira, and Paula Simão. 2021. "Is the 1-Minute Sit-To-Stand Test a Good Tool to Evaluate Exertional Oxygen Desaturation in Chronic Obstructive Pulmonary Disease?" Diagnostics 11, no. 2: 159. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11020159