
Can the Determination of HE4 and CA125 Markers Affect the Treatment of Patients with Endometrial Cancer?

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Characteristics
2.2. Biochemical Analysis of HE4 and CA125
2.3. Statistical Analysis
3. Results
3.1. Correlation between HE4, CA125 and Prognostic Factors
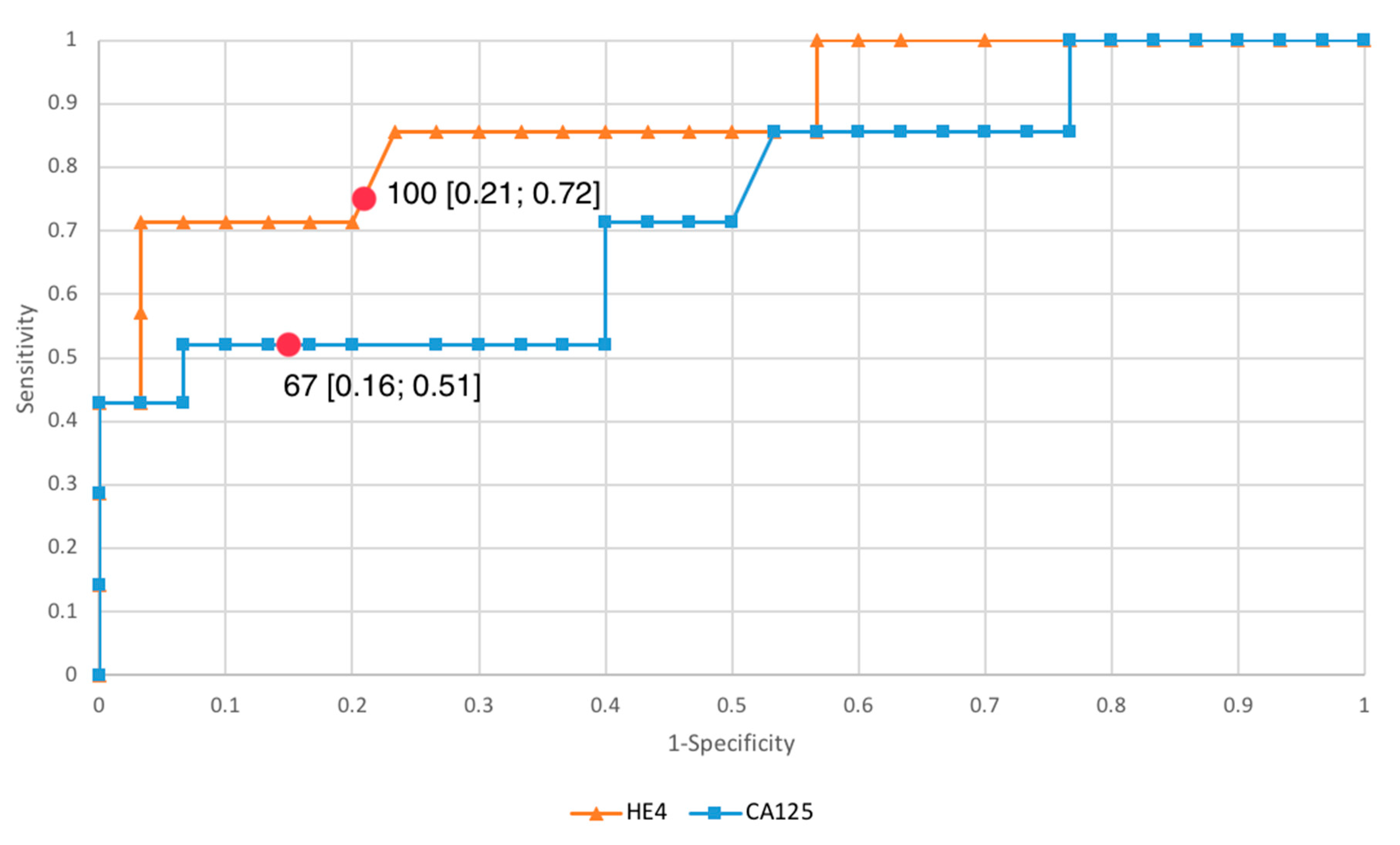
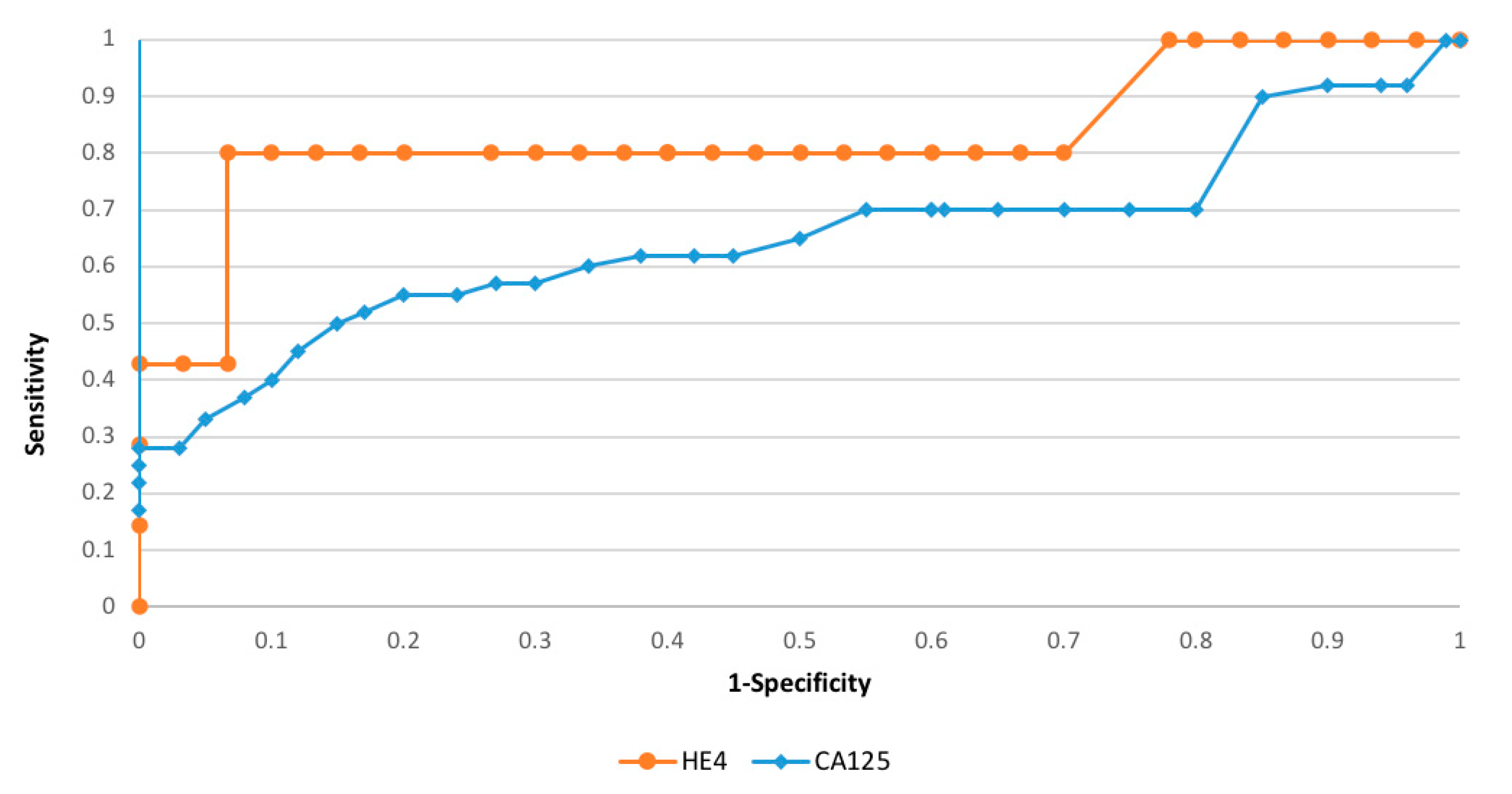
3.2. Evaluation of HE4 and CA125 as Diagnostic Tests
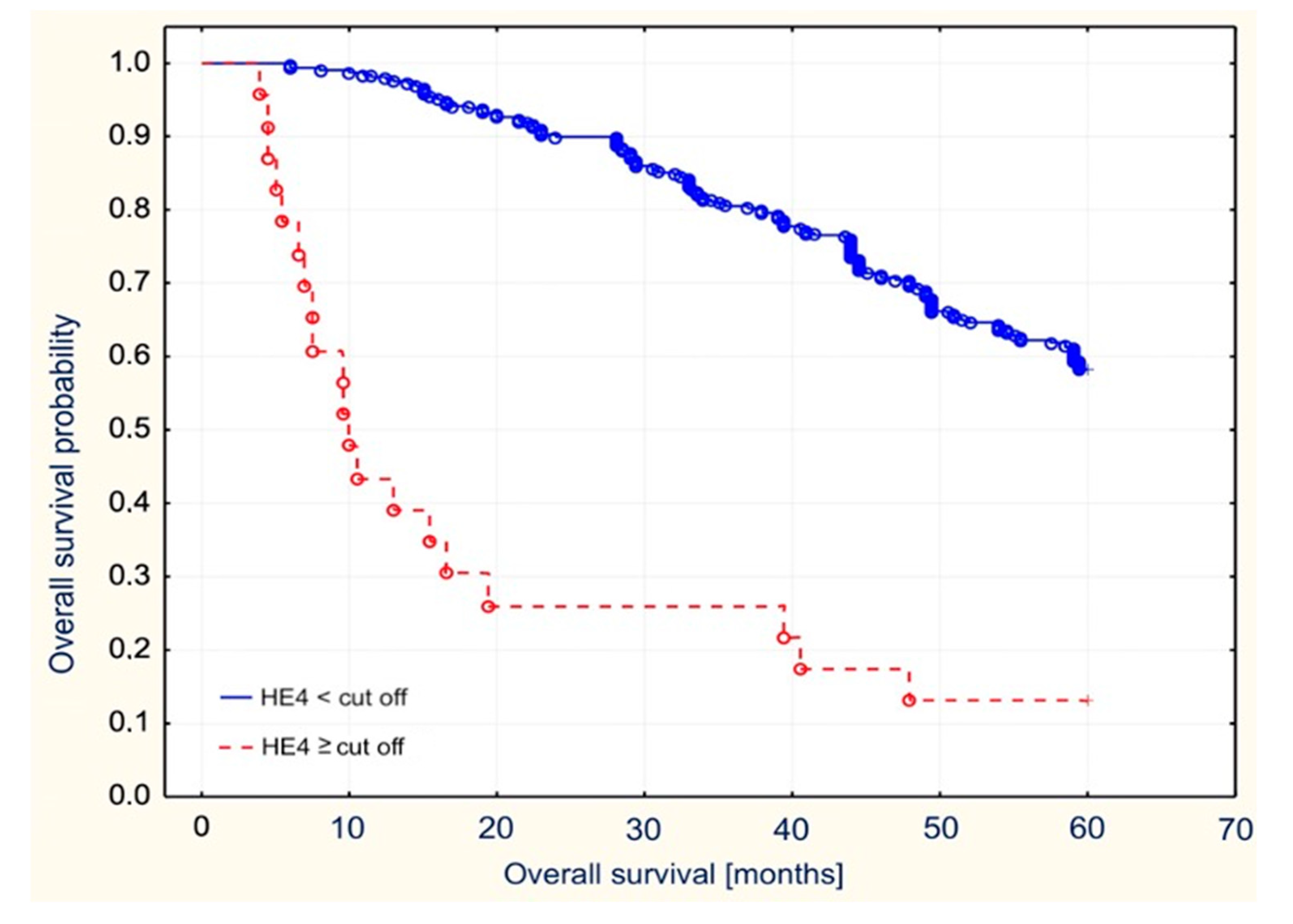
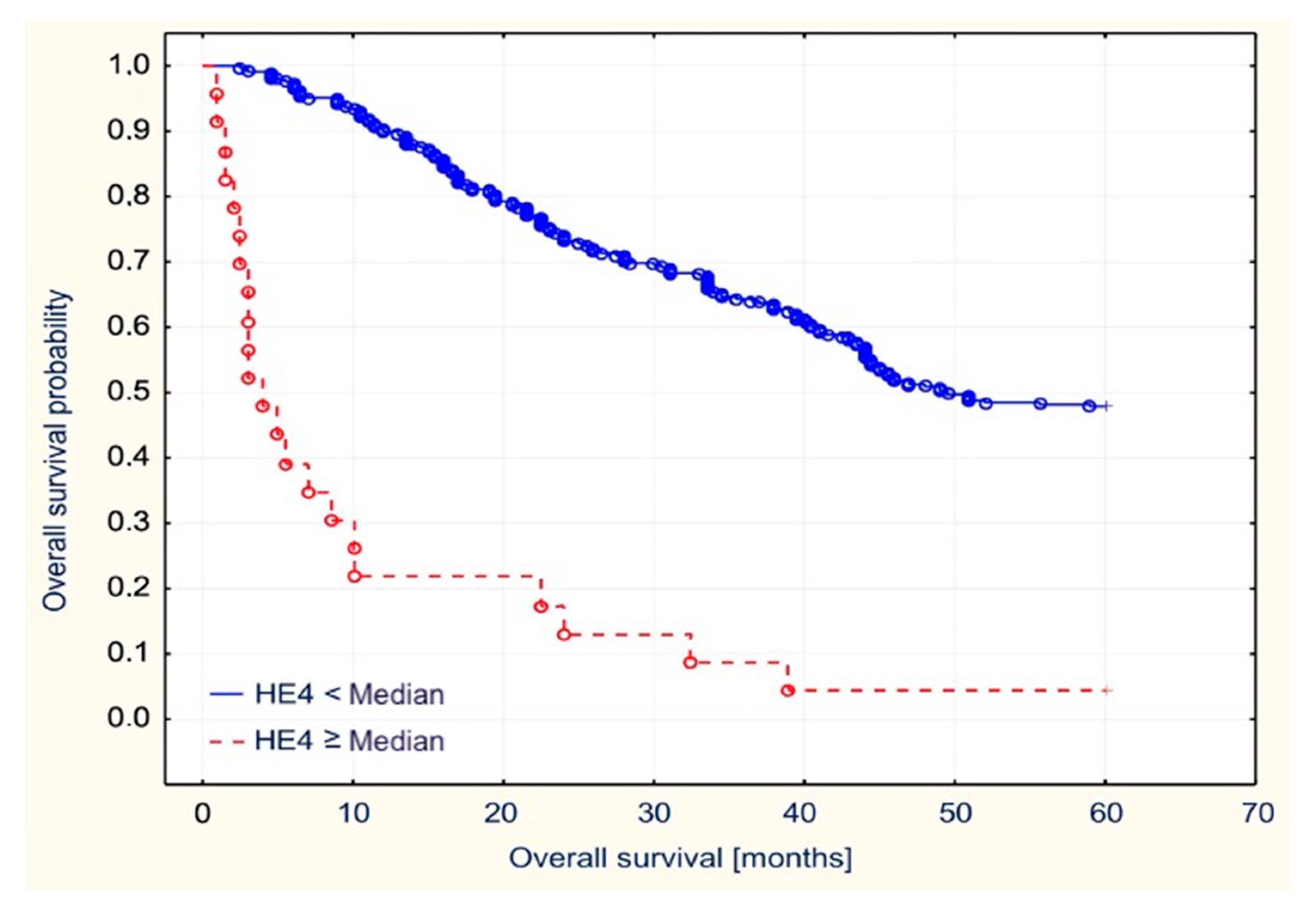
3.3. Survival Analysis Using the Kaplan–Meier Curves and Cox Proportional Hazard Regression
3.4. Univariate and Multivariate Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Dyba, T.; Randi, G.; Bettio, M.; Gavin, A.; Visser, O.; Bray, F. Cancer Incidence and Mortality Patterns in Europe: Estimates for 40 Countries and 25 Major Cancers in 2018. Eur. J. Cancer 2018, 103, 356–387. [Google Scholar] [CrossRef]
- Tejerizo-García, A.; Jiménez-López, J.S.; Muñoz-González, J.L.; Bartolomé-Sotillos, S.; Marqueta-Marqués, L.; López-González, G.; Gómez, J.F.P.-R. Overall Survival and Disease-Free Survival in Endometrial Cancer: Prognostic Factors in 276 Patients. OncoTargets Ther. 2013, 9, 1305–1313. [Google Scholar] [CrossRef] [Green Version]
- Gottwald, L.; Pluta, P.; Piekarski, J.; Spych, M.; Hendzel, K.; Topczewska-Tylinska, K.; Nejc, D.; Bibik, R.; Korczyński, J.; Ciałkowska-Rysz, A. Long-Term Survival of Endometrioid Endometrial Cancer Patients. Arch. Med. Sci. 2010, 6, 937–944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdalla, N.; Piórkowski, R.; Stanirowski, P.; Słomka, A.; Cendrowski, K.; Sawicki, W. Assessment of Levels of the Tumor Markers HE4 and CA125 Considering Staging, Grading and Histological Types of Endometrial Cancer. Menopausal Rev. 2016, 3, 133–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zamani, N.; Modares Gilani, M.; Mirmohammadkhani, M.; Sheikhhasani, S.; Mousavi, A.; Yousefi Sharami, S.R.; Akhavan, S.; Zamani, M.H.; Saffarieh, E. The Utility of CA125 and HE4 in Patients Suffering from Endometrial Cancer. Int. J. Women’s Health Reprod. Sci. 2019, 8, 95–100. [Google Scholar] [CrossRef]
- Chudecka-Głaz, A.; Cymbaluk-Płoska, A.; Wężowska, M. Could HE4 Level Measurements during First-Line Chemotherapy Predict Response to Treatment among Ovarian Cancer Patients? PLoS ONE 2018, 13, e0194270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zanotti, L.; Bignotti, E.; Calza, S.; Bandiera, E.; Ruggeri, G.; Galli, C.; Tognon, G.; Ragnoli, M.; Romani, C.; Tassi, R.A.; et al. Human Epididymis Protein 4 as a Serum Marker for Diagnosis of Endometrial Carcinoma and Prediction of Clinical Outcome. Clin. Chem. Lab. Med. 2012, 50, 2189–2198. [Google Scholar] [CrossRef]
- Angioli, R.; Miranda, A.; Aloisi, A.; Montera, R.; Capriglione, S.; De Cicco Nardone, C.; Terranova, C.; Plotti, F. A Critical Review on HE4 Performance in Endometrial Cancer: Where Are We Now? Tumor Biol. 2014, 35, 881–887. [Google Scholar] [CrossRef]
- Angioli, R.; Plotti, F.; Capriglione, S.; Scaletta, G.; Dugo, N.; Aloisi, A.; Piccolo, C.L.; Del Vescovo, R.; Terranova, C.; Zobel, B.B. Preoperative Local Staging of Endometrial Cancer: The Challenge of Imaging Techniques and Serum Biomarkers. Arch. Gynecol. Obstet. 2016, 294, 1291–1298. [Google Scholar] [CrossRef] [PubMed]
- Angioli, R.; Plotti, F.; Capriglione, S.; Montera, R.; Damiani, P.; Ricciardi, R.; Aloisi, A.; Luvero, D.; Cafà, E.V.; Dugo, N.; et al. The Role of Novel Biomarker HE4 in Endometrial Cancer: A Case Control Prospective Study. Tumor Biol. 2013, 34, 571–576. [Google Scholar] [CrossRef]
- Saarelainen, S.K.; Peltonen, N.; Lehtimäki, T.; Perheentupa, A.; Vuento, M.H.; Mäenpää, J.U. Predictive Value of Serum Human Epididymis Protein 4 and Cancer Antigen 125 Concentrations in Endometrial Carcinoma. Am. J. Obstet. Gynecol. 2013, 209, 142.e1–142.e6. [Google Scholar] [CrossRef]
- Omer, B.; Genc, S.; Takmaz, O.; Dirican, A.; Kusku-Kiraz, Z.; Berkman, S.; Gurdol, F. The Diagnostic Role of Human Epididymis Protein 4 and Serum Amyloid-A in Early-Stage Endometrial Cancer Patients. Tumor Biol. 2013, 34, 2645–2650. [Google Scholar] [CrossRef]
- Kalogera, E.; Scholler, N.; Powless, C.; Weaver, A.; Drapkin, R.; Li, J.; Jiang, S.-W.; Podratz, K.; Urban, N.; Dowdy, S.C. Correlation of Serum HE4 with Tumor Size and Myometrial Invasion in Endometrial Cancer. Gynecol. Oncol. 2012, 124, 270–275. [Google Scholar] [CrossRef] [Green Version]
- Stiekema, A.; Lok, C.; Korse, C.M.; van Driel, W.J.; van der Noort, V.; Kenter, G.G.; Van de Vijver, K.K. Serum HE4 Is Correlated to Prognostic Factors and Survival in Patients with Endometrial Cancer. Virchows Arch. 2017, 470, 655–664. [Google Scholar] [CrossRef]
- Antonsen, S.L.; Jensen, L.N.; Loft, A.; Berthelsen, A.K.; Costa, J.; Tabor, A.; Qvist, I.; Hansen, M.R.; Fisker, R.; Andersen, E.S.; et al. MRI, PET/CT and Ultrasound in the Preoperative Staging of Endometrial Cancer—A Multicenter Prospective Comparative Study. Gynecol. Oncol. 2013, 128, 300–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savelli, L.; Ceccarini, M.; Ludovisi, M.; Fruscella, E.; De Iaco, P.A.; Salizzoni, E.; Mabrouk, M.; Manfredi, R.; Testa, A.C.; Ferrandina, G. Preoperative Local Staging of Endometrial Cancer: Transvaginal Sonography vs. Magnetic Resonance Imaging. Ultrasound Obstet. Gynecol. 2008, 31, 560–566. [Google Scholar] [CrossRef] [PubMed]
- Haldorsen, I.S.; Husby, J.A.; Werner, H.M.J.; Magnussen, I.J.; Rørvik, J.; Helland, H.; Trovik, J.; Salvesen, Ø.O.; Espeland, A.; Salvesen, H.B. Standard 1.5-T MRI of Endometrial Carcinomas: Modest Agreement between Radiologists. Eur. Radiol. 2012, 22, 1601–1611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haldorsen, I.S.; Salvesen, H.B. Staging of Endometrial Carcinomas with MRI Using Traditional and Novel MRI Techniques. Clin. Radiol. 2012, 67, 2–12. [Google Scholar] [CrossRef] [PubMed]
- Husby, J.A.; Salvesen, Ø.O.; Magnussen, I.J.; Trovik, J.; Bjørge, L.; Salvesen, H.B.; Haldorsen, I.S. Tumour Apparent Diffusion Coefficient Is Associated with Depth of Myometrial Invasion and Is Negatively Correlated to Tumour Volume in Endometrial Carcinomas. Clin. Radiol. 2015, 70, 487–494. [Google Scholar] [CrossRef]
- Fischerova, D.; Frühauf, F.; Zikan, M.; Pinkavova, I.; Kocián, R.; Dundr, P.; Nemejcova, K.; Dusek, L.; Cibula, D. Factors Affecting Sonographic Preoperative Local Staging of Endometrial Cancer. Ultrasound Obstet. Gynecol. 2014, 43, 575–585. [Google Scholar] [CrossRef]
- Brennan, D.J.; Hackethal, A.; Mann, K.P.; Mutz-Dehbalaie, I.; Fiegl, H.; Marth, C.; Obermair, A. Serum HE4 Detects Recurrent Endometrial Cancer in Patients Undergoing Routine Clinical Surveillance. BMC Cancer 2015, 15, 33. [Google Scholar] [CrossRef] [Green Version]
- Fanfani, F.; Restaino, S.; Cicogna, S.; Petrillo, M.; Montico, M.; Perrone, E.; Radillo, O.; De Leo, R.; Ceccarello, M.; Scambia, G.; et al. Preoperative Serum Human Epididymis Protein 4 Levels in Early Stage Endometrial Cancer: A Prospective Study. Int. J. Gynecol. Cancer 2017, 27, 1200–1205. [Google Scholar] [CrossRef]
- Capriglione, S.; Plotti, F.; Miranda, A.; Lopez, S.; Scaletta, G.; Moncelli, M.; Luvero, D.; De Cicco Nardone, C.; Terranova, C.; Montera, R.; et al. Further insight into prognostic factors in endometrial cancer: The new serum biomarker HE4. Expert Rev. Anticancer. Ther. 2017, 17, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Plotti, F.; Capriglione, S.; Scaletta, G.; Luvero, D.; Lopez, S.; Nastro, F.F.; Terranova, C.; De Cicco Nardone, C.; Montera, R.; Angioli, R. Implementing the Risk of Endometrial Malignancy Algorithm (REM) Adding Obesity as a Predictive Factor: Results of REM-B in a Single-Center Survey. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 225, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Angioli, R.; Capriglione, S.; Aloisi, A.; Luvero, D.; Cafà, E.V.; Dugo, N.; Montera, R.; De Cicco Nardone, C.; Terranova, C.; Plotti, F. REM (Risk of Endometrial Malignancy): A Proposal for a New Scoring System to Evaluate Risk of Endometrial Malignancy. Clin. Cancer Res. 2013, 19, 5733–5739. [Google Scholar] [CrossRef] [Green Version]
- Angioli, R.; Capriglione, S.; Scaletta, G.; Aloisi, A.; Miranda, A.; De Cicco Nardone, C.; Terranova, C.; Plotti, F. The Role of HE4 in Endometrial Cancer Recurrence: How to Choose the Optimal Follow-up Program. Tumor Biol. 2016, 37, 4973–4978. [Google Scholar] [CrossRef] [PubMed]
- Moore, R.G.; Miller, C.M.; Brown, A.K.; Robison, K.; Steinhoff, M.; Lambert-Messerlian, G. Utility of Tumor Marker HE4 to Predict Depth of Myometrial Invasion in Endometrioid Adenocarcinoma of the Uterus. Int. J. Gynecol. Cancer 2011, 21, 1185–1190. [Google Scholar] [CrossRef] [PubMed]
- Mutz-Dehbalaie, I.; Egle, D.; Fessler, S.; Hubalek, M.; Fiegl, H.; Marth, C.; Widschwendter, A. HE4 Is an Independent Prognostic Marker in Endometrial Cancer Patients. Gynecol. Oncol. 2012, 126, 186–191. [Google Scholar] [CrossRef]
- Cymbaluk-Płoska, A.; Chudecka-Głaz, A.; Pius-Sadowska, E.; Sompolska-Rzechuła, A.; Machaliński, B.; Surowiec, A.; Menkiszak, J. Clinical Importance of Serum HE4 and MMP2 Levels in Endometrial Cancer Patients. OncoTargets Ther. 2017, 10, 3169–3175. [Google Scholar] [CrossRef] [Green Version]
- Bignotti, E.; Ragnoli, M.; Zanotti, L.; Calza, S.; Falchetti, M.; Lonardi, S.; Bergamelli, S.; Bandiera, E.; Tassi, R.A.; Romani, C.; et al. Diagnostic and Prognostic Impact of Serum HE4 Detection in Endometrial Carcinoma Patients. Br. J. Cancer 2011, 104, 1418–1425. [Google Scholar] [CrossRef] [Green Version]
- Abbink, K.; Zusterzeel, P.L.; Geurts-Moespot, A.J.; van Herwaarden, A.E.; Pijnenborg, J.M.; Sweep, F.C.; Massuger, L.F. HE4 Is Superior to CA125 in the Detection of Recurrent Disease in High-Risk Endometrial Cancer Patients. Tumor Biol. 2018, 40, 1010428318757103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dai, C.; Zheng, Y.; Li, Y.; Tian, T.; Wang, M.; Xu, P.; Deng, Y.; Hao, Q.; Wu, Y.; Zhai, Z.; et al. Prognostic Values of HE4 Expression in Patients with Cancer: A Meta-Analysis. Cancer Manag. Res. 2018, 10, 4491–4500. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subgroups | Number of Patients |
|---|---|
| Histopathological type | |
| Type I (endometrial endometrioid adenocarcinoma) | 302 |
| Type II (serous endometrial carcinoma, squamous adenocarcinoma and clear cell carcinoma) | 47 |
| Tumor grading | |
| G1 | 53 |
| G2 | 225 |
| G3 | 71 |
| Clinical staging | |
| FIGO I and II | 287 |
| FIGO III and IV | 62 |
| Myometrial infiltration | |
| Superficial myometrial infiltration (<1/2 of the thickness) | 56 |
| Deep myometrial infiltration (>1/2 of the thickness), | 293 |
| Lymph vessel involvement | |
| Yes | 102 |
| No | 247 |
| Lymph node metastases | |
| Yes | 62 |
| No | 287 |
| Mean HE4 | Median HE4 | p-Value | Mean CA125 | Median CA125 | p-Value | |
|---|---|---|---|---|---|---|
| Histopathological type | NS | NS | ||||
| Type II | 99.6 | 99.7 | 121.2 | 143.6 | ||
| Type I | 43.8 | 44.1 | 48.1 | 51.6 | ||
| Grading | 0.04 | NS | ||||
| G2 | 64.7 | 72.1 | 103.4 | 99.4 | ||
| G1 | 26.7 | 27.4 | 38.5 | 40.0 | ||
| Grading | 0.001 | 0.02 | ||||
| G3 | 64.7 | 72.1 | 166.2 | 199.1 | ||
| G1 | 26.7 | 27.4 | 43.8 | 46.7 | ||
| FIGO staging | 0.001 | 0.003 | ||||
| III and IV | 116.4 | 113.8 | 289.3 | 295.3 | ||
| I and II | 34.8 | 32.3 | 78.2 | 72.9 | ||
| Lymph vessels invasion | 0.007 | NS | ||||
| No | 189.7 | 167.2 | 115.1 | |||
| Yes | 61.2 | 53.5 | 43.9 | |||
| Lymph nodes metastasis | 0.042 | 0.01 | ||||
| No | 208.9 | 214.5 | 132.1 | 141.3 | ||
| Yes | 86.1 | 88.3 | 30.9 | 32.6 | ||
| Myometrium infiltration | 0.001 | 0.02 | ||||
| deep | 121.6 | 118.6 | 247.2 | 233.9 | ||
| superficial | 31.1 | 34.1 | 67.9 | 70.9 |
| FIGO Stage | Patient n | Recurrence Rate % | HE4 Median (pmol/L) | CA125 Median (U/mL) |
|---|---|---|---|---|
| I | 184 | 28.26 | 109.7 | 59.9 |
| II | 103 | 55.33 | 249.6 | 82.3 |
| III | 54 | 75.90 | 301.6 | 92.3 |
| IV | 8 | 87.51 | 333.8 | 161.4 |
| HE4 Median (Range) | CA125 Median (Range) | |||||
|---|---|---|---|---|---|---|
| Recurrence (n = 101) | Recurrence- Free (n = 186) | p-Value | Recurrence (n = 101) | Recurrence-Free (n = 186) | p-Value | |
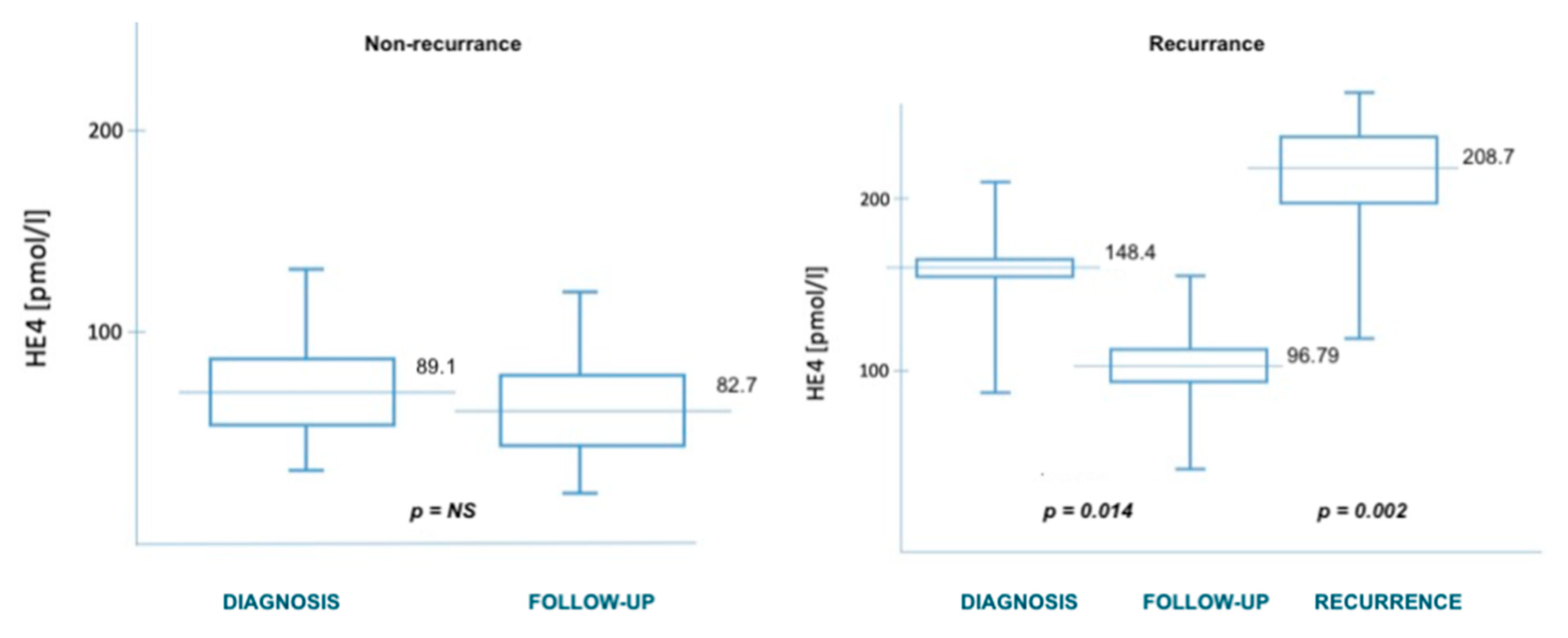
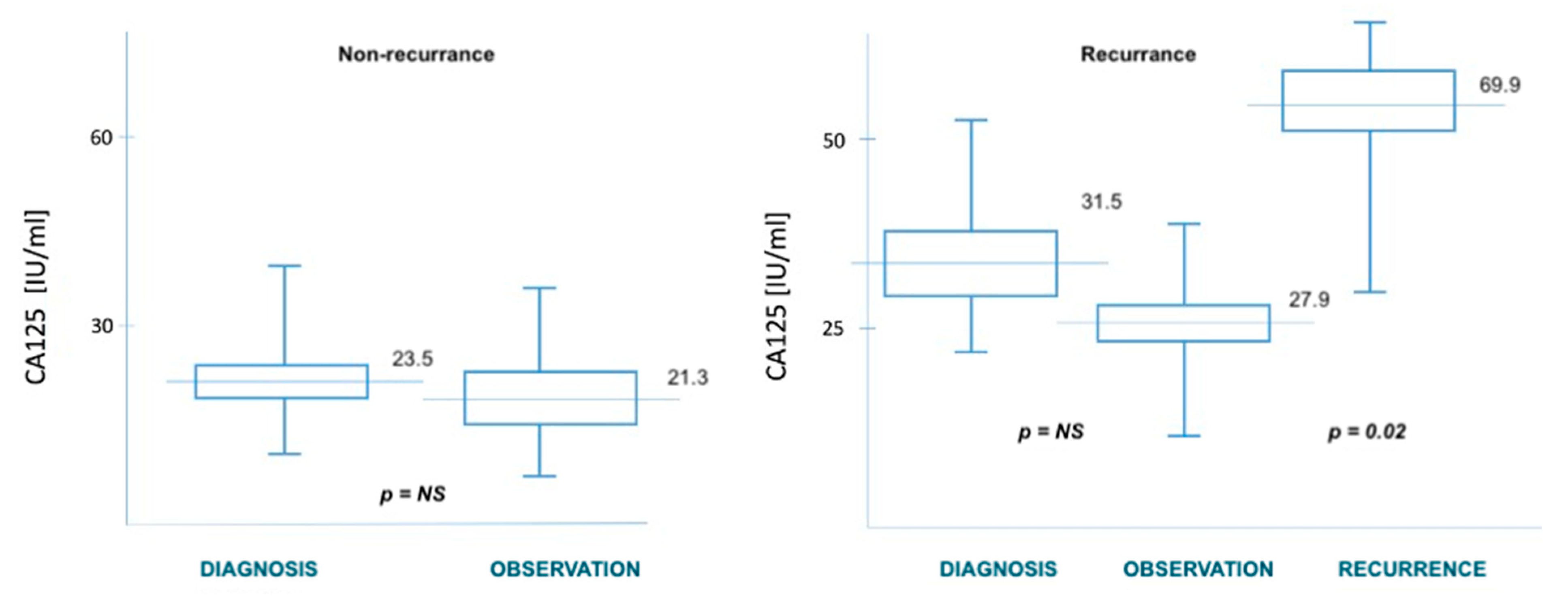
| diagnosis | 92.3 (70.6–101.3) | 55.1 (41.8–69.9) | 0.002 | 31.2 (22.9–42.3) | 23.5 (18.1–29.9) | NS |
| post-surgery | 74.6 (59.9–92.0) | 42.3 (36.2–54.8) | 0.001 | 24.8 (17.2–40.8) | 18.9 (11.8–25.6) | NS |
| observation | 102.7 (82.3–118.6) | 53.1 (40.8–66.2) | 0.001 | 27.9 (20.6–45.2) | 21.3 (14.8–34.5) | 0.048 |
| recurrence | 267.9 (199.1–289.3) | NA | 69.9 (57.9–80.3) | NA | ||
| locoregional recurrence (vaginal, pelvic) | 212.9 (187.5–232.4) | NA | 63.1 (51.6–77.4) | NA | ||
| distant recurrence (lung, bones) | 324.6 (301.7–342.8) | NA | 123.4 (102.2–140.3) | NA | ||
| Univariate Analysis (Cox Regression Model) | ||||||
|---|---|---|---|---|---|---|
| DFS | OS | |||||
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Age | 1.03 | 0.69–1.06 | 0.083 | 1.1 | 0.98–1.13 | 0.04 |
| Stage I, II vs. III, IV | 2.93 | 1.3–3.58 | 0.024 | 2.13 | 1.68–2.27 | 0.003 |
| Grade 1 vs. 3 | 1.31 | 1.1–1.67 | 0.043 | 1.61 | 1.34–2.45 | 0.01 |
| Metastases to lymph node | 2.21 | 1.43–2.98 | 0.002 | 2.02 | 1.57–2.54 | 0.001 |
| HE4 median | 1.96 | 1.52–2.23 | 0.015 | 1.83 | 1.22–2.01 | 0.004 |
| HE4 cut off (70 pmol/L) | 2.08 | 1.78–2.44 | 0.001 | 1.91 | 1.63–2.42 | 0.03 |
| Multivariate Analysis (Cox Regression Model) | ||||||
| DFS | OS | |||||
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| HE4 median | 1.34 | 0.8–1.63 | 0.01 | 1.21 | 0.7–1.71 | 0.003 |
| HE4 75 percentile | 0.98 | 0.56–1.04 | NS | 1.18 | 0.60–1.45 | 0.03 |
| HE4 95 percentile | 1.41 | 1.12–1.76 | 0.04 | 1.62 | 0.74–1.88 | 0.022 |
| HE4 cut off (70 pmol/L) | 2.31 | 1.99–2.76 | 0.01 | 1.89 | 1.08–2.06 | 0.004 |
| Univariate Analysis (Cox Regression Model) | ||||||
| DFS | OS | |||||
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Age | 1.04 | 0.83–1.23 | NS | 1.12 | 0.87–1.71 | 0.043 |
| Stage III, IV vs. I, II | 2.13 | 1.51–2.42 | 0.003 | 2.06 | 1.49–2.22 | 0.014 |
| Grade 1 vs. 3 | 1.41 | 1.20–1.88 | NS | 1.37 | 0.97–1.52 | NS |
| Metastases to lymph node | 1.92 | 1.32–2.24 | 0.045 | 1.76 | 1.35–1.90 | 0.023 |
| CA125 median | 1.76 | 1.41–1.99 | 0.033 | 1.42 | 1.19–1.68 | 0.025 |
| CA125 cut off (35 UI/mL) | 1.82 | 1.52–2.32 | 0.002 | 1.98 | 1.66–2.31 | 0.018 |
| Multivariate Analysis (Cox Regression Model) | ||||||
| DFS | OS | |||||
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| CA125 median | 1.11 | 0.89–1.33 | NS | 1.22 | 0.97–1.49 | 0.024 |
| CA125 75 percentile | 0.98 | 0.77–1.24 | NS | 1.01 | 0.68–1.20 | NS |
| CA125 95 percentile | 1.04 | 0.82–1.30 | 0.012 | 1.13 | 0.79–1.34 | NS |
| CA125 cut off (35 UI/mL) | 1.45 | 1.20–1.63 | 0.026 | 1.38 | 0.81–1.55 | 0.037 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cymbaluk-Płoska, A.; Gargulińska, P.; Bulsa, M.; Kwiatkowski, S.; Chudecka-Głaz, A.; Michalczyk, K. Can the Determination of HE4 and CA125 Markers Affect the Treatment of Patients with Endometrial Cancer? Diagnostics 2021, 11, 626. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11040626
Cymbaluk-Płoska A, Gargulińska P, Bulsa M, Kwiatkowski S, Chudecka-Głaz A, Michalczyk K. Can the Determination of HE4 and CA125 Markers Affect the Treatment of Patients with Endometrial Cancer? Diagnostics. 2021; 11(4):626. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11040626
Chicago/Turabian StyleCymbaluk-Płoska, Aneta, Paula Gargulińska, Michał Bulsa, Sebastian Kwiatkowski, Anita Chudecka-Głaz, and Kaja Michalczyk. 2021. "Can the Determination of HE4 and CA125 Markers Affect the Treatment of Patients with Endometrial Cancer?" Diagnostics 11, no. 4: 626. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11040626