
Pretreatment [18F]FDG PET/CT Prognostic Factors in Patients with Squamous Cell Cervical Carcinoma FIGO IIIC1

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients Characteristic
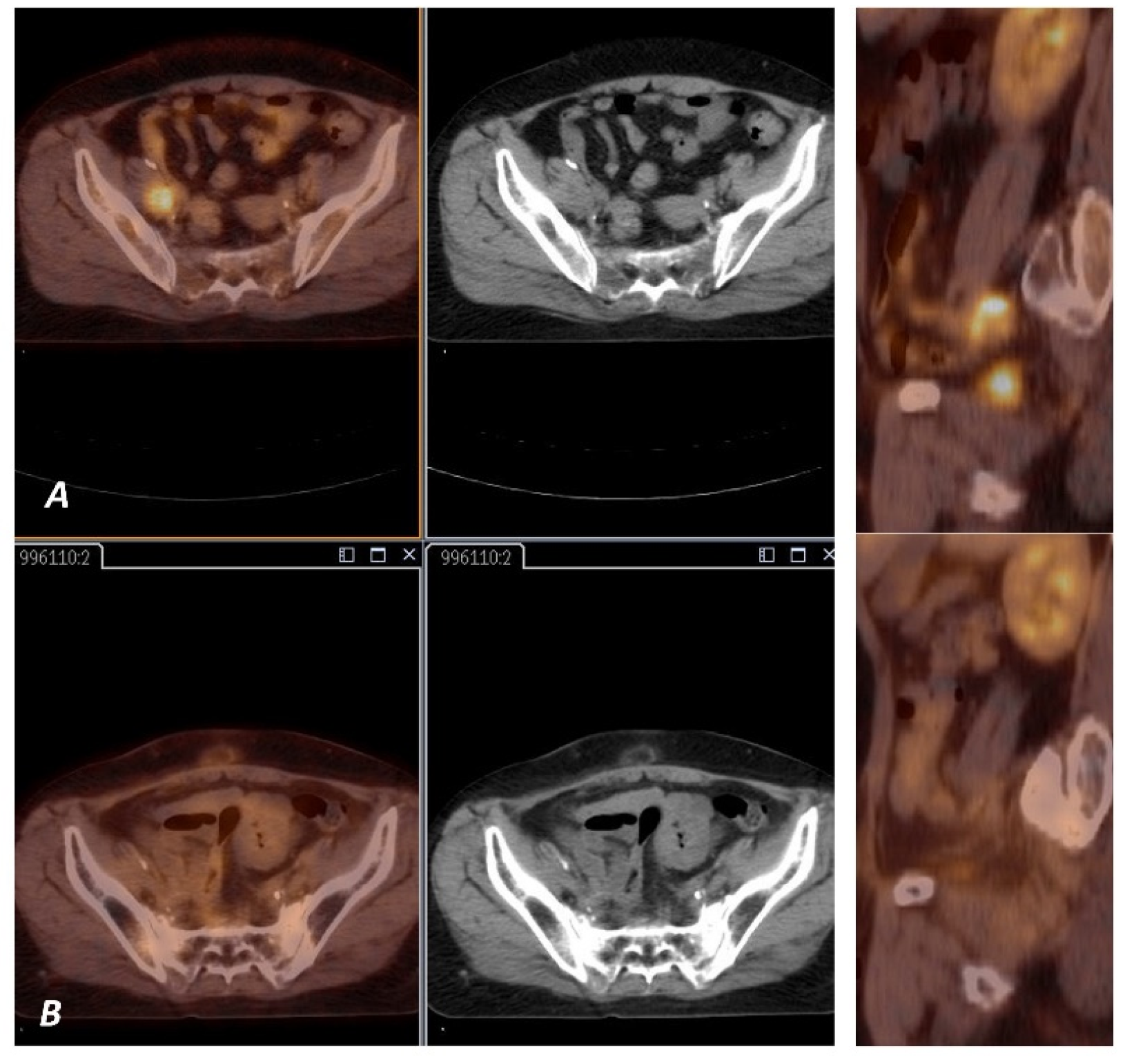
2.2. PET Imaging and Analysis
2.3. Follow-Up
2.4. Statistical Analysis
3. Results
3.1. Overall Survival Analysis
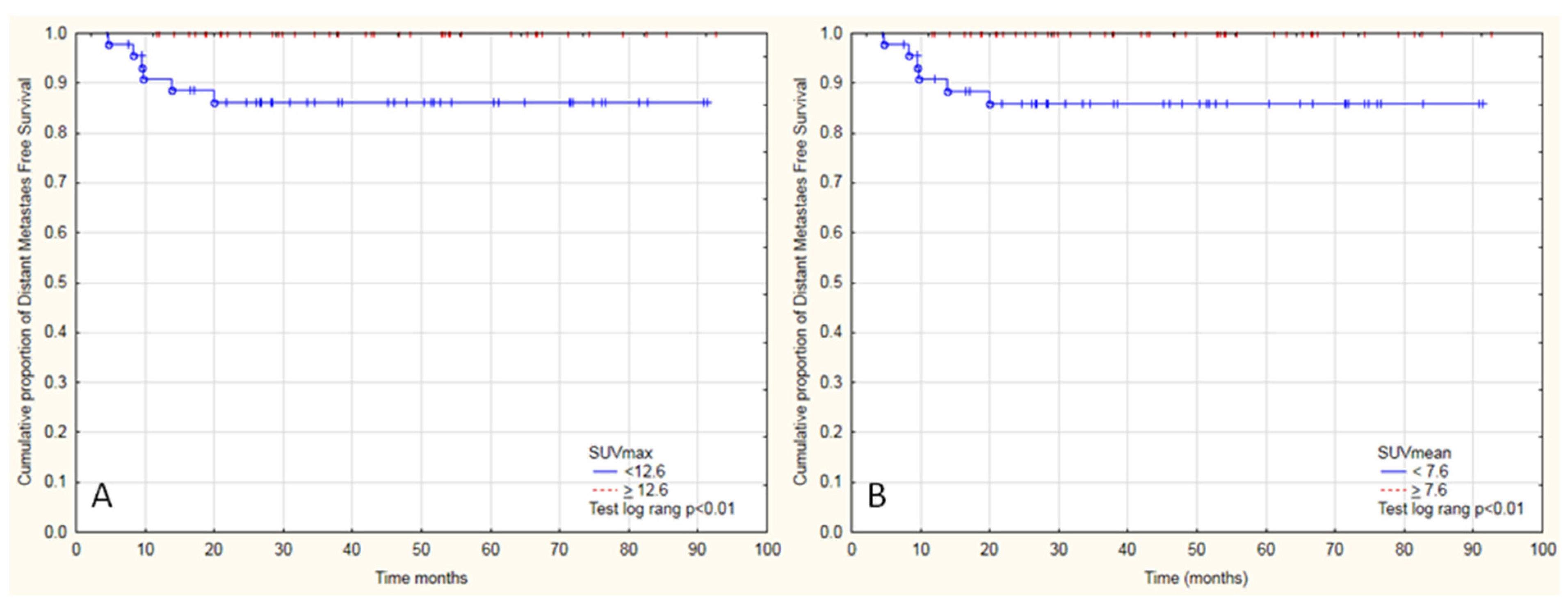
3.2. Distant Metastasis-Free Survival Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Arbyn, M.; Weiderpass, E.; Bruni, L.; de Sanjosé, S.; Saraiya, M.; Ferlay, J.; Bray, F. Estimates of incidence and mortality of cervical cancer in 2018: A worldwide analysis. Lancet Glob. Health 2020, 8, e191–e203. [Google Scholar] [CrossRef] [Green Version]
- Cegła, P.; Burchardt, E.; Wierzchosławska, E.; Roszak, A.; Cholewiński, W. The effect of different segmentation methods on primary tumour metabolic volume assessed in 18F-FDG-PET/CT in patients with cervical cancer, for radiotherapy planning. Wspolczesna Onkol. 2019, 23, 183–186. [Google Scholar] [CrossRef]
- Zhou, J.; Zhang, W.-W.; Wu, S.-G.; He, Z.-Y.; Sun, J.-Y.; Yang, G.-F.; Li, F.-Y. The prognostic value of histologic subtype in node-positive early-stage cervical cancer after hysterectomy and adjuvant radiotherapy. Int. J. Surg. 2017, 44, 1–6. [Google Scholar] [CrossRef]
- Fujiwara, K.; Monk, B.; Devouassoux-Shisheboran, M. Adenocarcinoma of the Uterine Cervix: Why is it different? Curr. Oncol. Rep. 2014, 16, 416. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.L.-Y.; Huang, C.-Y.; Huang, Y.-S.; Chen, R.-J.; Wang, C.-W.; Chen, Y.-H.; Cheng, J.C.-H.; Cheng, A.-L.; Kuo, S.-H. Differential clinical characteristics, treatment response and prognosis of locally advanced adenocarcinoma/adenosquamous carcinoma and squamous cell carcinoma of cervix treated with definitive radiotherapy. Acta Obstet. Gynecol. Scand. 2014, 93, 661–668. [Google Scholar] [CrossRef] [PubMed]
- Galic, V.; Herzog, T.J.; Lewin, S.N.; Neugut, A.I.; Burke, W.M.; Lu, Y.-S.; Hershman, D.L.; Wright, J.D. Prognostic significance of adenocarcinoma histology in women with cervical cancer. Gynecol. Oncol. 2012, 125, 287–291. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.-T.; Wang, C.-C.; Tsai, C.-S.; Lai, C.-H.; Chang, T.-C.; Chou, H.-H.; Lee, S.P.; Hong, J.-H. Clinical Behaviors and Outcomes for Adenocarcinoma or Adenosquamous Carcinoma of Cervix Treated by Radical Hysterectomy and Adjuvant Radiotherapy or Chemoradiotherapy. Int. J. Radiat. Oncol. 2012, 84, 420–427. [Google Scholar] [CrossRef]
- Lai, C.-H.; Hsueh, S.; Hong, J.-H.; Chang, T.-C.; Tseng, C.-J.; Chou, H.-H.; Huang, K.-G.; Lin, J.-D. Are adenocarcinomas and adenosquamous carcinomas different from squamous carcinomas in stage IB and II cervical cancer patients undergoing primary radical surgery? Int. J. Gynecol. Cancer 1999, 9, 28–36. [Google Scholar] [CrossRef]
- Park, J.-Y.; Kim, D.-Y.; Kim, J.-H.; Kim, Y.-M.; Nam, J.-H.; Kim, Y.-T. Outcomes after radical hysterectomy in patients with early-stage adenocarcinoma of uterine cervix. Br. J. Cancer 2010, 102, 1692–1698. [Google Scholar] [CrossRef]
- Schiffman, M.H.; Hildesheim, A. Cervical Cancer. Cancer Epidemiol. Prev. 1996, 2, 1090–1116. [Google Scholar] [CrossRef]
- Kidd, E.A.; Spencer, C.R.; Huettner, P.C.; Siegel, B.A.; Dehdashti, F.; Rader, J.S.; Grigsby, P.W. Cervical cancer histology and tumor differentiation affect18F-fluorodeoxyglucose uptake. Cancer 2009, 115, 3548–3554. [Google Scholar] [CrossRef] [PubMed]
- Kidd, E.A.; El Naqa, I.; Siegel, B.A.; Dehdashti, F.; Grigsby, P.W. FDG-PET-based prognostic nomograms for locally advanced cervical cancer. Gynecol. Oncol. 2012, 127, 136–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voglimacci, M.; Gabiache, E.; Lusque, A.; Ferron, G.; Ducassou, A.; Querleu, D.; Motton, S.; Chantalat, E.; Courbon, F.; Martinez, A. Chemoradiotherapy for locally advanced cervix cancer without aortic lymph node involvement: Can we consider metabolic parameters of pretherapeutic FDG-PET/CT for treatment tailoring? Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1551–1559. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.; Choi, J.Y.; Moon, S.H.; Bae, D.S.; Park, S.B.; Choe, Y.S.; Lee, K.H.; Kim, B.T. Prognostic significance of volume-based metabolic parameters in uterine cervical cancer determined using 18F-fluorodeoxyglucose positron emission tomography. Int. J. Gynecol. Cancer. 2012, 22, 1226–1233. [Google Scholar] [CrossRef] [PubMed]
- Höckel, M.; Schlenger, K.; Aral, B.; Mitze, M.; Schäffer, U.; Vaupel, P. Association between Tumor Hypoxia and Malignant Progression in Advanced Cancer of the Uterine Cervix1. Cancer Res. 1996, 56, 4509–4515. [Google Scholar] [PubMed]
- Hompland, T.; Fjeldbo, C.; Lyng, H. Tumor Hypoxia as a Barrier in Cancer Therapy: Why Levels Matter. Cancers 2021, 13, 499. [Google Scholar] [CrossRef] [PubMed]
- Hillestad, T.; Hompland, T.; Fjeldbo, C.S.; Skingen, V.E.; Salberg, U.B.; Aarnes, E.-K.; Nilsen, A.; Lund, K.V.; Evensen, T.S.; Kristensen, G.B.; et al. MRI Distinguishes Tumor Hypoxia Levels of Different Prognostic and Biological Significance in Cervical Cancer. Cancer Res. 2020, 80, 3993–4003. [Google Scholar] [CrossRef] [PubMed]
- Rajendran, J.G.; Krohn, K.A. F-18 Fluoromisonidazole for Imaging Tumor Hypoxia: Imaging the Microenvironment for Personalized Cancer Therapy. Semin. Nucl. Med. 2015, 45, 151–162. [Google Scholar] [CrossRef] [Green Version]
- Stieb, S.; Eleftheriou, A.; Warnock, G.; Guckenberger, M.; Riesterer, O. Longitudinal PET imaging of tumor hypoxia during the course of radiotherapy. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 2201–2217. [Google Scholar] [CrossRef]
- Schlenger, K.; Höckel, M.; Mitze, M.; Schäffer, U.; Weikel, W.; Knapstein, P.G.; Lambert, A. Tumor Vascularity—A Novel Prognostic Factor in Advanced Cervical Carcinoma. Gynecol. Oncol. 1995, 59, 57–66. [Google Scholar] [CrossRef]
- Fjeldbo, C.S.; Hompland, T.; Hillestad, T.; Aarnes, E.-K.; Günther, C.-C.; Kristensen, G.B.; Malinen, E.; Lyng, H. Combining imaging- and gene-based hypoxia biomarkers in cervical cancer improves prediction of chemoradiotherapy failure independent of intratumour heterogeneity. EBioMedicine 2020, 57, 102841. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.H.; Jung, U.S.; Min, K.J.; Lee, J.K.; Kim, S.; Eo, J.S. Prognostic value of total lesion glycolysis measured by 18F-FDG PET/CT in patients with locally advanced cervical cancer. Nucl. Med. Commun. 2016, 37, 843–848. [Google Scholar] [CrossRef] [PubMed]
- Pinho, D.F.; King, B.; Xi, Y.; Albuquerque, K.; Lea, J.; Subramaniam, R.M. Value of Intratumoral Metabolic Heterogeneity and Quantitative18F-FDG PET/CT Parameters in Predicting Prognosis for Patients With Cervical Cancer. Am. J. Roentgenol. 2020, 214, 908–916. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n | % | Average | Median | Min | Max | SD | |
|---|---|---|---|---|---|---|---|
| Age (Years) | 93 | 100.0 | 52.4 | 52.9 | 27.5 | 74.8 | 10.0 |
| BMI | 88 | 94.6 | 26.2 | 25.95 | 12.4 | 37.9 | 5.5 |
| FIGO Stage | |||||||
| IIA | 1 | 1.1 | |||||
| IIB | 39 | 41.9 | |||||
| IIIA | 2 | 2.2 | |||||
| IIIB | 48 | 51.6 | |||||
| IV | 3 | 3.2 | |||||
| Length of Hospitalization (Days) | 93 | 100.0 | 58.1 | 58 | 31 | 90 | 10.6 |
| SCC Grade | |||||||
| G1 | 3 | ||||||
| G2 | 48 | ||||||
| G3 | 19 | ||||||
| n.d. | 23 | ||||||
| Chemotherapy Courses | 93 | 100.0 | 4.2 | 4 | 1 | 7 | 1.2 |
| TD for Elective LN | 93 | 100.0 | 50.0 | 50.4 | 45 | 50.4 | 1.0 |
| TD for Primary | 93 | 100.0 | 47.9 | 50 | 45 | 50.4 | 2.6 |
| Boost with EBRT for LN+ (Gy) | |||||||
| Yes | 49 | 52.6 | 10.1 | 10 | 8 | 19 | 1.6 |
| No | 44 | 47.4 | |||||
| Brachytherapy | 93 | 100.0 | 26.9 | 28 | 14 | 28 | 3.1 |
| Follow-Up | 93 | 100.0 | 43.0 | 38 | 4.5 | 92.6 | 23.6 |
| n | Average | Median | Min | Max | SD | |
|---|---|---|---|---|---|---|
| Activity of FDG (mCi) | 93 | 8.945 | 8.700 | 4.3000 | 13.10 | 1.747 |
| Glucose Level (mg%) | 93 | 90.914 | 88.000 | 56.0000 | 160.00 | 17.454 |
| SUVmax | 93 | 14.133 | 12.890 | 4.5600 | 32.61 | 5.510 |
| SUVmean | 93 | 8.199 | 7.590 | 2.5800 | 17.93 | 3.188 |
| TumorSUV | 93 | 5076.946 | 3869.440 | 652.8600 | 2,6057.90 | 4230.602 |
| TLG | 93 | 322.353 | 245.640 | 26.0300 | 1667.71 | 272.469 |
| MTV | 93 | 37.059 | 34.010 | 7.0000 | 115.25 | 19.791 |
| SUVtotal | 93 | 23.284 | 21.570 | 10.6300 | 45.10 | 8.845 |
| TLGtotal | 93 | 354.185 | 258.840 | 45.5600 | 1769.20 | 309.062 |
| MTVtotal | 93 | 40.414 | 38.750 | 8.0600 | 116.56 | 20.280 |
| SUVLN | 93 | 9.150 | 7.530 | 1.9400 | 26.47 | 5.716 |
| TLGLN | 93 | 31.833 | 7.440 | 0.1000 | 1667.97 | 173.599 |
| MTVLN | 93 | 3.356 | 2.480 | 0.0500 | 12.97 | 2.783 |
| AUC-CSH | 93 | 0.582 | 0.578 | 0.5170 | 0.71 | 0.037 |
| Heterogenity | 93 | 0.268 | 0.271 | 0.1710 | 0.32 | 0.025 |
| PET Parameters | Death | Metastasis | Progression | Local Recurrence | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Hazard Ratio | CI 95% | p Value | Hazard Ratio | CI 95% | p Value | Hazard Ratio | CI 95% | p Value | Hazard Ratio | CI 95% | p Value | |
| SUVmax | 0.89 | 0.81–0.98 | 0.01 | 0.73 | 0.56–0.96 | 0.02 | 0.98 | 0.91–1.06 | 0.57 | 1.03 | 0.94–1.13 | 0.50 |
| SUVmean | 0.81 | 0.69–0.95 | 0.01 | 0.59 | 0.38–0.94 | 0.02 | 0.95 | 0.84–1.09 | 0.47 | 1.04 | 0.89–1.22 | 0.58 |
| TumorSUV | 1.00 | 1–1 | 0.42 | 1.00 | 1–1 | 0.09 | 1.00 | 1–1 | 0.96 | 1.00 | 1–1 | 0.81 |
| TLG * | 0.40 | 0.17–0.92 | 0.03 | 0.18 | 0.02–1.57 | 0.12 | 0.95 | 0.43–2.08 | 0.90 | 1.10 | 0.29–4.09 | 0.89 |
| MTV | 1.00 | 0.99–1.02 | 0.69 | 0.97 | 0.91–1.02 | 0.22 | 1.00 | 0.98–1.02 | 0.78 | 1.00 | 0.98–1.03 | 0.73 |
| SUVtotal | 0.96 | 0.92–1.01 | 0.13 | 0.97 | 0.88–1.07 | 0.54 | 1.00 | 0.96–1.05 | 0.97 | 2.24 | 0.7–7.14 | 0.17 |
| TLGtotal * | 0.47 | 0.21–1.07 | 0.07 | - | - | - | 1.00 | 1–1 | 0.75 | 1.01 | 0.96–1.07 | 0.62 |
| MTVotal | 1.00 | 0.99–1.02 | 0.65 | 0.97 | 0.92–1.02 | 0.26 | 1.00 | 0.98–1.02 | 0.75 | 1.00 | 0.98–1.03 | 0.71 |
| SUVLN | 1.00 | 0.93–1.07 | 0.96 | 1.88 | 0.34–10.28 | 0.47 | 1.02 | 0.96–1.09 | 0.54 | 1.02 | 0.96–1.09 | 0.54 |
| TLGLN * | 1.02 | 0.47–2.25 | 0.95 | 1.08 | 0.96–1.22 | 0.20 | 1.06 | 0.48–2.33 | 0.88 | 0.71 | 0.24–2.04 | 0.52 |
| MTVLN | 1.03 | 0.9–1.18 | 0.65 | 1.06 | 0.82–1.36 | 0.67 | 1.02 | 0.89–1.17 | 0.75 | 1.03 | 0.86–1.23 | 0.75 |
| Heterogeneity ** | 1.05 | 0.89–1.23 | 0.57 | 0.96 | 0.71–1.3 | 0.78 | 1.03 | 0.88–1.2 | 0.73 | 0.99 | 0.81–1.22 | 0.93 |
| Age | 0.99 | 0.95–1.03 | 0.58 | 0.96 | 0.71–1.3 | 0.78 | 1.00 | 0.96–1.04 | 0.90 | 1.00 | 0.95–1.06 | 0.88 |
| FIGO Stage | 1.37 | 0.91–2.05 | 0.13 | 1.03 | 0.48–2.24 | 0.94 | 1.52 | 1–2.32 | 0.05 | 1.55 | 0.58–4.1 | 0.38 |
| Time of Hospitalization | 0.97 | 0.93–1.01 | 0.19 | 0.98 | 0.91–1.06 | 0.64 | 1.00 | 0.96–1.04 | 0.83 | 0.97 | 0.92–1.02 | 0.24 |
| Tumor Grade | 2.19 | 0.97–4.95 | 0.06 | 3.90 | 0.68–22.24 | 0.13 | 1.43 | 0.59–3.46 | 0.43 | 0.70 | 0.19–2.57 | 0.59 |
| Boost to PLN+ | 0.73 | 0.31–1.7 | 0.46 | 1.31 | 0.27–6.52 | 0.74 | 1.48 | 0.58–3.79 | 0.41 | 1.90 | 0.66–5.51 | 0.23 |
| Chemotherapy Courses | 0.92 | 0.66–1.27 | 0.61 | 1.46 | 0.7–3.03 | 0.31 | 0.99 | 0.71–1.38 | 0.96 | 0.76 | 0.5–1.15 | 0.20 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burchardt, E.; Burchardt, W.; Cegła, P.; Kubiak, A.; Roszak, A.; Cholewiński, W. Pretreatment [18F]FDG PET/CT Prognostic Factors in Patients with Squamous Cell Cervical Carcinoma FIGO IIIC1. Diagnostics 2021, 11, 714. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11040714
Burchardt E, Burchardt W, Cegła P, Kubiak A, Roszak A, Cholewiński W. Pretreatment [18F]FDG PET/CT Prognostic Factors in Patients with Squamous Cell Cervical Carcinoma FIGO IIIC1. Diagnostics. 2021; 11(4):714. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11040714
Chicago/Turabian StyleBurchardt, Ewa, Wojciech Burchardt, Paulina Cegła, Anna Kubiak, Andrzej Roszak, and Witold Cholewiński. 2021. "Pretreatment [18F]FDG PET/CT Prognostic Factors in Patients with Squamous Cell Cervical Carcinoma FIGO IIIC1" Diagnostics 11, no. 4: 714. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11040714