
Diagnosis and Management of Rectal Neuroendocrine Tumors (NETs)

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
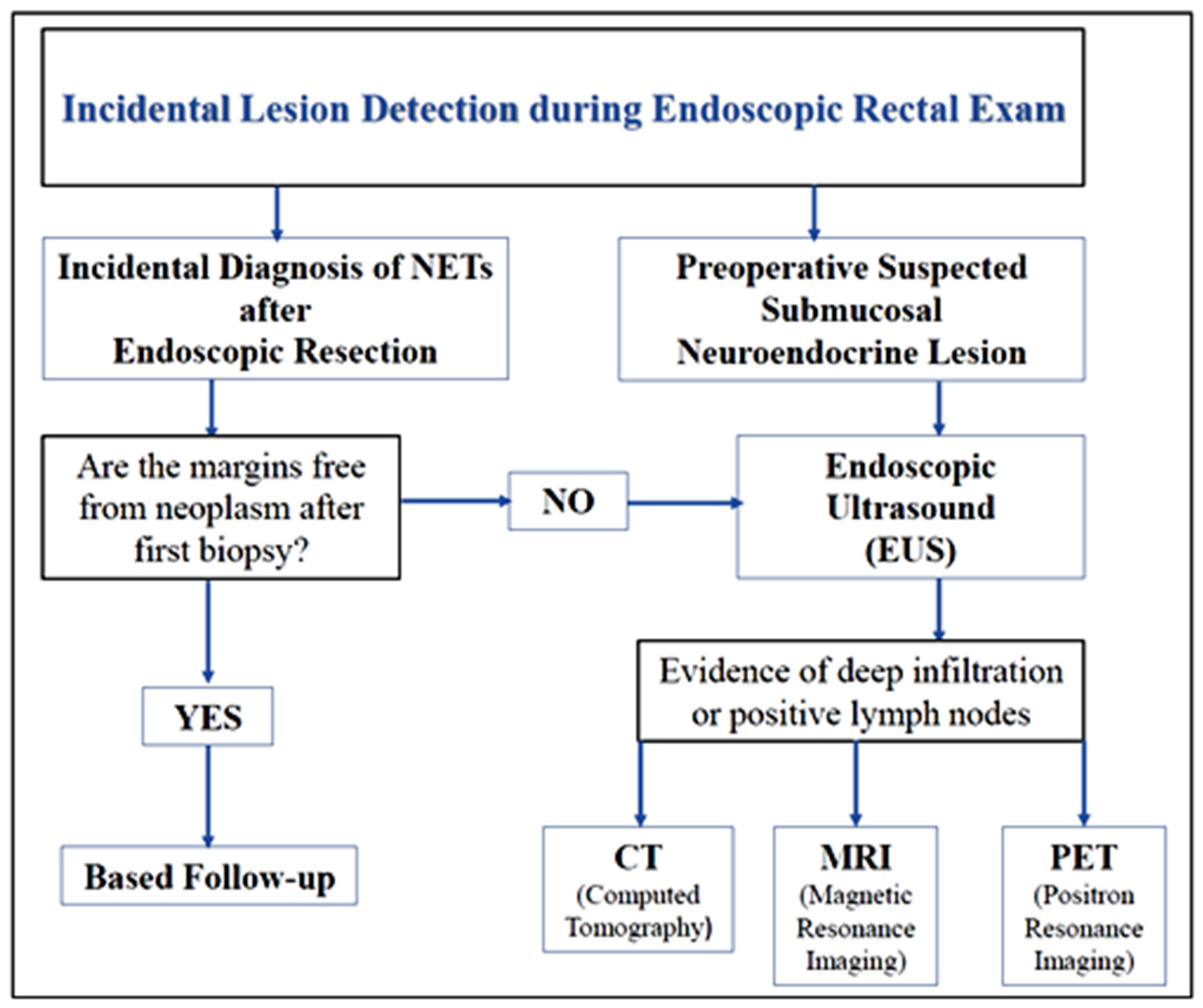
2. Diagnosis of Rectal NETs
3. Prognosis of Rectal NETs
- -
- Low Grade (G1): 2 mitotes/10 HPFs and <2% Ki67 index;
- -
- Intermediate Grade (G2): 2–20 mitotes/10 HPFs and 3–20% Ki67 index;
- -
- High grade (G3): 20 mitotes/10 HPFs and >20% Ki67 index.
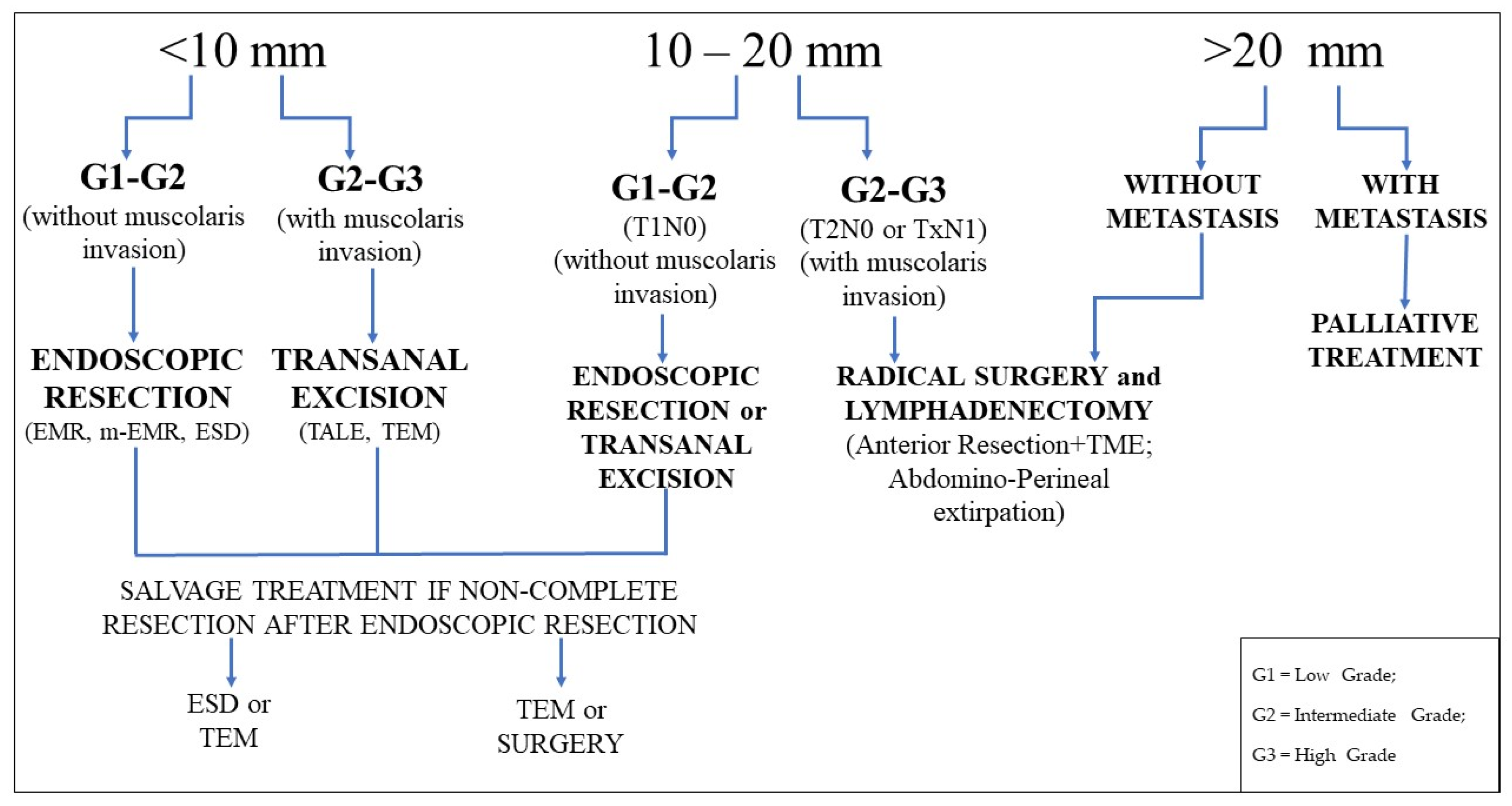
4. Management of Rectal NETs
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Wang, X.Y.; Chai, N.L.; Linghu, E.Q. Efficacy and safety of hybrid endoscopic submucosal dissection compared with endoscopic submucosal dissection for rectal neuroendocrine tumors and risk factors associated with incomplete endoscopic resection. Ann. Transl. Med. 2020, 8, 368. [Google Scholar] [CrossRef]
- Osagiede, O.; Habermann, E.; Day, C. Factors associated with worse outcomes for colorectal neuroendocrine tumors in radical versus local resection. J. Gastrointest. Oncol. 2020, 11, 836–846. [Google Scholar] [CrossRef] [PubMed]
- Modlin, I.M.; Sandor, A. An analysis of 8305 cases of carcinoid tumors. Cancer 1997, 79, 813–829. [Google Scholar] [CrossRef]
- Tsikitis, V.L.; Wertheim, B.C.; Guerrero, M.A. Trends of incidence and survival of gastrointestinal neuroendocrine tumors in the United States: A SEER analysis. J. Cancer 2012, 3, 292–302. [Google Scholar] [CrossRef] [PubMed]
- Basuroy, R.; Haji, A.; Ramage, J.K. Review article: The investigation and management of rectal neuroendocrine tumours. Aliment. Pharmacol. Ther. 2016, 44, 332–345. [Google Scholar] [CrossRef] [PubMed]
- Bang, B.W.; Park, J.S.; Kim, H.K. Endoscopic Resection for Small Rectal Neuroendocrine Tumors: Comparison of Endoscopic Submucosal Resection with Band Ligation and Endoscopic Submucosal Dissection. Gastroenterol. Res. Pract. 2016, 2016, 6198927. [Google Scholar] [CrossRef] [Green Version]
- Wang, A.Y.; Ahmad, N.A. Rectal carcinoids. Curr. Opin. Gastroenterol. 2006, 22, 529–535. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Wu, F.; Zhao, H. Analysis of the factors affecting lymph node metastasis and the prognosis of rectal neuroendocrine tumors. Int. J. Clin. Exp. Pathol. 2015, 8, 13331–13338. [Google Scholar]
- Ko, S.H.; Baeg, M.K.; Ko, S.Y. Clinical characteristics, risk factors and outcomes of asymptomatic rectal neuroendocrine tumors. Surg. Endosc. 2017, 31, 3864–3871. [Google Scholar] [CrossRef]
- Kim, H.H.; Park, S.J.; Lee, S.H. Efficacy of endoscopic submucosal resection with a ligation device for removing small rectal carcinoid tumor compared with endoscopic mucosal resection: Analysis of 100 cases. Dig. Endosc. 2012, 24, 159–163. [Google Scholar] [CrossRef]
- Dąbkowski, K.; Szczepkowski, M.; Kos-Kudła, B. Endoscopic management of rectal neuroendocrine tumours. How to avoid a mistake and what to do when one is made? Endokrynol. Pol. 2020, 71, 343–349. [Google Scholar] [CrossRef]
- Shim, K.N.; Yang, S.K.; Myung, S.J. Atypical endoscopic features of rectal carcinoid tumors. Endoscopy 2004, 36, 313–316. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.N.; Sohn, D. Atypical endoscopic features can be associated with metastasis in rectal carcinoid tumors. Surg. Endosc. 2008, 22, 1992–1996. [Google Scholar] [CrossRef]
- Takeda, K.; Kudo, S.E.; Misawa, M. Endocytoscopic findings of colorectal neuroendocrine tumors (with video). Endosc. Int. Open 2018, 6, E589–E593. [Google Scholar] [CrossRef]
- Son, H.J.; Sohn, D.K.; Hong, C.W. Factors associated with complete local excision of small rectal carcinoid tumor. Int. J. Colorectal Dis. 2013, 28, 57–61. [Google Scholar] [CrossRef]
- Lee, S.P.; Sung, I.; Kim, J.H. The effect of preceding Biopsy on complete endoscopic resection in rectal carcinoid tumor. J. Korean Med. Sci. 2014, 29, 512–518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caplin, M.; Sundin, A.; Nillson, O. ENETS Consensus Guidelines for the Management of Patients with Digestive Neuroendocrine Neoplasms: Colorectal Neuroendocrine Neoplasms. Neuroendocrinology 2012, 95, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Park, S.B.; Kim, D.J.; Kim, H.W. Is endoscopic ultrasonography essential for endoscopic resection of small rectal neuroendocrine tumors? World J. Gastroenterol. 2017, 23, 2037–2043. [Google Scholar] [CrossRef] [Green Version]
- Moon, J.S. Endoscopic ultrasound-guided fine needle aspiration in submucosal lesion. Clin. Endosc. 2012, 45, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.T.; Xu, G.Q.; Teng, X.D. Diagnostic accuracy of endoscopic ultrasonography for rectal neuroendocrine neoplasms. World J. Gastroenterol. 2014, 20, 10470–10477. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, K.; Katsumata, T.; Yoshizawa, S. Indications of endoscopic polypectomy for rectal carcinoid tumors and clinical usefulness of endoscopic Ultrasonography. Dis. Colon. Rectum. 2005, 48, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Wang, Z.; Zhang, Z. Evaluation of colonscopy in the diagnosis and treatment of rectal carcinoid tumors with diameter less than 1 cm in 21 patients. Oncol. Lett. 2013, 5, 1667–1671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cazacu, I.M.; Singh, B.S.; Luzuriaga Chavez, A.A. EUS and EUS-guided FNA/core biopsies in the evaluation of subepithelial lesions of the lower gastrointestinal tract: 10-year experience. Endosc. Ultrasound 2020, 9, 329–336. [Google Scholar]
- Soh, J.S.; Lee, H.S.; Lee, S. The clinical usefulness of endoscopic ultrasound-guided fine needle aspiration and biopsy for rectal and perirectal lesions. Intest. Res. 2015, 13, 135–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawahara, M.; Kammori, M.; Kanauchi, H. Immunohistochemical prognostic indicators of gastrointestinal carcinoid tumors. Eur. J. Surg. Oncol. 2002, 28, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Mohanty, S.K.; Tiwari, A.; Bhardwaj, N. Positivity for SATB2 distinguishes Islet1 positive rectal neuroendocrine tumours from pancreaticoduodenal neuroendocrine tumours. J. Clin. Pathol. 2020, 2020, 206645. [Google Scholar]
- Sappenfield, R.; Gonzalez, I.A.; Cao, D. Well-differentiated rectal neuroendocrine tumors: Analysis of histology, including insulinoma-associated protein 1 expression, and biologic behavior, involving a large cohort of 94 cases. Hum. Pathol. 2020, 104, 66–72. [Google Scholar] [CrossRef]
- Srirajaskanthan, R.; Kayani, I.; Quigley, A.M. The role of 68 Ga-DOTATATE PET in patients with neuroendocrine tumors and negative or equivocal findings on 111In-DTPA-octreotide scintigraphy. J. Nucl. Med. 2010, 51, 875–882. [Google Scholar] [CrossRef] [Green Version]
- Kwaan, R.; Goldberg, J.E.; Bleday, R. Rectal carcinoid tumors: Review of results after endoscopic and surgical therapy. Arch. Surg. 2008, 143, 471–475. [Google Scholar] [CrossRef]
- Jann, H.; Roll, S.; Couvelard, A. Neuroendocrine tumors of midgut and hindgut origin: Tumor-node-metastasis classification determines clinical outcome. Cancer 2011, 117, 3332–3341. [Google Scholar] [CrossRef]
- Park, C.H.; Cheon, J.H.; Kim, J.O. Criteria for decision making after endoscopic resection of well- differentiated rectal carcinoids with regard to potential lymphatic spread. Endoscopy 2011, 43, 790–795. [Google Scholar] [CrossRef]
- Ramage, J.K.; De Herder, W.W.; Delle Fave, G. Vienna Consensus Conference participants. ENETS Consensus Guidelines Update for Colorectal Neuroendocrine Neoplasms. Neuroendocrinology 2016, 103, 139–143. [Google Scholar] [CrossRef] [PubMed]
- He, L.; Deng, T.; Luo, H. Efficacy and safety of endoscopic resection therapies for rectal carcinoid tumors: A meta-analysis. Yonsei Med. J. 2015, 56, 72–81. [Google Scholar] [CrossRef] [PubMed]
- Zhou, P.H.; Yao, L.Q.; Qin, X.Y. Advantages of endoscopic submucosal dissection with needle-knife over endoscopic mucosal resection for small rectal carcinoid tumors: A retrospective study. Surg. Endosc. 2010, 24, 2607–2612. [Google Scholar] [CrossRef]
- Lee, J.; Park, Y.E.; Choi, J.H. Comparison between cap-assisted and ligation-assisted endoscopic mucosal resection for rectal neuroendocrine tumors. Ann. Gastroenterol. 2020, 33, 385–390. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Xie, H.; Xie, L. Endoscopic resection therapies for rectal neuroendocrine tumors: A systematic review and meta-analysis. J. Gastroenterol. Hepatol. 2014, 29, 259–268. [Google Scholar] [CrossRef]
- Lee, W.H.; Kim, S.W.; Lim, C.H. Efficacy of endoscopic mucosal resection using a dual-channel endoscope compared with endoscopic submucosal dissection in the treatment of rectal neuroendocrine tumors. Surg. Endosc. 2013, 27, 4313–4318. [Google Scholar] [CrossRef]
- So, H.; Yoo, S.H.; Han, S. Efficacy of Precut Endoscopic Mucosal Resection for Treatment of Rectal Neuroendocrine Tumors. Clin. Endosc. 2017, 50, 585–591. [Google Scholar] [CrossRef] [Green Version]
- Huang, J.; Lu, Z.S.; Yang, Y.S. Endoscopic mucosal resection with circumferential incision for treatment of rectal carcinoid tumours. World J. Surg. Oncol. 2014, 12, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheung, D.Y.; Choi, S.K.; Kim, H.K. Circumferential submucosal incision prior to endoscopic mucosal resection provides comparable clinical outcomes to submucosal dissection for well-differentiated neuroendocrine tumors of the rectum. Surg. Endosc. 2015, 29, 1500–1505. [Google Scholar] [CrossRef]
- Lee, H.J.; Kim, S.B.; Shin, C.M. A comparison of endoscopic treatments in rectal carcinoid tumors. Surg. Endosc. 2016, 30, 3491–3498. [Google Scholar] [CrossRef]
- Niimi, K.; Goto, O.; Fujishiro, M. Endoscopic mucosal resection with a ligation device or endoscopic submucosal dissection for rectal carcinoid tumours: An analysis of 24 consecutive cases. Dig. Endosc. 2012, 24, 443–447. [Google Scholar] [CrossRef] [PubMed]
- Oshitani, N.; Hamasaki, N.; Sawa, Y. Endoscopic resection of small rectal carcinoid tumours using an aspiration method with a transparent overcap. J. Int. Med. Res. 2000, 28, 241–246. [Google Scholar] [CrossRef] [Green Version]
- Park, S.B.; Kim, H.W.; Kang, D.H. Advantage of endoscopic mucosal resection with a cap for rectal neuroendocrine tumors. World J. Gastroenterol. 2015, 21, 9387–9393. [Google Scholar] [CrossRef]
- Mashimo, Y.; Matsuda, T.; Uraoka, T. Endoscopic submucosal resection with a ligation device is an effective and safe treatment for carcinoid tumors in the lower rectum. J. Gastroenterol. Hepatol. 2008, 23, 218–221. [Google Scholar] [CrossRef] [PubMed]
- Maione, F.; Chini, A.; Aprea, G. Indication and results of endoscopic submucosal dissection (ESD) for right located lateral spreading tumors (LST). Ann. Laparosc. Endosc. Surg. 2020, 3, 2518. [Google Scholar]
- Park, H.W.; Byeon, J.S.; Park, Y.S. Endoscopic submucosal dissection for treatment of rectal carcinoid tumors. Gastrointest Endosc. 2010, 72, 143–149. [Google Scholar] [CrossRef]
- Onozato, Y.; Kakizaki, S.; Iizuka, H. Endoscopic Treatment of Rectal Carcinoid Tumors. Dis. Colon Rectum. 2010, 53, 169–176. [Google Scholar] [CrossRef]
- Lee, D.S.; Jeon, S.W.; Park, S.Y. The feasibility of endoscopic submucosal dissection for rectal carcinoid tumors: Comparison with endoscopic mucosal resection. Endoscopy 2010, 42, 647–651. [Google Scholar] [CrossRef]
- Yan, F.H.; Lou, Z.; Hu, S.J. Endoscopic submucosal dissection versus transanal local excision for rectal carcinoid: A comparative study. World J. Surg. Oncol. 2016, 14, 162. [Google Scholar] [CrossRef] [Green Version]
- Kinoshita, T.; Kanehira, E.; Omura, K. Transanal endoscopic microsurgery in the treatment of rectal carcinoid tumor. Surg. Endosc. 2007, 21, 970–974. [Google Scholar] [CrossRef]
- de Mestier, L.; Lorenzo, D.; Fine, C. Endoscopic, transanal, laparoscopic, and transabdominal management of rectal neuroendocrine tumors. Best Pract. Res. Clin. Endocrinol. Metab. 2019, 33, 101293. [Google Scholar] [CrossRef]
- Chen, W.J.; Wu, N.; Zhou, J.L. Full thickness excision using transanal endoscopic microsurgery for treatment of rectal neuroendocrine tumors. World J. Gastroenterol. 2015, 21, 9142–9149. [Google Scholar] [CrossRef] [PubMed]
- Moore, J.S.; Cataldo, P.A.; Osler, T. Transanal endoscopic microsurgery is more effective than traditional excision for resection of rectal masses. Dis. Colon. Rectum. 2008, 51, 1026–1030. [Google Scholar] [CrossRef] [PubMed]
- McCarty, T.R.; Bazarbashi, A.N.; Hathorn, K.E. Endoscopic submucosal dissection (ESD) versus transanal endoscopic microsurgery (TEM) for treatment of rectal tumors: A comparative systematic review and meta-analysis. Surg. Endosc. 2020, 34, 1688–1695. [Google Scholar] [CrossRef] [PubMed]
- Ortenzi, M.; Ghiselli, R.; Trombettoni, M.M. Transanal endoscopic microsurgery as optimal option in treatment of rare rectal lesions: A single centre experience. World J. Gastrointest Endosc. 2016, 8, 623–627. [Google Scholar] [CrossRef]
- Brand, M.; Reimer, S.; Reibetanz, J.; Flemming, S.; Kornmann, M.; Meining, A. Endoscopic full thickness resection vs. transanal endoscopic microsurgery for local treatment of rectal neuroendocrine tumors—A retrospective analysis. Int. J. Colorectal Dis. 2021, 36, 971–976. [Google Scholar] [CrossRef]
- Meier, B.; Albrecht, H.; Wiedbrauck, T. Full-thickness resection of neuroendocrine tumors in the rectum. Endoscopy 2020, 52, 68–72. [Google Scholar] [CrossRef]
- Takatsu, Y.; Fukunaga, Y.; Nagasaki, T. Short- and long-term outcomes of laparoscopic total mesenteric excision for neuroendocrine tumors of the rectum. Dis. Colon. Rectum. 2017, 60, 284–289. [Google Scholar] [CrossRef]
- Sung, H.Y.; Kim, S.W.; Kang, W.K. Long-term prognosis of an endoscopically treated rectal neuroendocrine tumor:10-year experience in a single institution. Eur. J. Gastroenterol. Hepatol. 2012, 24, 978–983. [Google Scholar] [CrossRef]
- Cha, J.H.; Jung, D.H.; Kim, J.H. Long-term outcomes according to additional treatments after endoscopic resection for rectal small neuroendocrine tumors. Sci. Rep. 2019, 9, 4911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, H.S.; Kwon, M.J.; Kim, T.H. Lymphovascular invasion as a prognostic value in small rectal neuroendocrine tumor treated by local excision: A systematic review and meta-analysis. Pathol. Res. Pract. 2019, 215, 152642. [Google Scholar] [CrossRef] [PubMed]
- Moon, C.M.; Huh, K.C.; Jung, S.A. Long-Term Clinical Outcomes of Rectal Neuroendocrine Tumors According to the Pathologic Status after Initial Endoscopic Resection: A KASID Multicenter Study. Am. J. Gastroenterol. 2016, 111, 1276–1285. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Grading | Mitotic Count | Ki67 Index | |
|---|---|---|---|
| G1 (Low Grade) | <2 mitotes/10 HPFs | and | <2% Ki67 Index |
| G2 (Intermediate Grade) | 2–20 mitotes/10 HPFs | or | 3–20% Ki67 Index |
| G3 (High Grade) | >20 mitotes/10 HPFs | or | >20% Ki67 Index |
| T Stage | T Description | N/M Stage | N and M Description |
|---|---|---|---|
| TX | Primary tumour cannot be assessed | Nx | Lymph node status not detected |
| T0 | No evidence of primary tumour metastasis | N0 | Absence of Lymph Node |
| T1 | Tumour 2 cm or less, that invades lamina propria or submucosa | N1 | Regional Lymph node metastasis |
| T1a | Tumour <1 cm | ||
| T1b | Tumour 1–2 cm | ||
| T2 | Tumour >2 cm or that invades muscolaris propria | Mx | Distant metastasis not detected |
| T3 | Tumour that invades the subserosa or perirectal tissues | M0 | No distant metastasis |
| T4 | Tumour that invades peritoneum or other organs | M1 | Presence of Distant metastasis |
| Study | Year | Treatment | EN Bloc Resection Rate % (No.) | Histologic Complete Resection Rate % (No.) | Procedure Time Mean ± SD (Min) |
|---|---|---|---|---|---|
| OSHITANI et al. [43] | 2000 | EMR-C | 85.7% (6/7) | NR | NR |
| MASHIMO et al. [45] | 2008 | EMR-L | 95.2% (60/63) | NR | NR |
| ZHOU et al. [34] | 2010 | EMR ESD | 87% (20/23) 100% (20/20) | 52.2% (12/20) 100% (20/20) | 12.3 ± 15.4 28.4 ± 17.2 |
| PARK HW et al. [47] | 2010 | EMR ESD | 95.2% (59/62) 100% (31/31) | 71% (44/62) 90.3% (28/31) | 4.2 ± 3.2 11.4 ± 3.7 |
| ONOZATO et al. [48] | 2010 | Polipectomy EMR-D ESD | NR NR NR | 20% (1/5) 84.6% (22/26) 77.8% (7/9) | NR 9.3 ± 2.2 25.6 ± 8.8 |
| LEE DS et al. [49] | 2010 | EMR ESD | 89.3% (25/28) 100% (46/46) | 64.3% (18/28) 82.6% (38/46) | 12.0 ± 12.9 18.9 ± 7.3 |
| KIM et al. [10] | 2012 | ESMR-L EMR | 100% (45/45) 91% (50/55) | 93.3% (42/45) 65.5% (36/55) | 4.8 ± 0.9 5.0 ± 0.8 |
| NIIMI et al. [42] | 2012 | EMR-L ESD | 100% (11/11) 100% (26/26) | 100% (11/11) 92.3% (12/13) | 17.4 ± 4.4 28.6 ± 16.2 |
| LEE WH et al. [37] | 2013 | EMR-D ESD | 100% (44/44) 100% (26/26) | 86.3% (38/44) 88.4% (23/26) | 9.75 ± 7.11 22.38 ± 7.56 |
| HUANG et al. [39] | 2014 | CIEMR EMR | 100% (31/31) 96.5% (27/28) | 96.7% (30/31) 82.14% (23/28) | 7.6 4.2 |
| CHEUNG et al. [40] | 2014 | CSI-EMR ESD | 87.5% (14/16) 100% (17/17) | 81.2% (13/16) 88.2% (15/17) | 9.69 ± 3.61 20.2 ± 12.6 |
| PARK SB et al. [44] | 2015 | EMR-C ESD | 100% (65/65) 100% (51/51) | 92.3% (60/65) 78.4% (40/51) | 3.83 ± 1.17 14.43 ± 7.26 |
| BANG et al. [6] | 2016 | ESMR-L ESD | 100% (53/53) 100% (24/24) | 100% (53/53) 88.2% (13/24) | 5.3 ± 2.8 17.9 ± 9.1 |
| LEE HJ et al. [41] | 2016 | EMR-P EMR Strip Biopsy | 95.5% (64/68) 97.8% (45/47) 98.7% (74/75) | 69.4% (47/68) 51.1% (24/47) 82.7% (62/75) | 7.4 ± 4.9 5.6 ± 5.2 6.5 ± 3.9 |
| SO et al. [38] | 2017 | EMR-P | 98.6% (71/72) | 93.1% (67/72) | 5.5 ±2.5 |
| LEE J et al. [35] | 2020 | EMR-C EMR-L | 92.9% (39/42) 100% (120/120) | 83.3% (35/42) 92.5% (120/120) | 5.5 ± 2.5 5.5 ± 2.9 |
| WANG et al. [1] | 2020 | ESD Hybrid ESD | 98.2% (161/167) 99.2% (118/119) | 90.9% (149/164 94.1% (112/119) | 18.1 ± 9.7 13.2 ± 8.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maione, F.; Chini, A.; Milone, M.; Gennarelli, N.; Manigrasso, M.; Maione, R.; Cassese, G.; Pagano, G.; Tropeano, F.P.; Luglio, G.; et al. Diagnosis and Management of Rectal Neuroendocrine Tumors (NETs). Diagnostics 2021, 11, 771. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11050771
Maione F, Chini A, Milone M, Gennarelli N, Manigrasso M, Maione R, Cassese G, Pagano G, Tropeano FP, Luglio G, et al. Diagnosis and Management of Rectal Neuroendocrine Tumors (NETs). Diagnostics. 2021; 11(5):771. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11050771
Chicago/Turabian StyleMaione, Francesco, Alessia Chini, Marco Milone, Nicola Gennarelli, Michele Manigrasso, Rosa Maione, Gianluca Cassese, Gianluca Pagano, Francesca Paola Tropeano, Gaetano Luglio, and et al. 2021. "Diagnosis and Management of Rectal Neuroendocrine Tumors (NETs)" Diagnostics 11, no. 5: 771. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11050771