
Serum and Urine Biomarker Leucine-Rich Alpha-2 Glycoprotein 1 Differentiates Pediatric Acute Complicated and Uncomplicated Appendicitis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Study Population
2.3. Study Protocol
2.4. Serum LRG1 Collection and Analysis
2.5. Urine LRG-1 Collection and Analysis
2.6. Statistical Analysis
3. Results
3.1. Clinical Characteristics of the Study Population
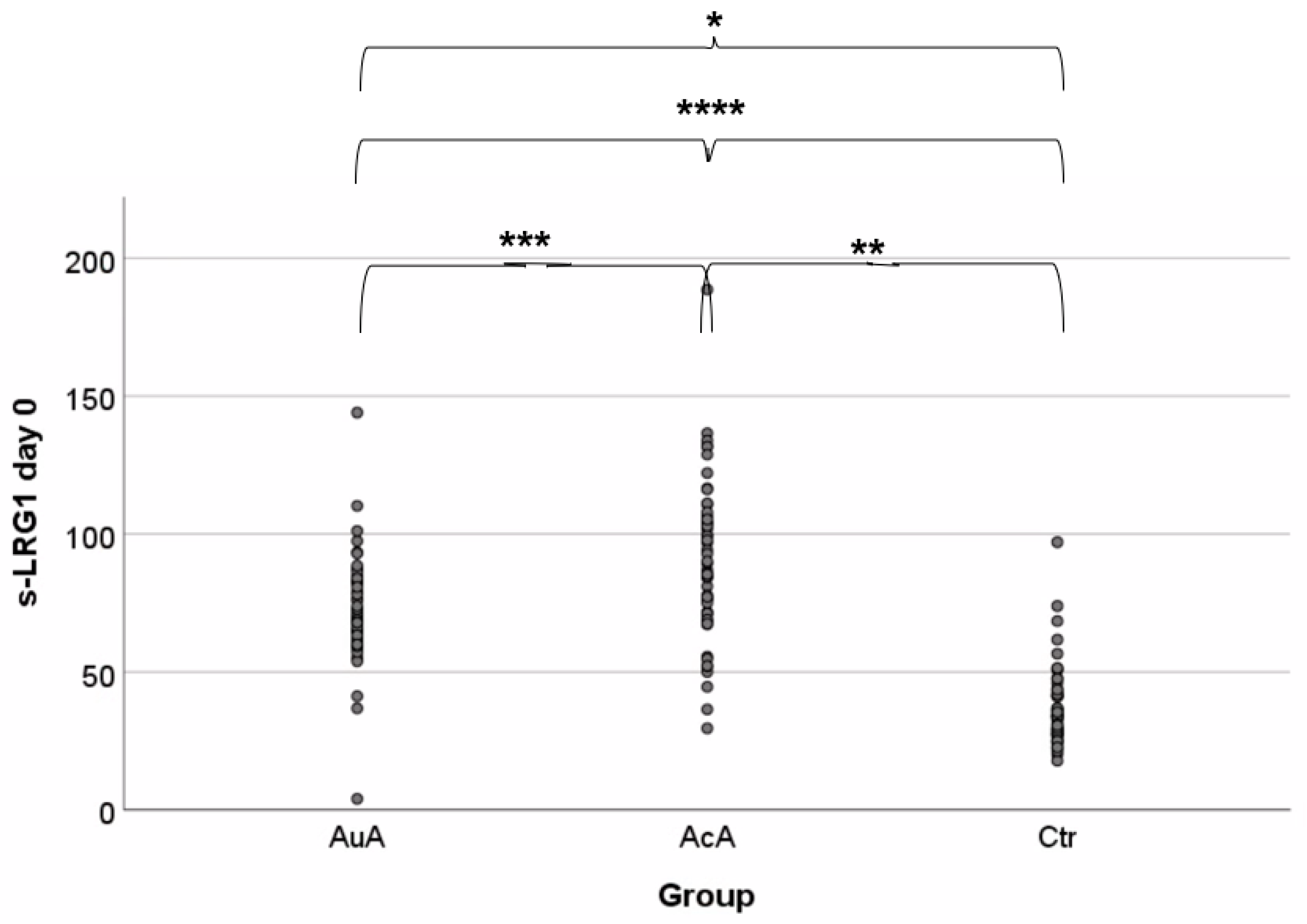
3.2. Serum Leucine-Rich Alpha Glycoprotein-1 Levels
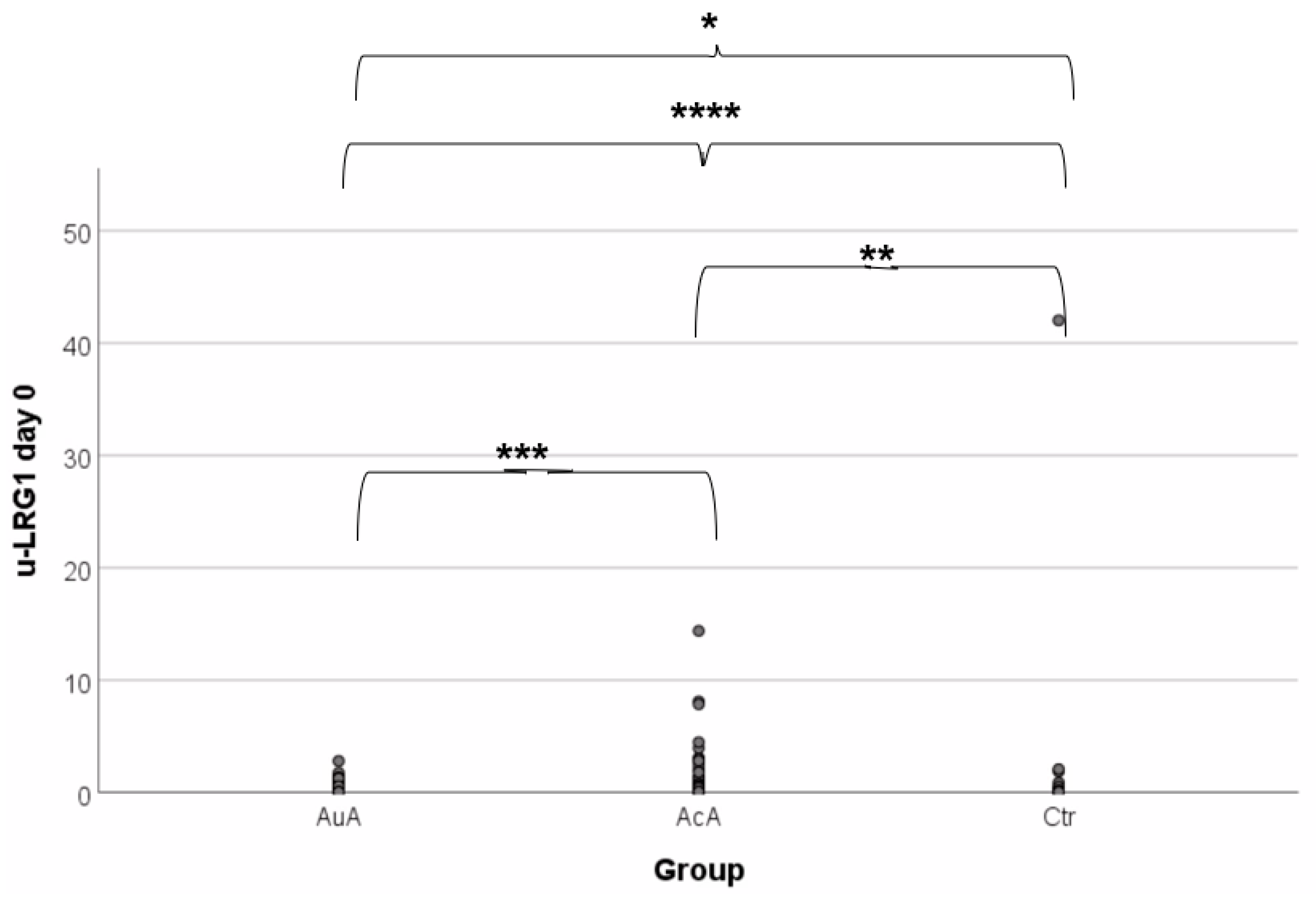
3.3. Urine Leucine-Rich Alpha-2 Glycoprotein-1 Levels
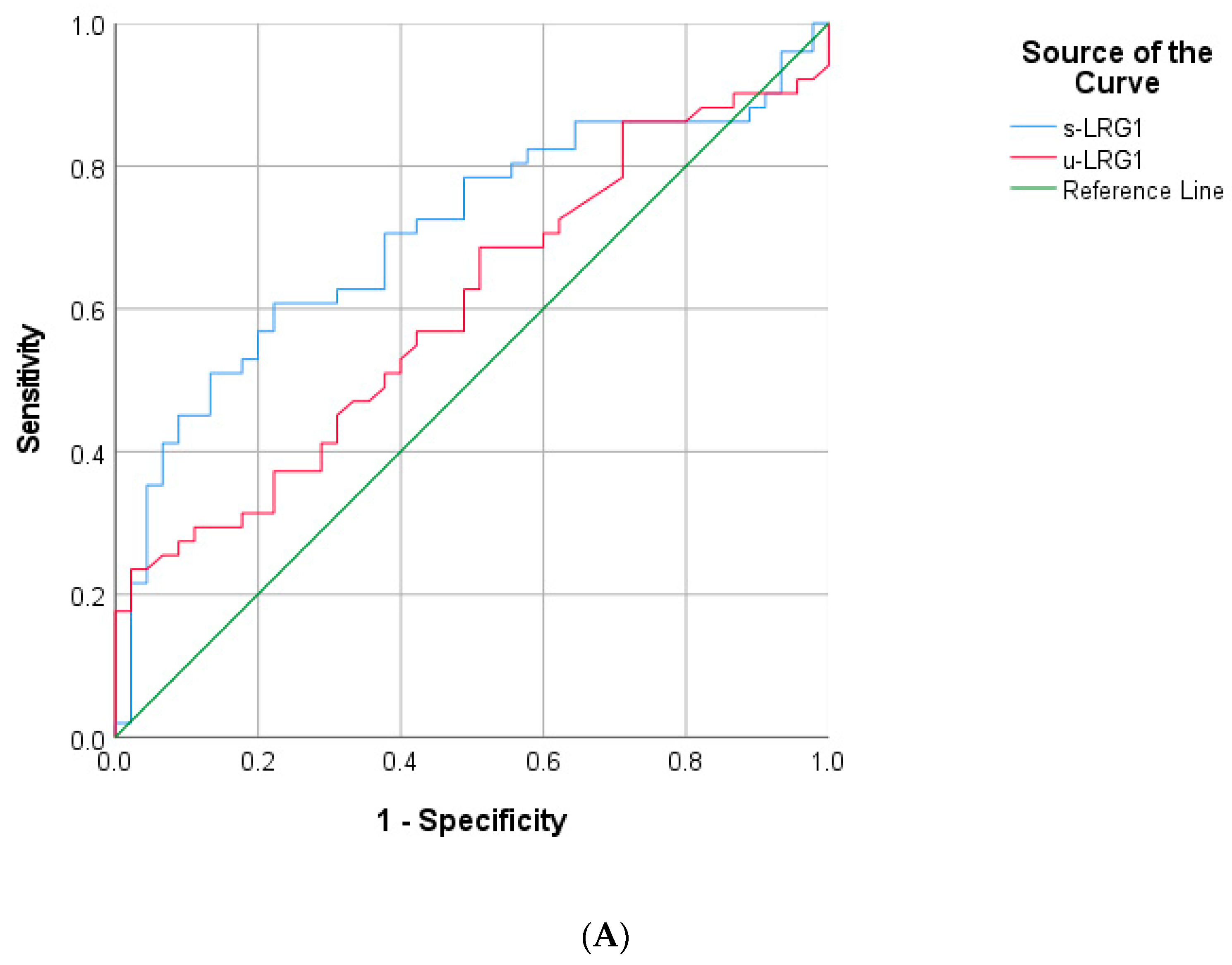
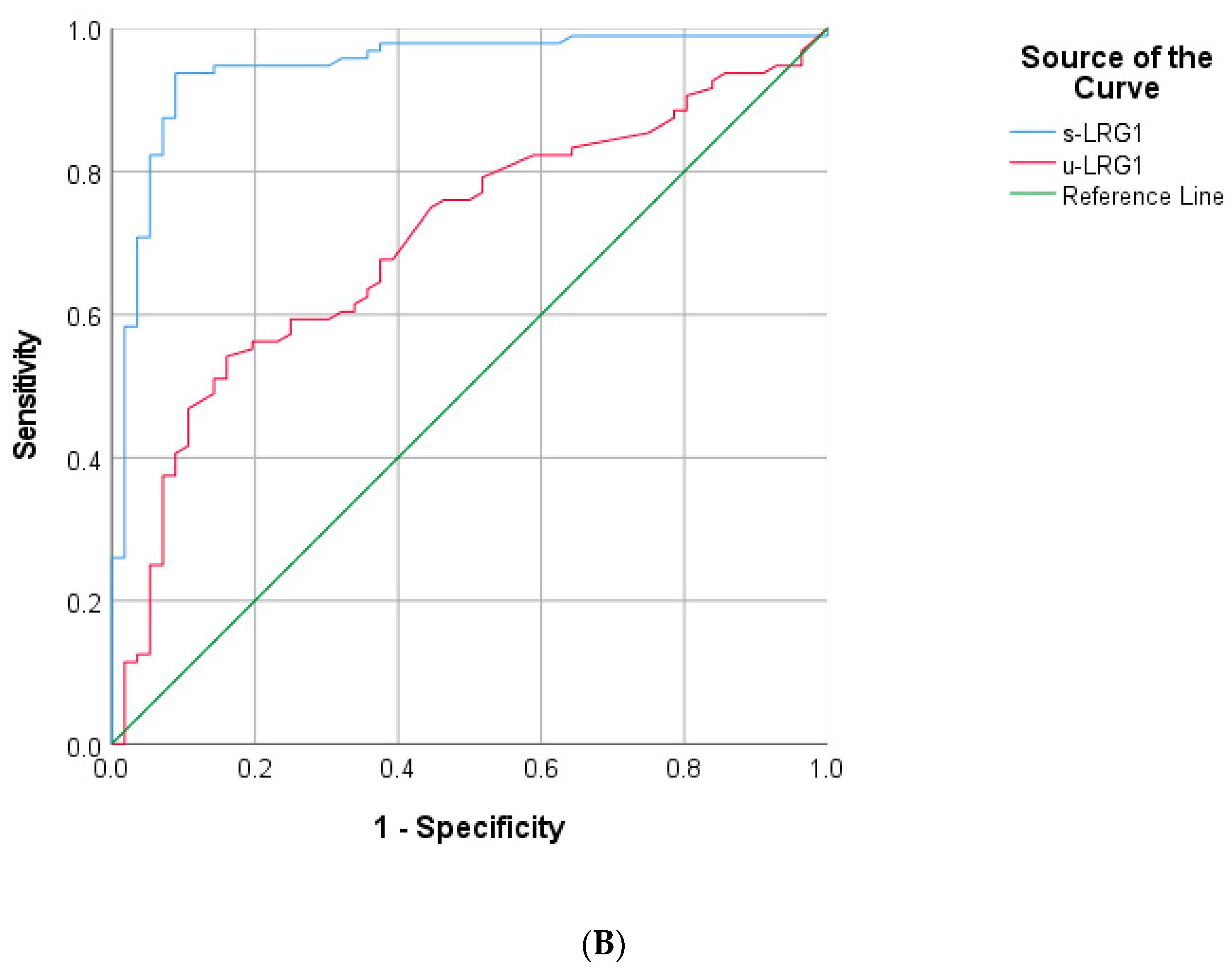
3.4. Threshold Sensitivity and Specificity of Leucine-Rich Alpha-2 Glycoprotein-1
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AA | Appendicitis |
| AcA | Acute complicated appendicitis |
| AuA | Acute uncomplicated appendicitis |
| ELISA | Enzyme-linked immunosorbent assay |
| IL-6 | Interleukin 6 |
| s-LRG1 | Serum Leucine-rich alpha-2 glycoprotein 1 |
| TNF-α | Tumor necrosis factor-alpha |
| u-LRG1 | Urine Leucine-rich alpha-2 glycoprotein 1 |
References
- Joshi, M.K.; Joshi, R.; Alam, S.E.; Agarwal, S.; Kumar, S. Negative Appendectomy: An Audit of Resident-Performed Surgery. How Can Its Incidence Be Minimized? Indian J. Surg. 2015, 77, 913–917. [Google Scholar] [CrossRef] [Green Version]
- D’Souza, N.; Nugent, K. Appendicitis. BMJ Clin. Evid. 2014, 8, 0408. [Google Scholar]
- Blomqvist, P.G.; Andersson, R.E.B.; Granath, F.; Lambe, M.P.; Ekbom, A.R. Mortality after appendectomy in Sweden, 1987–1996. Ann. Surg. 2001, 233, 455–460. [Google Scholar] [CrossRef] [PubMed]
- Zviedre, A.; Engelis, A.; Tretjakovs, P.; Jurka, A.; Zile, I.; Petersons, A. Role of serum cytokines in acute appendicitis and acute mesenteric lymphadenitis among children. Medicina 2016, 52, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Podany, A.B. Acute Appendicitis in Pediatric Patients: An Updated Narrative Review. J. Clin. Gastroenterol. Treat. 2017, 3, 1–9. [Google Scholar] [CrossRef]
- Kingsnorth, A.; Reilly, D.O. Clinical review Acute pancreatitis. BMJ 2006, 332, 1072–1076. [Google Scholar] [CrossRef] [PubMed]
- Kharbanda, A.B.; Rai, A.J.; Cosme, Y.; Liu, K.; Dayan, P.S. Novel serum and urine markers for pediatric appendicitis. Acad. Emerg. Med. 2012, 19, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Almaramhy, H.H. Acute appendicitis in young children less than 5 years: Review article. Ital. J Pediatr. 2017, 43, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Wray, C.J.; Kao, L.S.; Millas, S.G.; Tsao, K.; Ko, T.C. Acute Appendicitis: Controversies in Diagnosis and Management. Curr. Probl. Surg. 2013, 50, 54–86. [Google Scholar] [CrossRef] [Green Version]
- Coursey, C.A.; Nelson, R.C.; Patel, M.B.; Cochran, C.; Dodd, L.G.; DeLong, D.M.; Vaslef, S. Making the diagnosis of acute appendicitis: Do more preoperative CT scans mean fewer negative appendectomies? A 10-year study. Radiology 2010, 254, 460–468. [Google Scholar] [CrossRef]
- Bachur, R.G.; Hennelly, K.; Callahan, M.J.; Chen, C.; Monuteaux, M.C. Diagnostic imaging and negative appendectomy rates in children: Effects of age and gender. Pediatrics 2012, 129, 877–884. [Google Scholar] [CrossRef] [Green Version]
- Kentsis, A.; Lin, Y.Y.; Kurek, K.; Calicchio, M.; Wang, Y.Y.; Monigatti, F.; Bachur, R. Discovery and Validation of Urine Markers of Acute Pediatric Appendicitis Using High-Accuracy Mass Spectrometry. Ann. Emerg. Med. 2010, 55. [Google Scholar] [CrossRef] [Green Version]
- Kentsis, A.; Ahmed, S.; Kurek, K.; Brennan, E.; Bradwin, G.; Steen, H.; Bachur, R. Detection and diagnostic value of urine leucine-rich α-2-glycoprotein in children with suspected acute appendicitis. Ann. Emerg. Med. 2012, 60, 78–83. [Google Scholar] [CrossRef] [Green Version]
- Naka, T.; Fujimoto, M. LRG is a novel inflammatory marker clinically useful for the evaluation of disease activity in rheumatoid arthritis and inflammatory bowel disease. Immunol. Med. 2018, 41, 62–67. [Google Scholar] [CrossRef]
- Serada, S.; Fujimoto, M.; Terabe, F.; Iijima, H.; Shinzaki, S.; Matsuzaki, S.; Naka, T. Serum leucine-rich alpha-2 glycoprotein is a disease activity biomarker in ulcerative colitis. Inflamm. Bowel. Dis. 2012, 18, 2169–2179. [Google Scholar] [CrossRef] [PubMed]
- Kentsis, A. Challenges and opportunities for discovery of disease biomarkers using urine proteomics. Pediatr. Int. 2011, 53, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Druhan, L.J.; Lance, A.; Li, S.; Price, A.E.; Emerson, J.T.; Baxter, S.A.; Avalos, B.R. Leucine rich α-2 glycoprotein: A novel neutrophil granule protein and modulator of myelopoiesis. PLoS ONE 2017, 12, e0170261. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Huang, R.; Tang, Q.; Yu, Y.; Huang, Q.; Chen, Y.; Wang, X. Leucine-rich alpha-2-glycoprotein-1 is up-regulated in colorectal cancer and is a tumor promoter. Oncotargets Ther. 2018, 11, 2745–2752. [Google Scholar] [CrossRef] [Green Version]
- Oikonomou, K.A.; Kapsoritakis, A.N.; Theodoridou, C.; Karangelis, D.; Germenis, A.; Stefanidis, I.; Potamianos, S.P. Neutrophil gelatinase-associated lipocalin (NGAL) in inflammatory bowel disease: Association with pathophysiology of inflammation, established markers, and disease activity. J. Gastroenterol. 2012, 47, 519–530. [Google Scholar] [CrossRef]
- Shinzaki, S.; Matsuoka, K.; Iijima, H.; Mizuno, S.; Serada, S.; Fujimoto, M.; Naka, T. Leucine-rich Alpha-2 glycoprotein is a serum biomarker of mucosal healing in ulcerative colitis. J. Crohn’s Colitis 2017, 11, 84–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Donnell, L.C.; Druhan, L.J.; Avalos, B.R. Molecular characterization and expression analysis of leucine rich alpha2-glycoprotein, a novel marker of granulocytic differentiation. J. Leukoc. Biol. 2002, 72, 478–485. [Google Scholar]
- Wang, C.H.; Li, M.; Liu, L.L.; Zhou, R.Y.; Fu, J.; Zhang, C.Z.; Yun, J.P. LRG1 expression indicates unfavorable clinical outcome in hepatocellular carcinoma. Oncotarget 2015, 6, 42118–42129. [Google Scholar] [CrossRef] [Green Version]
- Andersen, J.D.; Boylan, K.L.M.; Jemmerson, R.; Geller, M.A.; Misemer, B.; Harrington, K.M.; Skubitz, A.P.N. Leucine-rich alpha-2-glycoprotein-1 is upregulated in sera and tumors of ovarian cancer patients. J. Ovarian Res. 2010, 3, 21. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Zhu, L.; Fang, J.; Ge, Z.; Li, X. LRG1 modulates epithelial-mesenchymal transition and angiogenesis in colorectal cancer via HIF-1α activation. J. Exp. Clin. Cancer Res. 2016, 35, 29. [Google Scholar] [CrossRef] [Green Version]
- Hao, L.; Xie, H.; Zhang, B.; Chen, D.; Wang, S.; Zhang, H.; He, S. LRG1 downregulation in allergic airway disorders and its expression in peripheral blood and tissue cells. J. Transl. Med. 2016, 14, 202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Codina, R.; Vanasse, A.; Kelekar, A.; Vezys, V.; Jemmerson, R. Cytochrome c-induced lymphocyte death from the outside in: Inhibition by serum leucine-rich alpha-2-glycoprotein-1. Apoptosis 2010, 15, 139–152. [Google Scholar] [CrossRef] [PubMed]
- Bozkurt, S.; Köse, A.; Erdogan, S.; Bozali, G.I.; Ayrik, C.; Arpaci, R.B.; Türkmenoglu, Ö. MPV and other inflammatory markers in diagnosing acute appendicitis. J. Pak. Med. Assoc. 2015, 65, 637–641. [Google Scholar]
- Sandanayake, N.S.; Sinclair, J.; Andreola, F.; Chapman, M.H.; Xue, A.; Webster, G.J.; Pereira, S.P. A combination of serum leucine-rich α-2-glycoprotein 1, CA19-9 and interleukin-6 differentiate biliary tract cancer from benign biliary strictures. Br. J. Cancer 2011, 105, 1370–1378. [Google Scholar] [CrossRef] [PubMed]
- Yap, T.L.; Fan, J.D.; Chen, Y.; Ho, M.F.; Choo, C.S.; Allen, J.; Nah, S.A. A novel noninvasive appendicitis score with a urine biomarker. J. Pediatr. Surg. 2019, 54, 91–96. [Google Scholar] [CrossRef] [Green Version]
- Kakar, M.; Delmore, M.; Broks, R.; Asare, L.; Butnere, M.; Saxena, A.; Engelis, A.; Kroica, J.; Saxena, A.; Petersons, A. Determining Acute Complicated and Uncomplicated Appendicitis Using Serum and Urine Biomarkers: Interleukin-6 and Neutrophil Gelatinase Lipocal. Pediatr. Surg. Int. 2020, 36, 629–636. [Google Scholar] [CrossRef]
- Rainer, T.H.; Leung, L.Y.; Chan, C.P.Y.; Leung, Y.K.; Cheng, N.M.; Lai, P.B.S.; Graham, C.A. Circulating human leucine-rich α-2-glycoprotein 1 mRNA and protein levels to detect acute appendicitis in patients with acute abdominal pain. Clin. Biochem. 2017, 50, 485–490. [Google Scholar] [CrossRef] [PubMed]
- Saloö, M.; Roth, B.; Stenstroöm, P.; Arnbjörnsson, E.; Ohlsson, B. Urinary biomarkers in pediatric appendicitis. Pediatr. Surg. Int. 2016, 32, 795–804. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Fujimoto, M.; Ohkawara, T.; Honda, H.; Serada, S.; Terada, Y.; Naka, T. Leucine rich α-2 glycoprotein is a potential urinary biomarker for renal tubular injury. Biochem. Biophys. Res. Commun. 2018, 498, 1045–1051. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| AuA | AcA | Ctr | Total | p-Value | |
|---|---|---|---|---|---|
| n = 45 | n = 52 | n = 56 | n = 153 | ||
| Gender, n (%) | |||||
| Boy | 23 (14.4) | 27 (18.3) | 39 (25.5) | 89 (58.2) | 0.081 * |
| Girl | 23 (15.0) | 24 (15.7) | 17 (11.1) | 64 (41.8) | |
| Age, Mdn (IQR) | 13.0 (10.0–15.0) | 12.0 (9.0–14.0) | 13.5 (10.3–15.0) | - | 0.101 *** |
| Type of surgery, n (%) | 85 (87.6) | ||||
| Laparoscopy | 41 (91.1) | 44 (84.6) | - | 0.333 * | |
| Laparotomy | 4 (8.9) | 8 (15.4) | - | 12 (12.4) | |
| Ultrasound, n (%) | 30 (43.5) | 39 (56.5) | - | 69 (0.83) | 0.349 * |
| Drainage tube, n (%) | 40 | ||||
| Yes | 9 (20.9) | 31 (60.8) | - | <0.001 * | |
| No | 34 (79.1) | 20 (39.2) | - | 54 | |
| Length of hospital stay, days (IQR) | 5 (4–6) | 6 (4–9) | - | - | 0.002 ** |
| AcA, μg/mL (IQR) | AuA, μg/mL (IQR) | Control, μg/mL (IQR) | p-Value | |
|---|---|---|---|---|
| DAY 0 | ||||
| Serum | 70.56 (62.64–83.43) | 88.12 (71.12–106.13) | 34.08 (27.50–42.37) | <0.001 |
| Urine | 0.10 (0.03–0.73) | 0.35 (0.05–1.38) | 0.04 (0.02–0.10) | <0.001 |
| DAY 2 | ||||
| Serum | 74.99 (61.00–96.03) | 87.90 (70.32–104.10) | 0.048 | |
| Urine | 0.08 (0.03–0.28) | 0.21 (0.06–0.98) | 0.017 | |
| DAY 5 | ||||
| Serum | 66.73 (56.98–85.28) | 80.97 (62.14–99.03) | 0.110 | |
| Urine | 0.04 (0.02–0.27) | 0.10 (0.03–0.25) | 0.102 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kakar, M.; Berezovska, M.M.; Broks, R.; Asare, L.; Delorme, M.; Crouzen, E.; Zviedre, A.; Reinis, A.; Engelis, A.; Kroica, J.; et al. Serum and Urine Biomarker Leucine-Rich Alpha-2 Glycoprotein 1 Differentiates Pediatric Acute Complicated and Uncomplicated Appendicitis. Diagnostics 2021, 11, 860. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11050860
Kakar M, Berezovska MM, Broks R, Asare L, Delorme M, Crouzen E, Zviedre A, Reinis A, Engelis A, Kroica J, et al. Serum and Urine Biomarker Leucine-Rich Alpha-2 Glycoprotein 1 Differentiates Pediatric Acute Complicated and Uncomplicated Appendicitis. Diagnostics. 2021; 11(5):860. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11050860
Chicago/Turabian StyleKakar, Mohit, Marisa Maija Berezovska, Renars Broks, Lasma Asare, Mathilde Delorme, Emile Crouzen, Astra Zviedre, Aigars Reinis, Arnis Engelis, Juta Kroica, and et al. 2021. "Serum and Urine Biomarker Leucine-Rich Alpha-2 Glycoprotein 1 Differentiates Pediatric Acute Complicated and Uncomplicated Appendicitis" Diagnostics 11, no. 5: 860. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11050860