
COVID-19 Vaccine and Death: Causality Algorithm According to the WHO Eligibility Diagnosis

 ,
,  ,
,  , ,
, ,  , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Structure of the WHO AEFI Guidelines
- -
- Is there strong evidence for other causes? To answer this question, it is fundamental to analyze the medical history of the patient, focusing on the clinical examination to confirm the relationship.
- -
- Is there a known causal association with the vaccine or vaccination? For this question, is important to analyze the vaccine product and vaccine quality. Moreover, it is important to exclude immunization errors and immunization stress-related responses.
- -
- Is there strong evidence against a causal association? At this point, a literature review should be performed in order to exclude the presence of published evidence against a causal association between vaccine administration and the event.
- -
- Finally, it is important to analyze other qualifying factors for classification (for example, pre-existing conditions, event-related to previous vaccinations, etc.).
- A.
- Consistent with causal association to immunization;
- B.
- Indeterminate;
- C.
- Inconsistent with causal association to immunization;
- D.
- Unclassifiable.
2.2. Adaptation of the Global WHO Guidelines to AEFI Post COVID-19 Vaccine
2.3. Vaccine Characteristics and Exhaustive Review of the Literature
2.4. Exemplificative Cases Needing AEFI Diagnosis after ChAdOx1 nCoV-19 Vaccine Administration
2.5. Autopsy Methodology
2.6. Tests and Biomarkers
- Thrombosis panel test (D-dimer, prothrombin time and international normalized ratio (PT/INR), partial thromboplastin time (PTT, aPTT), complete blood count (CBC), antiphospholipid antibodies, lupus anticoagulant testing, antithrombin, protein C, protein S, and ID-Heparin/PF4 antibody test).
- Genetic testing for thrombophilia (factor V Leiden mutation, factor II 20210 mutation).
- Molecular tests for detection of SARS-CoV-2 using other lung samples (i.e., bronchial wash (BW)/bronchoalveolar lavage (BAL) specimens, post-mortem lung swab).
- Molecular tests for detection of SARS-CoV-2 in atypical samples, using formalin-fixed paraffin-embedded (FFPE) tissue specimens.
- Panel for respiratory viruses (adenovirus, coronavirus (229E, HKU1, NL63, OC43), human metapneumovirus, human rhinovirus/enterovirus, influenza A, influenza A H1, influenza A H1-2009, influenza A H3, influenza B, parainfluenza 1, parainfluenza 2, parainfluenza 3, parainfluenza 4, respiratory syncytial virus A, respiratory syncytial virus B, chlamydia pneumonia, mycoplasma pneumonia).
- Panel for respiratory bacterial pathogens (Bordetella pertussis, Chlamydophyla pneumoniae, Mycoplasma pneumoniae, Legionella pneumophila, Haemophilus influenza, Streptococcus pneumonia, Streptococcus pyogenes, Acinetobacter calcoaceticus-baumannii, Enterobacter aerogenes-cloacae, Escherichia coli, Klebsiella pneumoniae, proteus spp., Pseudomonas aeruginosa, Serratia marcescens, Staphylococcus aureus).
- Tests for other viral infections (i.e., cytomegalo virus (CMV); Epstein–Barr virus (EBV); herpes simplex virus (HSV); varicella-zoster virus (VZV).
- Detection of the viral vector of the COVID-19 vaccine.
3. Results
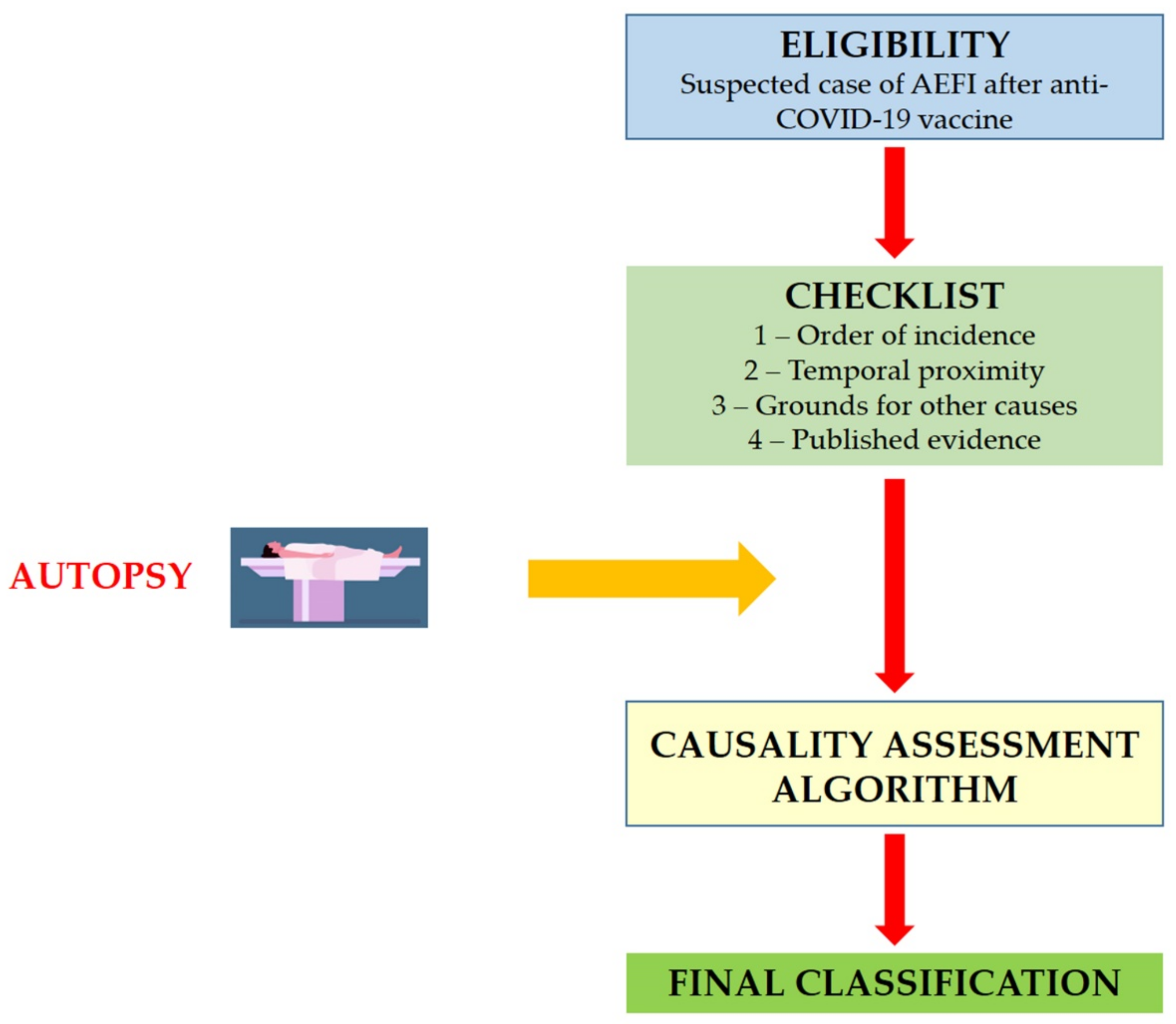
3.1. Structure of the AEFI Procedures for COVID-19 Vaccination
3.2. Eligibility
3.3. Checklist
3.4. Laboratory Tests and Results
3.5. Autopsy
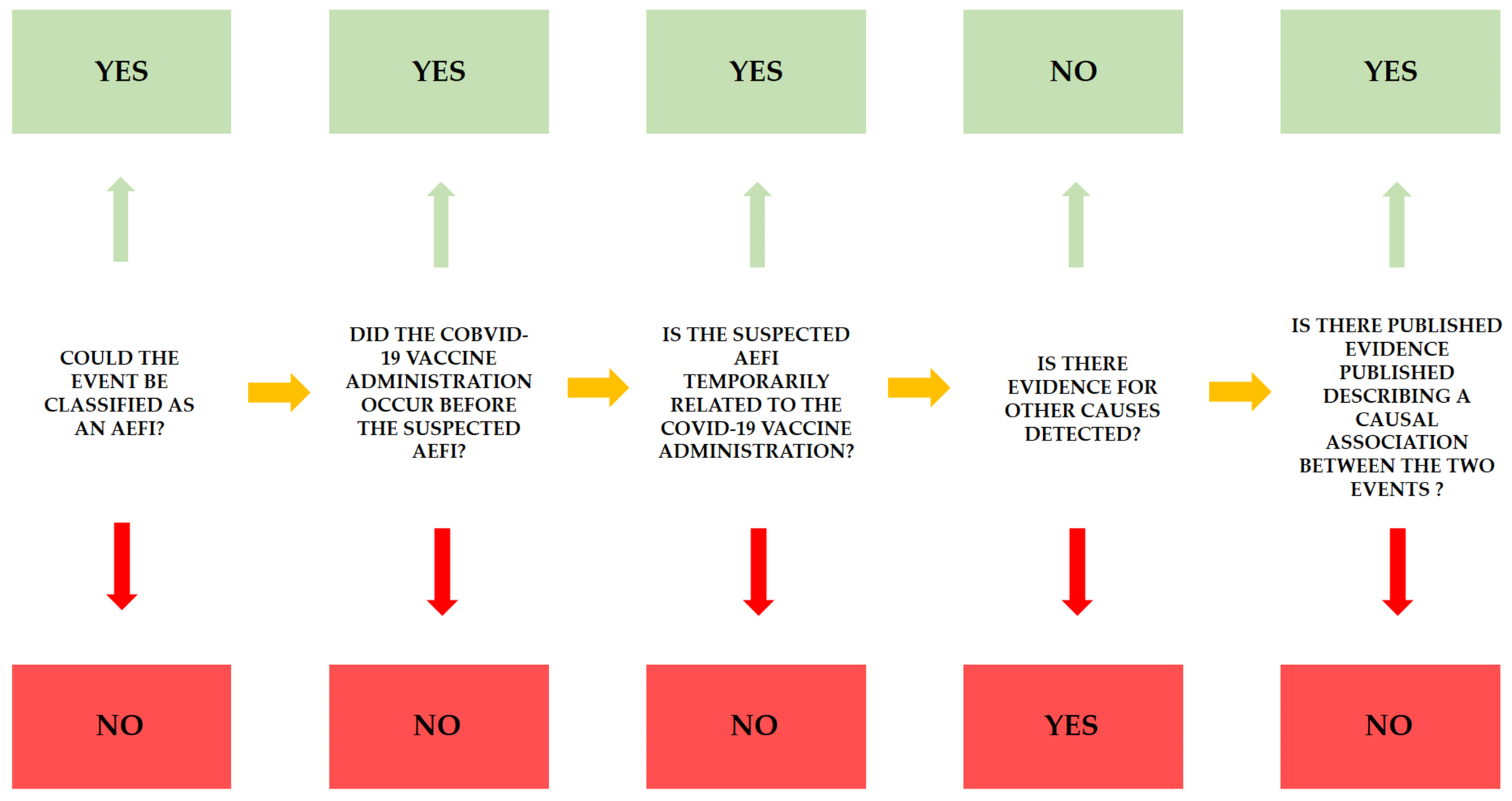
3.6. Algorithm and Classification
- The AEFI is related to vaccine administration (in the presence of clear evidence of vaccine administration, confirmed by a temporal relationship, after the exclusion of other causes. Moreover, there is published evidence that confirmed the relationship).
- The AEFI is probably related with vaccine administration (in the presence of clear evidence of vaccine administration, confirmed by a temporal relationship, after the exclusion of other causes, but there is no published evidence that confirmed the relationship).
- The AEFI could be related to vaccine administration (in the presence of clear evidence of vaccine administration, confirmed by a temporal relationship. The presence of other causes that could be related to symptoms).
- The AEFI could not be related to vaccine administration (in the presence of clear evidence of vaccine administration, there is no clear temporal relationship; moreover, the causal association is not clear).
- The AEFI is not related to vaccine administration (there is no evidence of vaccine administration).
3.7. Application
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- EMA. EMA Recommends First COVID-19 Vaccine for Authorisation in the EU. Available online: https://www.ema.europa.eu/en/news/ema-recommends-first-covid-19-vaccine-authorisation-eu (accessed on 27 March 2021).
- EMA. EMA Recommends COVID-19 Vaccine Moderna for Authorisation in the EU. Available online: https://www.ema.europa.eu/en/news/ema-recommends-covid-19-vaccine-moderna-authorisation-eu (accessed on 27 March 2021).
- EMA. EMA Recommends COVID-19 Vaccine AstraZeneca for Authorisation in the EU. Available online: https://www.ema.europa.eu/en/news/ema-recommends-covid-19-vaccine-astrazeneca-authorisation-eu (accessed on 27 March 2021).
- EMA. EMA Recommends COVID-19 Vaccine Janssen for Authorisation in the EU. Available online: https://www.ema.europa.eu/en/news/ema-recommends-covid-19-vaccine-janssen-authorisation-eu (accessed on 13 April 2021).
- Karpiński, T.M.; Ożarowski, M.; Seremak-Mrozikiewicz, A.; Wolski, H.; Wlodkowic, D. The 2020 race towards SARS-CoV-2 specific vaccines. Theranostics 2021, 11, 1690–1702. [Google Scholar] [CrossRef]
- EMA AstraZeneca’s COVID-19 Vaccine: EMA Finds Possible Link to very Rare Cases of Unusual Blood Clots with Low Blood Platelets. Available online: https://www.ema.europa.eu/en/news/astrazenecas-covid-19-vaccine-ema-finds-possible-link-very-rare-cases-unusual-blood-clots-low-blood (accessed on 10 April 2021).
- Schultz, N.H.; Sørvoll, I.H.; Michelsen, A.E.; Munthe, L.A.; Lund-Johansen, F.; Ahlen, M.T.; Wiedmann, M.; Aamodt, A.-H.; Skattør, T.H.; Tjønnfjord, G.E.; et al. Thrombosis and Thrombocytopenia after ChAdOx1 nCoV-19 Vaccination. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef]
- Wolf, M.E.; Luz, B.; Niehaus, L.; Bhogal, P.; Bäzner, H.; Henkes, H. Thrombocytopenia and Intracranial Venous Sinus Thrombosis after “COVID-19 Vaccine AstraZeneca” Exposure. J. Clin. Med. 2021, 10, 1599. [Google Scholar] [CrossRef]
- Greinacher, A.; Thiele, T.; Warkentin, T.E.; Weisser, K.; Kyrle, P.A.; Eichinger, S. Thrombotic Thrombocytopenia after ChAdOx1 nCov-19 Vaccination. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef]
- EMA COVID-19 Vaccine Janssen: EMA Finds Possible Link to very Rare Cases of Unusual Blood Clots with Low Blood Platelets. Available online: https://www.ema.europa.eu/en/news/covid-19-vaccine-janssen-ema-finds-possible-link-very-rare-cases-unusual-blood-clots-low-blood (accessed on 21 April 2021).
- WHO. Causality Assessment of an Adverse Event Following Immunization, 2nd ed.; World Health Organization: Geneva, Switzerland, 2019; ISBN 9789241513654. [Google Scholar]
- WHO Interim Recommendations for Use of the Pfizer–BioNTech COVID-19 Vaccine, BNT162b2, under Emergency Use Listing. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-vaccines-SAGE_recommendation-BNT162b2-2021.1 (accessed on 14 April 2021).
- WHO Interim Recommendations for Use of the Moderna mRNA-1273 Vaccine against COVID-19. Available online: https://www.who.int/publications/i/item/interim-recommendations-for-use-of-the-moderna-mrna-1273-vaccine-against-covid-19 (accessed on 14 April 2021).
- WHO Interim Recommendations for Use of the AZD1222 (ChAdOx1-S (Recombinant)) Vaccine against COVID-19 Developed by Oxford University and AstraZeneca. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-vaccines-SAGE_recommendation-AZD1222-2021.1 (accessed on 14 April 2021).
- WHO Interim Recommendations for the Use of the Janssen Ad26.COV2.S (COVID-19) Vaccine: Interim Guidance. Available online: https://apps.who.int/iris/handle/10665/340203 (accessed on 14 April 2021).
- Cines, D.B.; Bussel, J.B. SARS-CoV-2 Vaccine–Induced Immune Thrombotic Thrombocytopenia. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef]
- Scully, M.; Singh, D.; Lown, R.; Poles, A.; Solomon, T.; Levi, M.; Goldblatt, D.; Kotoucek, P.; Thomas, W.; Lester, W. Pathologic Antibodies to Platelet Factor 4 after ChAdOx1 nCoV-19 Vaccination. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Bayas, A.; Menacher, M.; Christ, M.; Behrens, L.; Rank, A.; Naumann, M. Bilateral superior ophthalmic vein thrombosis, ischaemic stroke, and immune thrombocytopenia after ChAdOx1 nCoV-19 vaccination. Lancet 2021, 397, e11. [Google Scholar] [CrossRef]
- Sadoff, J.; Davis, K.; Douoguih, M. Thrombotic Thrombocytopenia after Ad26.COV2.S Vaccination—Response from the Manufacturer. N. Engl. J. Med. 2021, 384, 1965–1966. [Google Scholar] [CrossRef] [PubMed]
- WHO Interim Guidance Infection Prevention and Control for the safe management of a dead body in the context of COVID-19. J. Hosp. Infect. 2020, 104, 246–251.
- Centers for Disease Control and Prevention Collection and Submission of Postmortem Specimens from Deceased Persons with Known or Suspected COVID-19. Available online: https://eaaf.org/wp-content/uploads/covid19-PDFs/EEUU/CDC-guidance-postmortem-specimens.pdf (accessed on 18 August 2020).
- Pomara, C.; Volti, G.L.; Cappello, F. COVID-19 Deaths: Are We Sure It Is Pneumonia? Please, Autopsy, Autopsy, Autopsy! J. Clin. Med. 2020, 9, 1259. [Google Scholar] [CrossRef] [PubMed]
- Sriwijitalai, W.; Wiwanitkit, V. COVID-19 in forensic medicine unit personnel: Observation from Thailand. J. Forensic Leg. Med. 2020, 72, 101964. [Google Scholar] [CrossRef] [PubMed]
- Pomara, C.; Salerno, M.; Sessa, F.; Esposito, M.; Barchitta, M.; Ledda, C.; Grassi, P.; Liberto, A.; Mattaliano, A.R.; Rapisarda, V.; et al. Safe Management Strategies in Clinical Forensic Autopsies of Confirmed COVID-19 Cases. Diagnostics 2021, 11, 457. [Google Scholar] [CrossRef]
- Sessa, F.; Bertozzi, G.; Cipolloni, L.; Baldari, B.; Cantatore, S.; D’Errico, S.; Di Mizio, G.; Asmundo, A.; Castorina, S.; Salerno, M.; et al. Clinical-Forensic Autopsy Findings to Defeat COVID-19 Disease: A Literature Review. J. Clin. Med. 2020, 9, 2026. [Google Scholar] [CrossRef]
- Pomara, C.; Fineschi, V. Forensic and Clinical Forensic Autopsy. An Atlas and Handbook, 2nd ed.; Pomara, C., Fineschi, V., Eds.; CRC Press: Boca Raton, FL, USA, 2020; ISBN 9780367330712. [Google Scholar]
- Sicily Regional taskforce for the implementation of diagnostic findings and autopsy exami-nations in Covid-19 positive corpses or in the event of post-vaccination deaths. Gazz. Uff. Della Reg. Sicil. 2021, 75, 32.
- Castaman, G.; Lunghi, B.; Missiaglia, E.; Bernardi, F.; Rodeghiero, F. Phenotypic homozygous activated protein C resistance associated with compound heterozygosity for Arg506Gln (factor V Leiden) and His1299 Arg substitutions in factor V. Br. J. Haematol. 1997, 99, 257–261. [Google Scholar] [CrossRef] [Green Version]
- Segers, O.; Simioni, P.; Tormene, D.; Bulato, C.; Gavasso, S.; Rosing, J.; Castoldi, E. Genetic modulation of the FVLeiden/normal FV ratio and risk of venous thrombosis in factor V Leiden heterozygotes. J. Thromb. Haemost. 2012, 10, 73–80. [Google Scholar] [CrossRef]
- Bafunno, V.; Santacroce, R.; Chetta, M.; D’Andrea, G.; Pisanelli, D.; Sessa, F.; Trotta, T.; Tagariello, G.; Peyvandi, F.; Margaglione, M. Polymorphisms in genes involved in autoimmune disease and the risk of FVIII inhibitor development in Italian patients with haemophilia A. Haemophilia 2010, 16, 469–473. [Google Scholar] [CrossRef]
- Varga, E. Inherited thrombophilia: Key points for genetic counseling. J. Genet. Couns. 2007, 16, 261–277. [Google Scholar] [CrossRef] [PubMed]
- Santacroce, R.; Santoro, R.; Sessa, F.; Iannaccaro, P.; Sarno, M.; Longo, V.; Gallone, A.; Vecchione, G.; Muleo, G.; Margaglione, M. Screening of mutations of hemophilia A in 40 Italian patients: A novel G-to-A mutation in intron 10 of the F8 gene as a putative cause of mild hemophilia a in southern Italy. Blood Coagul. Fibrinolysis 2008, 19, 197–202. [Google Scholar] [CrossRef]
- Bafunno, V.; Bury, L.; Tiscia, G.L.; Fierro, T.; Favuzzi, G.; Caliandro, R.; Sessa, F.; Grandone, E.; Margaglione, M.; Gresele, P. A novel congenital dysprothrombinemia leading to defective prothrombin maturation. Thromb. Res. 2014, 134, 1135–1141. [Google Scholar] [CrossRef] [PubMed]
- Esposito, M.; Montana, A.; Liberto, A.; Filetti, V.; Di Nunno, N.; Amico, F.; Salerno, M.; Loreto, C.; Sessa, F. Anaphylactic Death: A New Forensic Workflow for Diagnosis. Healthcare 2021, 9, 117. [Google Scholar] [CrossRef]
- Salthouse, T.N. Histopathologic Technic and Practical Histochemistry. Bull. Soc. Pharmacol. Environ. Pathol. 1977, 70, 549. [Google Scholar] [CrossRef]
- Facchetti, F.; Bugatti, M.; Drera, E.; Tripodo, C.; Sartori, E.; Cancila, V.; Papaccio, M.; Castellani, R.; Casola, S.; Boniotti, M.B.; et al. SARS-CoV2 vertical transmission with adverse effects on the newborn revealed through integrated immunohistochemical, electron microscopy and molecular analyses of Placenta. EBioMedicine 2020, 59, 102951. [Google Scholar] [CrossRef] [PubMed]
- Rohr, U.-P.; Wulf, M.-A.; Stahn, S.; Steidl, U.; Haas, R.; Kronenwett, R. Fast and reliable titration of recombinant adeno-associated virus type-2 using quantitative real-time PCR. J. Virol. Methods 2002, 106, 81–88. [Google Scholar] [CrossRef]
- Sessa, F.; Salerno, M.; Pomara, C. Autopsy Tool in Unknown Diseases: The Experience with Coronaviruses (SARS-CoV, MERS-CoV, SARS-CoV-2). Medicina 2021, 57, 309. [Google Scholar] [CrossRef]
- Cheung, K.S.; Hung, I.F.N.; Chan, P.P.Y.; Lung, K.C.; Tso, E.; Liu, R.; Ng, Y.Y.; Chu, M.Y.; Chung, T.W.H.; Tam, A.R.; et al. Gastrointestinal Manifestations of SARS-CoV-2 Infection and Virus Load in Fecal Samples From a Hong Kong Cohort: Systematic Review and Meta-analysis. Gastroenterology 2020, 159, 81–95. [Google Scholar] [CrossRef]
- Wu, Y.; Guo, C.; Tang, L.; Hong, Z.; Zhou, J.; Dong, X.; Yin, H.; Xiao, Q.; Tang, Y.; Qu, X.; et al. Prolonged presence of SARS-CoV-2 viral RNA in faecal samples. Lancet Gastroenterol. Hepatol. 2020, 5, 434–435. [Google Scholar] [CrossRef]
- De Cock, K.M.; Zielinski-Gutiérrez, E.; Lucas, S.B. Learning from the Dead. N. Engl. J. Med. 2019, 381, 1889–1891. [Google Scholar] [CrossRef]
- Bolcato, M.; Russo, M.; Trentino, K.; Isbister, J.; Rodriguez, D.; Aprile, A. Patient blood management: The best approach to transfusion medicine risk management. Transfus. Apher. Sci. 2020, 59, 102779. [Google Scholar] [CrossRef]
- Denis, M.M.; Tolley, N.D.; Bunting, M.; Schwertz, H.; Jiang, H.; Lindemann, S.; Yost, C.C.; Rubner, F.J.; Albertine, K.H.; Swoboda, K.J.; et al. Escaping the nuclear confines: Signal-dependent pre-mRNA splicing in anucleate platelets. Cell 2005, 122, 379–391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Best, M.G.; Vancura, A.; Wurdinger, T. Platelet RNA as a circulating biomarker trove for cancer diagnostics. J. Thromb. Haemost. 2017, 15, 1295–1306. [Google Scholar] [CrossRef] [Green Version]
- Rowley, J.W.; Schwertz, H.; Weyrich, A.S. Platelet mRNA: The meaning behind the message. Curr. Opin. Hematol. 2012, 19, 385–391. [Google Scholar] [CrossRef]
- Schubert, S.; Weyrich, A.S.; Rowley, J.W. A tour through the transcriptional landscape of platelets. Blood 2014, 124, 493–502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marino Gammazza, A.; Légaré, S.; Lo Bosco, G.; Fucarino, A.; Angileri, F.; Conway de Macario, E.; Macario, A.J.; Cappello, F. Human molecular chaperones share with SARS-CoV-2 antigenic epitopes potentially capable of eliciting autoimmunity against endothelial cells: Possible role of molecular mimicry in COVID-19. Cell Stress Chaperones 2020, 25, 737–741. [Google Scholar] [CrossRef] [PubMed]
- Angileri, F.; Legare, S.; Marino Gammazza, A.; Conway de Macario, E.; JL Macario, A.; Cappello, F. Molecular mimicry may explain multi-organ damage in COVID-19. Autoimmun. Rev. 2020, 19, 102591. [Google Scholar] [CrossRef] [PubMed]
- Levi, M.; Sivapalaratnam, S. Disseminated intravascular coagulation: An update on pathogenesis and diagnosis. Expert Rev. Hematol. 2018, 11, 663–672. [Google Scholar] [CrossRef]
- Zamboni, P. COVID-19 as a Vascular Disease: Lesson Learned from Imaging and Blood Biomarkers. Diagnostics 2020, 10, 440. [Google Scholar] [CrossRef]
- Arvin, A.M.; Fink, K.; Schmid, M.A.; Cathcart, A.; Spreafico, R.; Havenar-Daughton, C.; Lanzavecchia, A.; Corti, D.; Virgin, H.W. A perspective on potential antibody-dependent enhancement of SARS-CoV-2. Nature 2020, 584, 353–363. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.S.; Wheatley, A.K.; Kent, S.J.; DeKosky, B.J. Antibody-dependent enhancement and SARS-CoV-2 vaccines and therapies. Nat. Microbiol. 2020, 5, 1185–1191. [Google Scholar] [CrossRef] [PubMed]
- Marone, E.M.; Rinaldi, L.F. Upsurge of deep venous thrombosis in patients affected by COVID-19: Preliminary data and possible explanations. J. Vasc. Surg. Venous Lymphat. Disord. 2020, 8, 694–695. [Google Scholar] [CrossRef] [PubMed]
- Middeldorp, S.; Coppens, M.; van Haaps, T.F.; Foppen, M.; Vlaar, A.P.; Müller, M.C.A.; Bouman, C.C.S.; Beenen, L.F.M.; Kootte, R.S.; Heijmans, J.; et al. Incidence of venous thromboembolism in hospitalized patients with COVID-19. J. Thromb. Haemost. 2020, 18, 1995–2002. [Google Scholar] [CrossRef] [PubMed]
- Wright, F.L.; Vogler, T.O.; Moore, E.E.; Moore, H.B.; Wohlauer, M.V.; Urban, S.; Nydam, T.L.; Moore, P.K.; McIntyre, R.C. Fibrinolysis Shutdown Correlation with Thromboembolic Events in Severe COVID-19 Infection. J. Am. Coll. Surg. 2020, 231, 193–203.e1. [Google Scholar] [CrossRef] [PubMed]
- Snell, J. SARS-CoV-2 infection and its association with thrombosis and ischemic stroke: A review. Am. J. Emerg. Med. 2021, 40, 188–192. [Google Scholar] [CrossRef] [PubMed]
- Cipolloni, L.; Sessa, F.; Bertozzi, G.; Baldari, B.; Cantatore, S.; Testi, R.; D’Errico, S.; Di Mizio, G.; Asmundo, A.; Castorina, S.; et al. Preliminary post-mortem COVID-19 evidence of endothelial injury and factor VIII hyperexpression. Diagnostics 2020, 10, 575. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| 1. Order of events | |||||||
| Was the COVID-19 vaccine administered before the observed symptoms occurred? | Yes | No | |||||
| 2. Temporal proximity | |||||||
| Did the observed symptoms occur within 21 days following vaccination? | Yes | No | |||||
| Write the time interval between vaccination and occurrence of observed symptoms | Insert time in days | ||||||
| 3. Evidence for other causes | |||||||
| • For each question, please answer Y (Yes), N (No), UK (Unknown), NA (Not applicable) • Please write the reason for your choice in the note column. | |||||||
| Category | Items | Y | N | UK | NA | Note | |
| History | 3.1 Has the patient ever tested positive for COVID-19 infection? Please, write the time and the duration of COVID-19 infection | ||||||
| 3.2 Has the patient ever been vaccinated for COVID-19 infection before? If so, please write the name of vaccine and the vaccination date. | |||||||
| 3.3 Has the patient ever experienced any diseases after any type of vaccination? | |||||||
| Patient’s condition before appearance of symptoms | • Has the patient ever experienced any items below before the manifestation of COVID-19 vaccine severe adverse effects? If so, please indicate the event data. | ||||||
| 3.4 Upper respiratory infections | |||||||
| 3.5 Personal history of other venous thrombosis and embolism (ICD-10- CM Z86 Diagnosis Code) | |||||||
| 3.6 Severe cardiomyopathy (ICD-10-CM category I42) | |||||||
| 3.7 Other infections (i.e., HBV, HCV, HIV) | |||||||
| 3.8 Surgery | |||||||
| 3.9 Other pathologies | |||||||
| Patient examination | • Was a test among those listed below performed after the manifestation of COVID-19 vaccine severe adverse effects? If so, write the date of the test, test result, and specific other useful information. | ||||||
| 3.10 Post-mortem investigation (with histological and IHC investigations | |||||||
| 3.11 Thrombosis panel test | |||||||
| 3.12 Genetic testing for hypercoagulability | |||||||
| 3.13 Molecular tests for detection of SARS-CoV-2 using other lung samples | |||||||
| 3.14 Molecular tests for detection of SARS-CoV-2 in atypical samples, using formalin-fixed paraffin-embedded (FFPE) tissue specimens | |||||||
| 3.15 Panel for respiratory viruses | |||||||
| 3.16 Panel for respiratory bacterial pathogens | |||||||
| 3.17 Tests for other viral infections | |||||||
| 3.18 Detection of viral vector COVID-19 vaccine | |||||||
| Immunization anxiety | 3.19 Were the observed symptoms a stress response to vaccination? (e.g., acute stress response, vasovagal syncope, hyperventilation, anxiety, etc.) | ||||||
| Vaccine quality | 3.20 Could the vaccine given to this patient have a quality defect or be substandard or counterfeit? (i.e., checking production lot, storage condition, etc.) | ||||||
| Immunization errors (please, write type of error, if any) | 3.21 Did anything unusual occur during vaccination preparation? (e.g., incorrect mixing, use of expired vaccine, abnormal physical condition, etc.) | ||||||
| 3.22 Did anything unusual occur during the vaccination procedure? (e.g., Inoculation timing/dose/site/route, needle size error, etc.) | |||||||
| • If there are any suspicious causes other than those listed above, write the details below. | |||||||
| 4. Published evidence (literature, WHO GACVS, IOM etc.) regarding a causal association between the vaccine and observed symptoms. | |||||||
| Test | Method | Sample | Result | ||
|---|---|---|---|---|---|
| Case 1 | Case 2 | Case 1 | Case 2 | ||
| Genetic testing for hypercoagulability (Factor V Leiden Mutation, Factor II 20210 Mutation) | Real-time PCR (CVD6 MULTIPLEX REAL TIME, Nuclear Laser Medicine s.r.l., Settala (MI), Italy) | Hospitalization sample (blood), Cadaveric Blood, Cadaveric Tissue (spleen) | Hospitalization sample (blood), | Wild type | Wild Type |
| Molecular tests for detection of SARS-CoV-2 using other lung samples | Real-time PCR (Allplex™ SARS-CoV-2 Assay, Arrow Diagnostics, Genova, Italy) | Cadaveric lung swab | Bronchial wash sample | Negative | Negative |
| Molecular tests for detection of SARS-CoV-2 in atypical samples, using Formalin-Fixed Paraffin-Embedded (FFPE) tissue specimens | Real-time PCR (following the described protocol by Facchetti et al. [36]) | FFPE Tissues (lung and intestine tissues) | FFPE tissues (lung and intestine tissues) | Negative | Negative |
| Detection of viral vector COVID-19 vaccine virus | Real-time PCR (following the described protocol by Rohr et al. [37]) | Cadaveric Tissues (lung, spleen, cadaveric blood) | Cadaveric Tissues (lung, spleen, cadaveric blood) | Negative | Negative |
| IgG Anti-heparin/PF4 | Automated chemiluminescent anti-heparin/PF4 immunoassay | Hospitalization sample (blood) | Hospitalization sample (blood) | Negative 0.0.2 U/mL (>1 U/mL positive) | Negative 0.21 U/mL (>1 U/mL positive) |
| IgG Anti-polyanion/PF4 | Anti PF4/polyanion complex (PF4 Enhanced Test, Immucor, Waukesha, WI, USA). | Hospitalization sample (blood) | Hospitalization sample (blood) | Positive | Positive |
| Case 1 (Male, 50 y.o.) | Case 2 (Female, 37 y.o.) | |
|---|---|---|
| Macroscopic findings | Portal vein thrombosis with smaller thrombi in the splenic and upper mesenteric veins. Intracranial hemorrhage in the subarachnoid region. | Occlusive thrombus in the superior sagittal sinus and a very large hemorrhage in the frontal cerebral lobe. Moreover, in the axillary region of the left arm, a thrombus was detected |
| Microscopic findings (H&E staining) | The microscopic evaluation revealed numerous vascular thrombi and intense hemorrhagic phenomena localized in the meningeal space and extravasated in the brain tissue. The thrombotic phenomena involved small and medium vessels most likely due to damage of their walls, which induced endothelial activation and an inflammatory reaction with a procoagulant process and thrombotic reaction. | |
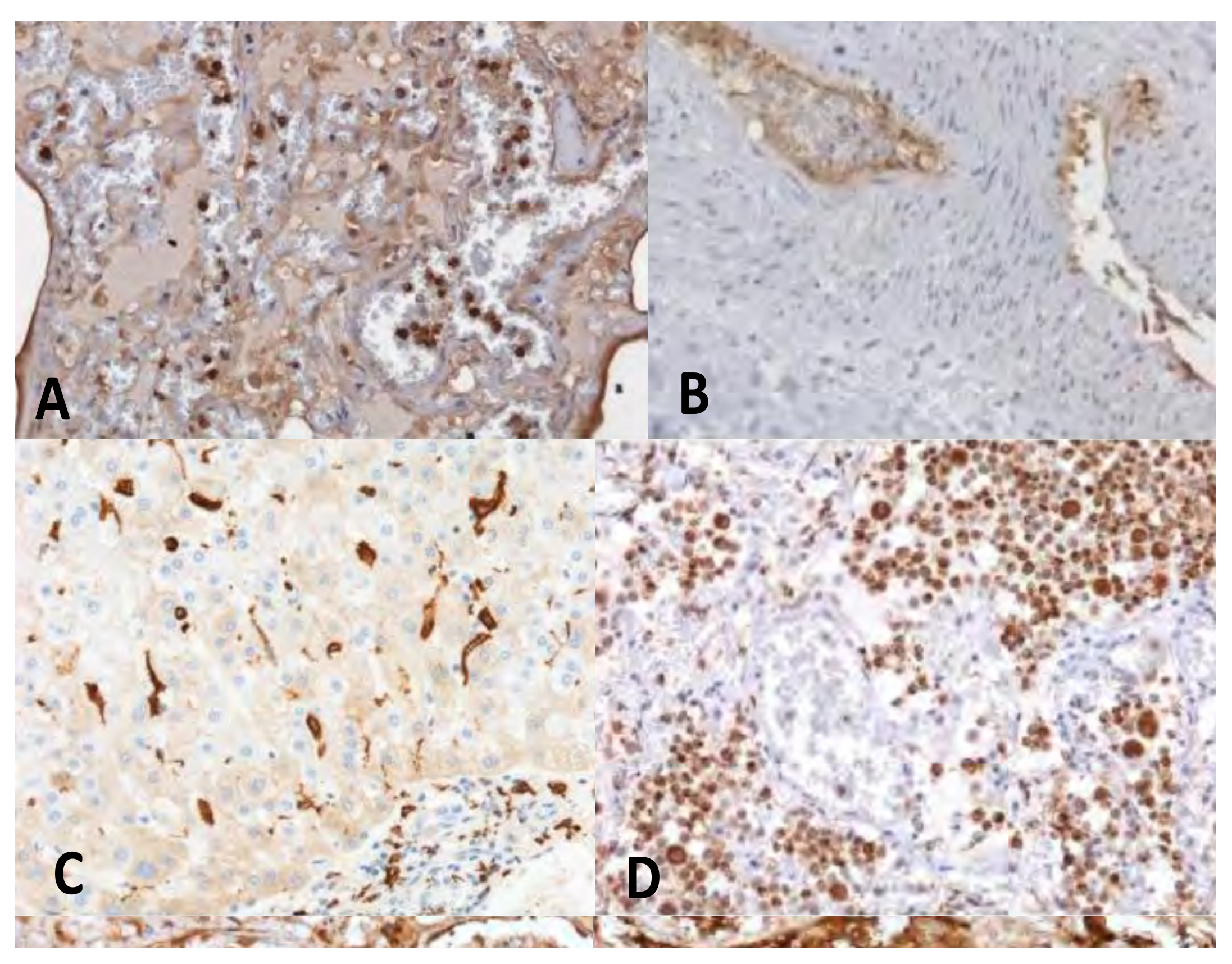
| IHC findings (Figure 3) | Immunohistochemistry showed at the level of the vascular and perivascular tissues of heart, lung, liver, kidney, ileum and deep veins, the expression of adhesion molecules (VICAM1) and activated inflammatory cells (CD66b+, CD 163, CD 61+) expressing the complement fraction C1r. At the endoluminal level the inflammatory cells appeared to be arranged in clusters with aggregated platelets. Finally, a massive deposition of immunoglobulins of the IgM and IgG classes was apparent in the same vascular and perivascular locations (Figure 3). | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pomara, C.; Sessa, F.; Ciaccio, M.; Dieli, F.; Esposito, M.; Giammanco, G.M.; Garozzo, S.F.; Giarratano, A.; Prati, D.; Rappa, F.; et al. COVID-19 Vaccine and Death: Causality Algorithm According to the WHO Eligibility Diagnosis. Diagnostics 2021, 11, 955. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11060955
Pomara C, Sessa F, Ciaccio M, Dieli F, Esposito M, Giammanco GM, Garozzo SF, Giarratano A, Prati D, Rappa F, et al. COVID-19 Vaccine and Death: Causality Algorithm According to the WHO Eligibility Diagnosis. Diagnostics. 2021; 11(6):955. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11060955
Chicago/Turabian StylePomara, Cristoforo, Francesco Sessa, Marcello Ciaccio, Francesco Dieli, Massimiliano Esposito, Giovanni Maurizio Giammanco, Sebastiano Fabio Garozzo, Antonino Giarratano, Daniele Prati, Francesca Rappa, and et al. 2021. "COVID-19 Vaccine and Death: Causality Algorithm According to the WHO Eligibility Diagnosis" Diagnostics 11, no. 6: 955. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11060955