
Overexpressed Proteins in HCC Cell-Derived Exosomes, CCT8, and Cofilin-1 Are Potential Biomarkers for Patients with HCC

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. HCC Cell Lines and Culture
2.2. Exosome Purification from Cell Culture Media and Patients’ Serum
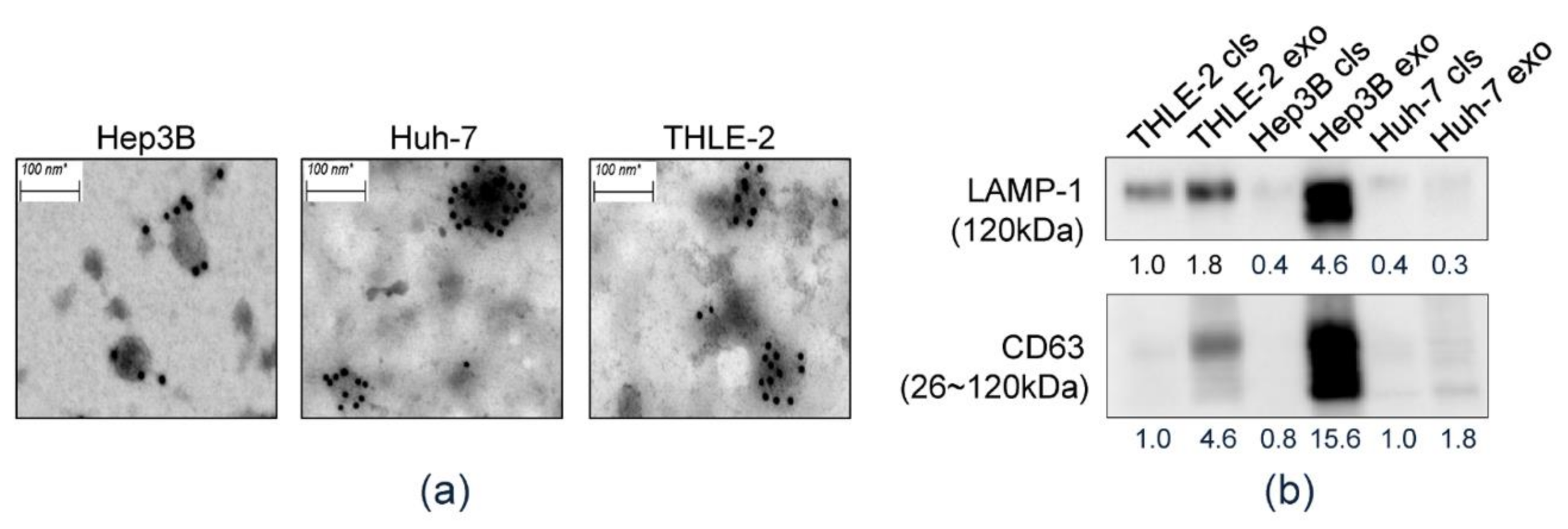
2.3. Transmission Electron Microscopy
2.4. Western Blot Analysis
2.5. Two-dimensional Gel Electrophoresis
2.6. Liquid Chromatography (LC)–Mass Spectrometry (MS)/MS For Peptides Analysis
2.7. ID Mapping and Gene Ontology (GO) Enrichment Analysis
2.8. Publicly Available Genomic Data Analysis
2.9. Quantitative Real-Time PCR (qRT-PCR)
2.10. Enzyme-Linked Immunosorbent Assay (ELISA)
2.11. Validation Cohort and Clinical Term Definitions
2.12. Statistical Analysis
3. Results
3.1. Isolation of HEX
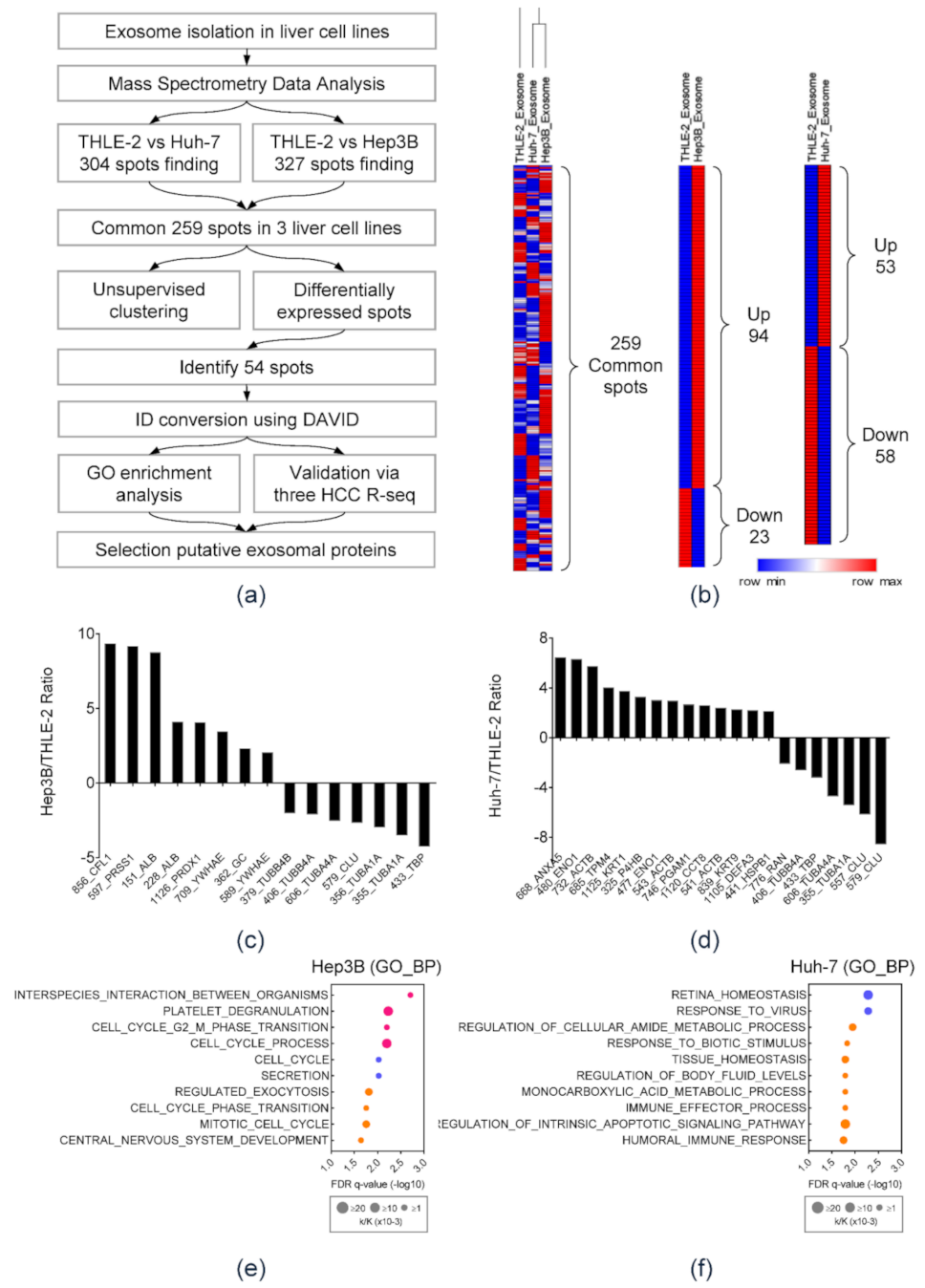
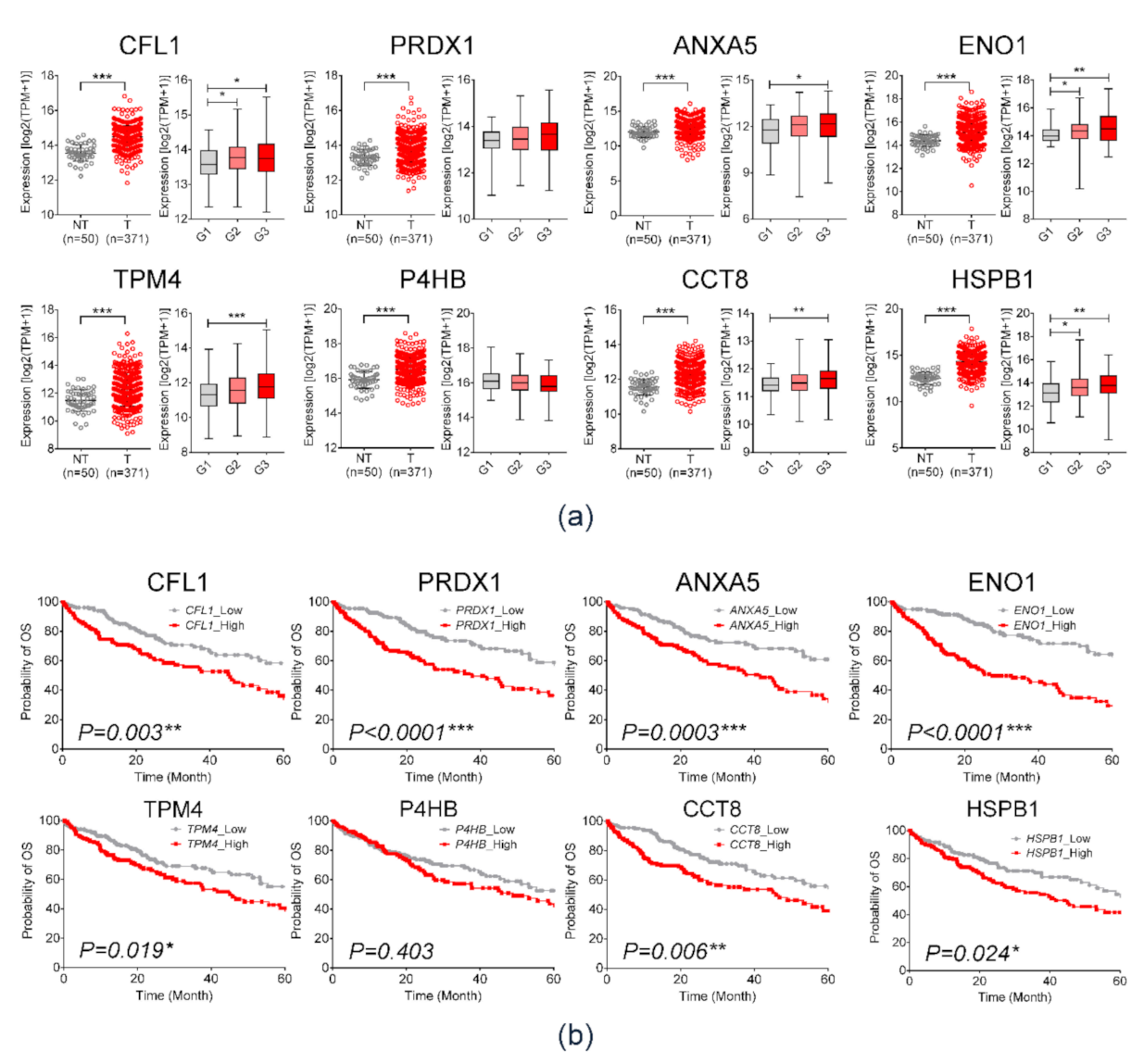
3.2. Mass Spectrometry Analysis and NGS RNA-seq Data Analysis of HCC-Derived Exosomal Protein Markers
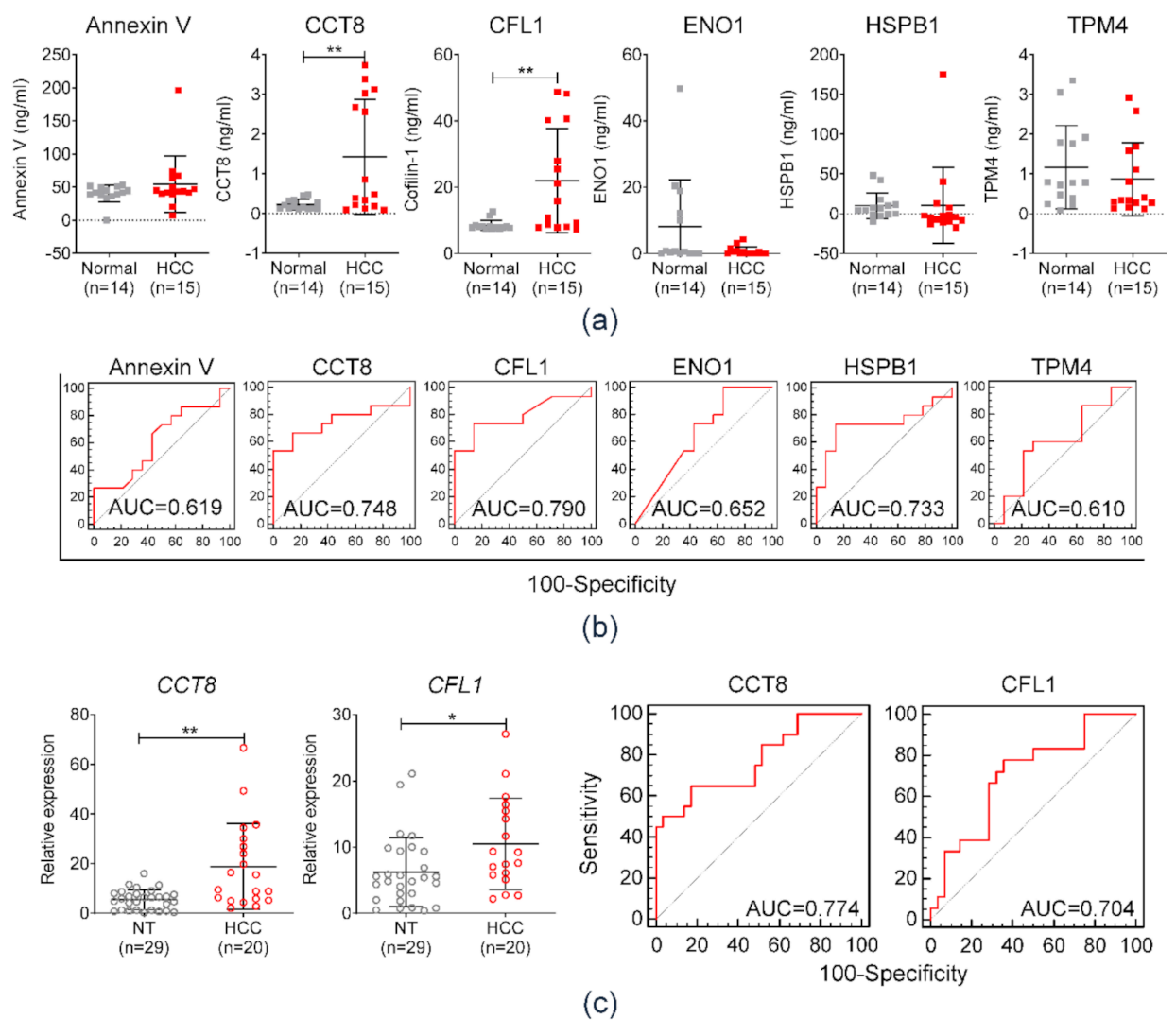
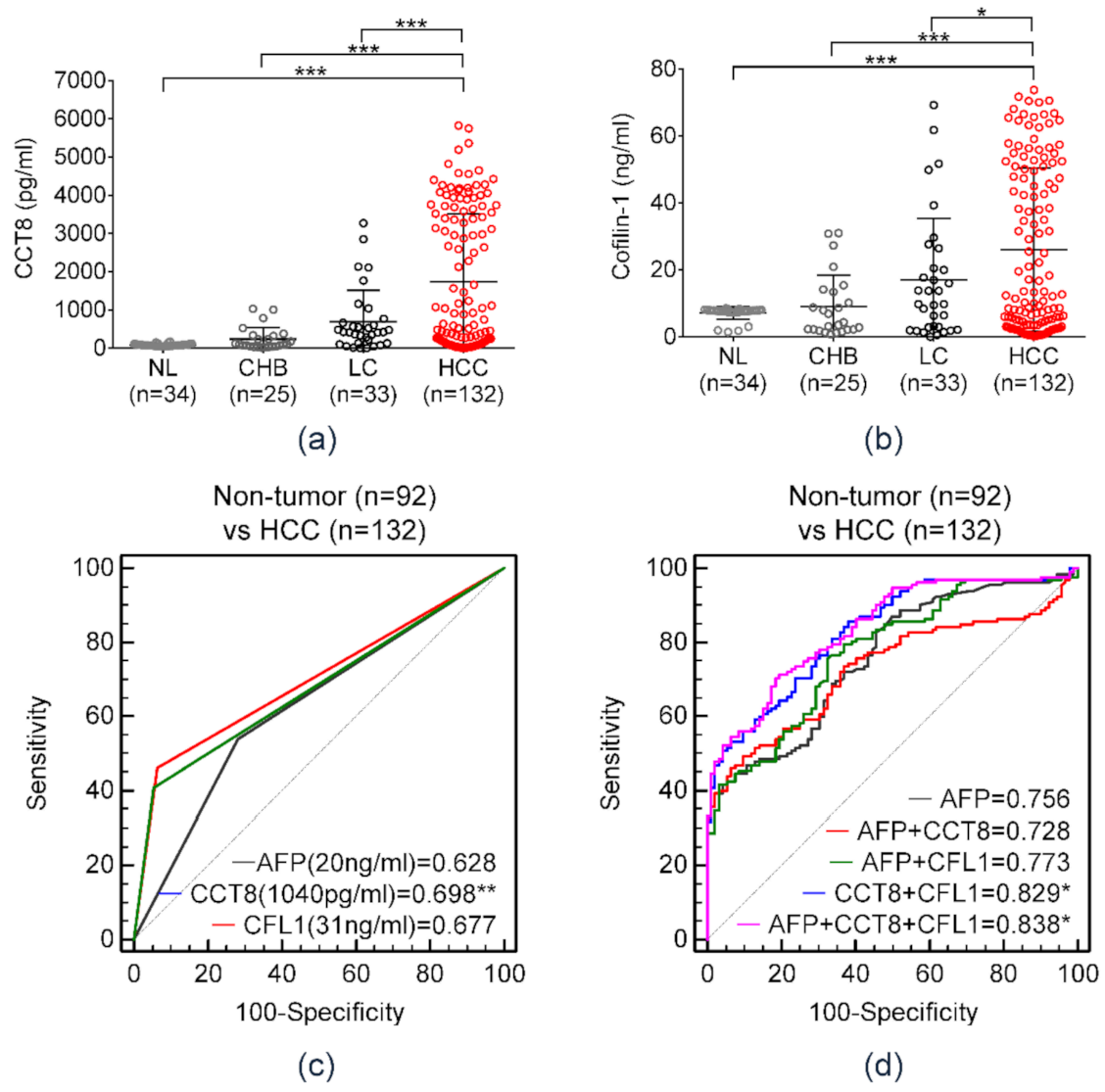
3.3. Diagnostic Performance of Serum Exosomal Protein Markers in the Test Set
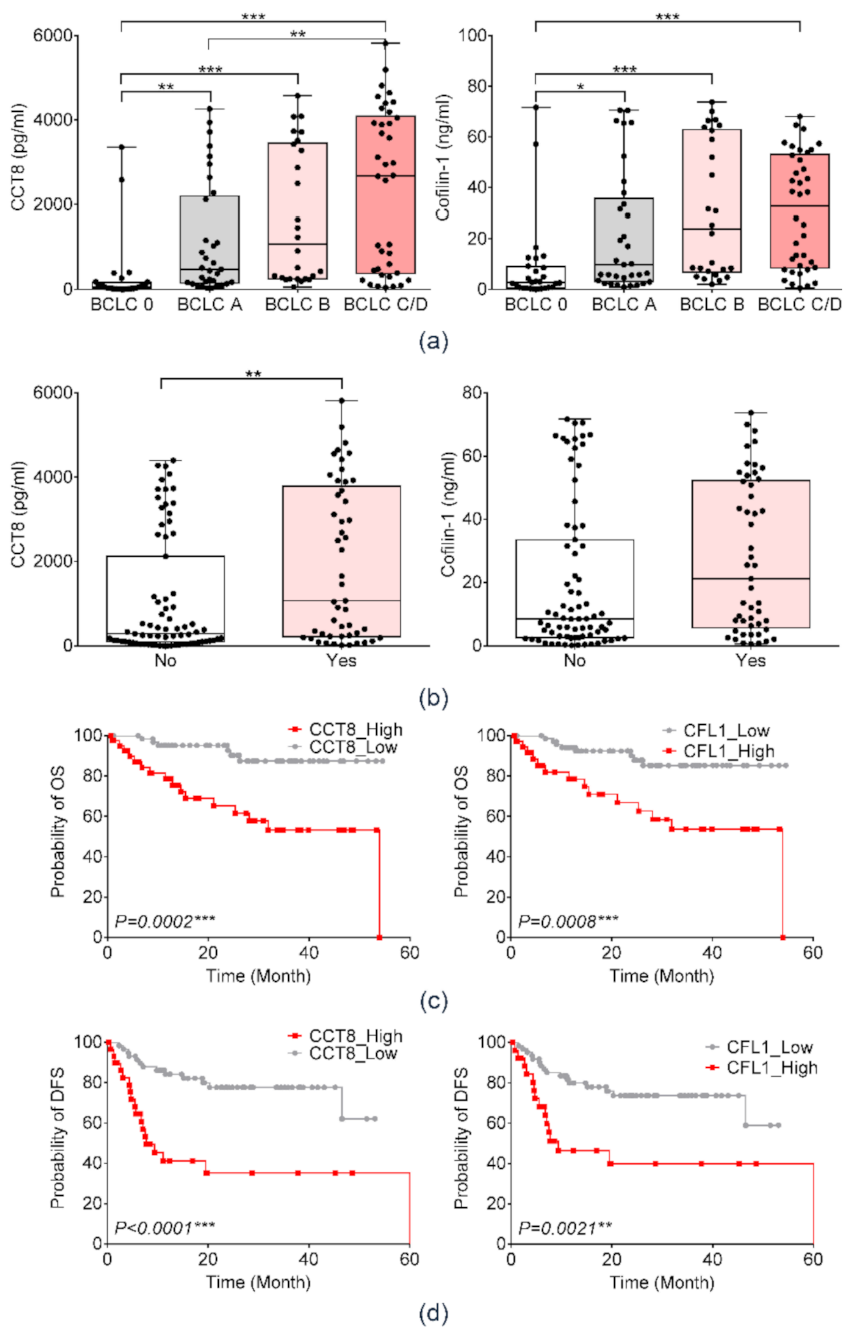
3.4. Clinical Relavance of Serum Protein Markers in the Validation Cohort
3.5. Prognostic Significance of Serum CFL1 and CCT8 in Patients With HCC
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ghouri, Y.A.; Mian, I.; Rowe, J.H. Review of hepatocellular carcinoma: Epidemiology, etiology, and carcinogenesis. J. Carcinog. 2017, 16, 1. [Google Scholar] [CrossRef]
- Yang, J.D.; Hainaut, P.; Gores, G.J.; Amadou, A.; Plymoth, A.; Roberts, L.R. A global view of hepatocellular carcinoma: Trends, risk, prevention and management. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 589–604. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.H.; Park, J.-W. Epidemiology of liver cancer in South Korea. Clin. Mol. Hepatol. 2018, 24, 1. [Google Scholar] [CrossRef] [PubMed]
- Cheung, A.H.-K.; Chow, C.; To, K.-F. Latest development of liquid biopsy. J. Thorac. Dis. 2018, 10, S1645. [Google Scholar] [CrossRef] [PubMed]
- Soung, Y.H.; Ford, S.; Zhang, V.; Chung, J. Exosomes in cancer diagnostics. Cancers 2017, 9, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jablonska, J.; Pietrowska, M.; Ludwig, S.; Lang, S.; Thakur, B.K. Challenges in the Isolation and Proteomic Analysis of Cancer Exosomes—Implications for Translational Research. Proteomes 2019, 7, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peterson, M.F.; Otoc, N.; Sethi, J.K.; Gupta, A.; Antes, T.J. Integrated systems for exosome investigation. Methods 2015, 87, 31–45. [Google Scholar] [CrossRef]
- Regev-Rudzki, N.; Wilson, D.W.; Carvalho, T.G.; Sisquella, X.; Coleman, B.M.; Rug, M.; Bursac, D.; Angrisano, F.; Gee, M.; Hill, A.F. Cell-cell communication between malaria-infected red blood cells via exosome-like vesicles. Cell 2013, 153, 1120–1133. [Google Scholar] [CrossRef] [Green Version]
- Miki, Y.; Yashiro, M.; Okuno, T.; Kuroda, K.; Togano, S.; Hirakawa, K.; Ohira, M. Clinico-pathological significance of exosome marker CD63 expression on cancer cells and stromal cells in gastric cancer. PLoS ONE 2018, 13, e0202956. [Google Scholar] [CrossRef] [Green Version]
- Park, K.S.; Kim, H.; Kim, N.G.; Cho, S.Y.; Choi, K.H.; Seong, J.K.; Paik, Y.K. Proteomic analysis and molecular characterization of tissue ferritin light chain in hepatocellular carcinoma. Hepatology 2002, 35, 1459–1466. [Google Scholar] [CrossRef]
- Cicinnati, V.R.; Shen, Q.; Sotiropoulos, G.C.; Radtke, A.; Gerken, G.; Beckebaum, S. Validation of putative reference genes for gene expression studies in human hepatocellular carcinoma using real-time quantitative RT-PCR. BMC Cancer 2008, 8, 350. [Google Scholar] [CrossRef] [Green Version]
- Korean Association for the Study of the Liver. KASL clinical practice guidelines for management of chronic hepatitis B. Clin. Mol. Hepatol. 2019, 25, 93. [Google Scholar] [CrossRef] [Green Version]
- Fukui, H.; Saito, H.; Ueno, Y.; Uto, H.; Obara, K.; Sakaida, I.; Shibuya, A.; Seike, M.; Nagoshi, S.; Segawa, M.; et al. Evidence-based clinical practice guidelines for liver cirrhosis 2015. J. Gastroenterol. 2016, 51, 629–650. [Google Scholar] [CrossRef] [Green Version]
- Kim, T.-H.; Kim, S.Y.; Tang, A.; Lee, J.M. Comparison of international guidelines for noninvasive diagnosis of hepatocellular carcinoma: 2018 update. Clin. Mol. Hepatol. 2019, 25, 245. [Google Scholar] [CrossRef] [Green Version]
- Heimbach, J.K.; Kulik, L.M.; Finn, R.S.; Sirlin, C.B.; Abecassis, M.M.; Roberts, L.R.; Zhu, A.X.; Murad, M.H.; Marrero, J.A. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology 2018, 67, 358–380. [Google Scholar] [CrossRef] [Green Version]
- Korean Liver Cancer Association. 2018 Korean Liver Cancer Association–National Cancer Center Korea Practice Guidelines for the Management of Hepatocellular Carcinoma. Gut Liver 2019, 13, 227. [Google Scholar] [CrossRef] [Green Version]
- Ayuso, C.; Rimola, J.; Vilana, R.; Burrel, M.; Darnell, A.; García-Criado, Á.; Bianchi, L.; Belmonte, E.; Caparroz, C.; Barrufet, M. Diagnosis and staging of hepatocellular carcinoma (HCC): Current guidelines. Eur. J. Radiol. 2018, 101, 72–81. [Google Scholar] [CrossRef]
- Bardelli, A.; Pantel, K. Liquid biopsies, what we do not know (yet). Cancer Cell 2017, 31, 172–179. [Google Scholar] [CrossRef] [Green Version]
- Whiteside, T.L. Tumor-derived exosomes and their role in cancer progression. In Advances in Clinical Chemistry; Elsevier: Amsterdam, The Netherlands, 2016; Volume 74, pp. 103–141. [Google Scholar]
- Pan, J.H.; Zhou, H.; Zhao, X.X.; Ding, H.; Li, W.; Qin, L.; Pan, Y.L. Role of exosomes and exosomal microRNAs in hepatocellular carcinoma: Potential in diagnosis and antitumour treatments. Int. J. Mol. Med. 2018, 41, 1809–1816. [Google Scholar] [CrossRef] [Green Version]
- Sohn, W.; Kim, J.; Kang, S.H.; Yang, S.R.; Cho, J.Y.; Cho, H.C.; Shim, S.G.; Paik, Y.H. Serum exosomal microRNAs as novel biomarkers for hepatocellular carcinoma. Exp. Mol. Med. 2015, 47, e184. [Google Scholar] [CrossRef]
- Jun, L.; Yang, G.; Zhisu, L. The utility of serum exosomal microRNAs in hepatocellular carcinoma. Biomed. Pharmacother. 2019, 111, 1221–1227. [Google Scholar] [CrossRef] [PubMed]
- He, M.; Qin, H.; Poon, T.C.; Sze, S.C.; Ding, X.; Co, N.N.; Ngai, S.M.; Chan, T.F.; Wong, N. Hepatocellular carcinoma-derived exosomes promote motility of immortalized hepatocyte through transfer of oncogenic proteins and RNAs. Carcinogenesis 2015, 36, 1008–1018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melo, S.A.; Luecke, L.B.; Kahlert, C.; Fernandez, A.F.; Gammon, S.T.; Kaye, J.; LeBleu, V.S.; Mittendorf, E.A.; Weitz, J.; Rahbari, N.; et al. Glypican-1 identifies cancer exosomes and detects early pancreatic cancer. Nature 2015, 523, 177–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moon, P.-G.; Lee, J.-E.; Cho, Y.-E.; Lee, S.J.; Jung, J.H.; Chae, Y.S.; Bae, H.-I.; Kim, Y.-B.; Kim, I.-S.; Park, H.Y. Identification of developmental endothelial locus-1 on circulating extracellular vesicles as a novel biomarker for early breast cancer detection. Clin. Cancer Res. 2016, 22, 1757–1766. [Google Scholar] [CrossRef] [Green Version]
- Huang, X.; Wang, X.; Cheng, C.; Cai, J.; He, S.; Wang, H.; Liu, F.; Zhu, C.; Ding, Z.; Huang, X. Chaperonin containing TCP 1, subunit 8 (CCT 8) is upregulated in hepatocellular carcinoma and promotes HCC proliferation. Apmis 2014, 122, 1070–1079. [Google Scholar]
- Wei, P.-L.; Huang, C.-Y.; Tai, C.-J.; Batzorig, U.; Cheng, W.-L.; Hunag, M.-T.; Chang, Y.-J. Glucose-regulated protein 94 mediates metastasis by CCT8 and the JNK pathway in hepatocellular carcinoma. Tumor Biol. 2016, 37, 8219–8227. [Google Scholar] [CrossRef]
- Collazo, J.; Zhu, B.; Larkin, S.; Martin, S.K.; Pu, H.; Horbinski, C.; Koochekpour, S.; Kyprianou, N. Cofilin drives cell-invasive and metastatic responses to TGF-β in prostate cancer. Cancer Res. 2014, 74, 2362–2373. [Google Scholar] [CrossRef] [Green Version]
- Liao, P.; Hsu, H.; Chen, T.; Chen, M.; Day, C.; Tu, C.; Lin, Y.; Tsai, F.-J.; Kuo, W.; Huang, C.-Y. Phosphorylation of cofilin-1 by ERK confers HDAC inhibitor resistance in hepatocellular carcinoma cells via decreased ROS-mediated mitochondria injury. Oncogene 2017, 36, 1978–1990. [Google Scholar] [CrossRef]
- Wang, Y.; Kuramitsu, Y.; Ueno, T.; Suzuki, N.; Yoshino, S.; Iizuka, N.; Zhang, X.; Oka, M.; Nakamura, K. Differential expression of up-regulated cofilin-1 and down-regulated cofilin-2 characteristic of pancreatic cancer tissues. Oncol. Rep. 2011, 26, 1595–1599. [Google Scholar]
- Shi, C.; Cai, Y.; Li, Y.; Li, Y.; Hu, N.; Ma, S.; Hu, S.; Zhu, P.; Wang, W.; Zhou, H. Yap promotes hepatocellular carcinoma metastasis and mobilization via governing cofilin/F-actin/lamellipodium axis by regulation of JNK/Bnip3/SERCA/CaMKII pathways. Redox Biol. 2018, 14, 59–71. [Google Scholar] [CrossRef]
- Estornes, Y.; Gay, F.; Gevrey, J.C.; Navoizat, S.; Nejjari, M.; Scoazec, J.Y.; Chayvialle, J.A.; Saurin, J.C.; Abello, J. Differential involvement of destrin and cofilin-1 in the control of invasive properties of Isreco1 human colon cancer cells. Int. J. Cancer 2007, 121, 2162–2171. [Google Scholar] [CrossRef]
- Peng, X.-C.; Gong, F.-M.; Zhao, Y.-W.; Zhou, L.-X.; Xie, Y.-W.; Liao, H.-L.; Lin, H.-J.; Li, Z.-Y.; Tang, M.-H.; Tong, A.-P. Comparative proteomic approach identifies PKM2 and cofilin-1 as potential diagnostic, prognostic and therapeutic targets for pulmonary adenocarcinoma. PLoS ONE 2011, 6, e27309. [Google Scholar] [CrossRef]
- Xu, Z.; Zhai, L.; Yi, T.; Gao, H.; Fan, F.; Li, Y.; Wang, Y.; Li, N.; Xing, X.; Su, N. Hepatitis B virus X induces inflammation and cancer in mice liver through dysregulation of cytoskeletal remodeling and lipid metabolism. Oncotarget 2016, 7, 70559. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Validation Cohort | |||
|---|---|---|---|---|
| Normal (n = 34) | CHB (n = 25) | LC (n = 33) | HCC (n = 132) | |
| Age (years), mean ± SD | 34.2 ± 7.5 | 45.2 ± 11.2 | 53.0 ± 9.9 | 55.2 ± 9.02 |
| Male sex, n (%) | 4 (11.8) | 18 (72) | 19 (57.6) | 109 (74.1) |
| AST, IU/ml | 19.60 ±5.46 | 50.44 ± 51.40 | 79.19 ± 100.91 | 71.57 ± 96.77 |
| ALT, IU/ml | 20.00 ± 15.12 | 57.26 ± 66.30 | 77.25 ± 100.99 | 48.12 ± 59.28 |
| Platelet, ×109/L | 290.40 ± 42.17 | 190.56 ± 44.38 | 123.35 ± 65.59 | 166.44 ± 84.17 |
| AFP (ng/mL), mean ± SD | 1.71 ± 0.76 | 17.55 ± 24.96 | 49.94 ± 104.09 | 4290.43 ± 14525.79 |
| Etiology, n HBV/HCV/alcohol/others | 28/3/2/0 | 108/7/4/13 | ||
| Albumin (g/L), mean ± SD | 4.56 ± 0.41 | 4.05 ± 0.53 | 4.28 ± 0.55 | |
| Bilirubin (mg/dL) mean ± SD | 0.81 ± 0.32 | 1.05 ± 1.03 | 1.34 ± 3.53 | |
| INR, mean ± SD | 1.23 ± 0.30 | 1.24 ± 0.11 | 1.25 ± 0.55 | |
| Modified UICC stage, I/II/III/IVa/Ivb, n (%) | 26 (19.7)/32(23.8)/24(18.2)/45(34.1)/5(3.8) | |||
| HCC vs. Non-Tumor (Normal, CHB, and LC) | |||||||
|---|---|---|---|---|---|---|---|
| p vs AFP | AUC | 95% CI | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | |
| AFP (>20 ng/mL) | 1 | 0.628 | 0.651–0.691 | 53.79 | 71.74 | 73.12 | 51.97 |
| CCT8 (>1040 pg/mL) | 0.0095 | 0.698 | 0.634–0.758 | 46.21 | 93.48 | 58.93 | 91.05 |
| CFL1 (>31 ng/mL) | 0.0758 | 0.677 | 0.612–0.738 | 40.91 | 94.57 | 91.53 | 52.73 |
| HCC vs. Non-Tumor (Normal, CHB, and LC) | ||||||||
|---|---|---|---|---|---|---|---|---|
| p vs. AFP | Cut-Off | AUC | 95% CI | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | |
| AFP + CCT8 | 0.169 | 0.6106 | 0.728 | 0.664–0.785 | 46.21 | 93.48 | 91.05 | 54.77 |
| AFP + CFL1 | 0.444 | 0.4704 | 0.773 | 0.712–0.826 | 75.76 | 67.39 | 76.92 | 65.96 |
| CCT8 + CFL1 | 0.045 | 0.4434 | 0.829 | 0.773–0.876 | 85.61 | 61.96 | 76.35 | 75.00 |
| AFP + CCT8 + CFL1 | 0.027 | 0.5438 | 0.838 | 0.783–0.884 | 70.46 | 81.52 | 84.55 | 65.79 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, H.J.; Baek, G.O.; Yoon, M.G.; Ahn, H.R.; Son, J.A.; Kim, S.S.; Cheong, J.Y.; Eun, J.W. Overexpressed Proteins in HCC Cell-Derived Exosomes, CCT8, and Cofilin-1 Are Potential Biomarkers for Patients with HCC. Diagnostics 2021, 11, 1221. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11071221
Cho HJ, Baek GO, Yoon MG, Ahn HR, Son JA, Kim SS, Cheong JY, Eun JW. Overexpressed Proteins in HCC Cell-Derived Exosomes, CCT8, and Cofilin-1 Are Potential Biomarkers for Patients with HCC. Diagnostics. 2021; 11(7):1221. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11071221
Chicago/Turabian StyleCho, Hyo Jung, Geum Ok Baek, Moon Gyeong Yoon, Hye Ri Ahn, Ju A Son, Soon Sun Kim, Jae Youn Cheong, and Jung Woo Eun. 2021. "Overexpressed Proteins in HCC Cell-Derived Exosomes, CCT8, and Cofilin-1 Are Potential Biomarkers for Patients with HCC" Diagnostics 11, no. 7: 1221. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11071221