
Molecular RNA Correlates of the SOFA Score in Patients with Sepsis

 , , ,
, , ,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Calculation of the SOFA Score
2.2. Time Points of Measurement, Sample Collection, and Patient Data
2.3. Inclusion and Exclusion Criteria of Patients
2.4. Bioinformatic Analysis
2.5. Statistical Analysis
2.6. Ethics Approval and Patient Consent for Study Participation
3. Results
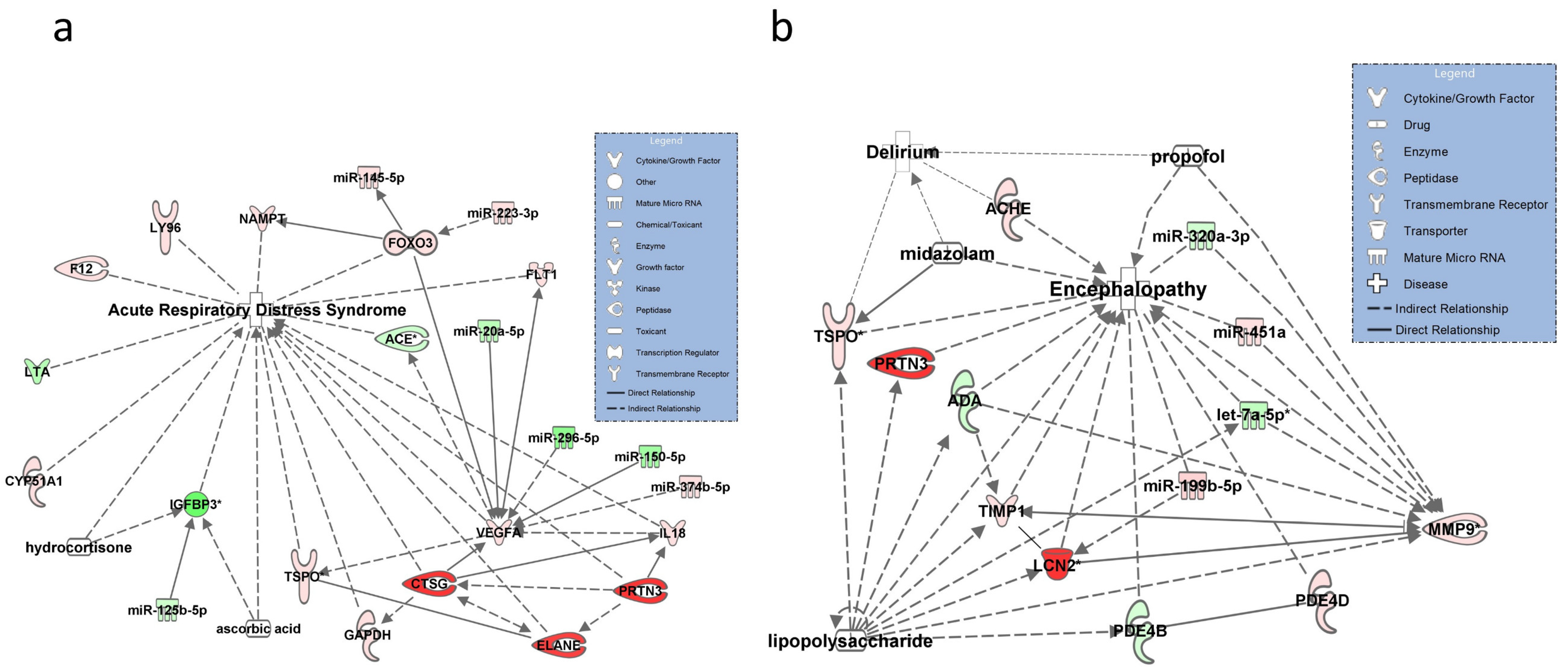
3.1. Networks for SOFA Criterion 1: Hypoxia
3.2. Networks for SOFA Criterion 2: Glasgow Coma Scale
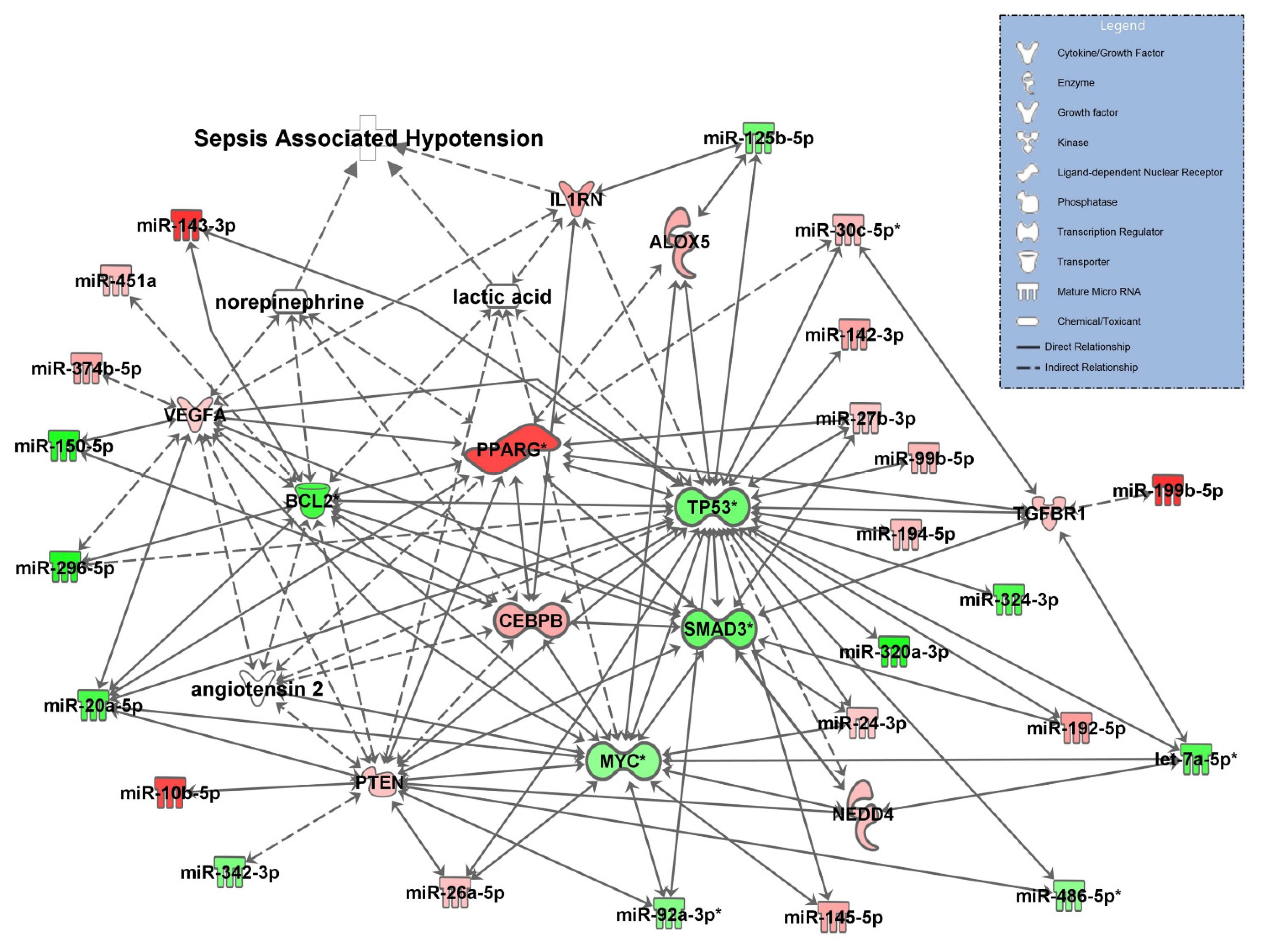
3.3. Network for SOFA Criterion 3: Circulatory Failure
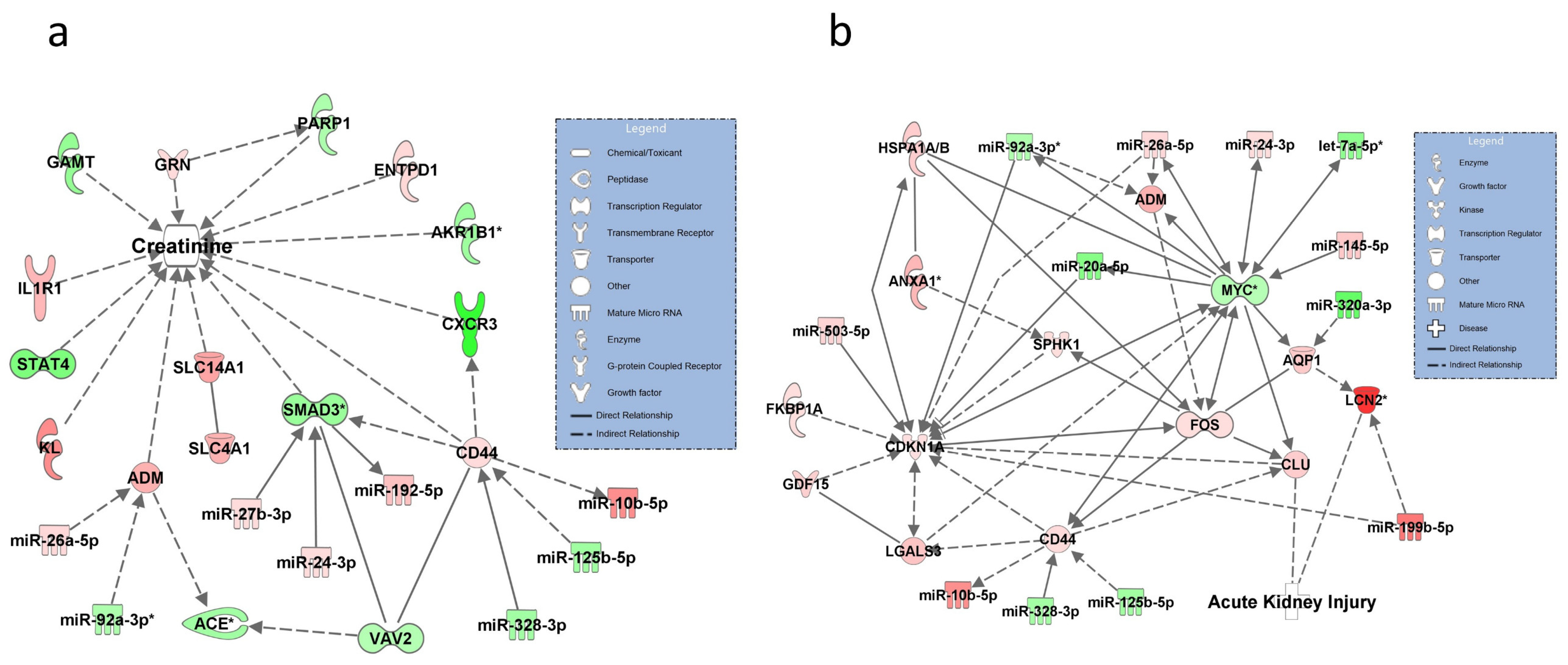
3.4. Networks for SOFA Criterion 4: Increase in Serum Creatinine
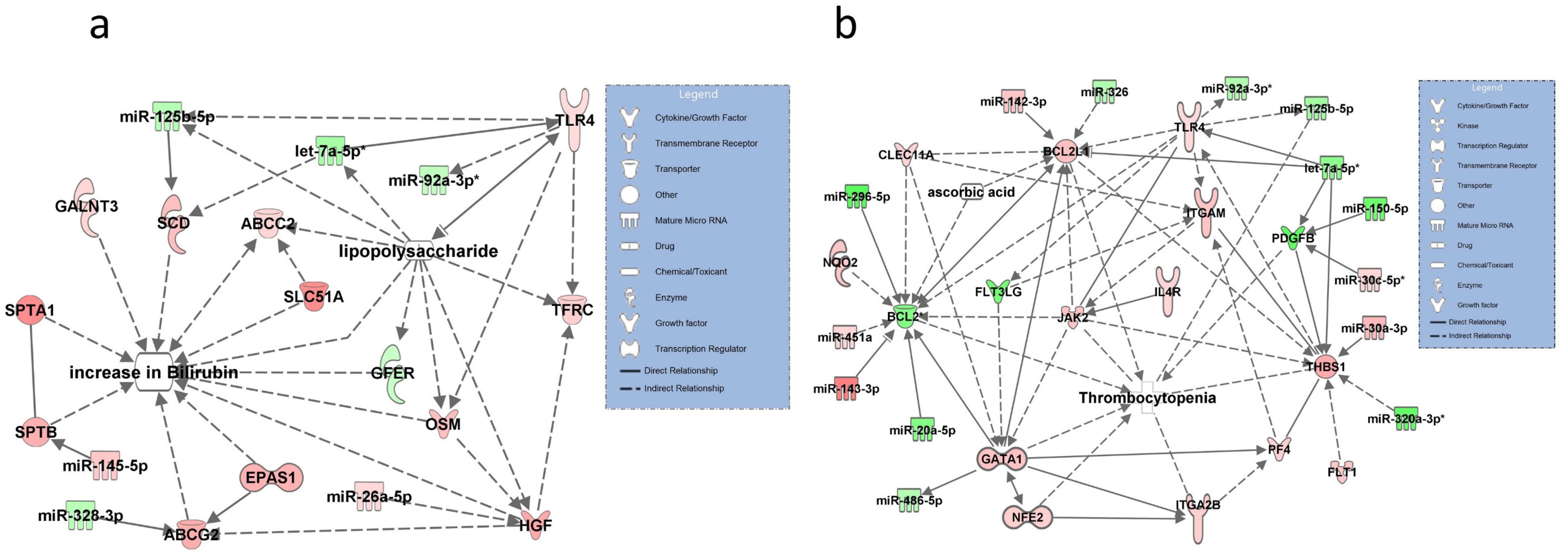
3.5. Networks for SOFA Criterion 5: Increase in Bilirubin
3.6. Networks for SOFA Criterion 6: Low Platelet Count
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ABCG2 | ATP-binding cassette super-family G member 2 |
| ACE | angiotensin converting enzyme |
| ACHE | acetylcholinesterase |
| ADM | adrenomedullin |
| AKR1B1 | aldose reductase |
| ANXA1 | lipocortin I |
| AQP1 | aquaporin 1 |
| BCL2 | apoptosis regulator |
| CEBPB | nuclear factor of IL-6 expression |
| CLU | clusterin |
| CYR5A1 | nicotinamide phosphoribosyltransferase |
| EPAS1 | hypoxia-inducible factor-2 alpha |
| F12 | coagulation factor XII |
| FOS | fos proto-oncogene, AP-1 transcription factor subunit |
| GATA 1 | GATA binding protein 1 |
| IGFBP3 | insulin like growth factor binding protein 3 |
| IL1RN | interleukin 1 receptor antagonist |
| ITGA 2b | integrin alpha 2B |
| JAK2 | janus kinase 2 |
| KL | Klotho |
| LNC2 | lipocalin 2, NGAL |
| LTA | Lymphotoxin alpha |
| LY96 | lymphocyte antigen 96 |
| MMP9 | matrix metalloproteinase-9 |
| MYC | bHLH transcription factor |
| NAMPT | nicotinamide phosphoribosyltransferase |
| PDE4B | cAMP-specific 3′,5′-cyclic phosphodiesterase 4B |
| PDGFB | platelet derived growth factor subunit B |
| PF4 | platelet factor 4 |
| PPARG | peroxisome proliferator activated receptor gamma |
| PTEN | phosphatase and tensin homolog |
| SCID | stearoyl-CoA desaturase |
| SMAD3 | SMAD family 3 |
| SPHK1 | sphingosine kinase 1 |
| THBS1 | thrombospondin 1 |
| TIMP1 | TIMP metallopeptidase inhibitor 1 |
| TLR4 | toll-like receptor 4 |
| TP53 | tumor protein 53 |
| TSPO | translocator protein/peripheral-type benzodiazepine receptor |
| EGFA | vascular endothelial growth factor A |
| VGFA | vascular growth factor A |
References
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonca, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef]
- Seymour, C.W.; Liu, V.X.; Iwashyna, T.J.; Brunkhorst, F.M.; Rea, T.D.; Scherag, A.; Rubenfeld, G.; Kahn, J.M.; Shankar-Hari, M.; Singer, M.; et al. Assessment of Clinical Criteria for Sepsis: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 762–774. [Google Scholar] [CrossRef] [Green Version]
- Lambden, S.; Laterre, P.F.; Levy, M.M.; Francois, B. The SOFA score-development, utility and challenges of accurate assessment in clinical trials. Crit. Care 2019, 23, 374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vincent, J.L.; de Mendonca, A.; Cantraine, F.; Moreno, R.; Takala, J.; Suter, P.M.; Sprung, C.L.; Colardyn, F.; Blecher, S. Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: Results of a multicenter, prospective study. Working group on “sepsis-related problems” of the European Society of Intensive Care Medicine. Crit. Care Med. 1998, 26, 1793–1800. [Google Scholar] [CrossRef] [PubMed]
- Reithmair, M.; Buschmann, D.; Marte, M.; Kirchner, B.; Hagl, D.; Kaufmann, I.; Pfob, M.; Chouker, A.; Steinlein, O.K.; Pfaffl, M.W.; et al. Cellular and extracellular miRNAs are blood-compartment-specific diagnostic targets in sepsis. J. Cell. Mol. Med. 2017, 21, 2403–2411. [Google Scholar] [CrossRef] [PubMed]
- Shankar-Hari, M.; Phillips, G.S.; Levy, M.L.; Seymour, C.W.; Liu, V.X.; Deutschman, C.S.; Angus, D.C.; Rubenfeld, G.D.; Singer, M.; Sepsis Definitions Task, F. Developing a New Definition and Assessing New Clinical Criteria for Septic Shock: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 775–787. [Google Scholar] [CrossRef] [PubMed]
- Kramer, A.; Green, J.; Pollard, J., Jr.; Tugendreich, S. Causal analysis approaches in Ingenuity Pathway Analysis. Bioinformatics 2014, 30, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Schnapp, L.M.; Donohoe, S.; Chen, J.; Sunde, D.A.; Kelly, P.M.; Ruzinski, J.; Martin, T.; Goodlett, D.R. Mining the acute respiratory distress syndrome proteome: Identification of the insulin-like growth factor (IGF)/IGF-binding protein-3 pathway in acute lung injury. Am. J. Pathol. 2006, 169, 86–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahasic, A.M.; Zhai, R.; Su, L.; Zhao, Y.; Aronis, K.N.; Thompson, B.T.; Mantzoros, C.S.; Christiani, D.C. IGF1 and IGFBP3 in acute respiratory distress syndrome. Eur. J. Endocrinol. 2012, 166, 121–129. [Google Scholar] [CrossRef] [Green Version]
- Kang, S.S.; Ren, Y.; Liu, C.C.; Kurti, A.; Baker, K.E.; Bu, G.; Asmann, Y.; Fryer, J.D. Lipocalin-2 protects the brain during inflammatory conditions. Mol. Psychiatry 2018, 23, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Pinelli, A.; Trivulzio, S.; Rossoni, G.; Redaelli, R.; Brenna, S. Factors involved in sudden coagulation observed in patients with acute myocardial infarction. Vivo 2012, 26, 1021–1025. [Google Scholar]
- Zhang, J.; Zhang, D.; Wu, G.Q.; Feng, Z.Y.; Zhu, S.M. Propofol inhibits the adhesion of hepatocellular carcinoma cells by upregulating microRNA-199a and downregulating MMP-9 expression. Hepatobiliary Pancreat. Dis. Int. 2013, 12, 305–309. [Google Scholar] [CrossRef]
- Shi, S.S.; Zhang, H.B.; Wang, C.H.; Yang, W.Z.; Liang, R.S.; Chen, Y.; Tu, X.K. Propofol Attenuates Early Brain Injury after Subarachnoid Hemorrhage in Rats. J. Mol. Neurosci. 2015, 57, 538–545. [Google Scholar] [CrossRef] [PubMed]
- Qiu, Z.K.; Li, M.S.; He, J.L.; Liu, X.; Zhang, G.H.; Lai, S.; Ma, J.C.; Zeng, J.; Li, Y.; Wu, H.W.; et al. Translocator protein mediates the anxiolytic and antidepressant effects of midazolam. Pharmacol. Biochem. Behav. 2015, 139 Pt A, 77–83. [Google Scholar] [CrossRef]
- Horiguchi, Y.; Ohta, N.; Yamamoto, S.; Koide, M.; Fujino, Y. Midazolam suppresses the lipopolysaccharide-stimulated immune responses of human macrophages via translocator protein signaling. Int. Immunopharmacol. 2019, 66, 373–382. [Google Scholar] [CrossRef] [PubMed]
- Mokrov, G.V.; Deeva, O.A.; Gudasheva, T.A. The Ligands of Translocator Protein: Design and Biological Properties. Curr. Pharm. Des. 2021, 27, 217–237. [Google Scholar] [CrossRef] [PubMed]
- Meng, Y.; Tian, M.; Yin, S.; Lai, S.; Zhou, Y.; Chen, J.; He, M.; Liao, Z. Downregulation of TSPO expression inhibits oxidative stress and maintains mitochondrial homeostasis in cardiomyocytes subjected to anoxia/reoxygenation injury. Biomed. Pharmacother. 2020, 121, 109588. [Google Scholar] [CrossRef] [PubMed]
- Fischer, J.E.; Benn, A.; Harbarth, S.; Nadal, D.; Fanconi, S. Diagnostic accuracy of G-CSF, IL-8, and IL-1ra in critically ill children with suspected infection. Intensive Care Med. 2002, 28, 1324–1331. [Google Scholar] [CrossRef]
- Dinarello, C.A. Biologic basis for interleukin-1 in disease. Blood 1996, 87, 2095–2147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Opal, S.M.; Fisher, C.J., Jr.; Dhainaut, J.F.; Vincent, J.L.; Brase, R.; Lowry, S.F.; Sadoff, J.C.; Slotman, G.J.; Levy, H.; Balk, R.A.; et al. Confirmatory interleukin-1 receptor antagonist trial in severe sepsis: A phase III, randomized, double-blind, placebo-controlled, multicenter trial. The Interleukin-1 Receptor Antagonist Sepsis Investigator Group. Crit. Care Med. 1997, 25, 1115–1124. [Google Scholar] [CrossRef] [PubMed]
- Nakada, T.A.; Takahashi, W.; Nakada, E.; Shimada, T.; Russell, J.A.; Walley, K.R. Genetic Polymorphisms in Sepsis and Cardiovascular Disease: Do Similar Risk Genes Suggest Similar Drug Targets? Chest 2019, 155, 1260–1271. [Google Scholar] [CrossRef]
- Antunes, B.M.; Rosa-Neto, J.C.; Batatinha, H.A.P.; Franchini, E.; Teixeira, A.M.; Lira, F.S. Physical fitness status modulates the inflammatory proteins in peripheral blood and circulating monocytes: Role of PPAR-gamma. Sci. Rep. 2020, 10, 14094. [Google Scholar] [CrossRef]
- Jadhav, A.P.; Sadaka, F.G. Angiotensin II in septic shock. Am. J. Emerg. Med. 2019, 37, 1169–1174. [Google Scholar] [CrossRef]
- Alexis, J.D.; Wang, N.; Che, W.; Lerner-Marmarosh, N.; Sahni, A.; Korshunov, V.A.; Zou, Y.; Ding, B.; Yan, C.; Berk, B.C.; et al. Bcr kinase activation by angiotensin II inhibits peroxisome-proliferator-activated receptor gamma transcriptional activity in vascular smooth muscle cells. Circ. Res. 2009, 104, 69–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, J.; Devalaraja-Narashimha, K.; Singaravelu, K.; Padanilam, B.J. Poly(ADP-ribose) polymerase-1 gene ablation protects mice from ischemic renal injury. Am. J. Physiol.-Renal Physiol. 2005, 288, F387–F398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haq, M.; Norman, J.; Saba, S.R.; Ramirez, G.; Rabb, H. Role of IL-1 in renal ischemic reperfusion injury. J. Am. Soc. Nephrol. 1998, 9, 614–619. [Google Scholar] [CrossRef] [PubMed]
- Hultström, M.; Becirovic-Agic, M.; Jönsson, S. Comparison of acute kidney injury of different etiology reveals in-common mechanisms of tissue damage. Physiol. Genom. 2018, 50, 127–141. [Google Scholar] [CrossRef] [PubMed]
- Moschen, A.R.; Adolph, T.E.; Gerner, R.R.; Wieser, V.; Tilg, H. Lipocalin-2: A Master Mediator of Intestinal and Metabolic Inflammation. Trends Endocrinol. Metab. 2017, 28, 388–397. [Google Scholar] [CrossRef] [PubMed]
- Makris, K.; Rizos, D.; Kafkas, N.; Haliassos, A. Neurophil gelatinase-associated lipocalin as a new biomarker in laboratory medicine. Clin. Chem. Lab. Med. 2012, 50, 1519–1532. [Google Scholar] [CrossRef]
- Guo, Q.M.; Malek, R.L.; Kim, S.; Chiao, C.; He, M.; Ruffy, M.; Sanka, K.; Lee, N.H.; Dang, C.V.; Liu, E.T. Identification of c-myc responsive genes using rat cDNA microarray. Cancer Res. 2000, 60, 5922–5928. [Google Scholar]
- Stanek, C.; Reinhardt, N.; Diesing, A.K.; Nossol, C.; Kahlert, S.; Panther, P.; Kluess, J.; Rothkötter, H.J.; Kuester, D.; Brosig, B.; et al. A chronic oral exposure of pigs with deoxynivalenol partially prevents the acute effects of lipopolysaccharides on hepatic histopathology and blood clinical chemistry. Toxicol. Lett. 2012, 215, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Marino, G.; Rustgi, V.K.; Salzberg, G.; Johnson, L.B.; Kuo, P.C.; Plotkin, J.S.; Flockhart, D.A. Pharmacokinetics and biochemical effects of hepapoietin in patients with chronic liver disease. Aliment. Pharmacol. Ther. 2002, 16, 235–242. [Google Scholar] [CrossRef]
- Vodovotz, Y.; Prelich, J.; Lagoa, C.; Barclay, D.; Zamora, R.; Murase, N.; Gandhi, C.R. Augmenter of liver regeneration (ALR) is a novel biomarker of hepatocellular stress/inflammation: In vitro, in vivo and in silico studies. Mol. Med. 2013, 18, 1421–1429. [Google Scholar] [CrossRef] [PubMed]
- Levéen, P.; Pekny, M.; Gebre-Medhin, S.; Swolin, B.; Larsson, E.; Betsholtz, C. Mice deficient for PDGF B show renal, cardiovascular, and hematological abnormalities. Genes Dev. 1994, 8, 1875–1887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Labbaye, C.; Quaranta, M.T.; Pagliuca, A.; Militi, S.; Licht, J.D.; Testa, U.; Peschle, C. PLZF induces megakaryocytic development, activates Tpo receptor expression and interacts with GATA1 protein. Oncogene 2002, 21, 6669–6679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lorenz, R.; Brauer, M. Platelet factor 4 (PF4) in septicaemia. Infection 1988, 16, 273–276. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SOFA Criteria | Clinical Condition | Bioinformatic Correlate | Selected Pharmacologic Intervention (Drugs and Compounds) | Canonical Pathway (Figure) |
|---|---|---|---|---|
| PaO2/FiO2 ratio | Hypoxia | Pulmonary capillary leak syndrome, ARDS2 | Ascorbic acid, hydrocortisone | Figure 2a |
| Glasgow Coma Scale | Impaired cognition | Encephalopathy, delirium | Midazolam, propofol, lipopolysaccharide | Figure 2b |
| Mean arterial blood pressure | Hypotension | Cardiovascular signaling in sepsis | Norepinephrine, angiotensin II, lactic acide | Figure 3 |
| Vasopressor administration | Circulatory failure | Norepinephrine, angiotensin II, lactate | ||
| Creatinine | Acute kidney injury | Increase in serum creatinine, acute kidney injury | Figure 4a,b | |
| Bilirubin | Acute liver failure | Increase in bilirubin | Lipopolysaccharide | Figure 5a |
| Platelet count | Coagulopathy | Low platelet count | Ascorbic acid | Figure 5b |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meidert, A.S.; Buschmann, D.; Brandes, F.; Kanev, K.; Billaud, J.-N.; Borrmann, M.; Witte, M.; Kirchner, B.; Reithmair, M.; Pfaffl, M.W.; et al. Molecular RNA Correlates of the SOFA Score in Patients with Sepsis. Diagnostics 2021, 11, 1649. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11091649
Meidert AS, Buschmann D, Brandes F, Kanev K, Billaud J-N, Borrmann M, Witte M, Kirchner B, Reithmair M, Pfaffl MW, et al. Molecular RNA Correlates of the SOFA Score in Patients with Sepsis. Diagnostics. 2021; 11(9):1649. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11091649
Chicago/Turabian StyleMeidert, Agnes S., Dominik Buschmann, Florian Brandes, Kristiyan Kanev, Jean-Noël Billaud, Melanie Borrmann, Matthias Witte, Benedikt Kirchner, Marlene Reithmair, Michael W. Pfaffl, and et al. 2021. "Molecular RNA Correlates of the SOFA Score in Patients with Sepsis" Diagnostics 11, no. 9: 1649. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11091649