
Do We Really Need Hazard Prevention at the Expense of Safeguarding Death Dignity in COVID-19?

 ,
,  ,
,  , ,
, , 
 and
and
Abstract
:1. Introduction
2. Materials and Methods
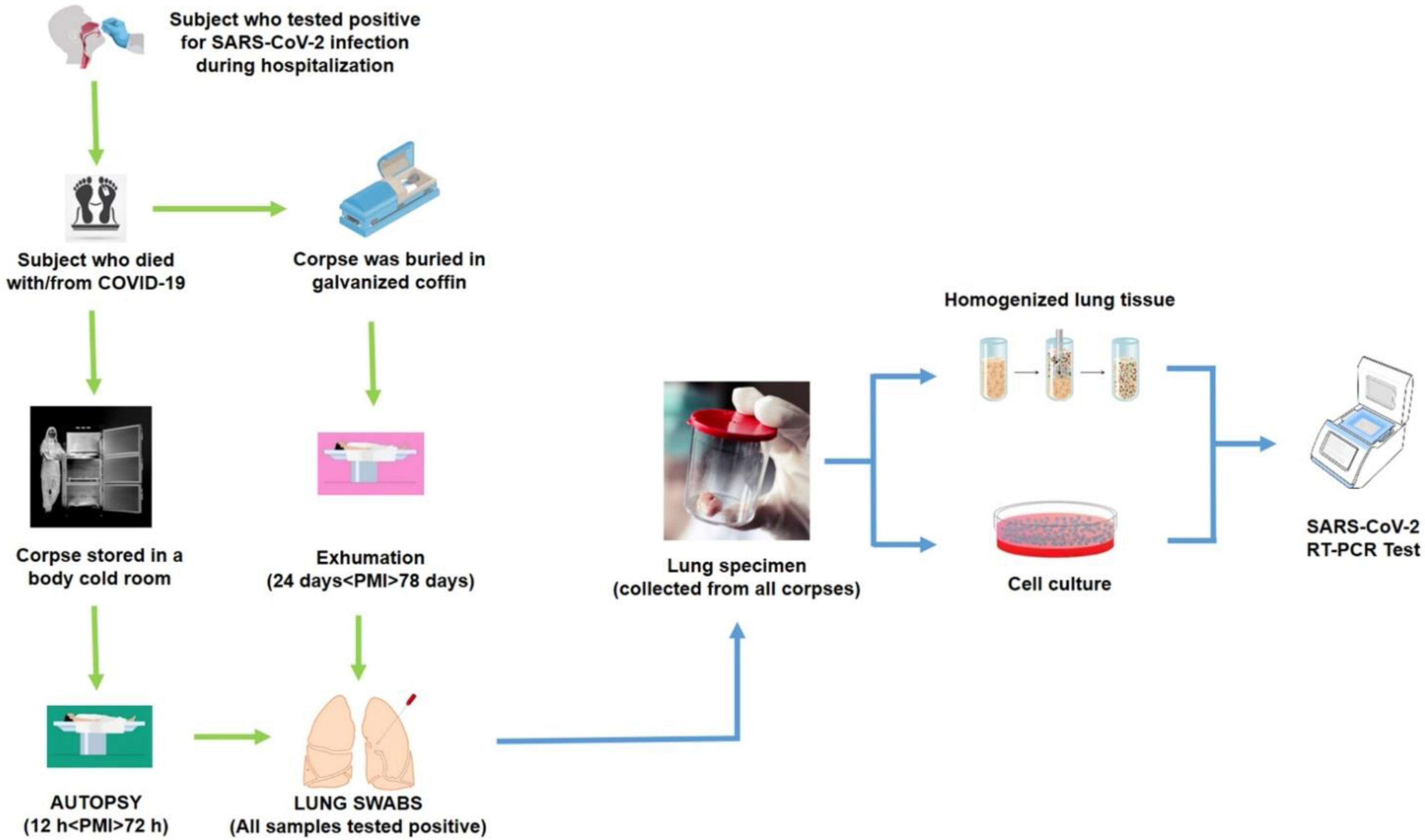
2.1. Patients, Autopsies and Sample Collection
2.2. Virus Isolation
2.3. RT-PCR
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shastri, J.; Parikh, S.; Aggarwal, V.; Agrawal, S.; Chatterjee, N.; Shah, R.; Devi, P.; Mehta, P.; Pandey, R. Severe SARS-CoV-2 Breakthrough Reinfection with Delta Variant After Recovery From Breakthrough Infection by Alpha Variant in a Fully Vaccinated Health Worker. Front. Med. 2021, 8, 1379. [Google Scholar] [CrossRef] [PubMed]
- D’Errico, S.; Zanon, M.; Montanaro, M.; Radaelli, D.; Sessa, F.; Di Mizio, G.; Montana, A.; Corrao, S.; Salerno, M.; Pomara, C. More than pneumonia: Distinctive features of SARS-CoV-2 infection. from autopsy findings to clinical implications: A systematic review. Microorganisms 2020, 8, 1642. [Google Scholar] [CrossRef]
- Paladino, L.; Vitale, A.M.; Caruso Bavisotto, C.; Conway de Macario, E.; Cappello, F.; Macario, A.J.L.; Gammazza, A.M. The Role of Molecular Chaperones in Virus Infection and Implications for Understanding and Treating COVID-19. J. Clin. Med. 2020, 9, 3518. [Google Scholar] [CrossRef] [PubMed]
- Robishaw, J.D.; Alter, S.M.; Solano, J.J.; Shih, R.D.; DeMets, D.L.; Maki, D.G.; Hennekens, C.H. Genomic surveillance to combat COVID-19: Challenges and opportunities. Lancet Microbe 2021, 2, e481–e484. [Google Scholar] [CrossRef]
- Kilic, T.; Weissleder, R.; Lee, H. Molecular and Immunological Diagnostic Tests of COVID-19: Current Status and Challenges. iScience 2020, 23, 101406. [Google Scholar] [CrossRef]
- Sessa, F.; Bertozzi, G.; Cipolloni, L.; Baldari, B.; Cantatore, S.; D’Errico, S.; Di Mizio, G.; Asmundo, A.; Castorina, S.; Salerno, M.; et al. Clinical-Forensic Autopsy Findings to Defeat COVID-19 Disease: A Literature Review. J. Clin. Med. 2020, 9, 2026. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.J.; Hanif, M.; Haider, M.A.; Ahmed, M.U.; Sundas, F.N.U.; Hirani, A.; Khan, I.A.; Anis, K.; Karim, A.H. Treatment Options for COVID-19: A Review. Front. Med. 2020, 7, 480. [Google Scholar] [CrossRef]
- Malik, S.; Gupta, A.; Zhong, X.; Rasmussen, T.P.; Manautou, J.E.; Bahal, R. Emerging Therapeutic Modalities against COVID-19. Pharmaceuticals 2020, 13, 188. [Google Scholar] [CrossRef] [PubMed]
- Marino Gammazza, A.; Légaré, S.; Lo Bosco, G.; Fucarino, A.; Angileri, F.; Oliveri, M.; Cappello, F. Molecular mimicry in the post-COVID-19 signs and symptoms of neurovegetative disorders? Lancet Microbe 2021, 2, e94. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC) Interim Clinical Guidance for Management of Patients with Confirmed Coronavirus Disease (COVID-19). Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-guidance-management-patients.html (accessed on 25 June 2021).
- Mondello, C.; Roccuzzo, S.; Malfa, O.; Sapienza, D.; Gualniera, P.; Ventura Spagnolo, E.; Di Nunno, N.; Salerno, M.; Pomara, C.; Asmundo, A. Pathological Findings in COVID-19 as a Tool to Define SARS-CoV-2 Pathogenesis. A Systematic Review. Front. Pharmacol. 2021, 12, 614586. [Google Scholar] [CrossRef]
- Cipolloni, L.; Sessa, F.; Bertozzi, G.; Baldari, B.; Cantatore, S.; Testi, R.; D’Errico, S.; Di Mizio, G.; Asmundo, A.; Castorina, S.; et al. Preliminary post-mortem COVID-19 evidence of endothelial injury and factor VIII hyperexpression. Diagnostics 2020, 10, 575. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention Collection and Submission of Postmortem Specimens from Deceased Persons with Known or Suspected COVID-19. Available online: https://eaaf.org/wp-content/uploads/covid19-PDFs/EEUU/CDC-guidance-postmortem-specimens.pdf (accessed on 18 August 2020).
- Logar, S.; Leese, M. Ethics Trade-Off Between Hazards Prevention and the Safeguard of Death Dignity During COVID-19. OMEGA J. Death Dying 2020. [Google Scholar] [CrossRef]
- Parekh, U.; Kanchan, T.; Krishan, K. Perils of human remains examination in COVID-19 times. J. Forensic Leg. Med. 2021, 77, 102101. [Google Scholar] [CrossRef] [PubMed]
- Pomara, C.; Li Volti, G.; Cappello, F. The post-lockdown era: What is next in Italy? Front. Pharmacol. 2020, 11, 1074. [Google Scholar] [CrossRef] [PubMed]
- Ussai, S.; Armocida, B.; Formenti, B.; Palestra, F.; Calvi, M.; Missoni, E. Hazard Prevention, Death and Dignity During COVID-19 Pandemic in Italy. Front. Public Health 2020, 8, 509. [Google Scholar] [CrossRef] [PubMed]
- González-Fernández, J.; Ibáñez-Bernáldez, M.; Martínez-Tejedor, J.A.; Alama-Carrizo, S.; Sánchez-Ugena, F.; Montero-Juanes, J.M. Management of corpses during the COVID-19 pandemic in Spain TT —Gestión de los cadáveres durante la pandemia por COVID-19 en España. Spanish J. Leg. Med. 2020, 46, 109–118. [Google Scholar] [CrossRef]
- Osborn, M.; Lucas, S.B.; Stewart, R.; Swift, B.; Youd, E. Autopsy Practice Relating to Possible Cases of COVID-19 (2019-nCov, Novel Coronavirus from China 2019/2020). Available online: https://www.rcpath.org/uploads/assets/d5e28baf-5789-4b0f-acecfe370eee6223/447e37d0-29dd-4994-a11fe27b93de0905/Briefing-on-COVID-19-autopsy-Feb-2020.pdf (accessed on 18 August 2020).
- WHO Interm Guidance Infection Prevention and Control for the safe management of a dead body in the context of COVID-19. J. Hosp. Infect. 2020, 104, 246–251.
- Pomara, C.; Volti, G.L.; Cappello, F. COVID-19 Deaths: Are We Sure It Is Pneumonia? Please, Autopsy, Autopsy, Autopsy! J. Clin. Med. 2020, 9, 1259. [Google Scholar] [CrossRef]
- Salerno, M.; Sessa, F.; Piscopo, A.; Montana, A.; Torrisi, M.; Patanè, F.; Murabito, P.; Li Volti, G.; Pomara, C. No Autopsies on COVID-19 Deaths: A Missed Opportunity and the Lockdown of Science. J. Clin. Med. 2020, 9, 1472. [Google Scholar] [CrossRef]
- Fineschi, V.; Aprile, A.; Aquila, I.; Arcangeli, M.; Asmundo, A.; Bacci, M.; Cingolani, M.; Cipolloni, L.; D’Errico, S.; De Casamassimi, I.; et al. Management of the corpse with suspect, probable or confirmed COVID-19 respiratory infection—Italian interim recommendations for personnel potentially exposed to material from corpses, including body fluids, in morgue structures, during autopsy practice. Pathol. J. Ital. Soc. Anat. Pathol. Diagn. Cytopathol. 2020, 112, 64–77. [Google Scholar]
- Pomara, C.; Salerno, M.; Sessa, F.; Esposito, M.; Barchitta, M.; Ledda, C.; Grassi, P.; Liberto, A.; Mattaliano, A.R.; Rapisarda, V.; et al. Safe Management Strategies in Clinical Forensic Autopsies of Confirmed COVID-19 Cases. Diagnostics 2021, 11, 457. [Google Scholar] [CrossRef] [PubMed]
- Musso, N.; Falzone, L.; Stracquadanio, S.; Bongiorno, D.; Salerno, M.; Esposito, M.; Sessa, F.; Libra, M.; Stefani, S.; Pomara, C. Post-Mortem Detection of SARS-CoV-2 RNA in Long-Buried Lung Samples. Diagnostics 2021, 11, 1158. [Google Scholar] [CrossRef]
- Yaacoub, S.; Schünemann, H.J.; Khabsa, J.; El-Harakeh, A.; Khamis, A.M.; Chamseddine, F.; El Khoury, R.; Saad, Z.; Hneiny, L.; Cuello Garcia, C.; et al. Safe management of bodies of deceased persons with suspected or confirmed COVID-19: A rapid systematic review. BMJ Glob. Health 2020, 5, e002650. [Google Scholar] [CrossRef]
- Corpuz, J.C.G. A dignified death: Management of dead bodies during COVID-19. J. Public Health 2021. [Google Scholar] [CrossRef]
- Pomara, C.; Fineschi, V. Forensic and Clinical Forensic Autopsy. An Atlas and Handbook, 2nd ed.; Pomara, C., Fineschi, V., Eds.; CRC Press: Boca Raton, FL, USA, 2020; ISBN 9780367330712. [Google Scholar]
- Rondinone, V.; Pace, L.; Fasanella, A.; Manzulli, V.; Parisi, A.; Capobianchi, M.R.; Ostuni, A.; Chironna, M.; Caprioli, E.; Labonia, M.; et al. VOC 202012/01 Variant Is Effectively Neutralized by Antibodies Produced by Patients Infected before Its Diffusion in Italy. Viruses 2021, 13, 276. [Google Scholar] [CrossRef]
- Manzulli, V.; Scioscia, G.; Giganti, G.; Capobianchi, M.R.; Lacedonia, D.; Pace, L.; Cipolletta, D.; Tondo, P.; De Nittis, R.; Rondinone, V.; et al. Real Time PCR and Culture-Based Virus Isolation Test in Clinically Recovered Patients: Is the Subject Still Infectious for SARS-CoV2? J. Clin. Med. 2021, 10, 309. [Google Scholar] [CrossRef]
- Lenoci, G.; Galante, D.; Ceci, E.; Manzulli, V.; Moramarco, A.M.; Chiaromonte, A.; Labarile, G.; Lattarulo, S.; Resta, A.; Pace, L.; et al. SARS-CoV-2 isolation from a 10-day-old newborn in Italy: A case report. IDCases 2020, 22, e00960. [Google Scholar] [CrossRef]
- Zacharias, M.; Stangl, V.; Thüringer, A.; Loibner, M.; Wurm, P.; Wolfgruber, S.; Zatloukal, K.; Kashofer, K.; Gorkiewicz, G. Rapid Antigen Test for Postmortem Evaluation of SARS-CoV-2 Carriage. Emerg. Infect. Dis. 2021, 27, 1734–1737. [Google Scholar] [CrossRef] [PubMed]
- Beltempo, P.; Curti, S.M.; Maserati, R.; Gherardi, M.; Castelli, M. Persistence of SARS-CoV-2 RNA in post-mortem swab 35 days after death: A case report. Forensic Sci. Int. 2021, 319, 110653. [Google Scholar] [CrossRef] [PubMed]
- Sablone, S.; Solarino, B.; Ferorelli, D.; Benevento, M.; Chironna, M.; Loconsole, D.; Sallustio, A.; Dell’Erba, A.; Introna, F. Post-mortem persistence of SARS-CoV-2: A preliminary study. Forensic Sci. Med. Pathol. 2021, 17, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Sawant, O.B.; Singh, S.; Wright, R.E., 3rd; Jones, K.M.; Titus, M.S.; Dennis, E.; Hicks, E.; Majmudar, P.A.; Kumar, A.; Mian, S.I. Prevalence of SARS-CoV-2 in human post-mortem ocular tissues. Ocul. Surf. 2021, 19, 322–329. [Google Scholar] [CrossRef]
- Aiello, F.; Ciotti, M.; Gallo Afflitto, G.; Rapanotti, M.C.; Caggiano, B.; Treglia, M.; Grelli, S.; Bernardini, S.; Mauriello, S.; Nucci, C.; et al. Post-Mortem RT-PCR Assay for SARS-CoV-2 RNA in COVID-19 Patients’ Corneal Epithelium, Conjunctival and Nasopharyngeal Swabs. J. Clin. Med. 2021, 10, 4256. [Google Scholar] [CrossRef] [PubMed]
- Adam, M. Is SARS-CoV-2 present in the periodontium? A post-mortem study. Evid. Based. Dent. 2021, 22, 60–61. [Google Scholar] [CrossRef]
- Mohammadi, A.; Esmaeilzadeh, E.; Li, Y.; Bosch, R.J.; Li, J.Z. SARS-CoV-2 detection in different respiratory sites: A systematic review and meta-analysis. EBioMedicine 2020, 59, 102903. [Google Scholar] [CrossRef]
- O’Keeffe, J. Field inquiry: COVID-19 risks from handling the deceased. Ccnse. CA 2021, 1–12. Available online: https://ncceh.ca/sites/default/files/Field%20Inquiry%20-%20COVID_19%20risks%20to%20deathcare%20occupations_Feb%202021_EN_Final.pdf (accessed on 22 September 2021).
- Bogdanović, M.; Skadrić, I.; Atanasijević, T.; Stojković, O.; Popović, V.; Savić, S.; Mihailović, Z.; Radnić, B.; Aćimović, T.; Damjanjuk, I.; et al. Case Report: Post-mortem Histopathological and Molecular Analyses of the Very First Documented COVID-19-Related Death in Europe. Front. Med. 2021, 8, 90. [Google Scholar] [CrossRef]
- Sessa, F.; Salerno, M.; Pomara, C. Autopsy Tool in Unknown Diseases: The Experience with Coronaviruses (SARS-CoV, MERS-CoV, SARS-CoV-2). Medicine 2021, 57, 309. [Google Scholar]
- Prescott, J.; Bushmaker, T.; Fischer, R.; Miazgowicz, K.; Judson, S.; Munster, V.J. Postmortem stability of Ebola virus. Emerg. Infect. Dis. 2015, 21, 856–859. [Google Scholar] [CrossRef] [Green Version]
- Rewar, S.; Mirdha, D. Transmission of Ebola Virus Disease: An Overview. Ann. Glob. Health 2014, 80, 444–451. [Google Scholar] [CrossRef]
- Francesconi, P.; Yoti, Z.; Declich, S.; Onek, P.A.; Fabiani, M.; Olango, J.; Andraghetti, R.; Rollin, P.E.; Opira, C.; Greco, D.; et al. Ebola hemorrhagic fever transmission and risk factors of contacts, Uganda. Emerg. Infect. Dis. 2003, 9, 1430–1437. [Google Scholar] [CrossRef]
- Katz, L.M.; Tobian, A.A.R. Ebola virus disease, transmission risk to laboratory personnel, and pretransfusion testing. Transfusion 2014, 54, 3247–3251. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC). How Are COVID-19 Burials Different from Ebola Burials? Available online: https://www.cdc.gov/coronavirus/2019-ncov/downloads/global-covid-19/COVID19vsEbola-burial-guide.pdf (accessed on 25 June 2021).
- Jefferson, T.; Spencer, E.A.; Brassey, J.; Heneghan, C. Viral cultures for COVID-19 infectious potential assessment—A systematic review. Clin. Infect. Dis. 2020, ciaa1764. [Google Scholar] [CrossRef]
- Cirrincione, L.; Rapisarda, V.; Ledda, C.; Vitale, E.; Provenzano, R.; Cannizzaro, E. Considerations on the Update of the Risk Assessment Document During the Pandemic State by COVID-19 in Italy. Front. Public Health 2021, 9, 933. [Google Scholar] [CrossRef] [PubMed]
- Ledda, C.; Costantino, C.; Cuccia, M.; Maltezou, H.C.; Rapisarda, V. Attitudes of Healthcare Personnel towards Vaccinations before and during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 2703. [Google Scholar] [CrossRef]


{kind=link}
| GROUP | ID | Cause of Death | PMI (Time Elapsed from Death to Autopsy) | SARS-CoV-2 Test | |||
|---|---|---|---|---|---|---|---|
| Nasopharyngeal Swab | Lung Swab | Homogenized Lung Tissue | Cell Culture | ||||
| SHORT PMI | S1 | interstitial pneumonia with fibrosis | 12 h | positive | positive | positive | negative |
| S2 | multiple organ dysfunction syndrome (MODS) | 12 h | positive | positive | positive | positive | |
| S3 | pulmonary edema | 24 h | positive | positive | negative | negative | |
| S4 | acute respiratory distress syndrome (ARDS) | 24 h | positive | positive | positive | negative | |
| S5 | MODS | 48 h | positive | positive | positive | negative | |
| S6 | interstitial pneumonia with fibrosis | 48 h | positive | positive | negative | negative | |
| S7 | cardiac failure | 72 h | positive | positive | positive | negative | |
| S8 | interstitial pneumonia with fibrosis | 72 h | positive | positive | negative | negative | |
| LONG PMI | S9 | ARDS | 24 days | positive | positive | negative | negative |
| S10 | septic shock | 32 days | positive | positive | negative | negative | |
| S11 | interstitial pneumonia with fibrosis | 45 days | positive | positive | negative | negative | |
| S12 | septic shock | 46 days | positive | positive | negative | negative | |
| S13 | interstitial pneumonia with fibrosis | 50 days | positive | positive | positive | negative | |
| S14 | ARDS | 54 days | positive | positive | positive | negative | |
| S15 | pulmonary edema | 61 days | positive | positive | positive | negative | |
| S16 | septic shock | 78 days | positive | positive | negative | negative | |
| Virus | SARS-CoV-2 | Ebola Virus |
|---|---|---|
| Category | RNA virus | RNA virus |
| Family | Coronaviridae | Filoviridae |
| Origin | Zoonotic | Zoonotic |
| Transmission | Contact with respiratory droplets of infected subjects. Transmission from asymptomatic individuals. | Contact with blood or body fluid of infected subjects. |
| Secondary transmission (fomites) | Unknown | Yes |
| Transmission from deceased subjects | Limited to a few hours after death. | Possible until 7 days after death. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pomara, C.; Sessa, F.; Galante, D.; Pace, L.; Fasanella, A.; Di Nunno, N.; Esposito, M.; Salerno, M. Do We Really Need Hazard Prevention at the Expense of Safeguarding Death Dignity in COVID-19? Diagnostics 2021, 11, 1913. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11101913
Pomara C, Sessa F, Galante D, Pace L, Fasanella A, Di Nunno N, Esposito M, Salerno M. Do We Really Need Hazard Prevention at the Expense of Safeguarding Death Dignity in COVID-19? Diagnostics. 2021; 11(10):1913. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11101913
Chicago/Turabian StylePomara, Cristoforo, Francesco Sessa, Domenico Galante, Lorenzo Pace, Antonio Fasanella, Nunzio Di Nunno, Massimiliano Esposito, and Monica Salerno. 2021. "Do We Really Need Hazard Prevention at the Expense of Safeguarding Death Dignity in COVID-19?" Diagnostics 11, no. 10: 1913. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11101913