
Fungal Septic Knee Arthritis Caused by Aspergillus fumigatus following Anterior Cruciate Ligament Reconstruction


 , and
, and
Abstract
:1. Introduction
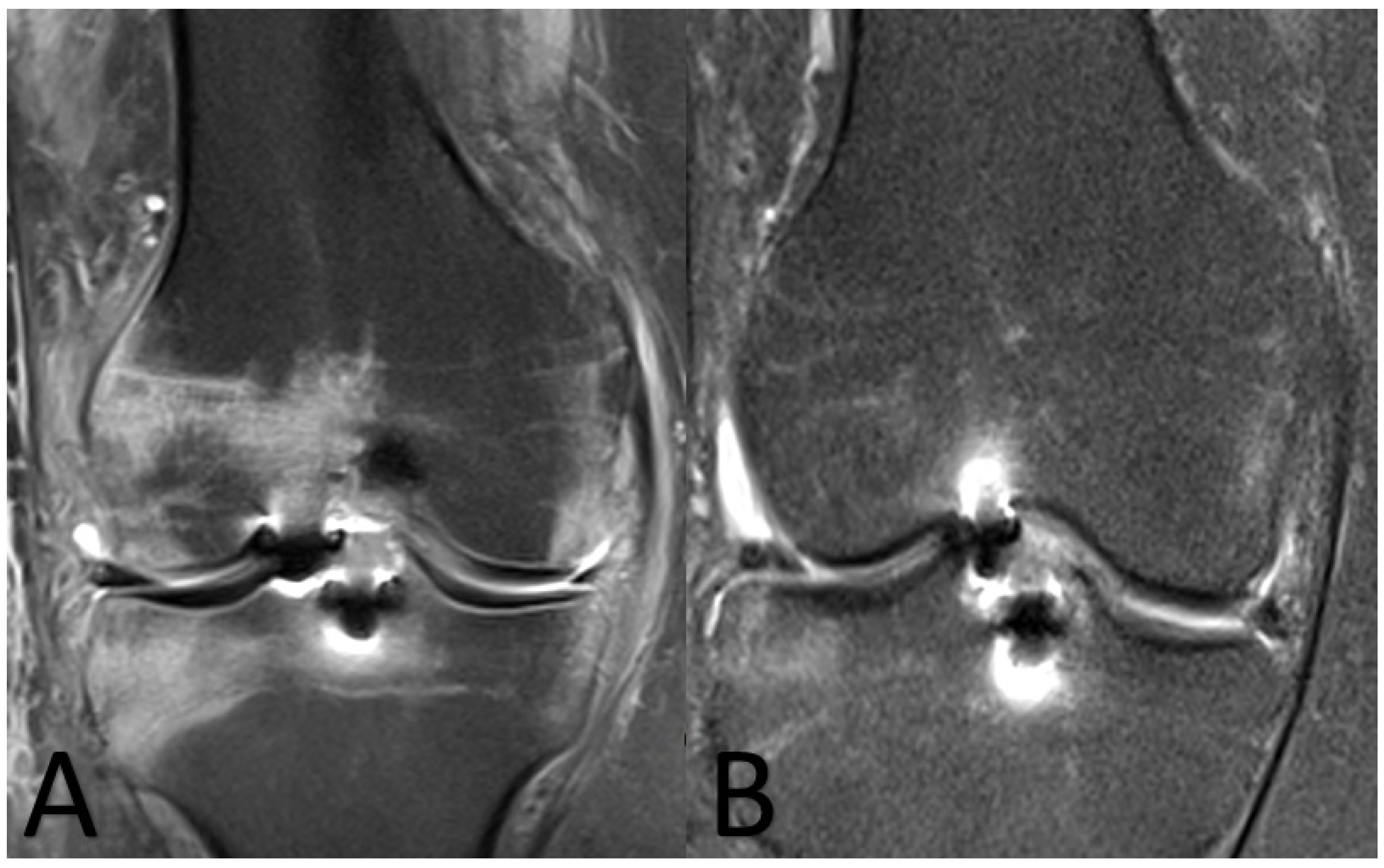
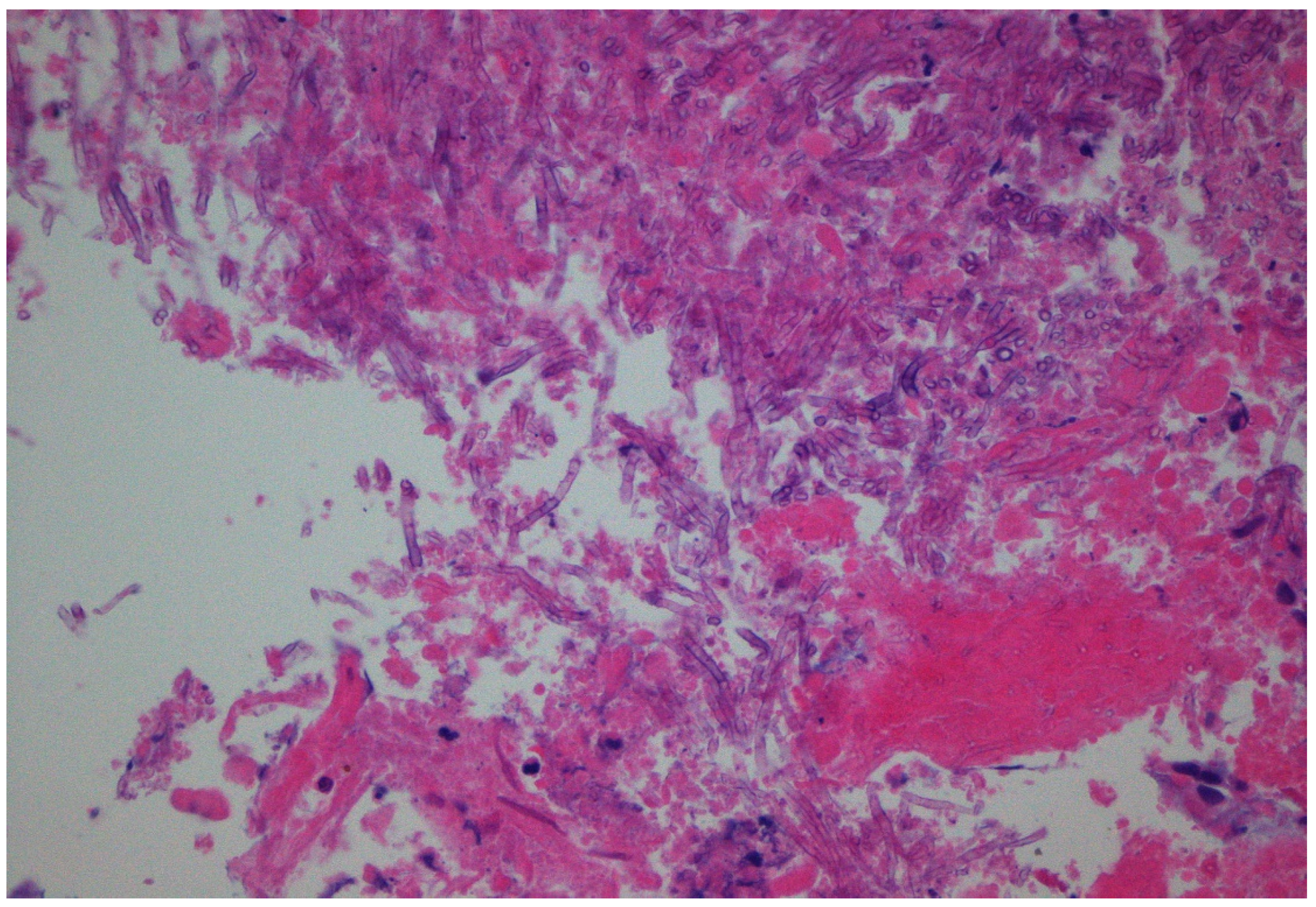
2. Case Presentation
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rousseau, R.; Labruyere, C.; Kajetanek, C.; Deschamps, O.; Makridis, K.G.; Djian, P. Complications After Anterior Cruciate Ligament Reconstruction and Their Relation to the Type of Graft: A Prospective Study of 958 Cases. Am. J. Sports Med. 2019, 47, 2543–2549. [Google Scholar] [CrossRef] [PubMed]
- Gamarra, S.; Chaves, M.; Cabeza, M.; Macedo, D.; Leonardelli, F.; Franco, D.; Boleas, M.; Garcia-Effron, G. Mucormycosis outbreak due to Rhizopus microsporus after arthroscopic anterior cruciate ligament reconstruction surgery evaluated by RAPD and MALDI-TOF Mass spectrometry. J. Mycol. Méd. 2018, 28, 617–622. [Google Scholar] [PubMed]
- Castro, C.E.F.; Smith, P.W.; Daccarett, M.S. Candida Glabrata Septic Arthritis Involving the Right Knee After Anterior Cruciate Ligament Graft Placement. MOJ Orthop. Rheumatol. 2016, 4, 00147. [Google Scholar]
- Waterman, B.R.; Arroyo, W.; Cotter, E.J.; Zacchilli, M.A.; Garcia, E.J.; Owens, B.D. Septic Arthritis After Anterior Cruciate Ligament Reconstruction: Clinical and Functional Outcomes Based on Graft Retention or Removal. Orthop. J. Sports Med. 2018, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burke, W.V.; Zych, G.A. Fungal infection following replacement of the anterior cruciate ligament: A case report. J. Bone Jt. Surg. Am. 2002, 84, 449–453. [Google Scholar] [CrossRef] [PubMed]
- Muscolo, L.D.; Carbo, L.; Aponte-Tinao, L.A.; Ayerza, M.A.; Makino, A. Massive Bone Loss from Fungal Infection after Anterior Cruciate Ligament Arthroscopic Reconstruction. Clin. Orthop. Relat. Res. 2009, 467, 2420–2425. [Google Scholar] [PubMed] [Green Version]
- Antkowiak, T.T.; Polage, C.R.; Wiedeman, J.A.; Meehan, J.P.; Jamali, A.A. Chondrolysis of the tibial plateau caused by articular as-pergillosis after ACL autograft reconstruction: Management with a fresh osteochondral allograft: A case report. J. Bone Jt. Surg. Am. 2011, 93, e1241-6. [Google Scholar]
- Sun, L.; Zhang, L.; Wang, K.; Wang, W.; Tian, M. Fungal osteomyelitis after arthroscopic anterior cruciate ligament reconstruction: A case report with review of the literature. Knee 2012, 19, 728–731. [Google Scholar]
- Mirzatolooei, F. Outbreak of serial knee joint sepsis after arthroscopic surgery: A case series with the guideline for treatment. Acta Medica Iran. 2014, 52, 310–314. [Google Scholar]
- Wang, C.; Lee, Y.H.D.; Siebold, R. Recommendations for the management of septic arthritis after ACL reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2013, 22, 2136–2144. [Google Scholar] [CrossRef]
- Koutserimpas, C.; Samonis, G.; Velivassakis, E.; Iliopoulou-Kosmadaki, S.; Kontakis, G.; Kofteridis, D.P. Candida glabrata prosthetic joint infection, successfully treated with anidulafungin: A case report and review of the literature. Mycoses 2017, 61, 266–269. [Google Scholar]
- Papachristou, S.G.; Iosifidis, E.; Sipsas, N.V.; Gamaletsou, M.N.; Walsh, T.J.; Roilides, E. Management of osteoarticular fungal infections in the setting of immunodeficiency. Expert Rev. Anti-Infect. Ther. 2020, 18, 461–474. [Google Scholar] [CrossRef]
- Koutserimpas, C.; Zervakis, S.G.; Maraki, S.; Alpantaki, K.; Ioannidis, A.; Kofteridis, D.P.; Samonis, G. Non-albicans Candida prosthetic joint infections: A systematic review of treatment. World J. Clin. Cases 2019, 7, 1430–1443. [Google Scholar]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease from the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Con-sortium. Clin. Infect. Dis. 2020, 71, 1367–1376. [Google Scholar] [PubMed] [Green Version]
- Gamaletsou, M.N.; Rammaert, B.; Bueno, M.A.; Moriyama, B.; Sipsas, N.V.; Kontoyiannis, D.P.; Roilides, E.; Zeller, V.; Prinapori, R.; Taj-Aldeen, S.J.; et al. Aspergillus osteomyelitis: Epidemiology, clinical manifestations, management, and outcome. J. Infect. 2014, 68, 478–493. [Google Scholar]
- Koutserimpas, C.; Chamakioti, I.; Zervakis, S.; Raptis, K.; Alpantaki, K.; Kofteridis, D.; Vrioni, G.; Samonis, G. Non-Candida Fungal Prosthetic Joint Infections. Diagnostics 2021, 11, 1410. [Google Scholar]
- Tashiro, M.; Izumikawa, K.; Minematsu, A.; Hirano, K.; Iwanaga, N.; Ide, S.; Mihara, T.; Hosogaya, N.; Takazono, T.; Morinaga, Y.; et al. Antifungal Susceptibilities of Aspergillus fumigatus Clinical Isolates Obtained in Nagasaki, Japan. Antimicrob. Agents Chemother. 2011, 56, 584–587. [Google Scholar]
- Nett, J.E.; Andes, D.R. Antifungal Agents: Spectrum of Activity, Pharmacology, and Clinical Indications. Infect. Dis. Clin. N. Am. 2016, 30, 51–83. [Google Scholar]
- Herbrecht, R.; Denning, D.W.; Patterson, T.F.; Bennett, J.E.; Greene, R.E.; Oestmann, J.W.; Kern, W.V.; Marr, K.A.; Ribaud, P.; Lortholary, O.; et al. Invasive Fungal Infections Group of the European Organisation for Research and Treatment of Cancer and the Global Aspergillus Study Group. Voriconazole versus amphotericin B for primary therapy of invasive aspergillosis. N. Engl. J. Med. 2002, 347, 408–415. [Google Scholar]
- Lamoth, F.; Lewis, R.E.; Kontoyiannis, D.P. Role and Interpretation of Antifungal Susceptibility Testing for the Management of Invasive Fungal Infections. J. Fungi 2020, 7, 17. [Google Scholar]
- Kidd, S.E.; Chen, S.C.-A.; Meyer, W.; Halliday, C.L. A New Age in Molecular Diagnostics for Invasive Fungal Disease: Are We Ready? Front. Microbiol. 2020, 10, 2903. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanguinetti, M.; Posteraro, B. MALDI-TOF Mass Spectrometry: Any Use for Aspergilli? Mycopathologia 2014, 178, 417–426. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Authors | Year | Causative Fungus | Diagnosis | Antifungal Treatment |
|---|---|---|---|---|
| Burke and Zych [5] | 2002 | Phycomycoses | Histopathology | Amphotericin B |
| Muscolo et al. [6] | 2009 | (1). Rhizopus microsporus (2). Rhizopus microsporus (3). Rhizopus microsporus (4). Rhizopus microsporus (5). Rhizopus microsporus (6). Candida albicans | Cultures and histopathology | Amphotericin B |
| Antkowiak et al. [7] | 2011 | Aspergillus flavus | Cultures and histopathology | Voriconazole and caspofungin |
| Sun et al. [8] | 2012 | Aspergillus spp. | Histopathology | NR |
| Mirzatolooei [9] | 2014 | Alternaria spp. | Cultures | NR |
| Castro et al. [3] | 2016 | Candida glabrata | Cultures | Caspofungin, micafungin, voriconazole |
| Gamarra et al. [2] | 2018 | (1). Rhizopus microsporus (2). Rhizopus microsporus (3). Rhizopus microsporus | Histopathology, PCR | Amphotericin B |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Samonis, G.; Koutserimpas, C.; Vrioni, G.; Kampos Martinez, E.; Kouloumentas, P.; Alpantaki, K.; Saroglou, G. Fungal Septic Knee Arthritis Caused by Aspergillus fumigatus following Anterior Cruciate Ligament Reconstruction. Diagnostics 2021, 11, 1975. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11111975
Samonis G, Koutserimpas C, Vrioni G, Kampos Martinez E, Kouloumentas P, Alpantaki K, Saroglou G. Fungal Septic Knee Arthritis Caused by Aspergillus fumigatus following Anterior Cruciate Ligament Reconstruction. Diagnostics. 2021; 11(11):1975. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11111975
Chicago/Turabian StyleSamonis, George, Christos Koutserimpas, Georgia Vrioni, Elsa Kampos Martinez, Panagiotis Kouloumentas, Kalliopi Alpantaki, and George Saroglou. 2021. "Fungal Septic Knee Arthritis Caused by Aspergillus fumigatus following Anterior Cruciate Ligament Reconstruction" Diagnostics 11, no. 11: 1975. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11111975