
Prediction of Neoadjuvant Chemotherapy Response in Osteosarcoma Using Convolutional Neural Network of Tumor Center 18F-FDG PET Images

Abstract
:1. Introduction
2. Materials and Methods
2.1. 18F-FDG PET/CT
2.2. Quantitative Analysis of 18F-FDG Uptake Heterogeneity
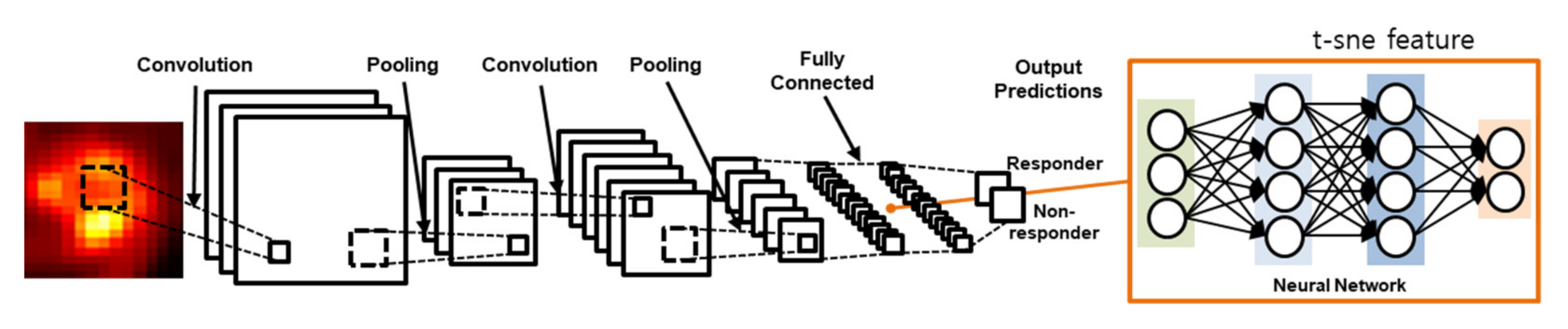
2.3. Convolutional Neural Network
2.4. Statistical Analysis
3. Results
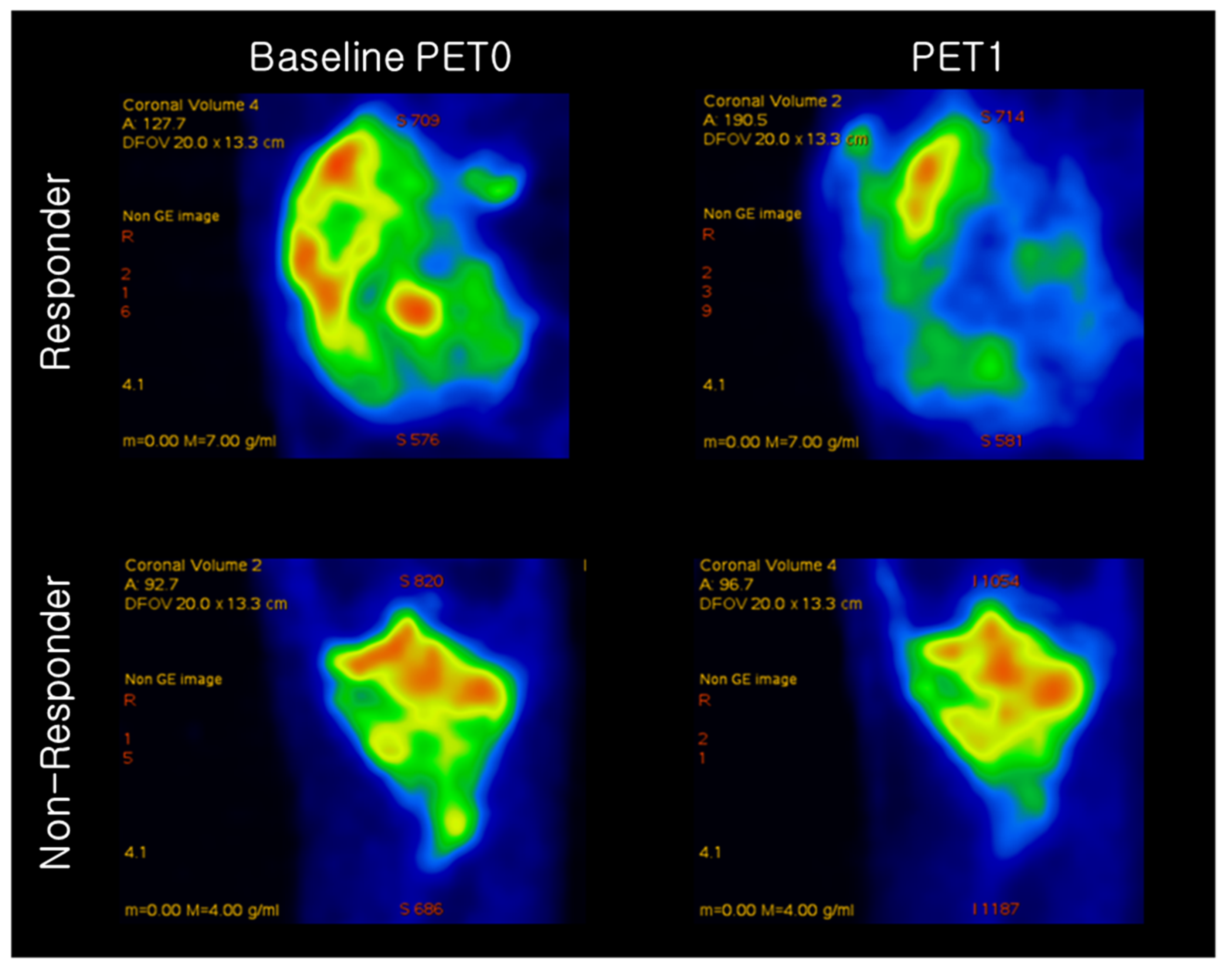
3.1. 18F-FDG Quantitative Analysis
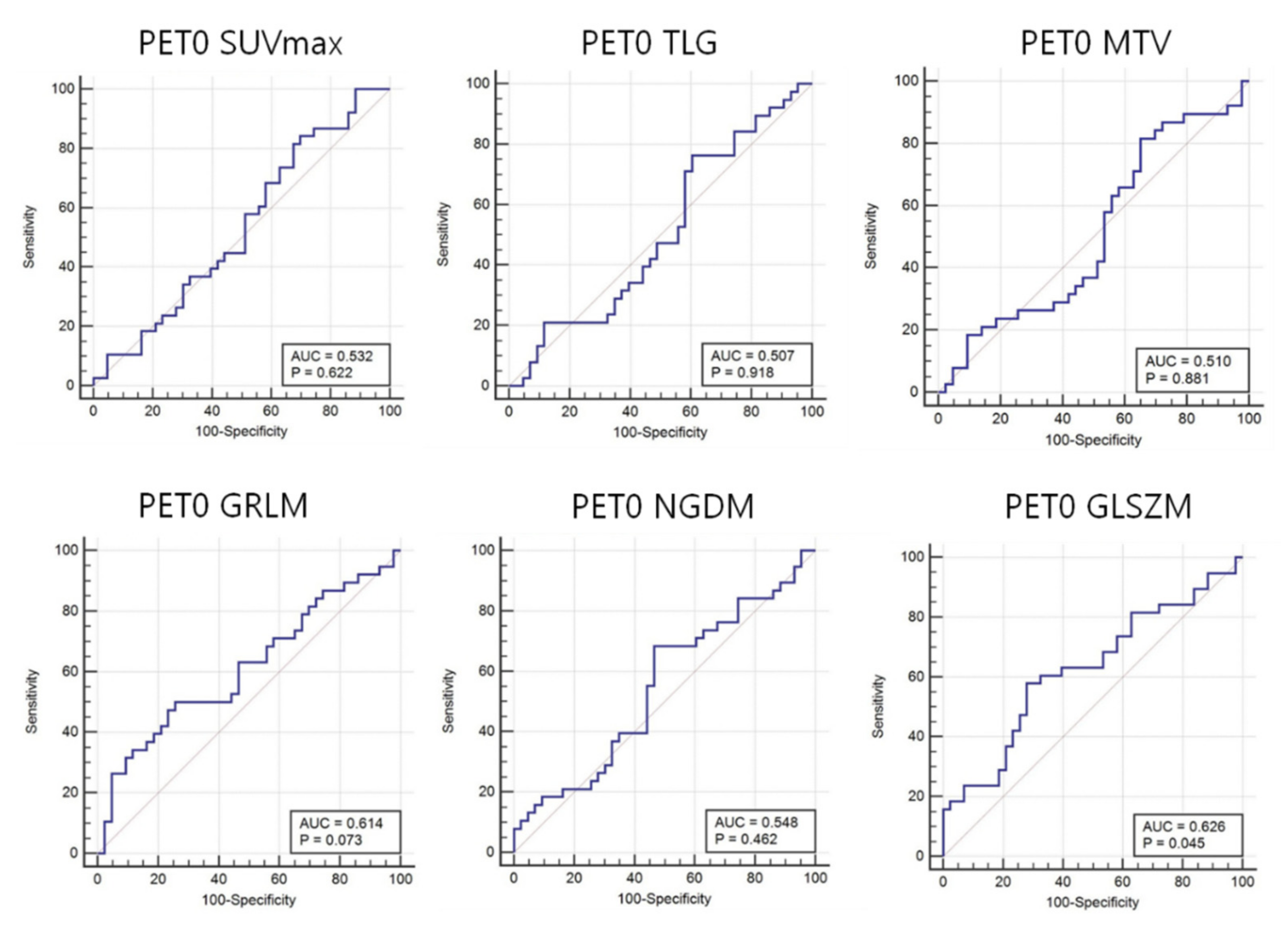
3.2. Quantitative 18F-FDG Heterogeneity Features
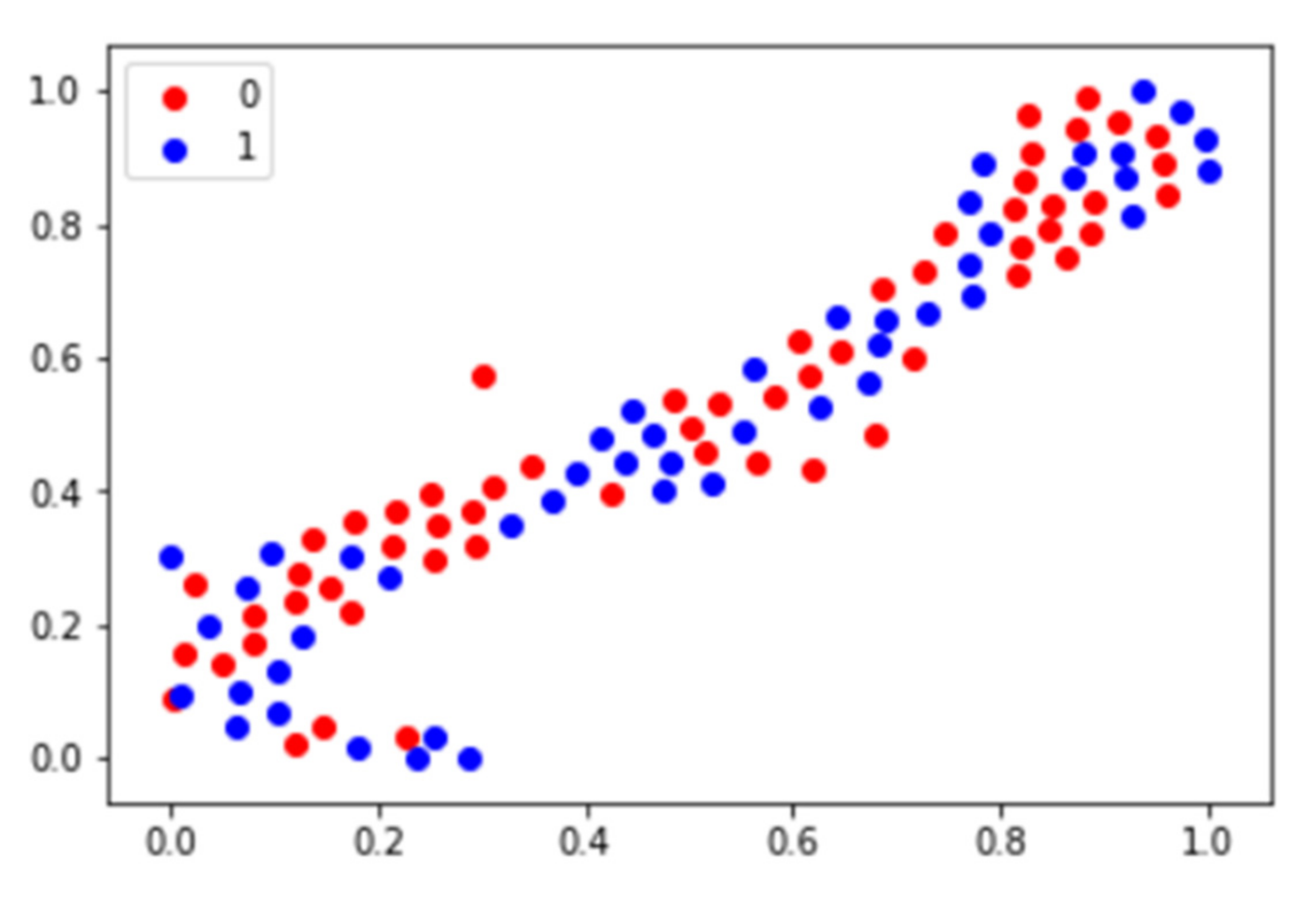
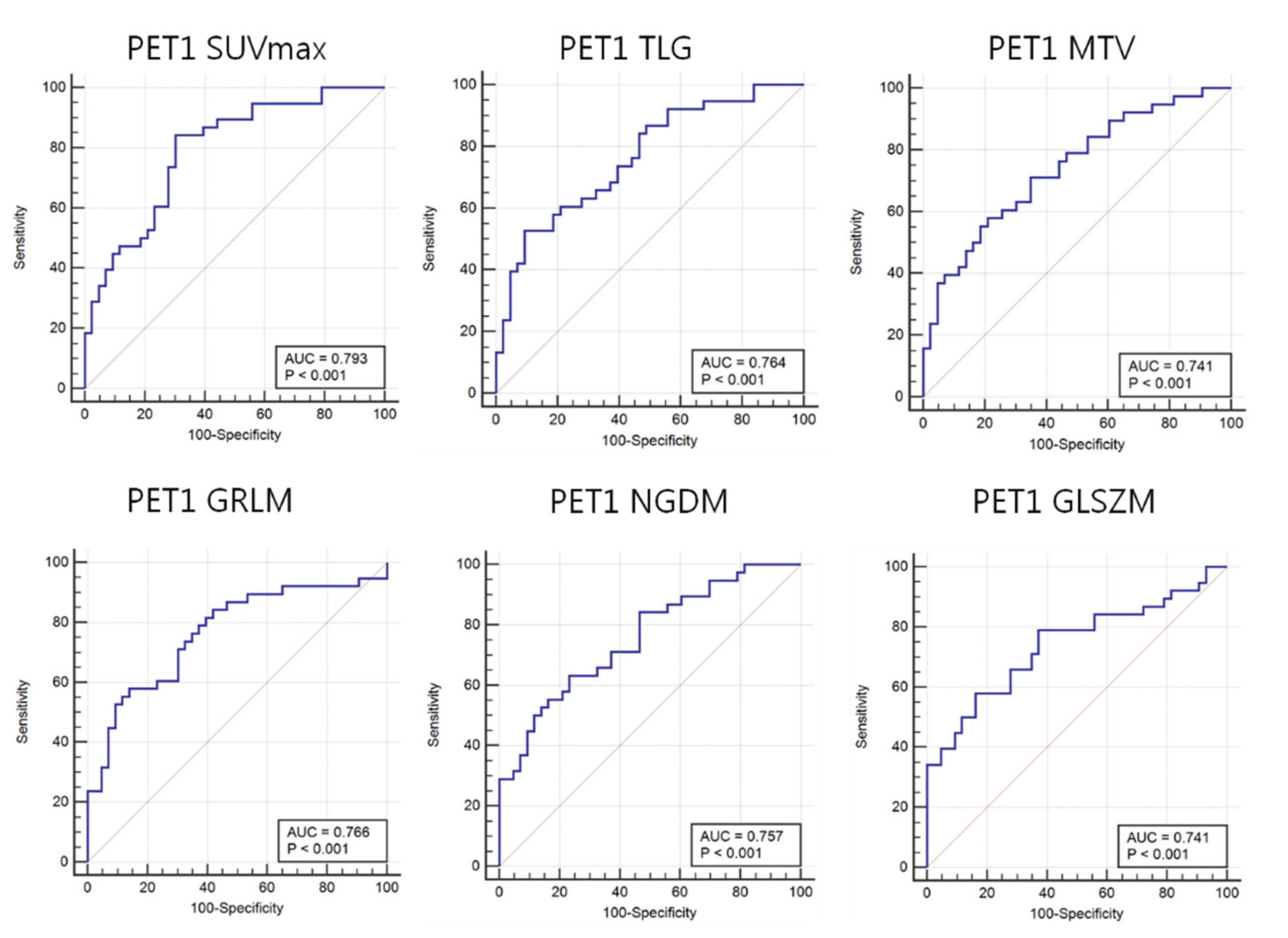
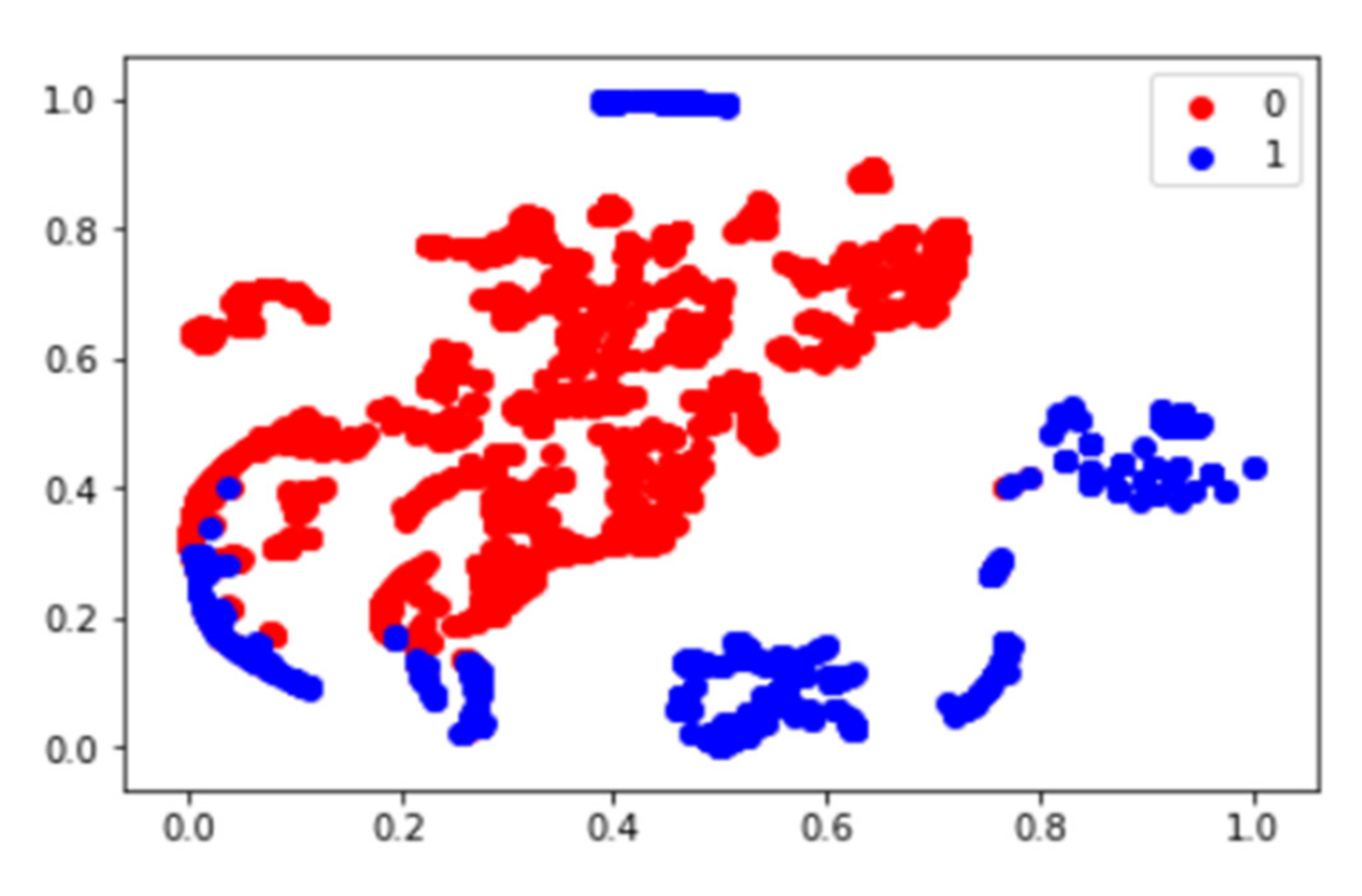
3.3. Predictive Accuracies of 18F-FDG PET 2D CNN
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Picci, P. Osteosarcoma (osteogenic sarcoma). Orphanet J. Rare Dis. 2007, 2, 6. [Google Scholar] [CrossRef] [Green Version]
- Misaghi, A.; Goldin, A.; Awad, M.; Kulidjian, A.A. Osteosarcoma: A comprehensive review. SICOT-J. 2018, 4, 12. [Google Scholar] [CrossRef] [Green Version]
- Bacci, G.; Longhi, A.; Fagioli, F.; Briccoli, A.; Versari, M.; Picci, P. Adjuvant and neoadjuvant chemotherapy for osteosarcoma of the extremities: 27 year experience at Rizzoli Institute, Italy. Eur. J. Cancer 2005, 41, 2836–2845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hagleitner, M.M.; De Bont, E.S.J.M.; Loo, D.M.W.M.T. Survival Trends and Long-Term Toxicity in Pediatric Patients with Osteosarcoma. Sarcoma 2012, 2012, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Bacci, G.; Ferrari, S.; Bertoni, F.; Ruggieri, P.; Picci, P.; Longhi, A.; Casadei, R.; Fabbri, N.; Forni, C.; Versari, M.; et al. Long-Term Outcome for Patients With Nonmetastatic Osteosarcoma of the Extremity Treated at the Istituto Ortopedico Rizzoli According to the Istituto Ortopedico Rizzoli/Osteosarcoma-2 Protocol: An Updated Report. J. Clin. Oncol. 2000, 18, 4016–4027. [Google Scholar] [CrossRef]
- Kim, M.S.; Lee, S.-Y.; Lee, T.R.; Cho, W.H.; Song, W.S.; Koh, J.-S.; Lee, J.A.; Yoo, J.Y.; Jeon, D.-G. Prognostic nomogram for predicting the 5-year probability of developing metastasis after neo-adjuvant chemotherapy and definitive surgery for AJCC stage II extremity osteosarcoma. Ann. Oncol. 2009, 20, 955–960. [Google Scholar] [CrossRef] [PubMed]
- Bajpai, J.; Gamnagatti, S.; Kumar, R.; Sreenivas, V.; Sharma, M.C.; Alam Khan, S.; Rastogi, S.; Malhotra, A.; Safaya, R.; Bakhshi, S. Role of MRI in osteosarcoma for evaluation and prediction of chemotherapy response: Correlation with histological necros is. Pediatr. Radiol. 2011, 41, 441–450. [Google Scholar] [CrossRef]
- Jeon, D.; Song, W.S. How can survival be improved in localized osteosarcoma? Expert Rev. Anticanc. 2014, 10, 1313–1325. [Google Scholar] [CrossRef]
- Coffin, C.M.; Lowichik, A.; Zhou, H. Treatment effects in pediatric soft tissue and bone tumors: Practical considerations for the pathologist. Am. J. Clin. Pathol. 2005, 123, 75–90. [Google Scholar] [CrossRef]
- Davis, A.; Bell, R.S.; Goodwin, P. Prognostic factors in osteosarcoma: A critical review. J. Clin. Oncol. 1994, 12, 423–431. [Google Scholar] [CrossRef] [PubMed]
- Wellings, R.; Davies, A.; Pynsent, P.; Carter, S.; Grimer, R. The value of computed tomographic measurements in Osteosarcoma as a Predictor of Response to Adjuvant chemotherapy. Clin. Radiol. 1994, 49, 19–23. [Google Scholar] [CrossRef]
- Ongolo-Zogo, P.; Thiesse, P.; Sau, J.; Desuzinges, C.; Blay, J.-Y.; Bonmartin, A.; Bochu, M.; Philip, T. Assessment of osteosarcoma response to neoadjuvant chemotherapy: Comparative usefulness of dynamic gadolinium-enhanced spin-echo magnetic resonance imaging and technetium-99 m skeletal angioscintigraphy. Eur. Radiol. 1999, 9, 907–914. [Google Scholar] [CrossRef] [PubMed]
- Holscher, H.C.; Bloem, J.L.; Nooy, M.A.; Taminiau, A.H.; Eulderink, F.; Hermans, J. The value of MR imaging in monitoring the effect of chemotherapy on bone sarcomas. Am. J. Roentgenol. 1990, 154, 763–769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costelloe, C.M.; Macapinlac, H.A.; Madewell, J.E.; Fitzgerald, N.E.; Mawlawi, O.R.; Rohren, E.M.; Raymond, A.K.; Lewis, V.O.; Anderson, P.M.; Bassett, R.L.; et al. 18F-FDG PET/CT as an Indicator of Progression-Free and Overall Survival in Osteosarcoma. J. Nucl. Med. 2009, 50, 340–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheon, G.J.; Kim, M.S.; Lee, J.A.; Lee, S.-Y.; Cho, W.H.; Song, W.S.; Koh, J.-S.; Yoo, J.Y.; Oh, D.H.; Shin, D.S.; et al. Prediction Model of Chemotherapy Response in Osteosarcoma by 18F-FDG PET and MRI. J. Nucl. Med. 2009, 50, 1435–1440. [Google Scholar] [CrossRef] [Green Version]
- Kong, C.-B.; Byun, B.H.; Lim, I.; Choi, C.W.; Lim, S.M.; Song, W.S.; Cho, W.H.; Jeon, D.-G.; Koh, J.-S.; Yoo, J.Y.; et al. 18F-FDG PET SUVmax as an indicator of histopathologic response after neoadjuvant chemotherapy in extremity osteosarcoma. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 728–736. [Google Scholar] [CrossRef]
- Nabi, H.A.; Zubeldia, J.M. Clinical applications of (18)F-FDG in oncology. J. Nucl. Med. Technol. 2002, 30, 3–9. [Google Scholar]
- Oh, J.-R.; Seo, J.-H.; Chong, A.; Min, J.-J.; Song, H.-C.; Kim, Y.-C.; Bom, H.-S. Whole-body metabolic tumour volume of 18F-FDG PET/CT improves the prediction of prognosis in small cell lung cancer. Eur. J. Nucl. Med. Mol. Imaging 2012, 39, 925–935. [Google Scholar] [CrossRef]
- Marinelli, B.; Espinet-Col, C.; Ulaner, G.A.; McArthur, H.L.; Gonen, M.; Jochelson, M.; Weber, W.A. Prognostic value of FDG PET/CT-based metabolic tumor volumes in metastatic triple negative breast cancer patients. Am. J. Nucl. Med. Mol. Imaging 2016, 6, 120–127. [Google Scholar] [PubMed]
- Byun, B.H.; Kong, C.-B.; Lim, I.; Kim, B.I.; Choi, C.W.; Song, W.S.; Cho, W.H.; Jeon, D.-G.; Koh, J.-S.; Lee, S.-Y.; et al. Early response monitoring to neoadjuvant chemotherapy in osteosarcoma using sequential 18 F-FDG PET/CT and MRI. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 1553–1562. [Google Scholar] [CrossRef]
- Akhil, V.; Raghav, G.; Arunachalam, N.; Srinivasu, D.S. Image Data-Based Surface Texture Characterization and Prediction Using Machine Learning Approaches for Additive Manufacturing. J. Comput. Inf. Sci. Eng. 2020, 20, 1–39. [Google Scholar] [CrossRef]
- Le, N.Q.K.; Huynh, T.-T. Identifying SNAREs by Incorporating Deep Learning Architecture and Amino Acid Embedding Representation. Front. Physiol. 2019, 10, 1501. [Google Scholar] [CrossRef] [PubMed]
- Le, N.Q.K.; Yapp, E.K.Y.; Nagasundaram, N.; Yeh, H.-Y. Classifying Promoters by Interpreting the Hidden Information of DNA Sequences via Deep Learning and Combination of Continuous FastText N-Grams. Front. Bioeng. Biotechnol. 2019, 7, 305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Z.; Wang, Y.; Yu, J.; Guo, Y.; Cao, W. Deep Learning based Radiomics (DLR) and its usage in noninvasive IDH1 prediction for low grade glioma. Sci. Rep. 2017, 7, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Lao, J.; Chen, Y.; Li, Z.-C.; Li, Q.; Zhang, J.; Liu, J.; Zhai, G. A Deep Learning-Based Radiomics Model for Prediction of Survival in Glioblastoma Multiforme. Sci. Rep. 2017, 7, 10353. [Google Scholar] [CrossRef] [PubMed]
- Ypsilantis, P.-P.; Siddique, M.; Sohn, H.-M.; Davies, A.; Cook, G.; Goh, V.; Montana, G. Predicting Response to Neoadjuvant Chemotherapy with PET Imaging Using Convolutional Neural Networks. PLoS ONE 2015, 10, e0137036. [Google Scholar] [CrossRef]
- Nioche, C.; Orlhac, F.; Boughdad, S.; Reuzé, S.; Goya-Outi, J.; Robert, C.; Pellot-Barakat, C.; Soussan, M.; Frouin, F.; Buvat, I. LIFEx: A Freeware for Radiomic Feature Calculation in Multimodality Imaging to Accelerate Advances in the Characterization of Tumor Heterogeneity. Cancer Res. 2018, 78, 4786–4789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Im, H.-J.; Bradshaw, T.; Solaiyappan, M.; Cho, S.Y. Current Methods to Define Metabolic Tumor Volume in Positron Emission Tomography: Which One is Better? Nucl. Med. Mol. Imaging 2018, 52, 5–15. [Google Scholar] [CrossRef]
- Srivastava, N.; Hinton, G.; Krizhevsky, A.; Sutskever, I.; Salakhutdinov, R. Dropout: A simple way to prevent neural networks from overfitting. J. Mach. Learn. Res. 2014, 15, 1929–1958. [Google Scholar] [CrossRef]
- Erickson, B.J.; Korfiatis, P.; Akkus, Z.; Kline, T.L. Machine Learning for Medical Imaging. Radiogr. 2017, 37, 505–515. [Google Scholar] [CrossRef]
- Shen, D.; Wu, G.; Suk, H.-I. Deep Learning in Medical Image Analysis. Annu. Rev. Biomed. Eng. 2017, 19, 221–248. [Google Scholar] [CrossRef] [Green Version]
- Fang, Y.-H.D.; Lin, C.-Y.; Shih, M.-J.; Wang, H.-M.; Ho, T.-Y.; Liao, C.-T.; Yen, T.-C. Development and Evaluation of an Open-Source Software Package “CGITA” for Quantifying Tumor Heterogeneity with Molecular Images. BioMed Res. Int. 2014, 2014, 1–9. [Google Scholar] [CrossRef]
- Ha, S.; Park, S.; Bang, J.-I.; Kim, E.-K.; Lee, H.-Y. Metabolic Radiomics for Pretreatment 18F-FDG PET/CT to Characterize Locally Advanced Breast Cancer: Histopathologic Characteristics, Response to Neoadjuvant Chemotherapy, and Prognosis. Sci. Rep. 2017, 7, 1556. [Google Scholar] [CrossRef] [PubMed]
- Yoon, H.; Kim, Y.; Chung, J.; Kim, B.S. Predicting neo-adjuvant chemotherapy response and progression-free survival of locally advanced breast cancer using textural features of intratumoral heterogeneity on F-18 FDG PET/CT and diffusion-weighted MR imaging. Breast J. 2019, 25, 373–380. [Google Scholar] [CrossRef]
- Cheng, N.-M.; Fang, Y.-H.D.; Lee, L.-Y.; Chang, J.T.-C.; Tsan, D.-L.; Ng, S.-H.; Wang, H.-M.; Liao, C.-T.; Yang, L.-Y.; Hsu, C.-H.; et al. Zone-size nonuniformity of 18F-FDG PET regional textural features predicts survival in patients with oropharyngeal cancer. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Hyun, S.H.; Kim, H.S.; Choi, S.H.; Choi, D.W.; Lee, J.K.; Lee, K.H.; Park, J.O.; Lee, K.-H.; Kim, B.-T.; Choi, J.Y. Intratumoral heterogeneity of 18F-FDG uptake predicts survival in patients with pancreatic ductal adenocarcinoma. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 1461–1468. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Zhou, Z.; Li, Y.; Chen, Z.; Lu, P.; Wang, W.; Liu, W.; Yu, L. Comparison of machine learning methods for classifying mediastinal lymph node metastasis of non-small cell lung cancer from 18F-FDG PET/CT images. EJNMMI Res. 2017, 7, 1–11. [Google Scholar] [CrossRef]
- Zeiler, M.D.; Fergus, R. Visualizing and understanding convolutional networks. In Proceedings of the European Conference on Computer Vision, Zurich, Switzerland, 6 September 2014; pp. 818–833. [Google Scholar]
- Wei, D.; Zhou, B.; Torralba, A.; Freeman, W. MNeuron: A Matlab Plugin to Visualize Neurons from Deep Models. 2017. Available online: https://donglaiw.github.io/proj/mneuron/index.html (accessed on 23 October 2021).
- Mahendran, A.; Vedaldi, A. Understanding deep image representations by inverting them. In Proceedings of the 2015 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Boston, MA, USA, 7–12 June 2015; pp. 5188–5196. [Google Scholar]
- Bergstra, J.; Bengio, Y. Random search for hyper-parameter optimization. J. Mach. Learn. Res. 2012, 13, 281–305. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Value |
|---|---|
| Sex, n (%) | |
| Female | 30 (29.50%) |
| Male | 75 (70.50%) |
| Age, n (%) | |
| years ≤ 19 | 80 (77.14%) |
| years >19 | 25 (22.86%) |
| Location of primary tumor, n (%) | |
| Femur | 59 (56.19%) |
| Tibia | 35 (33.33%) |
| Fibula | 5 (4.76%) |
| Humerus | 4 (3.80%) |
| Pelvis | 2 (1.92%) |
| AJCC stage, n (%) | |
| IIA | 37 (35.23%) |
| IIB | 64 (60.95%) |
| III | 2 (1.91%) |
| IV | 2 (1.91%) |
| Pathologic subtype, n (%) | |
| OB (Osteoblastic) | 78 (74.28%) |
| CB (Chondroblastic) | 13 (12.38%) |
| FB (Fibroblastic) | 7 (6.67%) |
| Others | 7 (6.67%) |
| Histologic response, n (%) | |
| Responder | 47 (45.76%) |
| Non-responder | 58 (54.24%) |
| Feature Family | Features |
|---|---|
| Intensity histogram | SUVmax |
| SUVmean | |
| Standard deviation (SUV_SD) | |
| Total lesion glycolysis (TLG) | |
| Metabolic tumor volume (MTV) | |
| 1st entropy | |
| Gray level co-occurrence matrix (GLCM) | Energy |
| Contrast | |
| Entropy | |
| Homogeneity | |
| Dissimilarity | |
| Neighboring gray level dependence matrix(NGLDM) | Contrast |
| Coarseness | |
| Busyness | |
| SNE (Small number emphasis) | |
| Gray level run length matrix(GLRLM) | SRE (Short run emphasis) |
| LRE (Long run emphasis) | |
| GLNU (Gray level non-uniformity) | |
| RLNU (Run length non-uniformity) | |
| SRLGE (Low gray level run emphasis) | |
| SGHGE (High gray level run emphasis) | |
| Gray level size zone matrix(GLSZM) | SAE (Small zone emphasis) |
| LAE (Large zone emphasis) | |
| GLN (Gray level non-uniformity) | |
| SZN (Zone size non-uniformity) | |
| LGLZE (Low gray level zone emphasis) | |
| HGLZE (High gray level zone emphasis) |
| Chemotherapy Response | Random Forest | Support Vector Machine |
|---|---|---|
| Sensitivity | 0.53 | 0.75 |
| Specificity | 0.61 | 0.83 |
| Precision | 0.54 | 0.57 |
| Dice coefficient | 0.49 | 0.48 |
| AUC | 0.55 | 0.52 |
| Accuracy | 0.55 | 0.54 |
| Features | Discrimination | Baseline PET0 | PET1 | ||
|---|---|---|---|---|---|
| AUC | p-Value | AUC | p-Value | ||
| SUV_max | Intensity | 0.532 | 0.622 | 0.793 | <0.001 |
| SUV_SD | Intensity | 0.505 | 0.940 | 0.802 | <0.001 |
| TLG | Intensity | 0.507 | 0.918 | 0.764 | <0.001 |
| Volume | Shape | 0.510 | 0.881 | 0.741 | <0.001 |
| GLRLM_SGHGE | Voxel-alignment | 0.614 | 0.073 | 0.766 | <0.001 |
| NGLDM_SNE | Neighborhood intensity difference | 0.548 | 0.462 | 0.757 | <0.001 |
| GLSZM_HGLZE | Intensity size zone | 0.626 | 0.045 | 0.741 | <0.001 |
| GLCM_entropy | Normalized Co-occurrence matrix | 0.588 | 0.165 | 0.744 | <0.001 |
| 2D CNN | Total Tumor Slices | Center 20 Slices | Center 10 Slices | Center Slice |
|---|---|---|---|---|
| Train accuracy | 0.984 | 0.983 | 0.966 | 0.988 |
| Test accuracy | 0.625 | 0.616 | 0.628 | 0.76 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.; Jeong, S.Y.; Kim, B.-C.; Byun, B.-H.; Lim, I.; Kong, C.-B.; Song, W.S.; Lim, S.M.; Woo, S.-K. Prediction of Neoadjuvant Chemotherapy Response in Osteosarcoma Using Convolutional Neural Network of Tumor Center 18F-FDG PET Images. Diagnostics 2021, 11, 1976. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11111976
Kim J, Jeong SY, Kim B-C, Byun B-H, Lim I, Kong C-B, Song WS, Lim SM, Woo S-K. Prediction of Neoadjuvant Chemotherapy Response in Osteosarcoma Using Convolutional Neural Network of Tumor Center 18F-FDG PET Images. Diagnostics. 2021; 11(11):1976. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11111976
Chicago/Turabian StyleKim, Jingyu, Su Young Jeong, Byung-Chul Kim, Byung-Hyun Byun, Ilhan Lim, Chang-Bae Kong, Won Seok Song, Sang Moo Lim, and Sang-Keun Woo. 2021. "Prediction of Neoadjuvant Chemotherapy Response in Osteosarcoma Using Convolutional Neural Network of Tumor Center 18F-FDG PET Images" Diagnostics 11, no. 11: 1976. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11111976