
Performance of Automated Point-of-Care Respiratory Rate Counting versus Manual Counting in Children under Five Admitted with Severe Febrile Illness to Kisantu Hospital, DR Congo

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Description of the Study Population
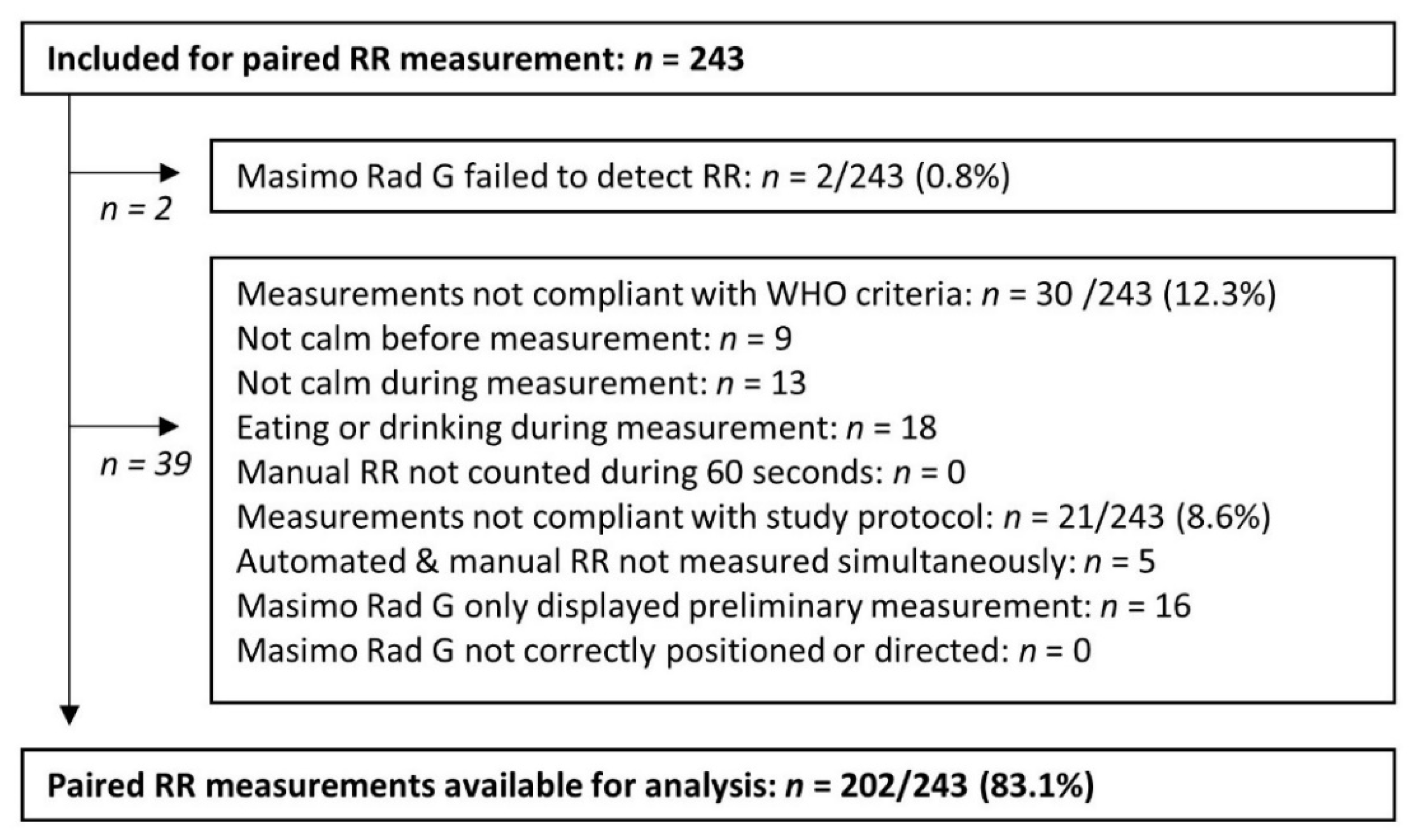
3.2. Description of Valid, Invalid and Unsuccesfull Paired RR Measurements
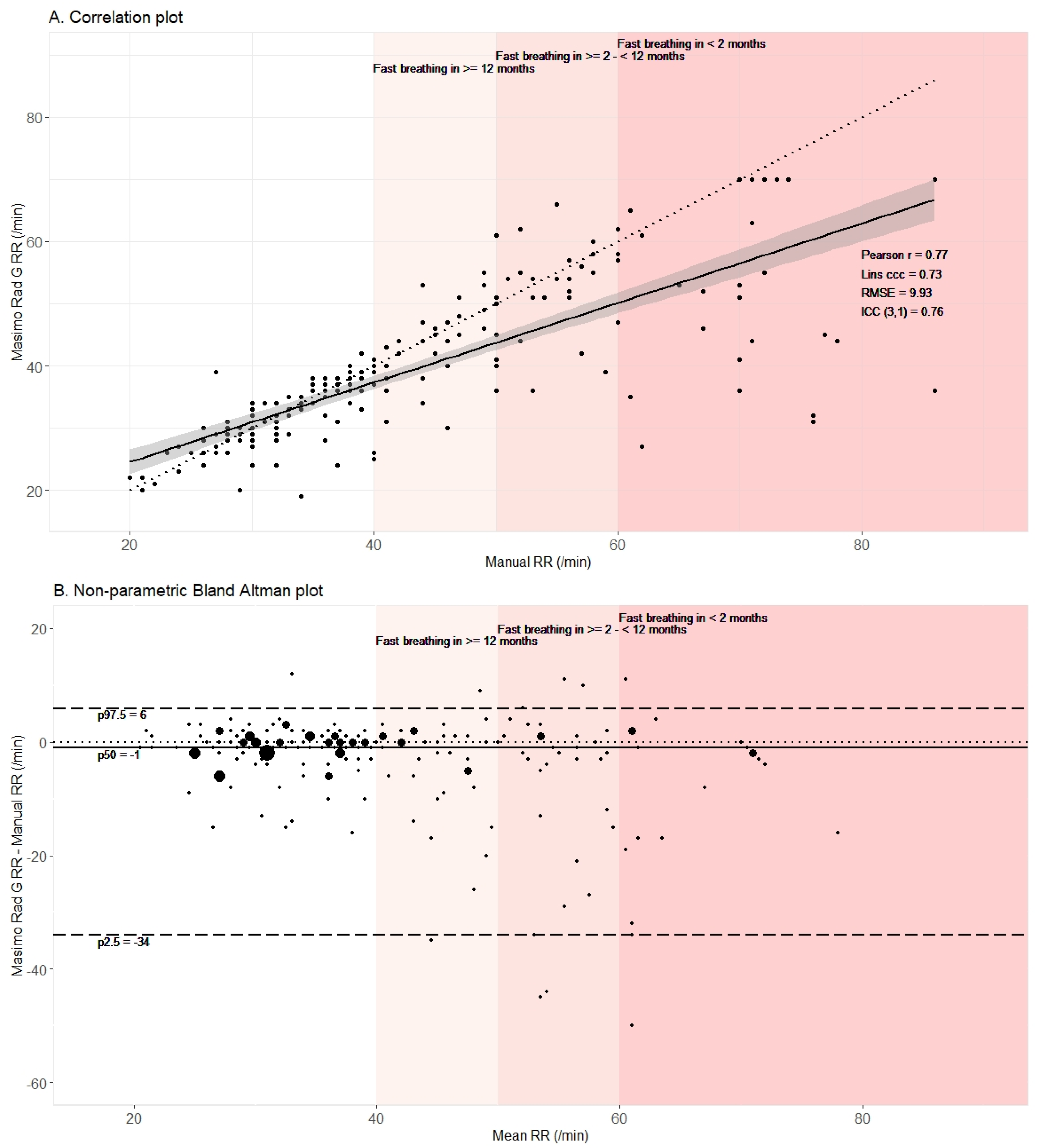
3.3. Automated Method Underestimated RR in Comparison to Manual Counting
3.4. Automated Method Failed to Adequately Detect Fast Breathing as Defined by Manual Counting
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Liu, L.; Oza, S.; Hogan, D.; Chu, Y.; Perin, J.; Zhu, J.; Lawn, J.E.; Cousens, S.; Mathers, C.; Black, R.E. Global, regional, and national causes of under-5 mortality in 2000–15: An updated systematic analysis with implications for the Sustainable Development Goals. Lancet 2016, 388, 3027–3035. [Google Scholar] [CrossRef] [Green Version]
- Roddy, P.; Dalrymple, U.; Jensen, T.O.; Dittrich, S.; Rao, V.B.; Pfeffer, D.A.; Twohig, K.A.; Roberts, T.; Bernal, O.; Guillen, E. Quantifying the incidence of severe-febrile-illness hospital admissions in sub-Saharan Africa. PLoS ONE 2019, 14, e0220371. [Google Scholar] [CrossRef] [Green Version]
- Daily, J. Fever Diagnostic Technology Landscape; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- World Health Organization. Integrated Management of Childhood Illnesses, 1st ed.; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- World Health Organization. Pocket Book of Hospital Care for Children: Guidelines for the Management of Common Childhood Illnesses, 2nd ed.; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Bhura, M.; Ariff, S.; Qazi, S.A.; Qazi, Z.; Ahmed, I.; Bin Nisar, Y.; Suhag, Z.; Soomro, A.W.; Soofi, S.B. Evaluating implementation of “management of Possible Serious Bacterial Infection (PSBI) when referral is not feasible” in primary health care facilities in Sindh province, Pakistan. PLoS ONE 2020, 15, e0240688. [Google Scholar] [CrossRef] [PubMed]
- Ogero, M.; Ayieko, P.; Makone, B.; Julius, T.; Malla, L.; Oliwa, J.; Irimu, G.; English, M. An observational study of monitoring of vital signs in children admitted to Kenyan hospitals: An insight into the quality of nursing care? J. Glob. Health 2018, 8, 010409. [Google Scholar] [CrossRef] [PubMed]
- Oresanya, O.; Counihan, H.; Nndaliman, I.; Alegbeleye, A.; Jiya, J.; Adesoro, O.; Dada, J.; Gimba, P.; Ozor, L.; Prosnitz, D.; et al. Effect of community-based intervention on improving access to treatment for sick under-five children in hard-to-reach communities in Niger State, Nigeria. J. Glob. Health 2019, 9, 010803. [Google Scholar] [CrossRef] [PubMed]
- Getachew, T.; Abebe, S.M.; Yitayal, M.; Persson, L.Å.; Berhanu, D. Assessing the quality of care in sick child services at health facilities in Ethiopia. BMC Health Serv. Res. 2020, 20, 1–12. [Google Scholar] [CrossRef]
- Ginsburg, A.S.; Lenahan, J.L.; Izadnegahdar, R.; Ansermino, J.M. A systematic review of tools to measure respiratory rate in order to identify childhood pneumonia. Am. J. Respir. Crit. Care Med. 2018, 197, 1116–1127. [Google Scholar] [CrossRef]
- Baker, K.; Alfvén, T.; Mucunguzi, A.; Wharton-Smith, A.; Dantzer, E.; Habte, T.; Matata, L.; Nanyumba, D.; Okwir, M.; Posada, M.; et al. Performance of four respiratory rate counters to support community health workers to detect the symptoms of pneumonia in children in low resource settings: A prospective, multicentre, hospital-based, single-blinded, comparative trial. EClinicalMedicine 2019, 12, 20–30. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Allen, J.; Zheng, D.; Chen, F. Recent development of respiratory rate measurement technologies. Physiol. Meas. 2019, 40, 07TR01. [Google Scholar] [CrossRef] [Green Version]
- UNICEF Supply Division Copenhagen. Target Product Profile Acute Respiratory Infection Diagnostic Aid (ARIDA); UNICEF: Copenhagen, Denmark, 2014.
- Baker, K.; Ward, C.; Maurel, A.; de Cola, M.A.; Smith, H.; Getachew, D.; Habte, T.; McWhorter, C.; LaBarre, P.; Karlstrom, J.; et al. Usability and acceptability of a multimodal respiratory rate and pulse oximeter device in case management of children with symptoms of pneumonia: A cross-sectional study in Ethiopia. Acta Paediatr. 2021, 110, 1620–1632. [Google Scholar] [CrossRef]
- Alwadhi, V.; Sarin, E.; Kumar, P.; Saboth, P.; Khera, A.; Gupta, S.; Kumar, H. Measuring accuracy of plethysmography based respiratory rate measurement using pulse oximeter at a tertiary hospital in India. Pneumonia 2020, 12, 4. [Google Scholar] [CrossRef] [PubMed]
- Dale, N.M.; Parshuram, C.; Tomlinson, G.; Shepherd, S.; Ashir, G.M.; Bukar, L.M.; Zlotkin, S. Performance of automated versus nurse-measured respiratory rate measurements in hospitalised malnourished children. Acta Paediatr. 2021, 110, 2249–2251. [Google Scholar] [CrossRef] [PubMed]
- Ward, C.; Baker, K.; Smith, H.; Maurel, A.; Getachew, D.; Habte, T.; McWhorter, C.; Labarre, P.; Karlstrom, J.; Black, J.; et al. Usability and acceptability of an automated respiratory rate counter to assess children for symptoms of pneumonia: A cross-sectional study in Ethiopia. Acta Paediatr. 2019, 109, 1196–1206. [Google Scholar] [CrossRef] [PubMed]
- Helldén, D.; Baker, K.; Habte, T.; Batisso, E.; Orsini, N.; Källander, K.; Alfvén, T. Does chest attachment of an automated respiratory rate monitor influence the actual respiratory rate in children under five? Am. J. Trop. Med. Hyg. 2020, 102, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Källander, K.; Ward, C.; Smith, H.; Bhattarai, R.; Ashish, K.C.; Timsina, D.; Lamichhane, B.; Maurel, A.; Ram Shrestha, P.; Baral, S.; et al. Usability and acceptability of an automated respiratory rate counter to assess childhood pneumonia in Nepal. Acta Paediatr. Int. J. Paediatr. 2020, 109, 1207–1220. [Google Scholar] [CrossRef] [PubMed]
- Baker, K. Acute Respiratory Infection Diagnostic Aid: Learnings and Next Steps. Malaria Consortium. 2019. Available online: https://www.malariaconsortium.org/resources/publications/1321/acute-respiratory-infection-diagnostic-aid-learnings-and-next-steps (accessed on 28 September 2021).
- Fouzas, S.; Priftis, K.N.; Anthracopoulos, M.B. Pulse oximetry in pediatric practice. Pediatrics 2011, 128, 740–752. [Google Scholar] [CrossRef] [Green Version]
- Land, K.J.; Boeras, D.I.; Chen, X.-S.; Ramsay, A.R.; Peeling, R.W. REASSURED diagnostics to inform disease control strategies, strengthen health systems and improve patient outcomes. Nat. Microbiol. 2019, 4, 46–54. [Google Scholar] [CrossRef]
- Fleming, K.A.; Horton, S.; Wilson, M.L.; Atun, R.; DeStigter, K.; Flanigan, J.; Sayed, S.; Adam, P.; Aguilar, B.; Andronikou, S.; et al. The Lancet Commission on diagnostics: Transforming access to diagnostics. Lancet 2021. [Google Scholar] [CrossRef]
- Turnbull, H.; Kasereka, M.C.; Amirav, I.; Sahika, S.E.; Solomon, I.; Aldar, Y.; Hawkes, M.T. Development of a novel device for objective respiratory rate measurement in low-resource settings. BMJ Innov. 2018, 4, 185–191. [Google Scholar] [CrossRef]
- Al-Halhouli, A.; Al-Ghussain, L.; El Bouri, S.; Habash, F.; Liu, H.; Zheng, D. Clinical evaluation of stretchable and wearable inkjet-printed strain gauge sensor for respiratory rate monitoring at different body postures. Appl. Sci. 2020, 10, 480. [Google Scholar] [CrossRef] [Green Version]
- Stasse, S.; Vita, D.; Kimfuta, J.; Da Silveira, V.C.; Bossyns, P.; Criel, B. Improving financial access to health care in the Kisantu district in the Democratic Republic of Congo: Acting upon complexity. Glob. Health Action 2015, 8, 25480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministère du Plan et Suivi de la Mise en Oeuvre de la Révolution de la Modernité, Ministère de la Santé Publique, ICF International. Democratic Republic of Congo Demographic and Health Survey 2013–2014: Key Findings; MPSMRM, MSP et ICF International: Rockville, MD, USA, 2014. [Google Scholar]
- Tack, B.; Phoba, M.-F.; Barbé, B.; Kalonji, L.M.; Hardy, L.; Van Puyvelde, S.; Ingelbeen, B.; Falay, D.; Ngbonda, D.; Van Der Sande, M.A.B.; et al. Non-typhoidal Salmonella bloodstream infections in Kisantu, DR Congo: Emergence of O5-negative Salmonella Typhimurium and extensive drug resistance. PLoS Negl. Trop. Dis. 2020, 14, e0008121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phoba, M.-F.; Lunguya, O.; Mayimon, D.V.; Lewo di Mputu, P.; Bertrand, S.; Vanhoof, R.; Verhaegen, J.; Van Geet, C.; Muyembe, J.J.; Jacobs, J. Multidrug-resistant Salmonella enterica, Democratic Republic of the Congo. Emerg. Infect. Dis. 2012, 18, 1692–1694. [Google Scholar] [CrossRef] [Green Version]
- Kalonji, L.M.; Post, A.; Phoba, M.-F.; Falay, D.; Ngbonda, D.; Muyembe, J.-J.; Bertrand, S.; Ceyssens, P.J.; Mattheus, W.; Verhaegen, J.; et al. Invasive salmonella infections at multiple surveillance sites in the Democratic Republic of the Congo, 2011–2014. Clin. Infect. Dis. 2015, 61, S346–S353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lunguya, O.; Lejon, V.; Phoba, M.-F.; Bertrand, S.; Vanhoof, R.; Glupczynski, G.; Verhaegen, J.; Muyembe-Tamfum, J.-J.; Jacobs, J. Antimicrobial resistance in invasive non-typhoid Salmonella from the Democratic Republic of the Congo: Emergence of decreased fluoroquinolone susceptibility and extended-spectrum Beta Lactamases. PLoS Negl. Trop. Dis. 2013, 7, e2103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, K.; Maurel, A.; Ward, C.; Getachew, D.; Habte, T.; McWhorter, C.; LaBarre, P.; Karlström, J.; Petzold, M.; Källander, K. Automated respiratory rate counter to assess children for symptoms of pneumonia: Protocol for cross-sectional usability and acceptability studies in Ethiopia and Nepal. JMIR Res. Protoc. 2020, 9, e14405. [Google Scholar] [CrossRef] [PubMed]
- Bunce, C. Correlation, agreement, and Bland-Altman Analysis: Statistical analysis of method comparison studies. Am. J. Ophthalmol. 2009, 148, 4–6. [Google Scholar] [CrossRef] [PubMed]
- Koo, T.K.; Li, M.Y. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- U.S. Department of Health and Human Services. Guidance for Industry and FDA Staff—Statistical Guidance on Reporting Results from Studies Evaluating Diagnostic Tests; U.S. Department of Health and Human Services: Rockville, MD, USA, 2007.
- English, M.; Berkley, J.; Mwangi, I.; Mohammed, S.; Ahmed, M.; Osier, F.; Muturi, N.; Ogutu, B.; Marsh, K.; Newton, C.R. Hypothetical performance of syndrome-based man-agement of acute paediatric admissions of children aged more than 60 days in a Kenyan district hospital. Bull. World Health Organ. 2003, 81, 166–173. [Google Scholar] [PubMed]
- Nadjm, B.; Amos, B.; Mtove, G.; Ostermann, J.; Chonya, S.; Wangai, H.; Kimera, J.; Msuya, W.; Mtei, F.; Dekker, D.; et al. WHO guidelines for antimicrobial treatment in children admitted to hospital in an area of intense Plasmodium falciparum transmission: Prospective study. BMJ 2010, 340, c1350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daw, W.J.; Kingshott, R.N.; Elphick, H.E. Poor inter-observer agreement in the measurement of respiratory rate in children: A prospective observational study. BMJ Paediatr. Open 2017, 1, e000173. [Google Scholar] [CrossRef] [PubMed]
- Lanaspa, M.; Valim, C.; Acacio, S.; Almendinger, K.; Ahmad, R.; Wiegand, R.; Bassat, Q. High reliability in respiratory rate assessment in children with respiratory symptomatology in a rural area in Mozambique. J. Trop. Pediatr. 2014, 60, 93–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartmann, V.; Liu, H.; Chen, F.; Hong, W.; Hughes, S.; Zheng, D. Toward accurate extraction of respiratory frequency from the photoplethysmogram: Effect of measurement site. Front. Physiol. 2019, 10, 732. [Google Scholar] [CrossRef]
- Hartmann, V.; Liu, H.; Chen, F.; Qiu, Q.; Hughes, S.; Zheng, D. Quantitative comparison of photoplethysmographic waveform characteristics: Effect of measurement site. Front. Physiol. 2019, 10, 198. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization; United Nations Children’s Fund; United Nations Population. Interagency List of Priority Medical Devices for Essential Interventions for Reproductive, Maternal, Newborn and Child Health; World Health Organization: Geneva, Switzerland, 2016.




{kind=link}
{kind=link}
{kind=link}
| Clinical Sign | Diagnostic Device/Technique | Definition |
|---|---|---|
| Respiratory rate | Manual or Automated RR with Rad G continuous pulse oximeter (Masimo, Irvine, CA, USA) | Fast breathing: <2 months: ≥60 breaths/min ≥2−<12 months: ≥50 breaths/min ≥12 months: ≥40 breaths/min |
| Heart rate | Rad G continuous pulse oximeter (Masimo, Irvine, CA, USA) | Tachycardia: <12 months: >160/min ≥12 months: >120/min |
| O2 saturation | Rad G continuous pulse oximeter (Masimo, Irvine, CA, USA) | Hypoxia: <90% |
| Tympanic temperature | Genius 3 (Covidien, Mansfield, USA) | Fever: >37.5 °C Hypothermia: <35.5 °C |
| Capillary hemoglobin | Hemocue 801 (Hemocue, Angelholm, Sweden) | Severe anemia: <5 g/dL Moderate anemia: ≥5−≤ 9.3 g/dL |
| Malnutrition | Weight: seca 876 scale (seca, Hamburg, Germany) | Severe acute malnutrition: - weight for height <−3 SD - peripheral upper arm circumference <115 mm if ≥6 months - or bilateral edema Moderate acute malnutrition: - weight for height ≥−3–<−2 SD - or peripheral upper arm circumference ≥115 mm−<125 mm if ≥6 months |
| Valid RR Measurements: n = 202 | Invalid RR Measurements: n = 39 i.e., Non-Compliance with WHO- Criteria or Study Protocol | ||
|---|---|---|---|
| Paired RR measurement | Median (p25–p75) or n (%) | p-value | |
| Manual RR counting (/min) | 39 (32–52) | 40 (34–52) | 0.32 |
| Fast breathing (according to WHO) | 87 (43.1%) | 19 (48.7%) | 0.64 |
| Automated RR counting (/min) | 36 (32–46) | 37 (34–46) | 0.31 |
| Fast breathing (according to WHO) | 68 (33.7%) | 12 (30.8%) | 0.87 |
| Clinical characteristics | Median (p25–p75) or n (%) | p-value | |
| Age | 0.14 Fisher | ||
| <2 months | 1 (0.5%) | 1 (2.6%) | |
| ≥2–<12 months | 60 (29.7%) | 15 (38.5%) | |
| ≥12 months | 141 (69.8%) | 23 (59.0%) | |
| Male gender | 104 (51.5%) | 15 (38.5%) | 0.19 |
| Weight (kg) | 9.8 (8.1–11.9) | 8.3 (6.8–10.9) | 0.03 |
| Tympanic temperature | 0.56 Fisher | ||
| Fever (>37.5 °C) | 57 (28.2%) | 14 (35.9%) | |
| Hypothermia (<35.5 °C) | 4 (2.0%) | 0 | |
| Tachycardia (according to WHO criteria) | 130 (64.4%) | 28 (71.8%) | 0.48 |
| Hypoxia (< 90%) | 8 (4.0%) | 1 (2.6%) | 1 Fisher |
| Respiratory distress (grunting/nasal flaring/chest retractions) | 47 (23.3%) | 8 (20.5%) | 0.87 |
| Anemia | 0.45 Fisher | ||
| Severe anemia (<5 g/dL) | 12 (5.9%) | 2 (5.1%) | |
| Moderate anemia (≥5–≤9.3 g/dL) | 117 (57.9%) | 27 (69.2%) | |
| Malnutrition (according to WHO) | 0.23 Fisher | ||
| Severe acute malnutrition | 25 (12.4%) | 8 (20.5%) | |
| Moderate acute malnutrition | 18 (8.9%) | 5 (12.8%) | |
| Malaria infection (positive microscopy) | 121 (59.9%) | 21 (53.8%) | 0.60 |
| Bloodstream infection (blood culture confirmed) | 18 (8.9%) | 3 (7.7%) | 1 Fisher |
| Fast Breathing by Manual Counting | No Fast Breathing by Manual Counting | Total | |
|---|---|---|---|
| Fast breathing by automated counting | 66 | 2 | 68 (33.7%) |
| No fast breathing by automated counting | 21 | 113 | 134 (66.3%) |
| Total | 87 (43.1%) | 115 (56.9%) | 202 |
| Agreement (95% CI) | PPA: 75.9% (65.3–84.1%) | NPA: 98.3% (93.2–99.7%) | Kappa: 0.76 (0.67–0.85) |
| Performance of the Automated Method in Comparison to Manual Counting | Fast Breathing Detected n = 66 | Failure to Detect Fast Breathing n = 21 | Odds Ratio Failure | |
|---|---|---|---|---|
| Clinical Characteristics | n (%) or Median (p25–p75) | OR (95% CI) | p-Value | |
| Infant (reference: ≥12 months) | 2.33 (0.77–7.23) | 0.12 | ||
| <2 months | 0 | 1 (4.8%) | ||
| ≥2−<12 months | 21 (31.8%) | 10 (47.6%) | ||
| Weight (kg) | 10 (8–12) | 9 (6–11) | 0.89 (0.74–1.07) | 0.21 |
| Fever (>37.5 °C) | 31 (47.0%) | 6 (28.6%) | 2.19 ( 0.70–7.79) | 0.21 |
| Respiratory distress (grunting/nasal flaring/chest retractions) | 29 (43.9%) | 7 (33.3%) | 0.64 (0.19–1.97) | 0.45 |
| Anemia (reference group: no anemia) | 0.66 (0.21–2.15) | 0.43 | ||
| Severe anemia(<5 g/dL) | 7 (10.6%) | 0 | ||
| Moderate anemia (≥5−≤9.3 g/dL) | 40 (60.6%) | 13 (61.9%) | ||
| Malnutrition (reference: no acute malnutrition) | ||||
| Severe acute malnutrition(according to WHO) | 9 (13.6%) | 6 (28.6) | 2.40 (0.60–9.16) | 0.19 |
| Moderate acute malnutrition(according to WHO) | 6 (9.1%) | 1 (4.8%) | 0.61 (0.01–5.73) | 1.0 |
| Malaria infection (positive microscopy) | 51 (77.3%) | 12 (57.1%) | 0.40 (0.12–1.28) | 0.09 |
| Bloodstream infection (blood culture confirmed) | 6 (9.1%) | 2 (9.5%) | 0.95 (0.15 –10.40) | 1.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tack, B.; Vita, D.; Mbaki, T.N.; Lunguya, O.; Toelen, J.; Jacobs, J. Performance of Automated Point-of-Care Respiratory Rate Counting versus Manual Counting in Children under Five Admitted with Severe Febrile Illness to Kisantu Hospital, DR Congo. Diagnostics 2021, 11, 2078. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11112078
Tack B, Vita D, Mbaki TN, Lunguya O, Toelen J, Jacobs J. Performance of Automated Point-of-Care Respiratory Rate Counting versus Manual Counting in Children under Five Admitted with Severe Febrile Illness to Kisantu Hospital, DR Congo. Diagnostics. 2021; 11(11):2078. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11112078
Chicago/Turabian StyleTack, Bieke, Daniel Vita, Thomas Nsema Mbaki, Octavie Lunguya, Jaan Toelen, and Jan Jacobs. 2021. "Performance of Automated Point-of-Care Respiratory Rate Counting versus Manual Counting in Children under Five Admitted with Severe Febrile Illness to Kisantu Hospital, DR Congo" Diagnostics 11, no. 11: 2078. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11112078