
Preclinical Validation of a Novel Injection-Molded Swab for the Molecular Assay Detection of SARS-CoV-2

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Preclinical Studies
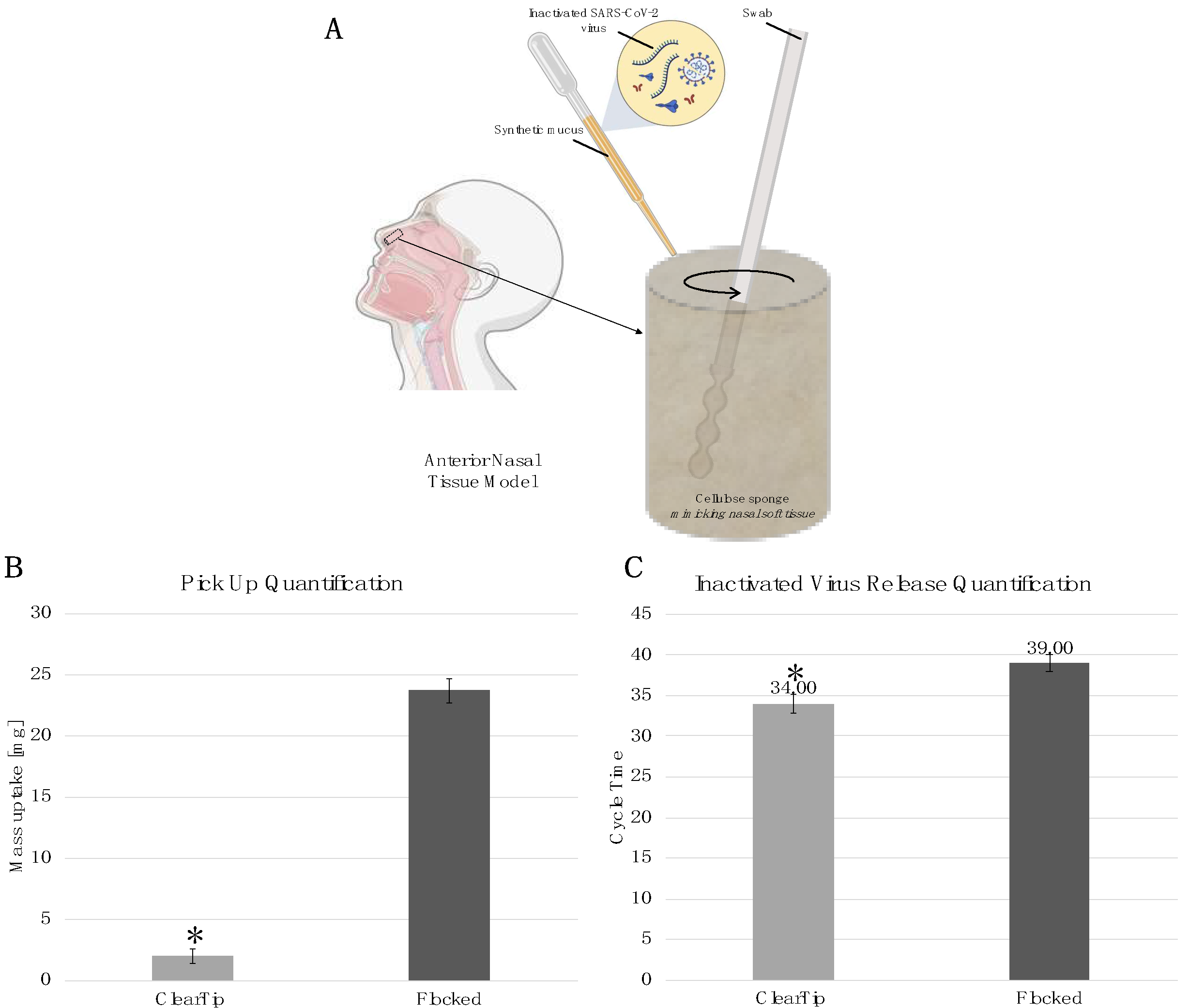
- Anterior Nasal Tissue Model Preparation
- 2.
- Pick-Up Swab Quantification
- 3.
- Swab Release Quantification
- 4.
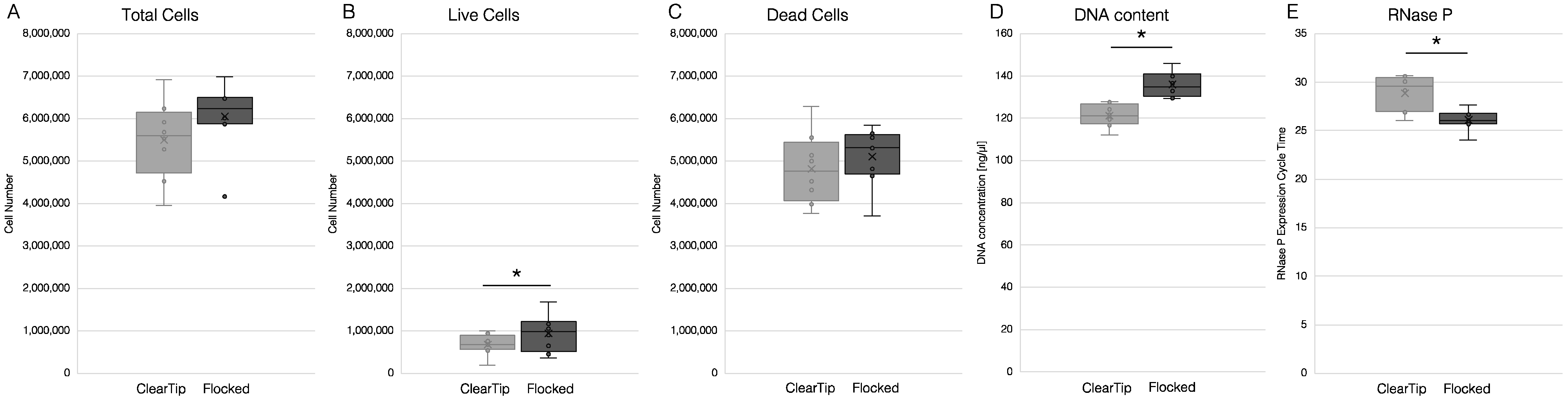
- Preclinical Human Sampling
2.3. Clinical Studies
2.3.1. Clinical Study I
- Study design and Oversight
- 2.
- Participants
- 3.
- Study procedures
2.3.2. Clinical Study II
- Study Design and Oversight
- 2.
- Participants
- 3.
- Study procedures
2.4. Statistical Analyses
3. Results
3.1. Benchtop Validation
3.2. Preclinical Human Sampling
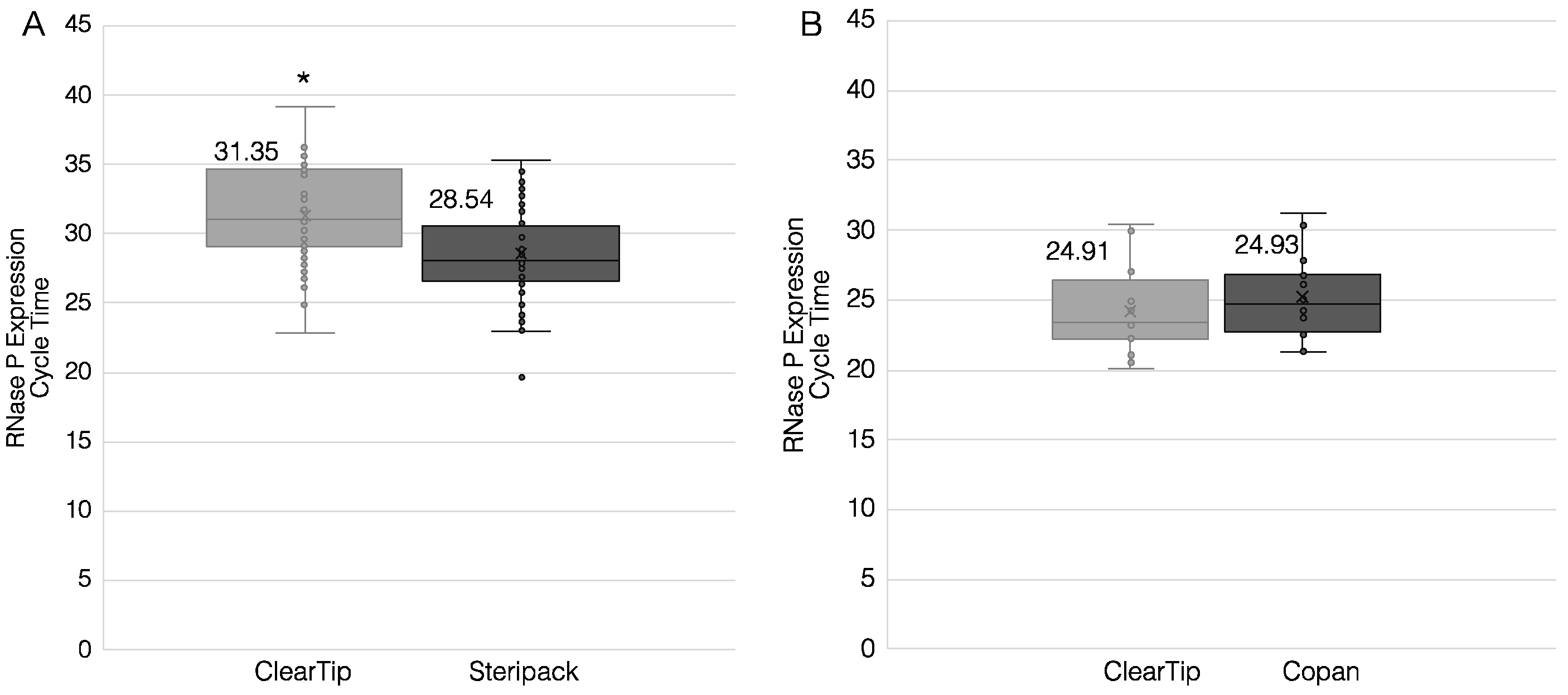
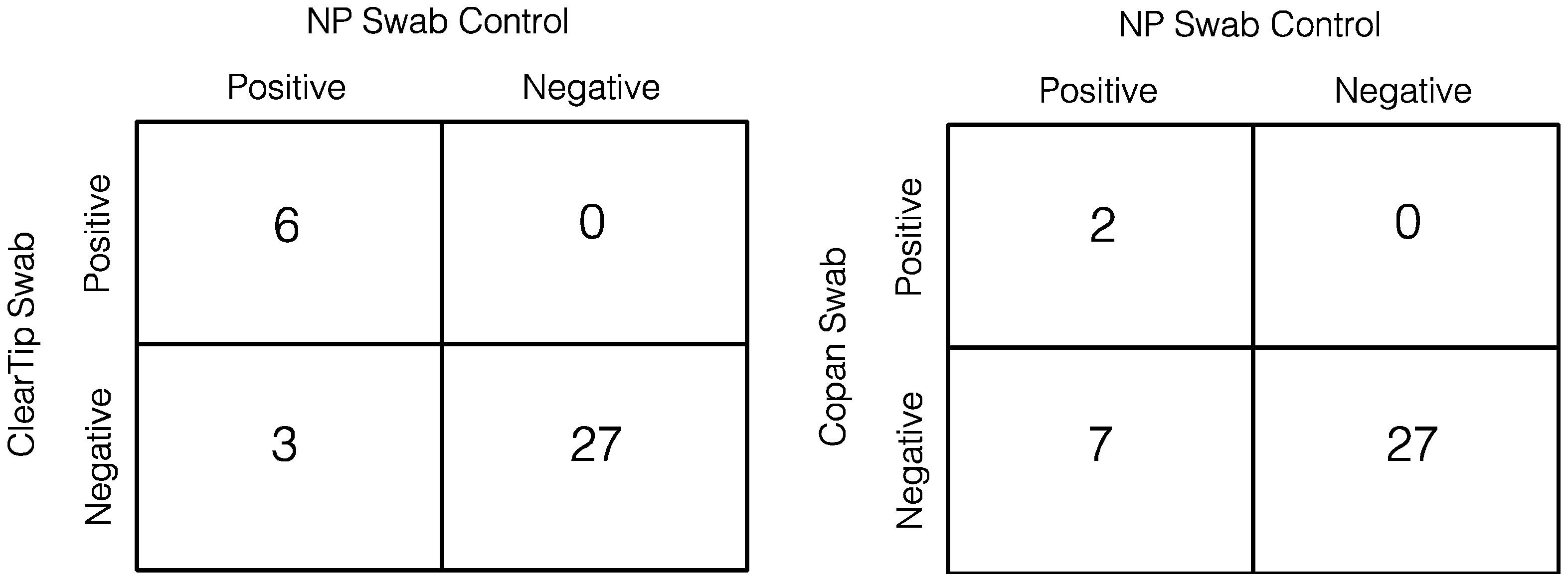
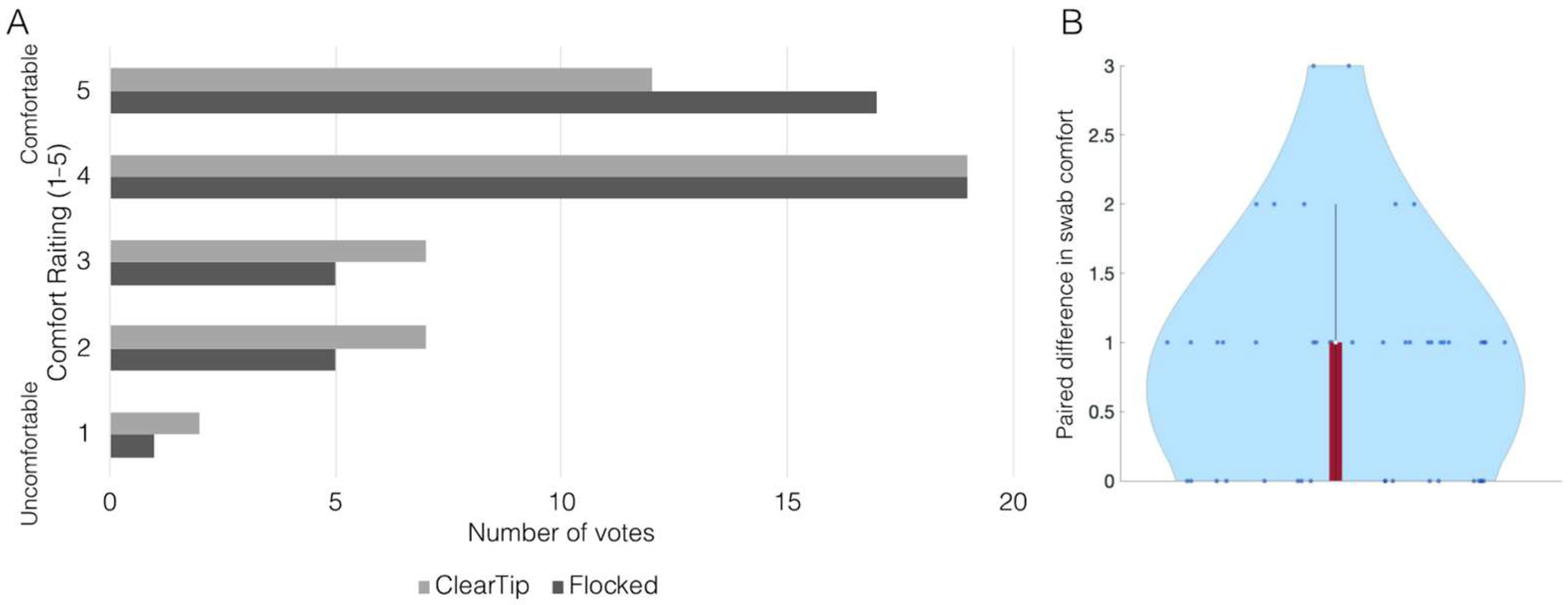
3.3. Clinical Studies
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Coronavirus Cases. Available online: https://www.worldometers.info/coronavirus/ (accessed on 27 July 2021).
- Zhao, H.-J.; Lu, X.-X.; Deng, Y.-B.; Tang, Y.-J.; Lu, J.-C. COVID-19: Asymptomatic carrier transmission is an underestimated problem. Epidemiol. Infect. 2020, 148, e116. [Google Scholar] [CrossRef] [PubMed]
- WHO. Laboratory Testing for 2019 Novel Coronavirus (2019-nCoV) in Suspected Human Cases. Interim Guidance. Available online: https://www.who.int/publications/i/item/10665-331501 (accessed on 27 July 2021).
- Callahan, C.J.; Lee, R.; Zulauf, K.E.; Tamburello, L.; Smith, K.P.; Previtera, J.; Cheng, A.; Green, A.; Azim, A.A.; Yano, A.; et al. Open Development and Clinical Validation of Multiple 3D-Printed Nasopharyngeal Collection Swabs: Rapid Resolution of a Critical COVID-19 Testing Bottleneck. J. Clin. Microbiol. 2020, 58, e00876-20. [Google Scholar] [CrossRef] [PubMed]
- Moisset, X.; Gautier, N.; Godet, T.; Parabère, S.; Pereira, B.; Meunier, E.; Gerbaud, L.; Lesens, O.; Henquell, C.; Beytout, J.; et al. Nasopharyngeal swab-induced pain for SARS-CoV-2 screening: A randomised controlled trial of conventional and self-swabbing. Eur. J. Pain 2021, 25, 924–929. [Google Scholar] [CrossRef]
- Marx, G.E.; Biggerstaff, B.J.; Nawrocki, C.C.; Totten, S.E.; Travanty, E.A.; Burakoff, A.W.; Scott, T.; De Hey, J.C.V.; Carlson, J.J.; Wendel, K.A.; et al. Detection of Severe Acute Respiratory Syndrome Coronavirus 2 on Self-Collected Saliva or Anterior Nasal Specimens Compared with Healthcare Personnel–Collected Nasopharyngeal Specimens. Clin. Infect. Dis. 2021, 73, S65–S73. [Google Scholar] [CrossRef]
- Péré, H.; Podglajen, I.; Wack, M.; Flamarion, E.; Mirault, T.; Goudot, G.; Hauw-Berlemont, C.; Le, L.; Caudron, E.; Carrabin, S.; et al. Nasal Swab Sampling for SARS-CoV-2: A Convenient Alternative in Times of Nasopharyngeal Swab Shortage. J. Clin. Microbiol. 2020, 58, e00721-20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pettit, M.E.; Boswell, S.A.; Qian, J.; Novak, R.; Springer, M. Accessioning and automation compatible anterior nares swab design. J. Virol. Methods 2021, 294, 114153. [Google Scholar] [CrossRef] [PubMed]
- Tay, J.K.; Cross, G.B.; Sun, L.; Chia, A.; Chee, J.; Loh, J.; Lim, Z.Y.; Ngiam, N.; Khang, W.P.; Yeap, S.; et al. Clinical Diagnostic Study of a Novel Injection Molded Swab for SARS-CoV-2 Testing. Infect. Dis. Ther. 2021, 10, 1015–1022. [Google Scholar] [CrossRef] [PubMed]
- Branche, A.R.; Walsh, E.E.; Formica, M.A.; Falsey, A.R. Detection of Respiratory Viruses in Sputum from Adults by Use of Automated Multiplex PCR. J. Clin. Microbiol. 2014, 52, 3590–3596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ren, T.; Wang, Q.; Xu, Y.; Cong, L.; Gou, J.; Tao, X.; Zhang, Y.; He, H.; Yin, T.; Zhang, H.; et al. Enhanced oral absorption and anticancer efficacy of cabazitaxel by overcoming intestinal mucus and epithelium barriers using surface polyethylene oxide (PEO) decorated positively charged polymer-lipid hybrid nanoparticles. J. Control. Release 2018, 269, 423–438. [Google Scholar] [CrossRef] [PubMed]
- Schuirmann, D.J. A comparison of the Two One-Sided Tests Procedure and the Power Approach for assessing the equivalence of average bioavailability. J. Pharmacokinet. Biopharm. 1987, 15, 657–680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kosinski, A.S. A weighted generalized score statistic for comparison of predictive values of diagnostic tests. Stat. Med. 2013, 32, 964–977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- U.S. Food & Drug. Administration. Medical Device Shortages During the COVID-19 Public Health Emergency. Available online: https://www.fda.gov/medical-devices/coronavirus-covid-19-and-medical-devices/medical-device-shortages-during-covid-19-public-health-emergency#shortage (accessed on 8 December 2021).
- Di Buduo, C.A.; Wray, L.S.; Tozzi, L.; Malara, A.; Chen, Y.; Ghezzi, C.E.; Smoot, D.; Sfara, C.; Antonelli, A.; Spedden, E.; et al. Programmable 3D silk bone marrow niche for platelet generation ex vivo and modeling of megakaryopoiesis pathologies. Blood 2015, 125, 2254–2264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghezzi, C.E.; Marelli, B.; Donelli, I.; Alessandrino, A.; Freddi, G.; Nazhat, S.N. Multilayered dense collagen-silk fibroin hybrid: A platform for mesenchymal stem cell differentiation towards chondrogenic and osteogenic lineages. J. Tissue Eng. Regen. Med. 2017, 11, 2046–2059. [Google Scholar] [CrossRef] [PubMed]
- Ghezzi, C.E.; Marelli, B.; Muja, N.; Nazhat, S.N. Immediate production of a tubular dense collagen construct with bioinspired mechanical properties. Acta Biomater. 2012, 8, 1813–1825. [Google Scholar] [CrossRef] [PubMed]
- Ghezzi, C.E.; Marelli, B.; Omenetto, F.G.; Funderburgh, J.L.; Kaplan, D.L. 3D Functional Corneal Stromal Tissue Equivalent Based on Corneal Stromal Stem Cells and Multi-Layered Silk Film Architecture. PLoS ONE 2017, 12, e0169504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siran, W.; Ghezzi, C.E.; Cairns, D.M.; Pollard, R.E.; Chen, Y.; Gomes, R.; McKay, T.B.; Pouli, D.; Jamali, A.; Georgakoudi, I.; et al. Human Corneal Tissue Model for Nociceptive Assessments. Adv. Heal. Mater. 2018, 7, e1800488. [Google Scholar] [CrossRef] [PubMed]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghezzi, C.E.; Hartigan, D.R.; Hardick, J.P.; Gore, R.; Adelfio, M.; Diaz, A.R.; McGuinness, P.D.; Robinson, M.L.; Buchholz, B.O.; Manabe, Y.C. Preclinical Validation of a Novel Injection-Molded Swab for the Molecular Assay Detection of SARS-CoV-2. Diagnostics 2022, 12, 206. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12010206
Ghezzi CE, Hartigan DR, Hardick JP, Gore R, Adelfio M, Diaz AR, McGuinness PD, Robinson ML, Buchholz BO, Manabe YC. Preclinical Validation of a Novel Injection-Molded Swab for the Molecular Assay Detection of SARS-CoV-2. Diagnostics. 2022; 12(1):206. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12010206
Chicago/Turabian StyleGhezzi, Chiara E., Devon R. Hartigan, Justin P. Hardick, Rebecca Gore, Miryam Adelfio, Anyelo R. Diaz, Pamela D. McGuinness, Matthew L. Robinson, Bryan O. Buchholz, and Yukari C. Manabe. 2022. "Preclinical Validation of a Novel Injection-Molded Swab for the Molecular Assay Detection of SARS-CoV-2" Diagnostics 12, no. 1: 206. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12010206