1. Introduction
Venous thromboembolism is the third most common cause of cardiovascular disease worldwide, following coronary artery disease and stroke [
1]. Its incidence has dramatically increased over the last two decades [
1,
2]. Venous thromboembolism occurs in two forms: pulmonary embolism and deep vein thrombosis (DVT). DVT is often associated with recurrent pulmonary embolism and venous thromboembolism [
3]. Recurrence rates during the disease course are approximately 20–36% [
4,
5]. Computed tomography (CT) venography of the lower extremities presents the most common diagnostic tool for ascertaining DVT [
4]. CT imaging has evolved from being a primary diagnostic tool to a critical component of individualized precision medicine [
6].
Visual analysis of CT scans to diagnose DVT is time-consuming and subjective, whereas computer classification is significantly faster and more objective. Radiomics is a unique tool for clinical diagnosis that extracts mineable high-throughput features from medical images using automated algorithms [
7]. Radiomics approaches have been widely applied in CT image interpretation throughout the last decade, and they have demonstrated promising results in differential diagnoses [
8]. Although radiomics models operate within an acceptable error range for specific tasks, radiomics-based techniques have a number of drawbacks. Handcrafted radiomic features, for example, are limited to current medical imaging expertise and prior operator experience and knowledge. As a result, these characteristics might not be properly representative [
9].
A convolutional neural network (CNN) can extract and learn deep features directly in a data-driven way, as opposed to traditional radiomics methods that rely on handcrafted features [
10]. In various deep-running fields, CNN is of high performance in image recognition, and many studies are based on CNNs in medical imaging, including various vision sectors [
11,
12]. CNN methods perform well in image classification and in the recognition of medical imaging [
13]. These architectures have strong potential for enhancing workflow processes in radiology. During the training phase, however, classification labels without lesion information may not provide effective supervised information on the suspected lesion area. This could make it difficult for CNN classification to extract useful information about lesions, especially small lesions, resulting in poor performance.
In this study, we used a large dataset comprising lower-extremity CT venography images to demonstrate the effectiveness of the proposed methodology for the automated classification of DVT lesions. We extensively evaluated the classification performance of two model types (CNN and conventional machine learning). The aim of the present study was to determine the feasibility of classifying DVT upon CT venography using suitable CNN method.
2. Materials and Methods
2.1. Study Design
This single-center retrospective study was approved by the institutional review board of our local ethics committee. This study was conducted in accordance with the principles of the Declaration of Helsinki. The requirement for written informed consent was waived given the retrospective nature of our study.
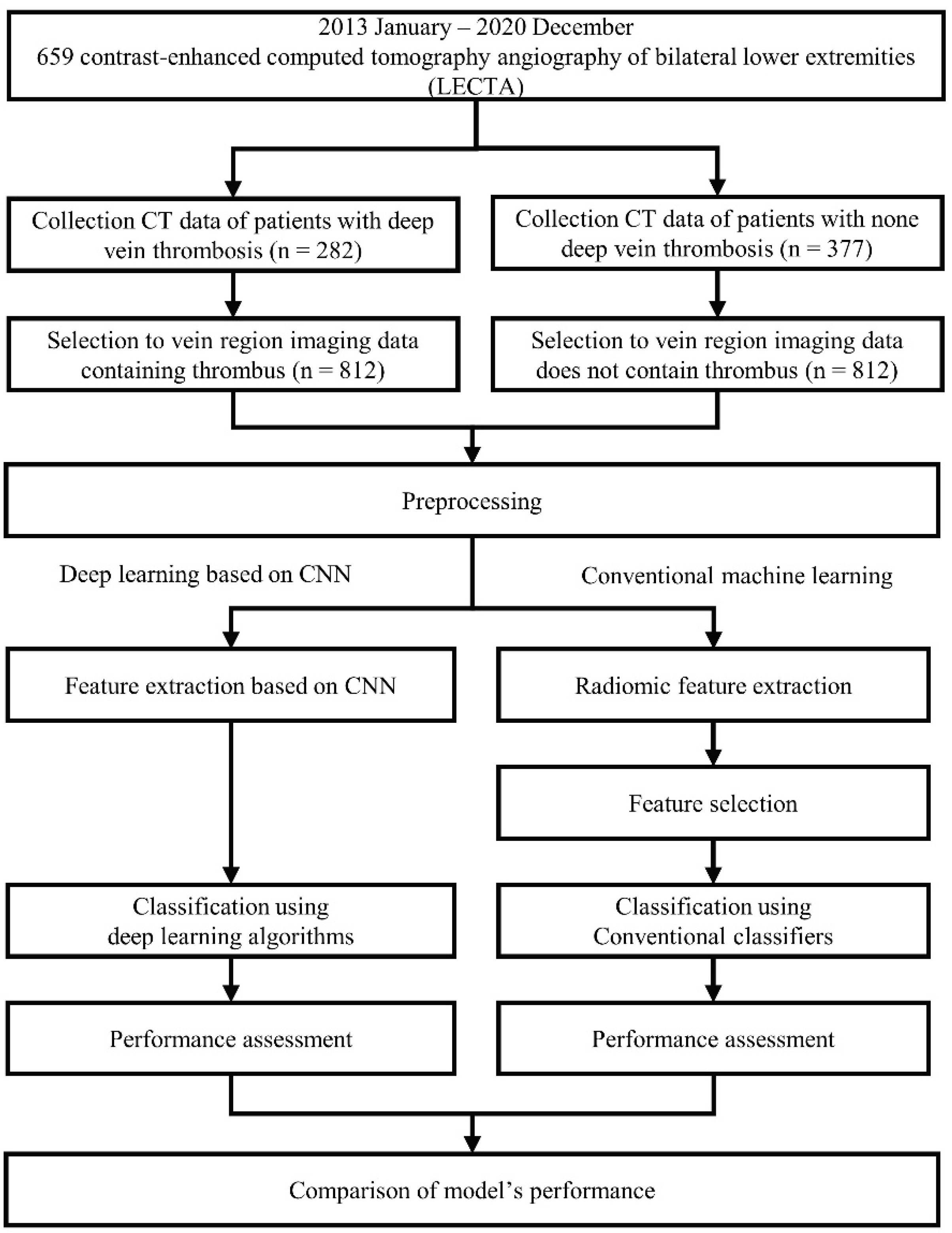
In this study, among the artificial intelligence (AI) algorithms, we define the machine-learning, which yields decision with specific function by parsing generated features and requires adjustment of engineer (such as feature selection) for prediction as “conventional machine learning”. The algorithms, which create features and make decisions on its own deep network are defined as “deep learning”. To distinguish the presence or absence of thrombosis in deep veins through image-based analyses, we applied four classifiers using embedded feature selection methods based on conventional machine learning as well as four deep learning algorithms based on CNN. We compared quantitative differences in performance and investigated the best model for classifying blood vessels into two categories. Moreover, we evaluated the likely reason for the obtained results according to each method’s classifier and structure.
Figure 1 shows the flowchart of the study design and process.
2.2. Data Acquisition and Preprocessing
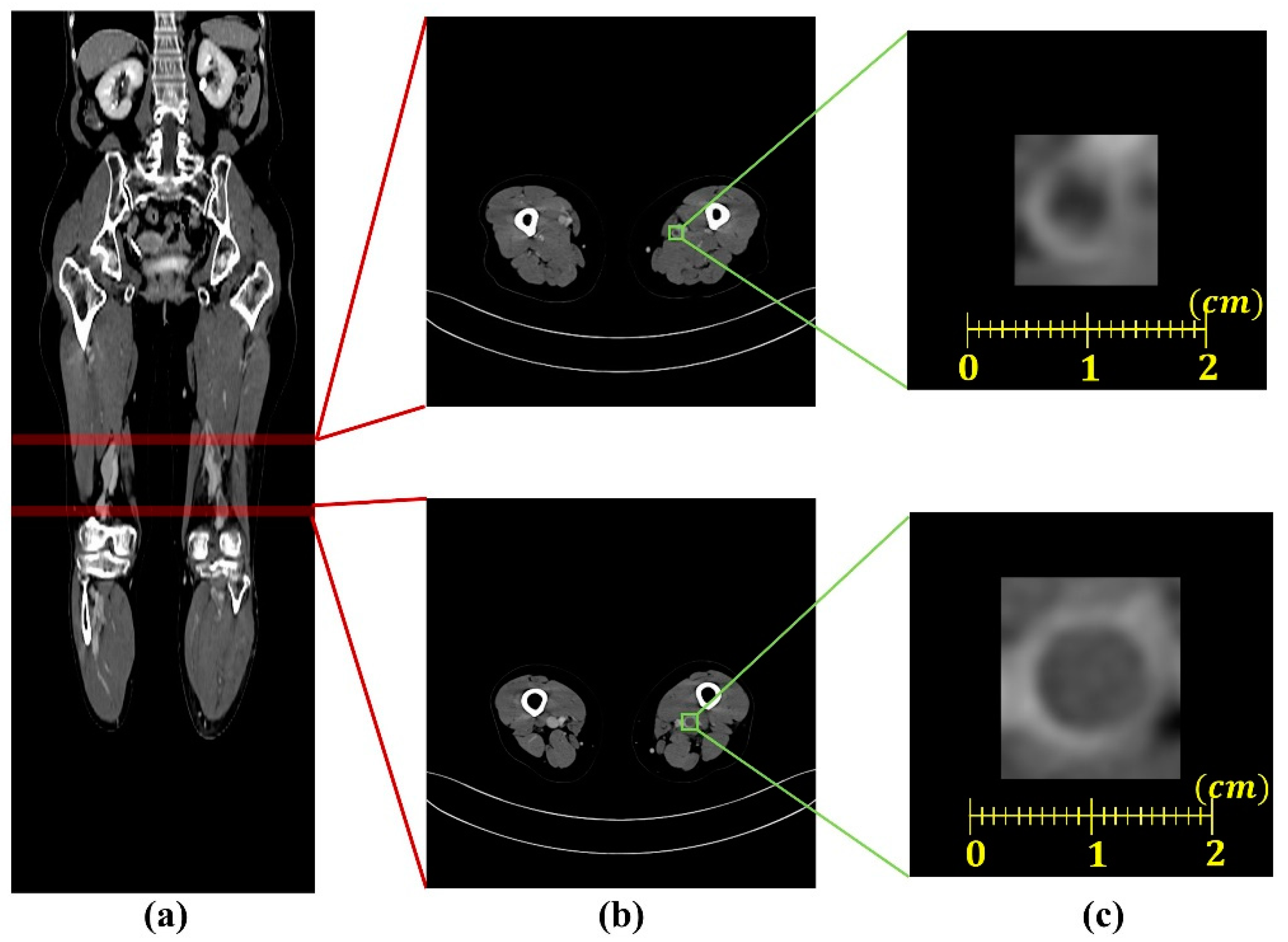
CT images from 282 patients with deep vein thrombosis and 377 patients with non-deep vein thrombosis (designated as healthy controls) were retrospectively collected from the Gil Medical Center (Incheon, Republic of Korea) in DICOM (digital imaging and communications in medicine) format. Each CT image window setting was set to a window width of 140HU and window level of 400HU for enhancing the contrast between the blood vessel walls and the thrombus. Because the range of pixel spacing was wide (0.695–0.977 mm
2) and the regions of the deep veins were diminutive, we uniformed the spacing of pixel to a mean value (0.891 mm
2) of the pixel spacing range. As shown in
Figure 2, from this preprocessed data, we selected 812 images of the deep vein region with thrombus from patients with deep vein thrombosis and 812 images of the deep vein region from non-deep vein thrombosis patients. Among the total of 1624 image data (deep vein with thrombus,
n = 650; healthy deep vein without thrombus,
n = 650), 976 data and 324 data were used for the training and validation set, respectively. The remaining 324 data from the total, excluding the training and validation set, were used as the testing set to evaluate performance.
2.3. Classification Using Conventional Machine Learning
Statistical texture analysis is a method for analyzing the distributions and correlations of brightness values in image pixels using mathematical methods. Statistical-based methods include first-order statistics calculated using feature values based on histograms within the region of interest (ROI) as well as second-order statistics measured from matrices formed based on the frequencies and relationships for each pixel value in the gray level [
14]. The first-order statistics and second-order statistics are used for classifying images [
13,
14]. Therefore, we applied radiomic features of first order statistics and second-order statistics to a conventional machine learning classifier for classifying the images. [
15,
16]. From a total of 1624 images, we extracted 74 features as follows: 18 from first-order statistics, 56 from second-order statistics (of which 24 were generated from gray level co-occurrence matrices [GLCM], 16 were generated from gray level run length matrices [GLRLM], and 16 were generated from gray level size zone matrices [GLSZM]) using the Python PyRadiomics module (version 3.0.1; Computational Imaging and Bioinformatics Lab, Harvard Medical School, Boston, MA, USA).
The conventional machine learning algorithms are generally efficient in terms of computational power and memory through a feature selection process. Moreover, model performance is improved by removing the features that adversely affect learning in the process. Feature selection methods are generally divided into three types: filter methods, wrapper methods, and embedded methods. Each method selects a suitable subset of features for classification.
The filter method ranks each feature by calculating the relevance of features based on performance evaluation metrics and leaves a specified number of features in the highest order. The wrapper method is used to find the best feature subset while repeating the training via the algorithm. The embedded method internally selects a subset of features from the machine learning algorithm. The filter method selects features independent of the machine learning algorithm. Thus, the selected features do not affect the final classifier. The wrapper method has a high probability of overfitting and is time consuming. However, the embedded method is more accurate than the filter method because it selects features based on a machine learning algorithm (e.g., the wrapper method) and is likewise advantageous in terms of computational aspects [
17]. Therefore, this study used an embedded method that takes advantage of each filter method, including the wrapper method.
The conventional machine learning algorithms used in the current study were logistic regression (LR), support vector machines (SVM), random forests (RF), and extreme gradient boosts (XGB). LR is an algorithm that uses regression to classify data by predicting the probability that data will be included in a particular category as a value between 0 and 1 [
18]. SVM is an algorithm for defining the optimal decision boundary to categorize data using support vectors, meaning that the data point is near the decision boundary [
19]. RF is a tree-based algorithm that draws conclusions by collecting classification results from multiple trees constructed through training [
20]. XGB is likewise a tree-based algorithm. In the classification process comprising multiple decision trees, weights are provided for incorrect answers through the gradient of the loss function to predict results. Rapid training is possible through parallel processing [
21]. The features selected from each algorithm are listed in
Table 1.
2.4. Classification Based on Deep Learning
Among deep learning methodologies, CNN-based deep learning (extracting features using convolution operations) has recently been applied in medical imaging, showing high performance [
22,
23]. VGGnet is one of the deep learning networks designed to investigate the relationship between network depth and accuracy. VGGnet uses fewer parameters as compared with previously proposed convolution networks. Specifically, VGG uses a 3 × 3 convolution filter for all layers and obtains a superior performance by implementing a deeper network structure. VGGnet generally shows good performance and has been applied to many networks [
24]. ResNet is a structure in which the output of the previous layer is connected to the input of the subsequent layer through a skip connection in order to enable learning using a deeper network structure [
25]. In this study, we used four CNN-based deep learning models (VGG16, VGG19, Resnet50, and Resnet152) to investigate the most effective model for classifying and differentiating normal veins and thrombosis containing veins as well as analyzing the obtained results according to the depth of the network. The experiments were performed in Python 3.6.10 (Python Software Foundation, Wilmington, DE, USA) using Keras 2.2.5 frameworks (Keras Global Limited, London, UK) on a Ubuntu 14.04 operating system (London, UK) with two NVIDIA Tesla P100 graphics processing units (GPUs; NVIDIA Corporate, Santa Clara, CA, USA) and 512 GB of random access memory (RAM).
2.5. Performance Evaluation
To evaluate the effectiveness of each algorithm, a performance evaluation was conducted using 324 test data that were not used for training. We calculated true positives (TP), false positives (FP), false negatives (FNs), and true negatives (TNs). Sensitivity, specificity, and accuracy were calculated according to Equations (1)–(3) specified below. Receiver operating characteristic (ROC) curves were estimated using these sensitivity and specificity values. Algorithm performances were compared according to area under the curve (AUC) values derived from ROC curves.
3. Results
We evaluated the performance of each model by applying fivefold cross-validation to assess model robustness. The results, including associated 95% confidence intervals, are shown in
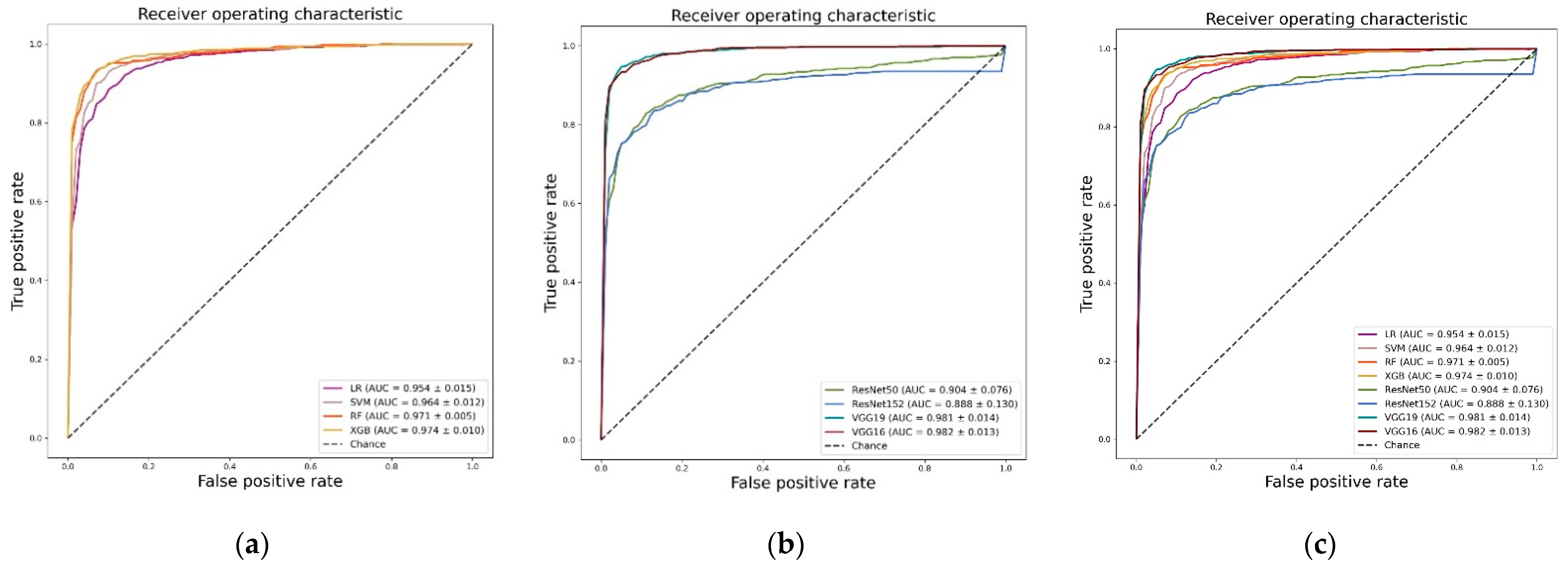
Table 2. The highest values are shown in bold. Based on AUC values, the algorithm with the highest performance was identified as the deep learning-based VGG16 network (0.982 ± 0.014), followed by the VGG19 model (0.981 ± 0.013). The VGG19 model added layers to the same model. Among the machine learning algorithms, XGB showed the highest performance (0.969 ± 0.005), with a difference of 0.007 as compared with VGG16.
Figure 3a–c shows the ROC curves, AUC values, and standard deviations for each model.
Table 3 and
Figure 3c shows a comparison between the average performances of machine learning-based algorithms and the average performances of deep learning-based algorithms. The deep learning algorithms showed a mean AUC of 0.939 (±0.043), a mean sensitivity of 0.897 (±0.057), a mean specificity of 0.894 (±0.028), and a mean accuracy of 0.890 (±0.045). The machine learning algorithms showed mean AUCs of 0.966 (±0.008), 0.917 (±0.025), 0.917 (±0.009), and 0.931 (±0.031), respectively. As demonstrated in
Table 2, the algorithm with the highest overall performance was the deep learning-based VGG16 model. The average algorithm performance was higher within the machine learning models. Additionally, the performances of machine learning algorithms did not meaningfully differ according to the classifier when standard deviation was considered. However, in the case of the deep learning models, we observed a substantial difference in performance depending on the model.
4. Discussion
In this study, we evaluated 659 patients who underwent CT venography in order to detect DVT and investigate quantitative differences in performance with respect to automated classification of DVT using conventional machine learning and CNN models. As shown in
Table 2 and
Figure 3c, the algorithm that demonstrated the highest performance based on AUC values was the deep learning-based VGG16 model. CNN-based models, which differ from conventional machine learning methods necessitating manual steps with respect to feature extraction and selection, extract meaningful feature maps for training from convolutional layers. CNN demonstrates high performance through fitting a model using many parameters extracted through this process and has proven its validity within the current study. The VGG16 model based on CNN obtained an AUC value that was 0.007 higher than the XGB algorithm (which showed the highest performance among the conventional machine learning algorithms). Therefore, an appropriate amount of data (in terms of efficacy for deep learning) was used in this study. We determined that the deep learning-based algorithm extracted features more effectively with respect to classification as compared with manual feature extraction and feature selection based on statistical texture analysis. However, as shown in
Figure 3b, the CNN-based ResNet model exhibited a statistically significantly lower performance. This result was likely due to the size of the image used as well as the deep structure of the Resnet-based model. Because the blood vessel area is quite small, the image size of the initial data was likewise small. Therefore, we judged that the high-dimensional features extracted from the deep layer were hindered in classifying the test data because of the information generated during the up-sampling process.
Conventional machine learning algorithms showed an overall high classification performance with an average AUC of 0.95 or more. We analyzed the features used for classification within the current study. In conventional machine learning algorithms, all algorithms select for the median, the median value of the gray level intensity, skewness, and the measured value of the asymmetry of the histogram via first-order statistics. Two features are predicted as having the most statistically significant impact on classifying the two categories. Features are ranked in the top 10 in order of importance for all four algorithms. The tree-based models (i.e., RF and XGB) with relatively high performances have the following features in common: mean (the mean values of gray level intensity), root mean squared (the square-root values of the mean of all the squared intensity), gray level variance (the variance of intensities for the gray level zones), and zone percentage (the ratio of the number of gray level zones and the number of connected voxels). Specifically, the GLCM-based cluster shade feature showed the highest feature importance for both models and had the most effective influence on classification in the current study. Additionally, in comparing performance differences according to classifier type, tree-based RF and XGB models and deep learning-based VGG models (i.e., nonlinear classifiers) showed higher performance compared to LR and SVM (i.e., linear classifiers). This indicates that our data are more suitable for nonlinear classifiers.
This study had several limitations. First, this retrospective study only considered data from a single medical center, leading to the possibility of selection bias. With the initiative towards prospective studies within academic medicine as well as pharmaceutical initiatives, we need to be prepared to accept AI in clinical practice. Second, the modest number of normal cases evaluated via CT venography hindered the training and validation of the CNN within the current study. Nevertheless, we considered patients with DVT in the clinical setting in order to minimize the spectrum bias. Third, we did not assess performance using coronal or sagittal reformatted CT images. Combining several CT images may improve performance. This prospective methodology should be investigated in the future.
In summary, we evaluated conventional machine learning and CNN-based methods for classifying DVT using a large dataset of CT venography in the current study. We found that CNN models classified DVT on serial CT images more effectively, especially via the VGG16 model and showed more accuracy in distinguishing DVT with a slightly higher AUC value as compared with the other AI algorithms. Our findings guide future research directions and will ultimately inform medical guidelines.
Author Contributions
J.H.H. and J.W.S. were responsible for data acquisition and data analysis as well as drafting the manuscript. J.H.K. and K.G.K. conceived the study and study design, performed the statistical and computational work, and performed most of the assays. S.P. and Y.J.K. participated in the writing of the paper and in analyzing the study data. All authors reviewed authorship criteria within a previously submitted version and agreed to the authorship based on the specified criteria. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the GRRC program of Gyeonggi province. [GRRC-Gachon2020(B01), AI-based Medical Image Analysis, and by the Gachon Gil Medical Center(FRD2019-11-02(3)), and by the Gachon Program (GCU-202106290001).
Institutional Review Board Statement
All procedures performed in human participants were conducted in accordance with the Declaration of Helsinki and were approved by the Institutional Ethical Committee at Gachon University Gil Medical Center (protocol GAIRB2021-225, approval 13 July 2021).
Informed Consent Statement
Not applicable.
Data Availability Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare that they have no actual or potential competing financial or non-financial interests.
References
- Glynn, R.J.; Rosner, B. Comparison of risk factors for the competing risks of coronary heart disease, stroke, and venous thromboembolism. Am. J. Epidemiol. 2005, 162, 975–982. [Google Scholar] [CrossRef] [PubMed]
- Danin-Mankowitz, H.; Ugarph-Morawski, A.; Braunschweig, F.; Wandell, P. The risk of venous thromboembolism and physical activity level, especially high level: A systematic review. J. Thrombsis Thrombolysis 2021, 52, 508–516. [Google Scholar] [CrossRef] [PubMed]
- Di Nisio, M.; van Es, N.; Büller, H.R. Deep vein thrombosis and pulmonary embolism. Lancet 2016, 388, 3060–3073. [Google Scholar] [CrossRef]
- Chopard, R.; Albertsen, I.E.; Piazza, G. Diagnosis and Treatment of Lower Extremity Venous Thromboembolism: A Review. JAMA 2020, 324, 1765–1776. [Google Scholar] [CrossRef]
- Khan, F.; Rahman, A.; Carrier, M.; Kearon, C.; Weitz, J.I.; Schulman, S.; Rodger, M.A. Long term risk of symptomatic recurrent venous thromboembolism after discontinuation of anticoagulant treatment for first unprovoked venous thromboembolism event: Systematic review and meta-analysis. BMJ 2019, 366, l4363. [Google Scholar] [CrossRef] [Green Version]
- Lambin, P.; Leijenaar, R.T.H.; Deist, T.M.; Peerlings, J.; de Jong, E.E.C.; van Timmeren, J.; Walsh, S. Radiomics: The bridge between medical imaging and personalized medicine. Nat. Rev. Clin. Oncol. 2017, 14, 749–762. [Google Scholar] [CrossRef]
- Bhandari, A.; Ibrahim, M.; Sharma, C.; Liong, R.; Gustafson, S.; Prior, M. CT-based radiomics for differentiating renal tumours: A systematic review. Abdom. Radiol. 2021, 46, 2052–2063. [Google Scholar] [CrossRef]
- Zhou, Z.; Li, S.; Qin, G.; Folkert, M.; Jiang, S.; Wang, J. Multi-Objective-Based Radiomic Feature Selection for Lesion Malignancy Classification. IEEE J. Biomed. Health Inform. 2020, 24, 194–204. [Google Scholar] [CrossRef]
- Lao, J.; Chen, Y.; Li, Z.C.; Li, Q.; Zhang, J.; Liu, J.; Zhai, G. A Deep Learning-Based Radiomics Model for Prediction of Survival in Glioblastoma Multiforme. Sci. Rep. 2017, 7, 10353. [Google Scholar] [CrossRef]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef]
- Tajbakhsh, N.; Shin, J.Y.; Gurudu, S.R.; Hurst, R.T.; Kendall, C.B.; Gotway, M.B.; Liang, J. Convolutional neural networks for medical image analysis: Full training or fine tuning? IEEE Trans. Med. Imaging 2016, 35, 1299–1312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anwar, S.M.; Majid, M.; Qayyum, A.; Awais, M.; Alnowami, M.; Khan, M.K. Medical image analysis using convolutional neural networks: A review. J. Med. Syst. 2018, 42, 1–13. [Google Scholar]
- Ker, J.; Wang, L.; Rao, J.; Lim, T. Deep learning applications in medical image analysis. IEEE Access 2017, 6, 9375–9389. [Google Scholar] [CrossRef]
- Davnall, F.; Yip, C.S.; Ljungqvist, G.; Selmi, M.; Ng, F.; Sanghera, B.; Goh, V. Assessment of tumor heterogeneity: An emerging imaging tool for clinical practice? Insights Imaging 2012, 3, 573–589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haralick, R.M.; Shanmugam, K.; Dinstein, I. Textural Features for Image Classification. IEEE Trans. Syst. Man Cybern. 1973, 6, 610–621. [Google Scholar]
- Materka, A.; Strzelecki, M. Texture Analysis Methods—A Review. COST B11 Report 1998, 10, 4968. [Google Scholar]
- Liu, H.; Zhou, M.; Liu, Q. An embedded feature selection method for imbalanced data classification. IEEE/CAA J. Autom. Sin. 2019, 6, 703–715. [Google Scholar] [CrossRef]
- Vapnik, V.N. An overview of statistical learning theory. IEEE Trans. Neural Netw. 1999, 10, 988–999. [Google Scholar] [CrossRef] [Green Version]
- Breiman, L. Random forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef] [Green Version]
- Cortes, C.; Vapnik, V. Support-vector networks. Mach. Learn. 1995, 20, 273–297. [Google Scholar] [CrossRef]
- Chen, T.; Guestrin, C. (Eds.) Xgboost: A scalable tree boosting system. In Proceedings of the 22nd ACM Sigkdd International Conference on Knowledge Discovery and Data Mining, San Francisco, CA, USA, 13–17 August 2016. [Google Scholar]
- Lee, J.-G.; Jun, S.; Cho, Y.-W.; Lee, H.; Kim, G.B.; Seo, J.B.; Kim, N. Deep learning in medical imaging: General overview. Korean J. Radiol. 2017, 18, 570–584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torres-Velázquez, M.; Chen, W.-J.; Li, X.; McMillan, A.B. Application and construction of deep learning networks in medical imaging. IEEE Trans. Radiat. Plasma Med. Sci. 2020, 5, 137–139. [Google Scholar] [CrossRef] [PubMed]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:14091556. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. (Eds.) Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016. [Google Scholar]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 



{kind=link}
{kind=link}
{kind=link}