
Deep Learning Model Based on 3D Optical Coherence Tomography Images for the Automated Detection of Pathologic Myopia


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
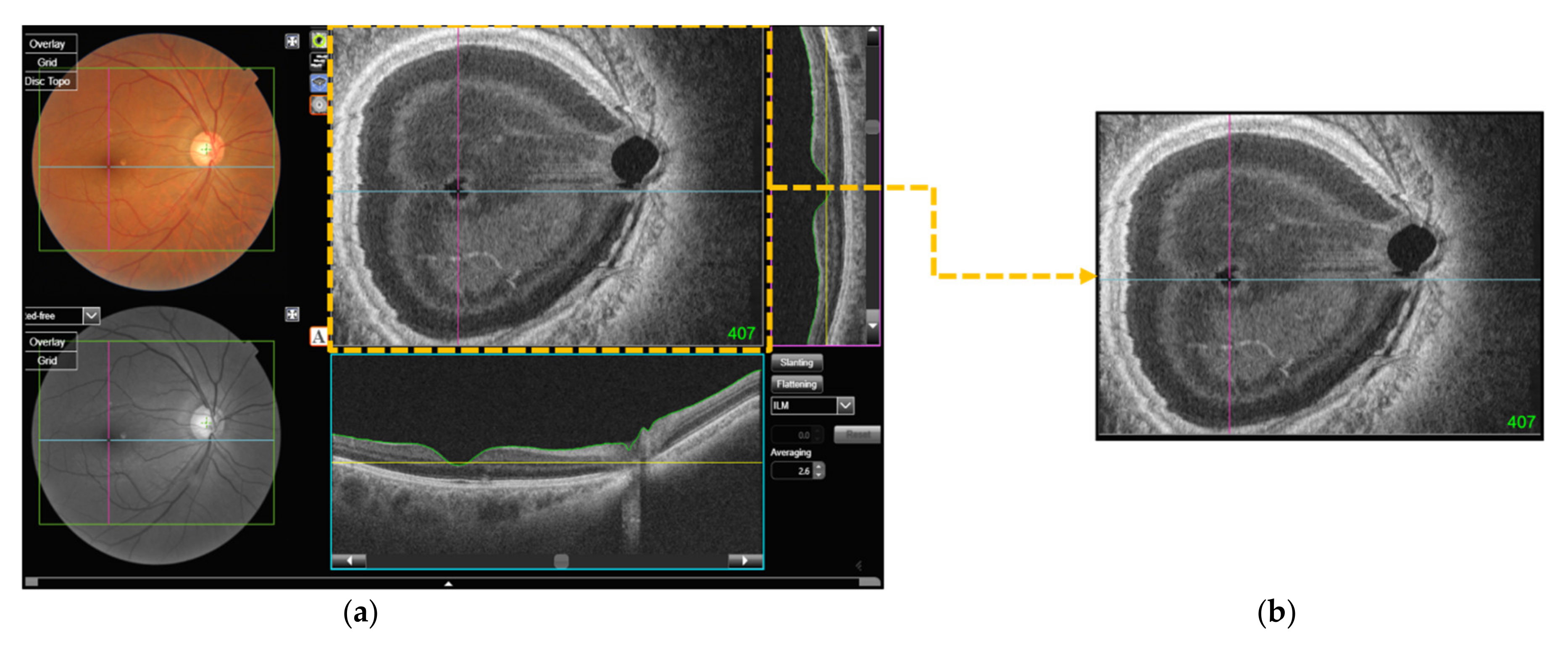
2.2. Data Acquisition
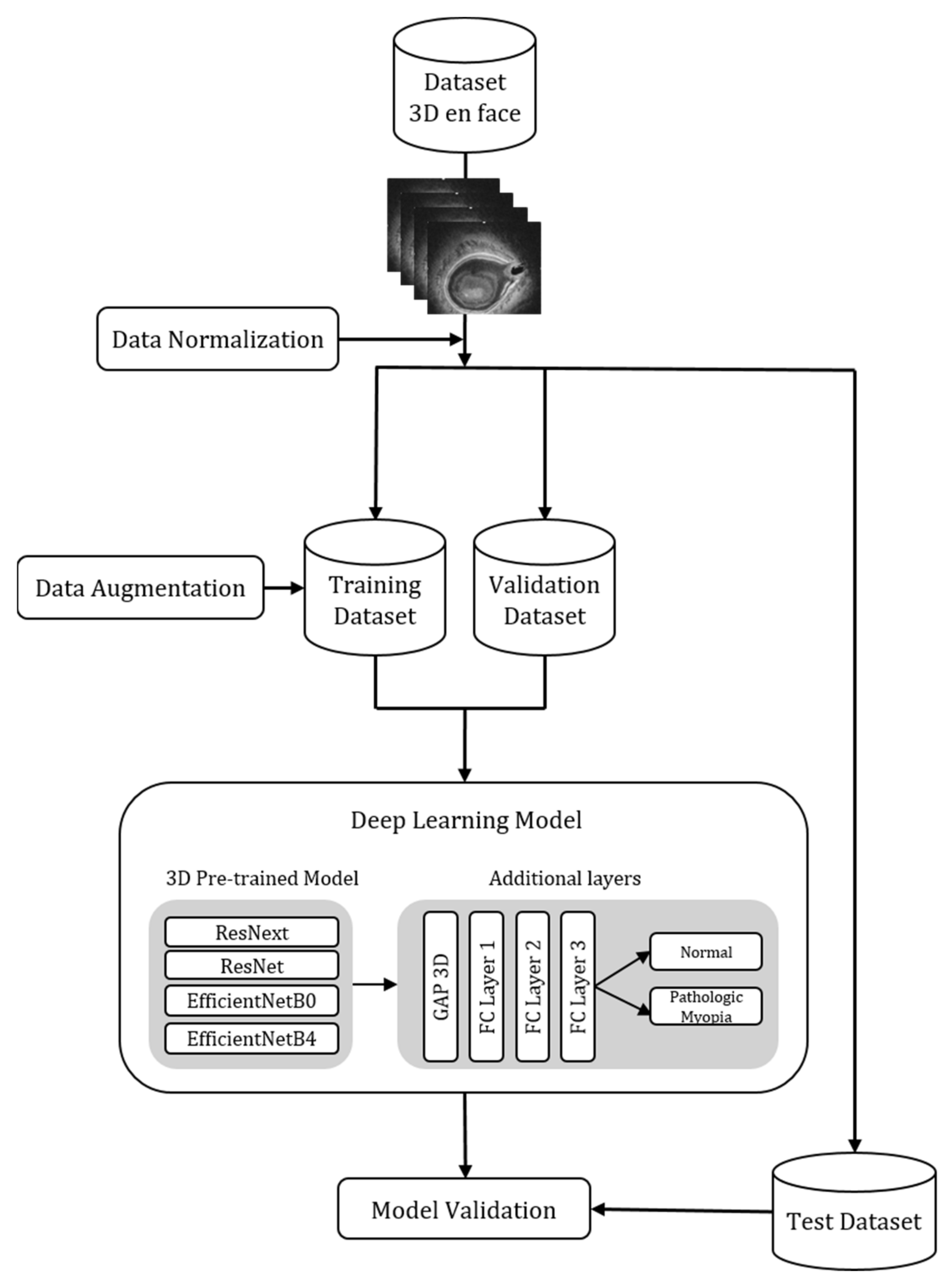
2.3. Model Architecture
2.4. Statistical Analysis
3. Results
3.1. Demographics
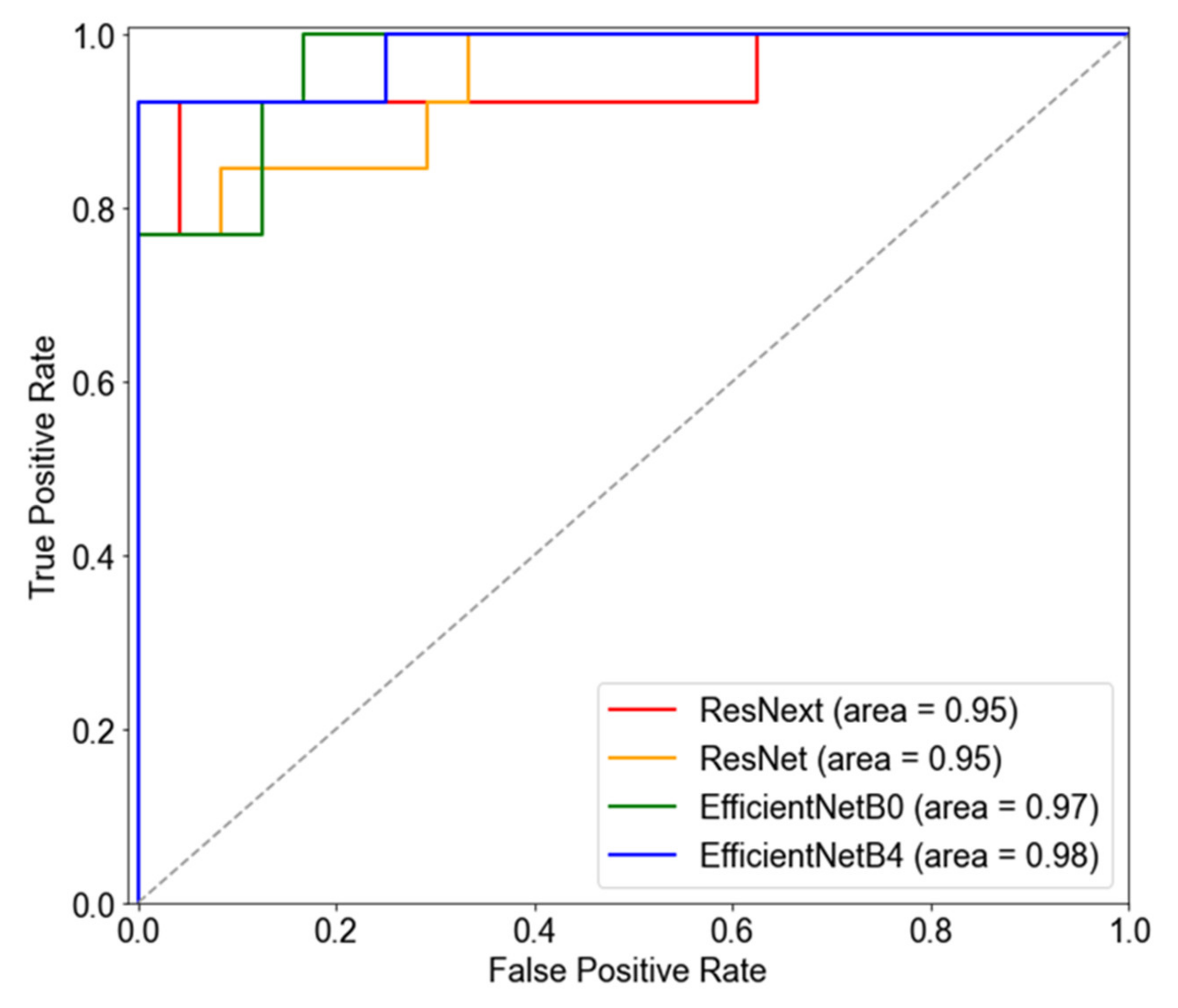
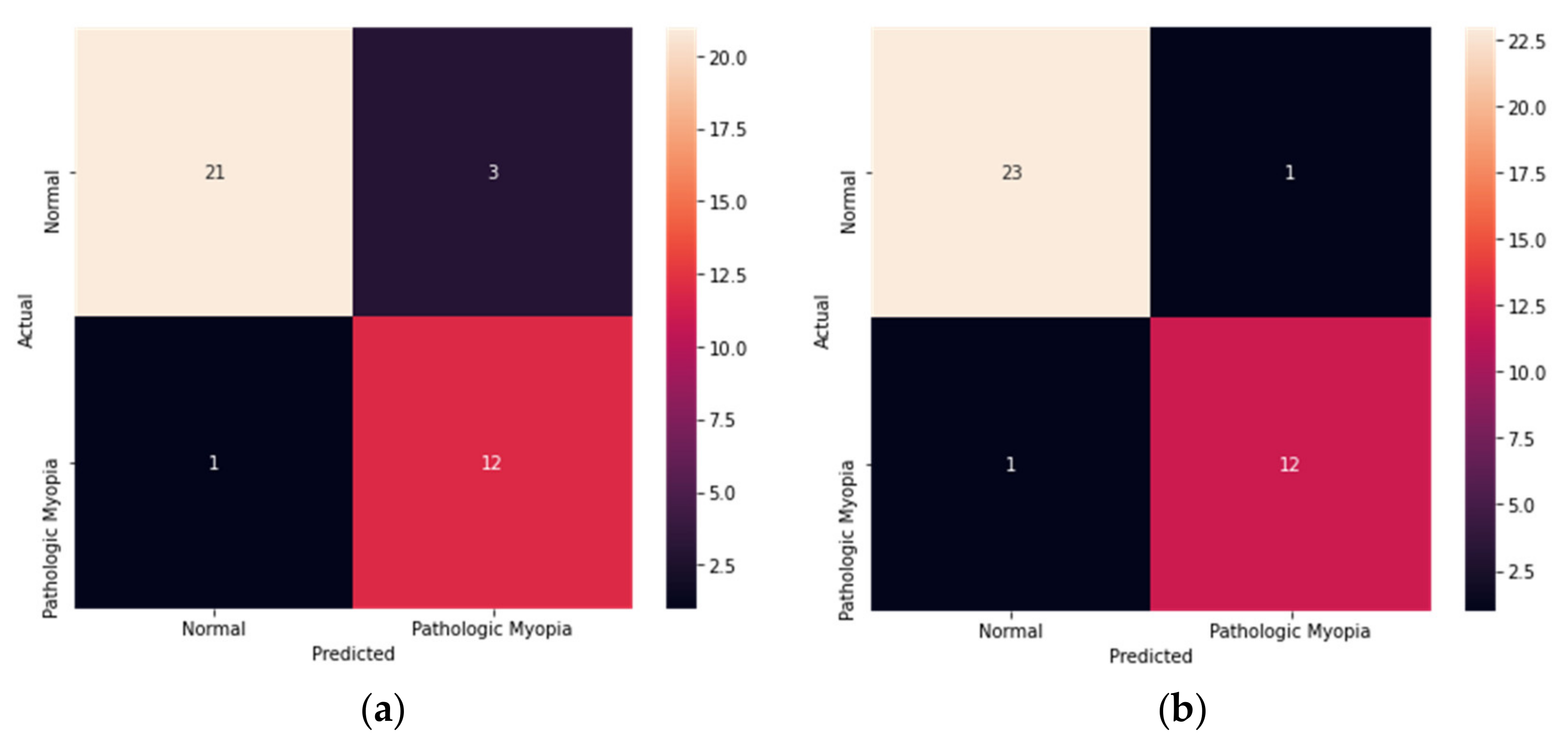
3.2. Model Performance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wong, T.Y.; Ferreira, A.; Hughes, R.; Carter, G.; Mitchell, P. Epidemiology and Disease Burden of Pathologic Myopia and Myopic Choroidal Neovascularization: An Evidence-Based Systematic Review. Am. J. Ophthalmol. 2013, 157, 9–25.e12. [Google Scholar] [CrossRef] [PubMed]
- Ohno-Matsui, K.; Wu, P.-C.; Yamashiro, K.; Vutipongsatorn, K.; Fang, Y.; Cheung, C.M.G.; Lai, T.Y.Y.; Ikuno, Y.; Cohen, S.Y.; Gaudric, A.; et al. IMI Pathologic Myopia. Investig. Opthalmol. Vis. Sci. 2021, 62, 5. [Google Scholar] [CrossRef] [PubMed]
- Hemelings, R.; Elen, B.; Blaschko, M.B.; Jacob, J.; Stalmans, I.; De Boever, P. Pathological myopia classification with simultaneous lesion segmentation using deep learning. Comput. Methods Programs Biomed. 2020, 199, 105920. [Google Scholar] [CrossRef] [PubMed]
- Varma, R.; Kim, J.S.; Burkemper, B.S.; Wen, G.; Torres, M.; Hsu, C.; Choudhury, F.; Azen, S.P.; McKean-Cowdin, R.; for the Chinese American Eye Study Group. Prevalence and Causes of Visual Impairment and Blindness in Chinese American Adults: The Chinese American eye study. JAMA Ophthalmol. 2016, 134, 785–793. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohno-Matsui, K. What is the fundamental nature of pathologic myopia? Retina 2017, 37, 1043–1048. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Medrano, J.; Montero, J.A.; Flores-Moreno, I.; Arias, L.; García-Layana, A.; Ruiz-Moreno, J.M. Myopic maculopathy: Current status and proposal for a new classification and grading system (ATN). Prog. Retin. Eye Res. 2018, 69, 80–115. [Google Scholar] [CrossRef]
- Wolffsohn, J.S.; Flitcroft, D.I.; Gifford, K.L.; Jong, M.; Jones, L.; Klaver, C.C.W.; Logan, N.S.; Naidoo, K.; Resnikoff, S.; Sankaridurg, P.; et al. IMI—Myopia Control Reports Overview and Introduction. Investig. Opthalmol. Vis. Sci. 2019, 60, M1–M19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moriyama, M.; Ohno-Matsui, K.; Hayashi, K.; Shimada, N.; Yoshida, T.; Tokoro, T.; Morita, I. Topographic Analyses of Shape of Eyes with Pathologic Myopia by High-Resolution Three-Dimensional Magnetic Resonance Imaging. Ophthalmology 2011, 118, 1626–1637. [Google Scholar] [CrossRef] [PubMed]
- Wang, N.-K.; Wu, Y.-M.; Wang, J.-P.; Liu, L.; Yeung, L.; Chen, Y.-P.; Chen, Y.-H.; Yeh, L.-K.; Wu, W.-C.; Chuang, L.-H.; et al. Clinical Characteristics of Posterior Staphylomas in Myopic Eyes with Axial Length Shorter Than 26.5 Millimeters. Am. J. Ophthalmol. 2015, 162, 180–190.e1. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.J.; Choi, J.E.; Roh, H.C.; Eun, J.S.; Kim, J.M.; Shin, Y.K.; Kang, M.C.; Chung, J.K.; Lee, C.; Lee, D.; et al. Deep learning models for screening of high myopia using optical coherence tomography. Sci. Rep. 2021, 11, 21663. [Google Scholar] [CrossRef]
- Kim, Y.C.; Chang, D.J.; Park, S.J.; Choi, I.Y.; Gong, Y.S.; Kim, H.-A.; Bin Hwang, H.; Jung, K.I.; Park, H.-Y.L.; Park, C.K.; et al. Machine learning prediction of pathologic myopia using tomographic elevation of the posterior sclera. Sci. Rep. 2021, 11, 6950. [Google Scholar] [CrossRef] [PubMed]
- Du, R.; Xie, S.; Fang, Y.; Igarashi-Yokoi, T.; Moriyama, M.; Ogata, S.; Tsunoda, T.; Kamatani, T.; Yamamoto, S.; Cheng, C.-Y.; et al. Deep Learning Approach for Automated Detection of Myopic Maculopathy and Pathologic Myopia in Fundus Images. Ophthalmol. Retin. 2021, 5, 1235–1244. [Google Scholar] [CrossRef]
- Kang, E.Y.-C.; Hsieh, Y.-T.; Li, C.-H.; Huang, Y.-J.; Kuo, C.-F.; Kang, J.-H.; Chen, K.-J.; Lai, C.-C.; Wu, W.-C.; Hwang, Y.-S. Deep Learning—Based Detection of Early Renal Function Impairment Using Retinal Fundus Images: Model Development and Validation. JMIR Med. Inform. 2020, 8, e23472. [Google Scholar] [CrossRef] [PubMed]
- Ran, A.R.; Cheung, C.Y.; Wang, X.; Chen, H.; Luo, L.-Y.; Chan, P.P.; Wong, M.O.M.; Chang, R.T.; Mannil, S.S.; Young, A.L.; et al. Detection of glaucomatous optic neuropathy with spectral-domain optical coherence tomography: A retrospective training and validation deep-learning analysis. Lancet Digit. Health 2019, 1, e172–e182. [Google Scholar] [CrossRef] [Green Version]
- Lin, A.C.; Lee, C.S.; Blazes, M.; Lee, A.Y.; Gorin, M.B. Assessing the Clinical Utility of Expanded Macular OCTs Using Machine Learning. Transl. Vis. Sci. Technol. 2021, 10, 32. [Google Scholar] [CrossRef] [PubMed]
- Yoo, T.K.; Choi, J.Y.; Kim, H.K. Feasibility study to improve deep learning in OCT diagnosis of rare retinal diseases with few-shot classification. Med. Biol. Eng. Comput. 2021, 59, 401–415. [Google Scholar] [CrossRef] [PubMed]
- De Fauw, J.; Ledsam, J.R.; Romera-Paredes, B.; Nikolov, S.; Tomasev, N.; Blackwell, S.; Askham, H.; Glorot, X.; O’Donoghue, B.; Visentin, D.; et al. Clinically applicable deep learning for diagnosis and referral in retinal disease. Nat. Med. 2018, 24, 1342–1350. [Google Scholar] [CrossRef] [PubMed]
- Maetschke, S.; Antony, B.; Ishikawa, H.; Wollstein, G.; Schuman, J.; Garnavi, R. A feature agnostic approach for glaucoma detection in OCT volumes. PLoS ONE 2019, 14, e0219126. [Google Scholar] [CrossRef] [PubMed]
- Faghihi, H.; Hajizadeh, F.; Riazi-Esfahani, M. Optical Coherence Tomographic Findings in Highly Myopic Eyes. J. Ophthalmic Vis. Res. 2010, 5, 110–121. [Google Scholar] [PubMed]
- Flitcroft, D.I.; He, M.; Jonas, J.B.; Jong, M.; Naidoo, K.; Ohno-Matsui, K.; Rahi, J.; Resnikoff, S.; Vitale, S.; Yannuzzi, L. IMI—Defining and Classifying Myopia: A Proposed Set of Standards for Clinical and Epidemiologic Studies. Investig. Opthalmol. Vis. Sci. 2019, 60, M20–M30. [Google Scholar] [CrossRef] [Green Version]
- Ohno-Matsui, K.; Kawasaki, R.; Jonas, J.B.; Cheung, C.M.G.; Saw, S.-M.; Verhoeven, V.; Klaver, C.; Moriyama, M.; Shinohara, K.; Kawasaki, Y.; et al. International Photographic Classification and Grading System for Myopic Maculopathy. Am. J. Ophthalmol. 2015, 159, 877–883.e7. [Google Scholar] [CrossRef] [PubMed]
- Fang, Y.; Du, R.; Nagaoka, N.; Yokoi, T.; Shinohara, K.; Xu, X.; Takahashi, H.; Onishi, Y.; Yoshida, T.; Ohno-Matsui, K. OCT-Based Diagnostic Criteria for Different Stages of Myopic Maculopathy. Ophthalmology 2019, 126, 1018–1032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohno-Matsui, K.; Jonas, J.B. Posterior staphyloma in pathologic myopia. Prog. Retin. Eye Res. 2018, 70, 99–109. [Google Scholar] [CrossRef]
- Choi, S.S.; Elsner, A.E.; Zawadzki, R.J.; Vohnsen, B. Clinical Applications of High Resolution In-Vivo Retinal Imaging. J. Ophthalmol. 2013, 2013, 312974. [Google Scholar] [CrossRef] [Green Version]
- Yao, P.; Shen, S.; Xu, M.; Liu, P.; Zhang, F.; Xing, J.; Shao, P.; Kaffenberger, B.; Xu, R.X. Single Model Deep Learning on Imbalanced Small Datasets for Skin Lesion Classification. IEEE Trans. Med. Imaging 2021, online ahead of print. [Google Scholar] [CrossRef]
- Cubuk, E.D.; Zoph, B.; Shlens, J.; Le, Q.V. Randaugment: Practical automated data augmentation with a reduced search space. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition Workshops, Seattle, WA, USA, 14–19 June 2020; pp. 702–703. [Google Scholar] [CrossRef]
- Huang, M.-L.; Lin, T.-Y. Considering breast density for the classification of benign and malignant mammograms. Biomed. Signal Process. Control 2021, 67, 102564. [Google Scholar] [CrossRef]
- Tan, C.; Sun, F.; Kong, T.; Zhang, W.; Yang, C.; Liu, C. A survey on deep transfer learning. In Proceedings of the International Conference on Artificial Neural Networks, Rhodes, Greece, 4–7 October 2018; Springer: Berlin/Heidelberg, Germany, 2018; pp. 270–279. [Google Scholar] [CrossRef] [Green Version]
- Ko, H.; Chung, H.; Kang, W.S.; Kim, K.W.; Shin, Y.; Kang, S.J.; Lee, J.H.; Kim, Y.J.; Kim, N.Y.; Jung, H.; et al. COVID-19 Pneumonia Diagnosis Using a Simple 2D Deep Learning Framework with a Single Chest CT Image: Model Development and Validation. J. Med. Internet Res. 2020, 22, e19569. [Google Scholar] [CrossRef]
- Tran, D.; Bourdev, L.; Fergus, R.; Torresani, L.; Paluri, M. Learning spatiotemporal features with 3d convolutional networks. In Proceedings of the IEEE International Conference on Computer Vision, Santiago, Chile, 7–13 December 2015; pp. 4489–4497. [Google Scholar] [CrossRef] [Green Version]
- Hara, K.; Kataoka, H.; Satoh, Y. Learning spatio-temporal features with 3d residual networks for action recognition. In Proceedings of the IEEE International Conference on Computer Vision Workshops, Venice, Italy, 22–29 October 2017; pp. 3154–3160. [Google Scholar] [CrossRef] [Green Version]
- Xie, S.; Girshick, R.; Dollár, P.; Tu, Z.; He, K. Aggregated residual transformations for deep neural networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 1492–1500. [Google Scholar]
- Tan, M.; Le, Q. Efficientnet: Rethinking model scaling for convolutional neural networks. Int. Conf. Mach. Learn. 2019, 2019, 6105–6114. [Google Scholar]
- Clevert, D.-A.; Unterthiner, T.; Hochreiter, S. Fast and accurate deep network learning by exponential linear units (elus). arXiv 2015, arXiv:151107289. [Google Scholar]
- Kingma, D.P.; Ba, J. Adam: A method for stochastic optimization. arXiv 2014, arXiv:14126980. [Google Scholar]
- Selvaraju, R.R.; Cogswell, M.; Das, A.; Vedantam, R.; Parikh, D.; Batra, D. Grad-cam: Visual explanations from deep networks via gradient-based localization. In Proceedings of the IEEE International Conference on Computer Vision, Venice, Italy, 22–29 October 2017; pp. 618–626. [Google Scholar]
- TensorFlow. Available online: https://www.tensorflow.org/ (accessed on 26 January 2022).
- Paszke, A.; Gross, S.; Massa, F.; Lerer, A.; Bradbury, J.; Chanan, G.; Killeen, T.; Lin, Z.; Gimelshein, N.; Antiga, L.; et al. Pytorch: An imperative style, high-performance deep learning library. Adv. Neural. Inf. Process. Syst. 2019, 32, 8026–8037. [Google Scholar]
- Pérez-García, F.; Sparks, R.; Ourselin, S. TorchIO: A Python library for efficient loading, preprocessing, augmentation and patch-based sampling of medical images in deep learning. Comput. Methods Programs Biomed. 2021, 208, 106236. [Google Scholar] [CrossRef] [PubMed]
- Bradski, G.; Kaehler, A. Learning OpenCV: Computer Vision with the OpenCV Library; O’Reilly Media Inc.: Sebastopol, CA, USA, 2008. [Google Scholar]
- Marques, G.; Agarwal, D.; Díez, I.D.L.T. Automated medical diagnosis of COVID-19 through EfficientNet convolutional neural network. Appl. Soft Comput. 2020, 96, 106691. [Google Scholar] [CrossRef] [PubMed]
- Ng, D.S.C.; Cheung, C.; Luk, F.O.; Mohamed, S.; Brelen, M.E.; Yam, J.C.; Tsang, C.W.; Lai, T. Advances of optical coherence tomography in myopia and pathologic myopia. Eye 2016, 30, 901–916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoo, T.K.; Ryu, I.H.; Kim, J.K.; Lee, I.S. Deep learning for predicting uncorrected refractive error using posterior segment optical coherence tomography images. Eye 2021, 201, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.C.; Koo, Y.H.; Jung, K.I.; Park, C.K. Impact of Posterior Sclera on Glaucoma Progression in Treated Myopic Normal-Tension Glaucoma Using Reconstructed Optical Coherence Tomographic Images. Investig. Opthalmol. Vis. Sci. 2019, 60, 2198–2207. [Google Scholar] [CrossRef] [PubMed]
- Forte, R.; Cennamo, G.; Pascotto, F.; de Crecchio, G. En Face Optical Coherence Tomography of the Posterior Pole in High Myopia. Am. J. Ophthalmol. 2008, 145, 281–288.e1. [Google Scholar] [CrossRef] [PubMed]
- Kang, E.Y.-C.; Yeung, L.; Lee, Y.-L.; Wu, C.-H.; Peng, S.-Y.; Chen, Y.-P.; Gao, Q.-Z.; Lin, C.; Kuo, C.-F.; Lai, C.-C. A Multimodal Imaging–Based Deep Learning Model for Detecting Treatment-Requiring Retinal Vascular Diseases: Model Development and Validation Study. JMIR Med. Inform. 2021, 9, e28868. [Google Scholar] [CrossRef] [PubMed]
- Wong, Y.L.; Man, R.E.K.; Fenwick, E.; Saw, S.M.; Wong, C.W.; Cheung, C.M.G.; Lamoureux, E.L. Public Health Impact of Pathologic Myopia. In Pathologic Myopia; Springer: Berlin/Heidelberg, Germany, 2021; pp. 59–65. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Normal (n = 238) | Pathologic Myopia (n = 129) | p Value | |
|---|---|---|---|---|
| Sex | <0.001 | |||
| Male | 153 (64.3%) | 57 (44.2%) | ||
| Female | 85 (35.7%) | 72 (55.8%) | ||
| Age | 51.3 ± 13.3 | 55.7 ± 15.4 | 0.006 | |
| Axial Length | 25.6 ± 0.7 | 27.7 ± 2.2 | <0.001 | |
| Choroidal Thickness | 259.1 ± 98.3 | 169.2 ± 98.9 | <0.001 | |
| Total (n = 367) | Training Set (n = 293) | Validation Set (n = 37) | Test Set (n = 37) | |
|---|---|---|---|---|
| Normal | 238 (64.9) | 190 (64.8) | 24 (64.9) | 24 (64.9) |
| Pathologic Myopia | 129 (35.1) | 103 (35.2) | 13 (35.1) | 13 (35.1) |
| Model | Accuracy | Sensitivity | Specificity | AUROC |
|---|---|---|---|---|
| ResNext50 | 0.89 | 0.92 | 0.88 | 0.95 |
| ResNet18 | 0.86 | 0.85 | 0.88 | 0.95 |
| EfficientNetB0 | 0.89 | 0.92 | 0.88 | 0.97 |
| EfficientNetB4 | 0.95 | 0.93 | 0.96 | 0.98 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.-J.; Ko, T.; Park, C.-K.; Kim, Y.-C.; Choi, I.-Y. Deep Learning Model Based on 3D Optical Coherence Tomography Images for the Automated Detection of Pathologic Myopia. Diagnostics 2022, 12, 742. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12030742
Park S-J, Ko T, Park C-K, Kim Y-C, Choi I-Y. Deep Learning Model Based on 3D Optical Coherence Tomography Images for the Automated Detection of Pathologic Myopia. Diagnostics. 2022; 12(3):742. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12030742
Chicago/Turabian StylePark, So-Jin, Taehoon Ko, Chan-Kee Park, Yong-Chan Kim, and In-Young Choi. 2022. "Deep Learning Model Based on 3D Optical Coherence Tomography Images for the Automated Detection of Pathologic Myopia" Diagnostics 12, no. 3: 742. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12030742