
Utility of Red Cell Distribution Width (RDW) as a Noninvasive Biomarker for the Diagnosis of Acute Appendicitis: A Systematic Review and Meta-Analysis of 5222 Cases

 ,
,  ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
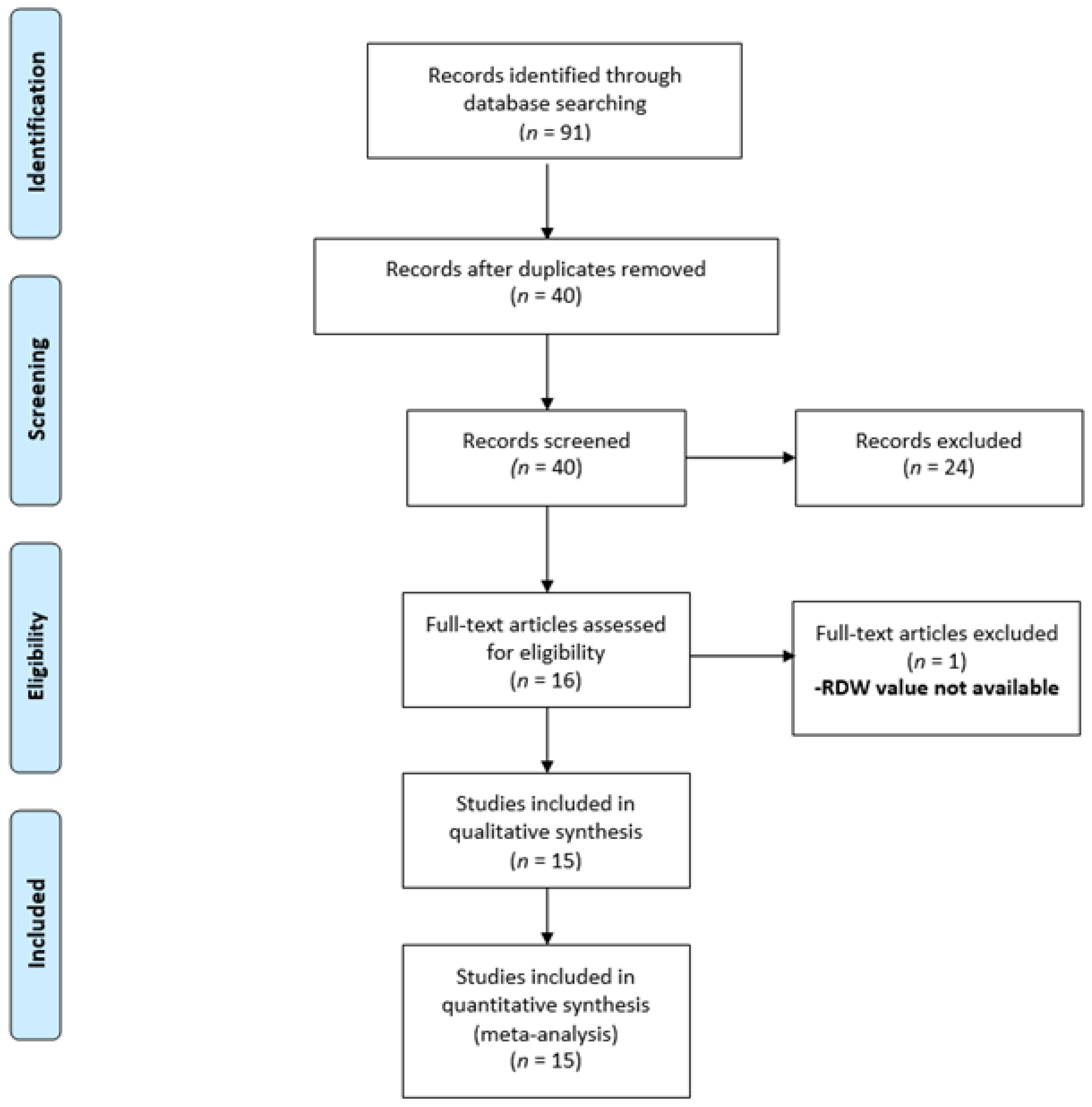
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Data Extraction
2.4. Methodological Quality Assessment
2.5. Statistical Analysis
3. Results
3.1. Study Characteristics
3.2. Methodological Quality Assessment
3.3. Outcome Analysis
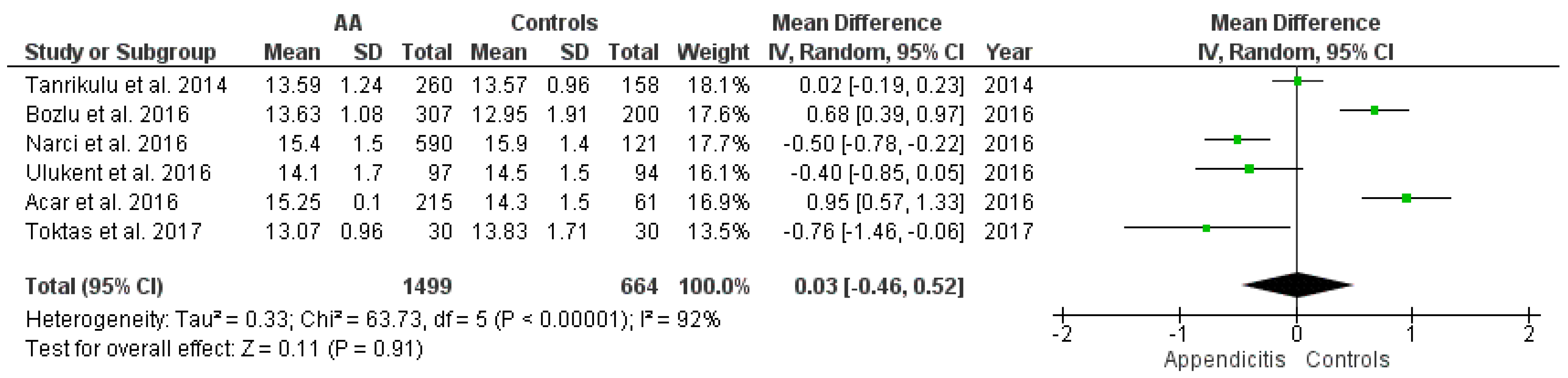
3.3.1. RDW Values among the AA Group vs. Healthy Controls
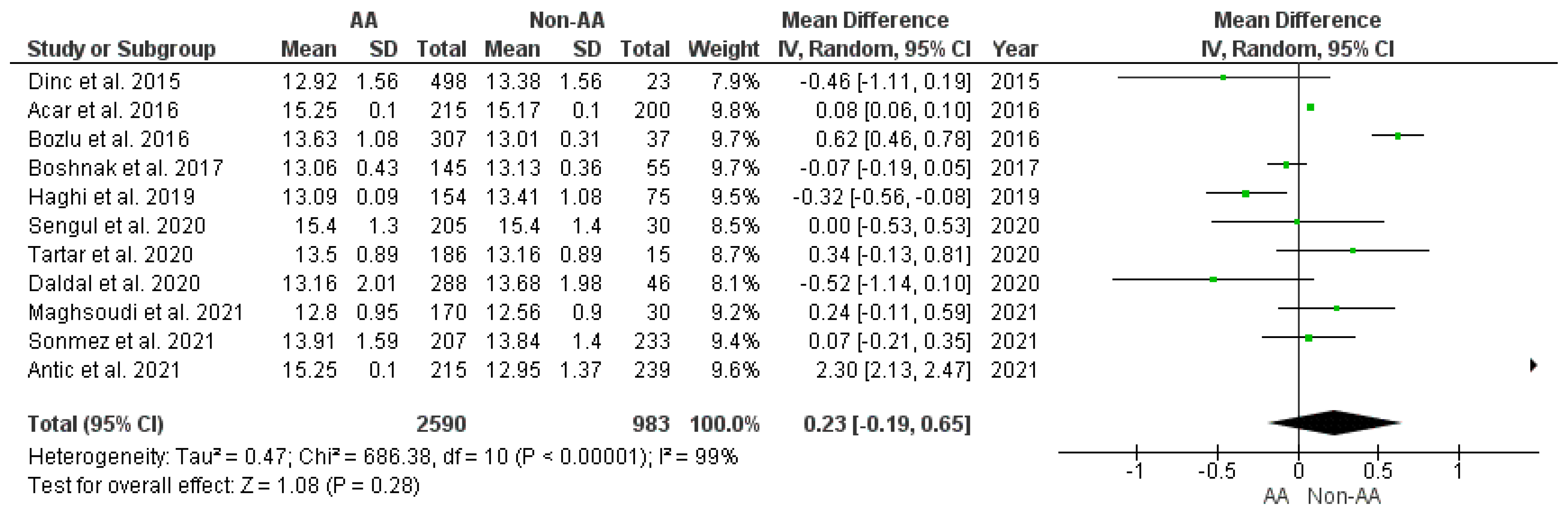
3.3.2. RDW Values among the AA vs. Non-AA Group
3.3.3. RDW Values among the AA vs. Non-AA Group in Pediatric Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database | Studies |
|---|---|
| PubMed | 27 |
| EMBASE | 19 |
| Web of Science | 18 |
| Scopus | 27 |
| Total | 91 |
| Duplications | 51 |
| After duplications removed | 40 |
References
- Andersson, R.E. Meta-analysis of the clinical and laboratory diagnosis of appendicitis. Br. J. Surg. 2004, 91, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Lounis, Y.; Hugo, J.; Demarche, M.; Seghaye, M.C. Influence of age on clinical presentation, diagnosis delay and outcome in pre-school children with acute appendicitis. BMC Pediatrics 2020, 20, 151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boshnak, N.; Boshnaq, M.; Elgohary, H. Evaluation of Platelet Indices and Red Cell Distribution Width as New Biomarkers for the Diagnosis of Acute Appendicitis. J. Investig. Surg. 2018, 31, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Maita, S.; Andersson, B.; Svensson, J.F.; Wester, T. Nonoperative treatment for nonperforated appendicitis in children: A systematic review and meta-analysis. Pediatric Surg. Int. 2020, 36, 261–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pogorelić, Z.; Anand, S.; Žuvela, T.; Singh, A.; Križanac, Z.; Krishnan, N. Incidence of complicated appendicitis during the COVID-19 Pandemic versus the pre-pandemic period: A systematic review and meta-analysis of 2782 pediatric appendectomies. Diagnostics 2022, 12, 127. [Google Scholar] [CrossRef] [PubMed]
- Podda, M.; Gerardi, C.; Cillara, N.; Fearnhead, N.; Gomes, C.A.; Birindelli, A.; Mulliri, A.; Davies, R.J.; Di Saverio, S. Antibiotic treatment and appendectomy for uncomplicated acute appendicitis in adults and children: A systematic review and metaanalysis. Ann. Surg. 2019, 270, 1028–1040. [Google Scholar] [CrossRef]
- Yang, J.; Liu, C.; He, Y.; Cai, Z. Laboratory markers in the prediction of acute perforated appendicitis in children. Emerg. Med. Int. 2019, 2019, 4608053. [Google Scholar] [CrossRef]
- Kulik, D.M.; Uleryk, E.M.; Maguire, J.L. Does this child have appendicitis? A systematic review of clinical prediction rules for children with acute abdominal pain. J. Clin. Epidemiol. 2013, 66, 95–104. [Google Scholar] [CrossRef]
- Pogorelić, Z.; Rak, S.; Mrklić, I.; Jurić, I. Prospective validation of Alvarado score and Pediatric Appendicitis Score for the diagnosis of acute appendicitis in children. Pediatric Emerg. Care 2015, 31, 164–168. [Google Scholar] [CrossRef]
- Russell, W.S.; Schuh, A.M.; Hill, J.G.; Hebra, A.; Cina, R.A.; Smith, C.D.; Streck, C.J. Clinical practice guidelines for pediatric appendicitis evaluation can decrease computed tomography utilization while maintaining diagnostic accuracy. Pediatric Emerg. Care 2013, 29, 568–573. [Google Scholar] [CrossRef] [Green Version]
- Hwang, M.E. Sonography and computed tomography in diagnosing acute appendicitis. Radiol. Technol. 2018, 89, 224–237. [Google Scholar] [PubMed]
- Estey, A.; Poonai, N.; Lim, R. Appendix not seen: The predictive value of secondary inflammatory sonographic signs. Pediatric Emerg. Care 2013, 29, 435–439. [Google Scholar] [CrossRef] [PubMed]
- Chong, C.F.; Thien, A.; Mackie, A.J.; Tin, A.S.; Tripathi, S.; Ahmad, M.A.; Tan, L.T.; Ang, S.H.; Telisinghe, P.U. Comparison of RIPASA and Alvarado scores for the diagnosis of acute appendicitis. Singap. Med. J. 2011, 52, 340–345. [Google Scholar]
- Alvarado, A. A practical score for the early diagnosis of acute appendicitis. Ann. Emerg. Med. 1986, 15, 557–564. [Google Scholar] [CrossRef]
- Andersson, M.; Kolodziej, B.; Andersson, R.E. Validation of the Appendicitis Inflammatory Response (AIR) Score. World J. Surg. 2021, 45, 2081–2091. [Google Scholar] [CrossRef]
- Pogorelić, Z.; Mihanović, J.; Ninčević, S.; Lukšić, B.; Elezović Baloević, S.; Polašek, O. Validity of appendicitis inflammatory response score in distinguishing perforated from non-perforated appendicitis in children. Children 2021, 8, 309. [Google Scholar] [CrossRef]
- Andersson, M.; Ruber, M.; Ekerfelt, C.; Hallgren, H.B.; Olaison, G.; Andersson, R.E. Can new inflammatory markers improve the diagnosis of acute appendicitis? World J. Surg. 2014, 38, 2777–2783. [Google Scholar] [CrossRef]
- Destek, S.; Gül, V.O.; Mente¸s, M.Ö.; Çiçek, A.F. Diagnostic efficacy of serum procalcitonin, IL-6, IL-2, and D-dimer levels in an experimental acute appendicitis model. Turk. J. Gastroenterol. 2019, 30, 641–647. [Google Scholar] [CrossRef]
- Rivera-Chavez, F.A.; Wheeler, H.; Lindberg, G.; Munford, R.S.; O’Keefe, G.E. Regional and systemic cytokine responses to acute inflammation of the vermiform appendix. Ann. Surg. 2003, 237, 408–416. [Google Scholar] [CrossRef]
- Pogorelić, Z.; Lukšić, B.; Ninčević, S.; Lukšić, B.; Polašek, O. Hyponatremia as a predictor of perforated acute appendicitis in pediatric population: A prospective study. J. Pediatric Surg. 2021, 56, 1816–1821. [Google Scholar] [CrossRef]
- Shogilev, D.J.; Duus, N.; Odom, S.R.; Shapiro, N.I. Diagnosing appendicitis: Evidence-based review of the diagnostic approach in 2014. West. J. Emerg. Med. 2014, 15, 859–871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pogorelić, Z.; Lukšić, A.M.; Mihanović, J.; Đikić, D.; Balta, V. Hyperbilirubinemia as an indicator of perforated acute appendicitis in pediatric population: A prospective study. Surg. Infect. 2021, 22, 1064–1071. [Google Scholar] [CrossRef] [PubMed]
- Chiang, J.J.Y.; Angus, M.I.; Nah, S.A.; Jacobsen, A.S.; Low, Y.; Choo, C.S.C.; Yap, T.L.; Chen, Y. Time course response of inflammatory markers in pediatric appendicitis. Pediatric Surg. Int. 2020, 36, 493–500. [Google Scholar] [CrossRef] [PubMed]
- Pogorelić, Z.; Domjanović, J.; Jukić, M.; Poklepović Perišić, T. Acute appendicitis in children younger than five years of age: Diagnostic challenge for pediatric surgeons. Surg. Infect. 2020, 21, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Maloney, C.; Edelman, M.C.; Bolognese, A.C.; Lipskar, A.M.; Rich, B.S. The Impact of pathological criteria on pediatric negative appendectomy rate. J. Pediatric Surg. 2019, 54, 1794–1799. [Google Scholar] [CrossRef]
- Aktimur, R.; Cetinkunar, S.; Yildirim KOzdas, S.; Aktimur, S.H.; Gokakin, A.K. Mean platelet volume is a significant biomarker in the differential diagnosis of acute appendicitis. Inflamm. Cell Signal. 2015, 2, e930. [Google Scholar]
- Pogorelić, Z.; Silov, N.; Jukić, M.; Elezović Baloević, S.; Poklepović Peričić, T.; Jerončić, A. Ertapenem monotherapy versus gentamicin plus metronidazole for perforated appendicitis in pediatric patients. Surg. Infect. 2019, 20, 625–630. [Google Scholar] [CrossRef]
- Galai, T.; Beloosesky, O.Z.; Scolnik, D.; Rimon, A.; Glatstein, M. Misdiagnosis of acute appendicitis in children attending the Emergency Department: The experience of a large, tertiary care pediatric hospital. Eur. J. Pediatric Surg. 2017, 27, 138–141. [Google Scholar] [CrossRef]
- Lippi, G.; Plebani, M. Red blood cell distribution width (RDW) and human pathology. One size fits all. Clin. Chem. Lab. Med. 2014, 52, 1247–1249. [Google Scholar] [CrossRef]
- Rastgoo Haghi, A.; Pourmohammad, P.; Seyf Rabiee, M.A. Accuracy of mean platelet volume (MPV) and red cell distribution width (RDW) for the diagnosis of acute appendicitis: Evaluation of possible new biomarkers. Adv. J. Emerg. Med. 2020, 4, e20. [Google Scholar]
- Narci, H.; Turk, E.; Karagulle, E.; Togan, T.; Karabulut, K. The role of red cell distribution width in the diagnosis of acute appendicitis: A retrospective case-controlled study. World J. Emerg. Surg. 2013, 8, 46–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bozlu, G.; Taskinlar, H.; Unal, S.; Alakaya, M.; Nayci, A.; Kuyucu, N. Diagnostic value of red blood cell distribution width in children with acute appendicitis. Pediatrics Int. 2016, 58, 202–205. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Cochrane Handbook for Systematic Reviews of Interventions (Version 6.2) [Internet]. Cochrane. 2021. Available online: www.training.cochrane.org/handbook (accessed on 1 April 2022).
- Tartar, T.; Bakal, Ü.; Saraç, M.; Aydin, S.; Kazez, A. Diagnostic value of laboratory results in children with acute appendicitis. Turk. J. Biochem. 2020, 45, 553–558. [Google Scholar] [CrossRef]
- Dinc, T.; Senol, K.; Yildiz, B.; Kayilioglu, I.; Sozen, I.; Coskun, F. Association between red cell distribution width and mean platelet volume with appendicitis: A myth or a fact? Bratisl. Lek. Listy 2015, 116, 499–501. [Google Scholar] [CrossRef] [Green Version]
- Sengul, S.; Guler, Y.; Calis, H.; Karabulut, Z. The Role of Serum Laboratory Biomarkers for Complicated and Uncomplicated Appendicitis in Adolescents. J Coll. Physicians Surg. Pak. 2020, 30, 420–424. [Google Scholar]
- Antić, J.; Jokić, R.; Bukarica, S.; Lukić, I.; Dobrijević, D.; Rakić, G.; Pajić, M.; Trajković, V.; Milenković, M. Predictive Value of Red Blood Cell Distribution Width, Mean Platelet Volume and Platelet Distribution Width in Children with Acute Appendicitis. Children 2021, 8, 1041. [Google Scholar] [CrossRef]
- Toktas, O.; Aslan, M. Mean platelet volume, red cell distribution width, neutrophil to lymphocyte ratio and platelet to lymphocyte ratio in the diagnosis of acute appendicitis. East. J. Med. 2017, 22, 5–9. [Google Scholar] [CrossRef]
- Daldal, E.; Dagmura, H. The Correlation between Complete Blood Count Parameters and Appendix Diameter for the Diagnosis of Acute Appendicitis. Healthcare 2020, 8, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maghsoudi, L.H.; Kabir, K.; Soltanian, A.; Pak, H.; Ahmadinejad, M.; Ahmadi, A.K. A cross-sectional study on evaluation of complete blood count-associated parameters for the diagnosis of acute appendicitis. Health Sci. Rep. 2021, 4, e326. [Google Scholar] [CrossRef] [PubMed]
- Ulukent, S.C.; Sarici, I.S.; Ulutas, K.T. All CBC parameters in diagnosis of acute appendicitis. Int. J. Clin. Exp. Med. 2016, 9, 11871–11876. [Google Scholar]
- Tanrikulu, C.S.; Tanrikulu, Y.; Sabuncuoglu, M.Z.; Karamercan, M.A.; Akkapulu, N.; Coskun, F. Mean platelet volume and red cell distribution width as a diagnostic marker in acute appendicitis. Irani. Red Crescent Med. J. 2014, 16, e10211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Acar, E.; Özcan, Ö.; Deliktaş, H.; Beydilli, H.; Kırlı, İ.; Alataş, Ö.D.; Şahin, C.; Yıldırım, B.; Belli, A.K. Laboratory markers has many valuable parameters in the discrimination between acute appendicitis and renal colic. Ulus Travma Acil Cerrahi Derg. 2016, 22, 17–22. [Google Scholar] [CrossRef] [Green Version]
- Sönmez, A.; Avcı, A.; Sönmez, G.; Gülen, M.; Acehan, S.; Avcı, B.Ş.; Kuvvetli, A.; Satar, S. The efficacy of hemogram parameters in the differential diagnosis of renal colic and acute appendicitis in the emergency department. Ulus Travma Acil Cerrahi Derg. 2021, 27, 26–33. [Google Scholar]
- Ferris, M.; Quan, S.; Kaplan, B.S.; Molodecky, N.; Ball, C.G.; Chernoff, G.W.; Bhala, N.; Ghosh, S.; Dixon, E.; Ng, S.; et al. The global incidence of appendicitis: A systematic review of population-based studies. Ann. Surg. 2017, 266, 237–241. [Google Scholar] [CrossRef] [Green Version]
- Almström, M.; Svensson, J.F.; Svenningsson, A.; Hagel, E.; Wester, T. Population-based cohort study on the epidemiology of acute appendicitis in children in Sweden in 1987–2013. BJS Open 2018, 2, 142–150. [Google Scholar] [CrossRef]
- Lin, K.B.; Chan, C.L.; Yang, N.P.; Lai, R.K.; Liu, Y.H.; Zhu, S.Z.; Pan, R.H. Epidemiology of appendicitis and appendectomy for the low-income population in Taiwan, 2003–2011. BMC Gastroenterol. 2015, 15, 18. [Google Scholar] [CrossRef] [Green Version]
- Kwan, K.Y.; Nager, A.L. Diagnosing pediatric appendicitis: Usefulness of laboratory markers. Am. J. Emerg. Med. 2010, 28, 1009–1015. [Google Scholar] [CrossRef]
- Pogorelic, Z.; Buljubasic, M.; Susnjar, T.; Jukic, M.; Pericic, T.P.; Juric, I. Comparison of open and laparoscopic appendectomy in children: A 5-year single center experience. Indian Pediatrics 2019, 56, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Pogorelić, Z.; Beara, V.; Jukić, M.; Rashwan, H.; Šušnjar, T. A new approach to laparoscopic appendectomy in children-clipless/sutureless Harmonic scalpel laparoscopic appendectomy. Langenbecks Arch. Surg. 2022, 407, 779–787. [Google Scholar] [CrossRef] [PubMed]
- Mihanović, J.; Šikić, N.L.; Mrklić, I.; Katušić, Z.; Karlo, R.; Jukić, M.; Jerončić, A.; Pogorelić, Z. Comparison of new versus reused Harmonic scalpel performance in laparoscopic appendectomy in patients with acute appendicitis-a randomized clinical trial. Langenbecks Arch. Surg. 2021, 406, 153–162. [Google Scholar] [CrossRef] [PubMed]
- Perko, Z.; Bilan, K.; Pogorelić, Z.; Druzijanić, N.; Srsen, D.; Kraljević, D.; Juricić, J.; Krnić, D. Acute appendicitis and ileal perforation with a toothpick treated by laparoscopy. Coll. Antropol. 2008, 32, 307–309. [Google Scholar] [PubMed]
- Lou, Y.; Wang, M.; Mao, W. Clinical usefulness of measuring red blood cell distribution width in patients with Hepatitis B. PLoS ONE 2012, 7, e37644. [Google Scholar] [CrossRef] [Green Version]
- May, J.E.; Marques, M.B.; Reddy, V.V.B.; Gangaraju, R. Three neglected numbers in the CBC: The RDW, MPV, and NRBC count. Cleve Clin. J. Med. 2019, 86, 167–172. [Google Scholar] [CrossRef]
- Felker, G.M.; Allen, L.A.; Pocock, S.J.; Shaw, L.K.; McMurray, J.J.; Pfeffer, M.A.; Swedberg, K.; Wang DYusuf, S.; Michelson, E.L.; Granger, C.B.; et al. Red cell distribution width as a novel prognostic marker in heart failure: Data from the CHARM Program and the Duke Databank. J. Am. Coll. Cardiol. 2007, 50, 40–47. [Google Scholar] [CrossRef] [Green Version]
- Şenol, K.; Saylam, B.; Kocaay, F.; Tez, M. Red cell distribution width as a predictor of mortality in acute pancreatitis. Am. J. Emerg. Med. 2013, 31, 687–689. [Google Scholar] [CrossRef]
- Bilgiç, I.; Dolu, F.; Şenol, K.; Tez, M. Prognostic significance of red cell distribution width in acute mesenteric ischemia. Perfusion 2015, 30, 161–165. [Google Scholar] [CrossRef]
- Kim, J.; Kim, K.; Lee, J.H.; Jo, Y.H.; Rhee, J.E.; Kim, T.Y.; Kang, K.W.; Kim, Y.J.; Hwang, S.S.; Jang, H.Y. Red blood cell distribution width as an independent predictor of all-cause mortality in out of hospital cardiac arrest. Resuscitation 2012, 83, 1248–1252. [Google Scholar] [CrossRef]
- Spell, D.W.; Jones, D.V., Jr.; Harper, W.F.; David, B.J. The value of a complete blood count in predicting cancer of the colon. Cancer Detect. Prev. 2004, 28, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Al-Rawi, Z.S.; Gorial, F.I.; Al-Bayati, A.A. Red Cell Distribution Width in Rheumatoid arthritis. Mediterr. J. Rheumatol. 2018, 29, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, R.M.; Robinson, T.J. Monitoring dietary compliance in coeliac disease using red cell distribution width. Int. J. Clin. Pract. 2002, 56, 249–250. [Google Scholar]
- Akbulut, S.; Koç, C.; Şahin, T.T.; Şahin, E.; Tuncer, A.; Demyati, K.; Şamdancı, E.; Çolak, C.; Yılmaz, S. An investigation into the factors predicting acute appendicitis and perforated appendicitis. Ulus Travma Acil Cerrahi Derg. 2021, 27, 434–442. [Google Scholar] [PubMed]
- Stefanutti, G.; Ghirardo, V.; Gamba, P. Inflammatory markers for acute appendicitis in children: Are they helpful? J. Pediatr. Surg. 2007, 42, 773–776. [Google Scholar] [CrossRef] [PubMed]
- Rouzrokh, M.; Fard, F.E.; Momeni, N.; Tavassoli, A. Diagnostic role of ESR, CRP, leukocytosis and Neutrophil/Lymphocyte in peripheral blood smear in children under 14 with acute appendicitis. Pajoohandeh 2011, 16, 42–46. [Google Scholar]




| Author, Year | Study Design | Sample Size | ||
|---|---|---|---|---|
| AA | Non-AA | Controls | ||
| Tanrikulu et al., 2014 [45] | Retrospective | 260 | - | 158 |
| Dinc et al., 2015 [38] | Retrospective | 498 | 23 | - |
| Narci et al., 2016 [31] | Retrospective | 590 | - | 121 |
| Ulukent et al., 2016 [44] | Retrospective | 97 | - | 94 |
| Bozlu et al., 2016 [32] | Retrospective | 307 | 37 | 200 |
| Acar et al., 2016 [46] | Retrospective | 215 | 200 | 61 |
| Boshnak et al., 2017 [3] | Prospective | 145 | 55 | - |
| Toktas et al., 2017 [41] | Retrospective | 30 | - | 30 |
| Haghi et al., 2019 [30] | Retrospective | 154 | 75 | - |
| Tartar et al., 2020 [37] | Retrospective | 186 | 15 | - |
| Sengul et al., 2020 [39] | Retrospective | 205 | 30 | - |
| Daldal et al., 2020 [42] | Retrospective | 288 | 46 | - |
| Antić et al., 2021 [40] | Retrospective | 223 | 239 | - |
| Maghsoudi et al., 2021 [43] | Cross-sectional | 170 | 30 | - |
| Sönmez at al., 2021 [47] | Retrospective | 207 | 233 | - |
| Study | Reporting | External Validity | Internal Validity—Bias | Internal Validity—Confounding | Power | Total Scores |
|---|---|---|---|---|---|---|
| Methodological Assessment by Observer 1 | ||||||
| Tanrikulu et al., 2014 [45] | 10 | 3 | 5 | 3 | 5 | 26 |
| Dinc et al., 2015 [38] | 10 | 3 | 5 | 3 | 0 | 21 |
| Narci et al., 2016 [31] | 9 | 3 | 5 | 3 | 5 | 25 |
| Ulukent et al., 2016 [44] | 10 | 3 | 5 | 3 | 3 | 24 |
| Bozlu et al., 2016 [32] | 10 | 3 | 5 | 3 | 0 | 21 |
| Acar et al., 2016 [46] | 10 | 3 | 5 | 3 | 2 | 23 |
| Boshnak et al., 2017 [3] | 10 | 3 | 5 | 3 | 1 | 22 |
| Toktas et al., 2017 [41] | 10 | 3 | 5 | 3 | 0 | 21 |
| Haghi et al., 2019 [30] | 10 | 3 | 5 | 3 | 3 | 24 |
| Tartar et al., 2020 [37] | 10 | 3 | 5 | 3 | 0 | 21 |
| Sengul et al., 2020 [39] | 9 | 3 | 5 | 3 | 0 | 20 |
| Daldal et al., 2020 [42] | 10 | 3 | 5 | 4 | 0 | 22 |
| Antić et al., 2021 [40] | 10 | 3 | 5 | 3 | 5 | 26 |
| Maghsoudi et al., 2021 [43] | 10 | 3 | 5 | 3 | 0 | 21 |
| Sönmez at al., 2021 [47] | 10 | 3 | 5 | 3 | 5 | 26 |
| Methodological Assessment by Observer 2 | ||||||
| Tanrikulu et al., 2014 [45] | 10 | 3 | 5 | 3 | 5 | 26 |
| Dinc et al., 2015 [38] | 10 | 3 | 5 | 4 | 0 | 22 |
| Narci et al., 2016 [31] | 10 | 3 | 5 | 3 | 5 | 26 |
| Ulukent et al., 2016 [44] | 10 | 3 | 5 | 3 | 3 | 24 |
| Bozlu et al., 2016 [32] | 10 | 3 | 5 | 3 | 0 | 21 |
| Acar et al., 2016 [46] | 10 | 3 | 5 | 4 | 2 | 24 |
| Boshnak et al., 2017 [3] | 10 | 3 | 5 | 4 | 1 | 23 |
| Toktas et al., 2017 [41] | 10 | 3 | 5 | 3 | 0 | 21 |
| Haghi et al., 2019 [30] | 10 | 3 | 5 | 4 | 3 | 25 |
| Tartar et al., 2020 [37] | 10 | 3 | 5 | 4 | 0 | 22 |
| Sengul et al., 2020 [39] | 10 | 3 | 5 | 5 | 0 | 22 |
| Daldal et al., 2020 [42] | 10 | 3 | 5 | 4 | 0 | 22 |
| Antić et al., 2021 [40] | 10 | 3 | 5 | 4 | 5 | 27 |
| Maghsoudi et al., 2021 [43] | 10 | 3 | 5 | 3 | 0 | 21 |
| Sönmez at al., 2021 [47] | 10 | 3 | 5 | 3 | 5 | 26 |
| Average Scores and Interobserver Agreement | |||||
|---|---|---|---|---|---|
| Study | Observer 1 | Observer 2 | Mean | Kappa | p |
| Tanrikulu et al., 2014 [45] | 26 | 26 | 26 | 0.935 | <0.0001 |
| Dinc et al., 2015 [38] | 21 | 22 | 21.5 | ||
| Narci et al., 2016 [31] | 25 | 26 | 25.5 | ||
| Ulukent et al., 2016 [44] | 24 | 24 | 24 | ||
| Bozlu et al., 2016 [32] | 21 | 21 | 21 | ||
| Acar et al., 2016 [46] | 23 | 24 | 23.5 | ||
| Boshnak et al., 2017 [3] | 22 | 23 | 22.5 | ||
| Toktas et al., 2017 [41] | 21 | 21 | 21 | ||
| Haghi et al., 2019 [30] | 24 | 25 | 24.5 | ||
| Tartar et al., 2020 [37] | 21 | 22 | 21.5 | ||
| Sengul et al., 2020 [39] | 20 | 22 | 21 | ||
| Daldal et al., 2020 [42] | 22 | 22 | 22 | ||
| Antić et al., 2021 [40] | 26 | 27 | 26.5 | ||
| Maghsoudi et al., 2021 [43] | 21 | 21 | 21 | ||
| Sönmez at al., 2021 [47] | 26 | 26 | 26 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anand, S.; Krishnan, N.; Jukić, M.; Križanac, Z.; Llorente Muñoz, C.M.; Pogorelić, Z. Utility of Red Cell Distribution Width (RDW) as a Noninvasive Biomarker for the Diagnosis of Acute Appendicitis: A Systematic Review and Meta-Analysis of 5222 Cases. Diagnostics 2022, 12, 1011. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12041011
Anand S, Krishnan N, Jukić M, Križanac Z, Llorente Muñoz CM, Pogorelić Z. Utility of Red Cell Distribution Width (RDW) as a Noninvasive Biomarker for the Diagnosis of Acute Appendicitis: A Systematic Review and Meta-Analysis of 5222 Cases. Diagnostics. 2022; 12(4):1011. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12041011
Chicago/Turabian StyleAnand, Sachit, Nellai Krishnan, Miro Jukić, Zvonimir Križanac, Carlos Martin Llorente Muñoz, and Zenon Pogorelić. 2022. "Utility of Red Cell Distribution Width (RDW) as a Noninvasive Biomarker for the Diagnosis of Acute Appendicitis: A Systematic Review and Meta-Analysis of 5222 Cases" Diagnostics 12, no. 4: 1011. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12041011