
CT-Angiography-Based Outcome Prediction on Diabetic Foot Ulcer Patients: A Statistical Learning Approach

 ,
,
Abstract
:1. Introduction
2. Methods and Materials
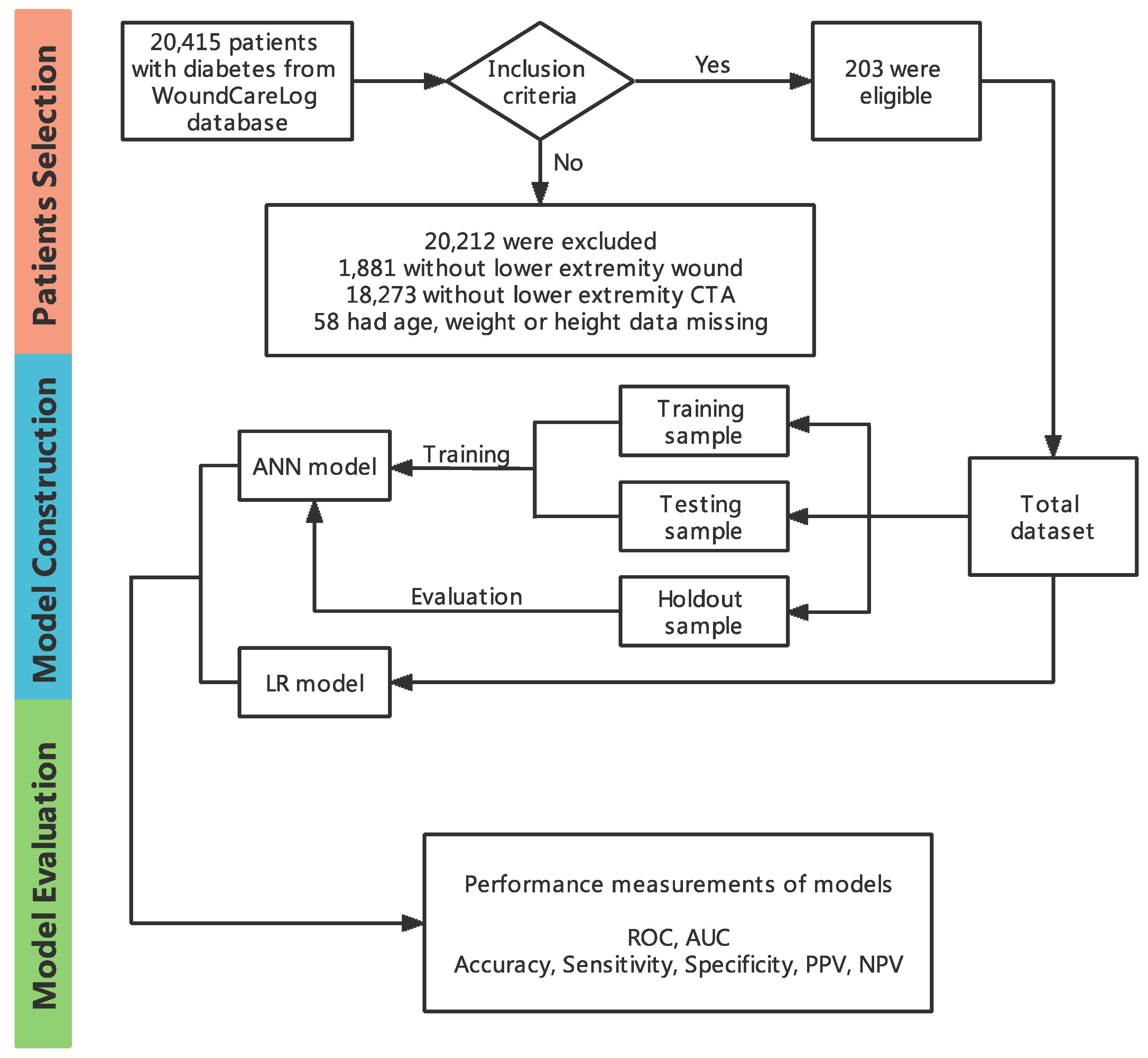
2.1. Study Identification and Data Extraction
2.2. Inclusion and Exclusion Criteria
2.3. Definition of Wound Grading
2.4. CT Scanning Protocol and Contrast Material Injection Protocol
2.5. CT Angiography Images Assessment
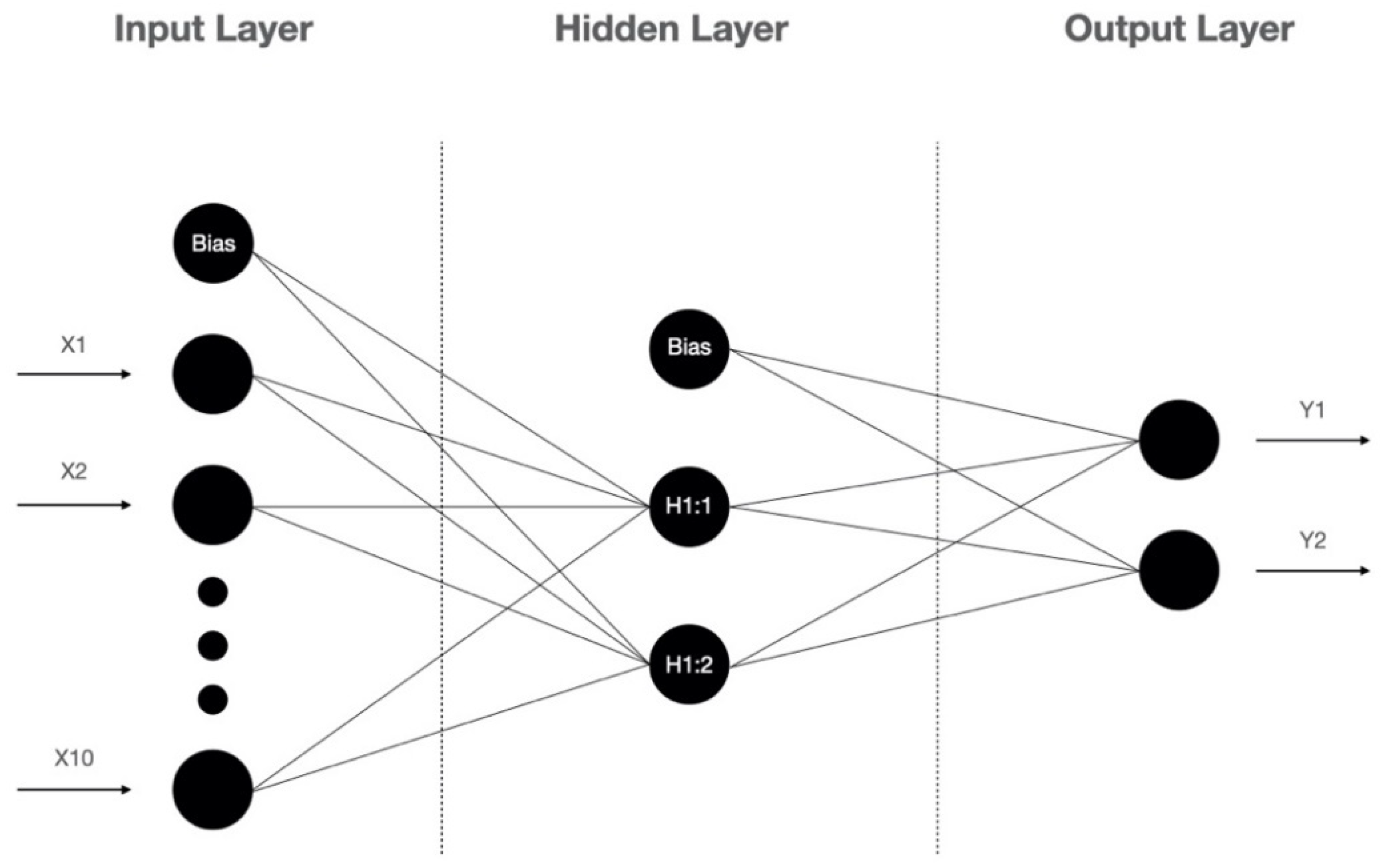
2.6. Artificial Neural Network Model
2.7. Statistical Analysis
3. Results
3.1. Patients’ Characteristics, and Comparisons between Patients with a Low and High Wagner Score
3.2. Correlation Analysis
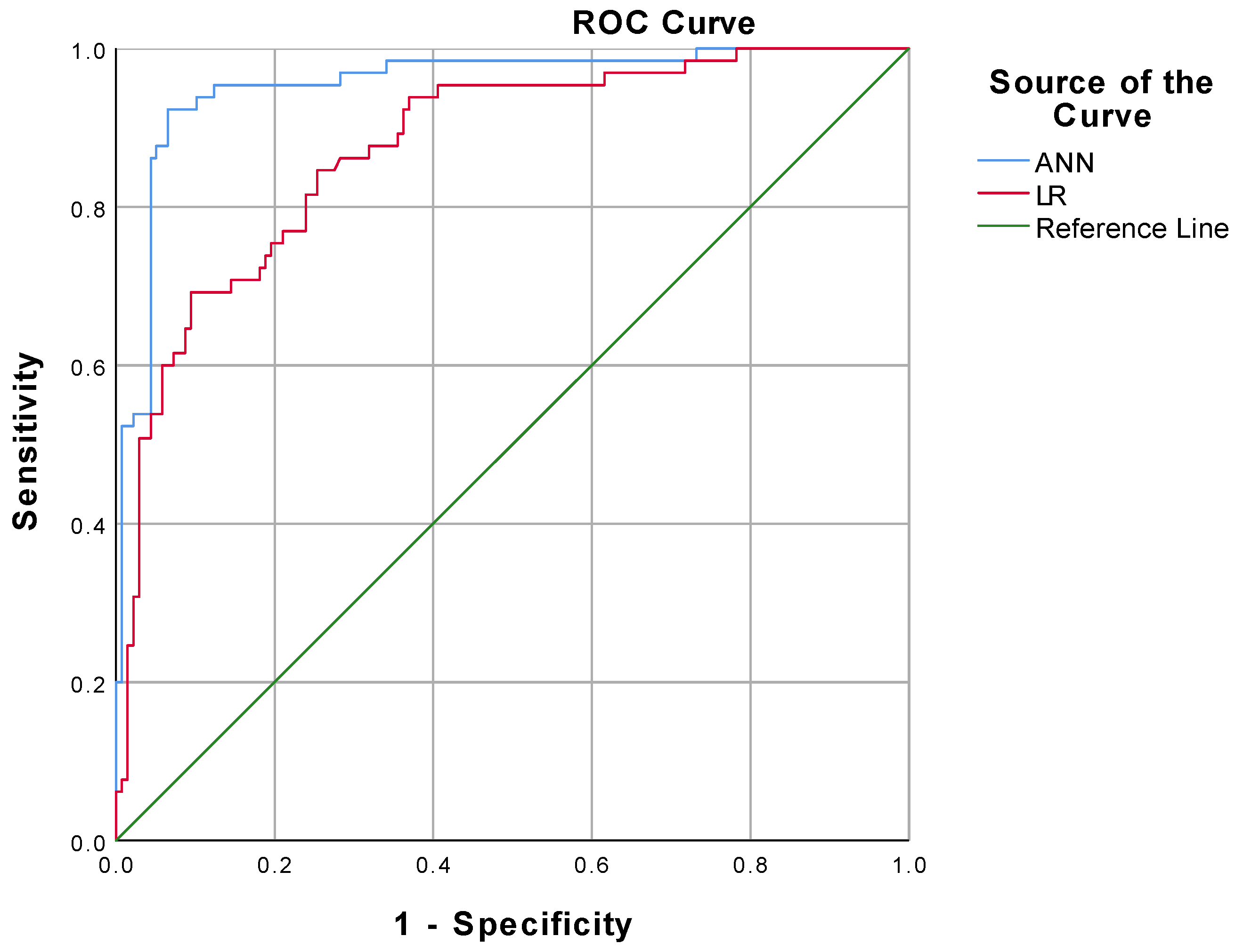
3.3. Model Analysis and Model Evaluation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Armstrong, D.G.; Boulton, A.J.M.; Bus, S.A. Diabetic Foot Ulcers and Their Recurrence. N. Engl. J. Med. 2017, 376, 2367–2375. [Google Scholar] [CrossRef]
- Lavery, L.A.; Davis, K.E.; Berriman, S.J.; Braun, L.; Nichols, A.; Kim, P.J.; Margolis, D.; Peters, E.J.; Attinger, C. WHS guidelines update: Diabetic foot ulcer treatment guidelines. Wound Repair Regen. 2016, 24, 112–126. [Google Scholar] [CrossRef] [PubMed]
- Walsh, J.W.; Hoffstad, O.J.; Sullivan, M.O.; Margolis, D.J. Association of diabetic foot ulcer and death in a population-based cohort from the United Kingdom. Diabet. Med. 2016, 33, 1493–1498. [Google Scholar] [CrossRef] [PubMed]
- Kerr, M.; Barron, E.; Chadwick, P.; Evans, T.; Kong, W.M.; Rayman, G.; Sutton-Smith, M.; Todd, G.; Young, B.; Jeffcoate, W.J. The cost of diabetic foot ulcers and amputations to the National Health Service in England. Diabet. Med. 2019, 36, 995–1002. [Google Scholar] [CrossRef] [PubMed]
- Boulton, A.J.; Vileikyte, L.; Ragnarson-Tennvall, G.; Apelqvist, J. The global burden of diabetic foot disease. Lancet 2005, 366, 1719–1724. [Google Scholar] [CrossRef]
- Harding, J.L.; Pavkov, M.E.; Gregg, E.W.; Burrows, N.R. Trends of Nontraumatic Lower-Extremity Amputation in End-Stage Renal Disease and Diabetes: United States, 2000–2015. Diabetes Care 2019, 42, 1430–1435. [Google Scholar] [CrossRef]
- Hingorani, A.; LaMuraglia, G.M.; Henke, P.; Meissner, M.H.; Loretz, L.; Zinszer, K.M.; Driver, V.R.; Frykberg, R.; Carman, T.L.; Marston, W.; et al. The management of diabetic foot: A clinical practice guideline by the Society for Vascular Surgery in collaboration with the American Podiatric Medical Association and the Society for Vascular Medicine. J. Vasc. Surg. 2016, 63, 3S–21S. [Google Scholar] [CrossRef] [Green Version]
- Everett, E.; Mathioudakis, N. Update on management of diabetic foot ulcers. Ann. N. Y. Acad. Sci. 2018, 1411, 153–165. [Google Scholar] [CrossRef]
- Dixon, D.; Edmonds, M. Managing Diabetic Foot Ulcers: Pharmacotherapy for Wound Healing. Drugs 2021, 81, 29–56. [Google Scholar] [CrossRef]
- Wang, Y.; Shao, T.; Wang, J.; Huang, X.; Deng, X.; Cao, Y.; Zhou, M.; Zhao, C. An update on potential biomarkers for diagnosing diabetic foot ulcer at early stage. Biomed. Pharmacother. 2021, 133, 110991. [Google Scholar] [CrossRef]
- Tabur, A.P.D.S.; Eren, M.A.; Çelik, Y.; Dağ, O.F.; Sabuncu, T.; Sayiner, Z.A.; Savas, E. The major predictors of amputation and length of stay in diabetic patients with acute foot ulceration. Wien. Klin. Wochenschr. 2015, 127, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Mey, L.; Szymanska, A.F.; Takhar, H.S.; Cuccia, D.J.; Mazhar, A.; Yu, K. SFDI biomarkers provide a quantitative ulcer risk metric and can be used to predict diabetic foot ulcer onset. J. Diabetes Its Complicat. 2020, 34, 107624. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Hasan, R.; Firwana, B.; Elraiyah, T.; Tsapas, A.; Prokop, L.; Mills, J.; Murad, M.H. A systematic review and meta-analysis of tests to predict wound healing in diabetic foot. J. Vasc. Surg. 2016, 63, 29S–36S.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Met, R.; Bipat, S.; Legemate, D.A.; Reekers, J.A.; Koelemay, M.J.W. Diagnostic Performance of Computed Tomography Angiography in Peripheral Arterial Disease. JAMA J. Am. Med. Assoc. 2009, 301, 415–424. [Google Scholar] [CrossRef]
- Meyersohn, N.M.; Walker, T.G.; Oliveira, G.R. Advances in Axial Imaging of Peripheral Vascular Disease. Curr. Cardiol. Rep. 2015, 17, 87. [Google Scholar] [CrossRef]
- Laswed, T.; Rizzo, E.; Guntern, D.; Doenz, F.; Denys, A.; Schnyder, P.; Qanadli, S.D. Assessment of occlusive arterial disease of abdominal aorta and lower extremities arteries: Value of multidetector CT angiography using an adaptive acquisition method. Eur. Radiol. 2007, 18, 263–272. [Google Scholar] [CrossRef]
- Schernthaner, R.; Stadler, A.; Lomoschitz, F.; Weber, M.; Fleischmann, D.; Lammer, J.; Loewe, C. Multidetector CT angiography in the assessment of peripheral arterial occlusive disease: Accuracy in detecting the severity, number, and length of stenoses. Eur. Radiol. 2007, 18, 665–671. [Google Scholar] [CrossRef]
- Atosona, A.; Larbie, C. Prevalence and Determinants of Diabetic Foot Ulcers and Lower Extremity Amputations in Three Selected Tertiary Hospitals in Ghana. J. Diabetes Res. 2019, 2019, 7132861. [Google Scholar] [CrossRef]
- Yazdanpanah, L.; Shahbazian, H.; Nazari, I.; Arti, H.R.; Ahmadi, F.; Mohamadianinejad, S.E.; Cheraghian, B.; Latifi, S.M. Prevalence and related risk factors of diabetic foot ulcer in Ahvaz, south west of Iran. Diabetes Metab. Syndr. Clin. Res. Rev. 2018, 12, 519–524. [Google Scholar] [CrossRef]
- Ahmadi, S.A.Y.; Shirzadegan, R.; Mousavi, N.; Farokhi, E.; Soleimaninejad, M.; Jafarzadeh, M. Designing a Logistic Regression Model for a Dataset to Predict Diabetic Foot Ulcer in Diabetic Patients: High-Density Lipoprotein (HDL) Cholesterol Was the Negative Predictor. J. Diabetes Res. 2021, 2021, 5521493. [Google Scholar] [CrossRef]
- Ramesh, A.N.; Kambhampati, C.; Monson, J.R.T.; Drew, P.J. Artificial intelligence in medicine. Ann. R. Coll. Surg. Engl. 2004, 86, 334–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dong, W.; Nie, L.-J.; Wu, M.-J.; Xie, T.; Liu, Y.-K.; Tang, J.-J.; Dong, J.-Y.; Qing, C.; Lu, S.-L. WoundCareLog APP—A new application to record wound diagnosis and healing. Chin. J. Traumatol. 2019, 22, 296–299. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.-H.; Tsai, J.-S.; Huang, C.-H.; Lin, C.-H.; Yang, H.-M.; Chan, Y.-S.; Hsieh, S.-H.; Hsu, B.; Huang, Y.-Y. Risk factors for lower extremity amputation in diabetic foot disease categorized by Wagner classification. Diabetes Res. Clin. Pract. 2012, 95, 358–363. [Google Scholar] [CrossRef] [PubMed]
- Bradley, A.P. The use of the area under the ROC curve in the evaluation of machine learning algorithms. Pattern Recognit. 1997, 30, 1145–1159. [Google Scholar] [CrossRef] [Green Version]
- Hossin, M.; Sulaiman, M.N. A Review on Evaluation Metrics for Data Classification Evaluations. Int. J. Data Min. Knowl. Manag. Process 2015, 5, 2. [Google Scholar] [CrossRef]
- Prompers, L.; Schaper, N.; Apelqvist, J.; Edmonds, M.; Jude, E.; Mauricio, D.; Uccioli, L.; Urbancic, V.; Bakker, K.; Holstein, P.; et al. Prediction of outcome in individuals with diabetic foot ulcers: Focus on the differences between individuals with and without peripheral arterial disease. The EURODIALE Study. Diabetologia 2008, 51, 747–755. [Google Scholar] [CrossRef] [Green Version]
- Brownrigg, J.; Apelqvist, J.; Bakker, K.; Schaper, N.; Hinchliffe, R. Evidence-based Management of PAD & the Diabetic Foot. Eur. J. Vasc. Endovasc. Surg. 2013, 45, 673–681. [Google Scholar] [CrossRef] [Green Version]
- Prompers, L.; Huijberts, M.; Apelqvist, J.; Jude, E.; Piaggesi, A.; Bakker, K.; Edmonds, M.; Holstein, P.; Jirkovska, A.; Mauricio, D.; et al. High prevalence of ischaemia, infection and serious comorbidity in patients with diabetic foot disease in Europe. Baseline results from the Eurodiale study. Diabetologia 2007, 50, 18–25. [Google Scholar] [CrossRef] [Green Version]
- Willmann, J.K.; Baumert, B.; Schertler, T.; Wildermuth, S.; Pfammatter, T.; Verdun, F.R.; Seifert, B.; Marincek, B.; Böhm, T. Aortoiliac and Lower Extremity Arteries Assessed with 16–Detector Row CT Angiography: Prospective Comparison with Digital Subtraction Angiography. Radiology 2005, 236, 1083–1093. [Google Scholar] [CrossRef] [Green Version]
- Karamanli, H.; Yalcinoz, T.; Yalcinoz, M.A.; Yalcinoz, T. A prediction model based on artificial neural networks for the diagnosis of obstructive sleep apnea. Sleep Breath. 2015, 20, 509–514. [Google Scholar] [CrossRef]
- Yin, M.; Ma, J.; Xu, J.; Li, L.; Chen, G.; Sun, Z.; Liu, Y.; He, S.; Ye, J.; Mo, W. Use of artificial neural networks to identify the predictive factors of extracorporeal shock wave therapy treating patients with chronic plantar fasciitis. Sci. Rep. 2019, 9, 4207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, C.-C.; Wang, Y.-C.; Chen, J.-Y.; Liou, Y.-J.; Bai, Y.-M.; Lai, I.-C.; Chen, T.-T.; Chiu, H.-W.; Li, Y.-C. Artificial neural network prediction of clozapine response with combined pharmacogenetic and clinical data. Comput. Methods Programs Biomed. 2008, 91, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Finne, P.; Finne, R.; Auvinen, A.; Juusela, H.; Aro, J.; Määttänen, L.; Hakama, M.; Rannikko, S.; Tammela, T.L.; Stenman, U.-H. Predicting the outcome of prostate biopsy in screen-positive men by a multilayer perceptron network. Urology 2000, 56, 418–422. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Classification | Total (n = 203) |
|---|---|---|
| Gender (n [%]) | Male | 141 (69.5) |
| Female | 62 (30.5) | |
| Age (years) | 67 ± 11 | |
| BMI (kg/m2) | 23.9 (22.4, 26.4) | |
| DM duration (years) | 10 (4, 15) | |
| DFU duration (years) | 1 (1, 3) | |
| Limb symptoms (n [%]) | Asymptomatic | 129 (63.5) |
| Mild or moderate claudication | 25 (12.3) | |
| Severe claudication | 22 (10.8) | |
| Critical limb ischemia | 27 (13.3) | |
| Degree of lower extremity arterial stenosis | Degree 0 | 19 (9.4) |
| Degree 1 | 36 (17.7) | |
| Degree 2 | 66 (32.5) | |
| Degree 3 | 82 (40.4) | |
| Segment of lower extremity arterial stenosis | No stenosis | 19 (9.4) |
| Abdominal aorta | 26 (12.8) | |
| Common iliac artery | 19 (9.4) | |
| External iliac artery | 9 (4.4) | |
| Deep femoral artery | 8 (3.9) | |
| Femoral artery | 48 (23.6) | |
| Popliteal artery | 26 (12.8) | |
| Anterior tibial artery | 37 (18.2) | |
| Posterior tibial artery | 5 (2.5) | |
| Peroneal artery | 3 (1.5) | |
| Dorsalis pedis artery | 3 (1.5) | |
| Arterial calcification | No | 67 (33.0) |
| Yes | 136 (67.0) | |
| Comorbidities | No comorbidity | 40 (19.7) |
| Cerebral vascular accident | 50 (24.6) | |
| Dyslipidemia | 26 (12.8) | |
| Hypertension | 115 (56.7) | |
| Ischemic heart disease | 71 (35.0) | |
| Nephropathy | 22 (10.8) | |
| Retinopathy | 10 (4.9) | |
| Peripheral neuropathy | 58 (28.6) |
| Characteristics | Low Wagner Score | High Wagner Score | p Value |
|---|---|---|---|
| Patients (n) | 138 | 65 | — |
| Gender (n [%]) | 0.304 | ||
| Male | 99 | 42 | |
| Female | 39 | 23 | |
| Age (years) | 64 ± 11 | 72 ± 10 | 0.000 ** |
| BMI (kg/m2) | 24.8 (22.6, 26.9) | 23.4 (21.5, 24.7) | 0.000 ** |
| DM duration (years) | 7 (3, 11) | 11 (8, 24) | 0.000 ** |
| DFU duration (years) | 1 (1, 2) | 2 (1, 6) | 0.017 * |
| Limb symptoms (n [%]) | 0.003 ** | ||
| Asymptomatic | 89 | 40 | |
| Mild or moderate claudication | 18 | 7 | |
| Severe claudication | 8 | 14 | |
| Critical limb ischemia | 23 | 4 | |
| Degree of lower extremity arterial stenosis | 0.000 ** | ||
| Degree 0 | 18 | 1 | |
| Degree 1 | 32 | 4 | |
| Degree 2 | 34 | 32 | |
| Degree 3 | 54 | 28 | |
| Segment of lower extremity arterial stenosis | 0.008 ** | ||
| No stenosis | 18 | 1 | |
| Abdominal aorta | 24 | 2 | |
| Common iliac artery | 10 | 9 | |
| External iliac artery | 6 | 3 | |
| Deep femoral artery | 4 | 4 | |
| Femoral artery | 31 | 17 | |
| Popliteal artery | 13 | 13 | |
| Anterior tibial artery | 25 | 12 | |
| Posterior tibial artery | 2 | 3 | |
| Peroneal artery | 3 | 0 | |
| Dorsalis pedis artery | 2 | 1 | |
| Arterial calcification | 0.081 | ||
| No | 51 | 16 | |
| Yes | 87 | 49 | |
| Comorbidities | 0.113 | ||
| No | 23 | 17 | |
| Yes | 115 | 48 |
| Variables | Spearman’s Coefficient (ρ) | p Value |
|---|---|---|
| Gender | −0.072 | 0.306 |
| Age | 0.331 | 0.000 ** |
| BMI | −0.249 | 0.000 ** |
| DM duration | 0.343 | 0.000 ** |
| DFU duration | 0.168 | 0.017 * |
| Comorbidity | −0.111 | 0.114 |
| Limb symptoms | 0.009 | 0.903 |
| Degree of lower extremity arterial stenosis | 0.174 | 0.013 * |
| Segment of lower extremity arterial stenosis | 0.178 | 0.011 * |
| Arterial calcification | 0.122 | 0.082 |
| Performance Matrix | Formula | ANN (%) | ANN Holdout (%) | LR (%) |
|---|---|---|---|---|
| Accuracy | 91.6 | 88.9 | 82.8 | |
| Sensitivity | 92.3 | 90.0 | 69.2 | |
| Specificity | 93.5 | 88.5 | 90.6 | |
| PPV | 87.0 | 75.0 | 77.6 | |
| NPV | 94.2 | 95.8 | 92.5 |
| AUC | S.E. | 95% Confidence Interval | ||
|---|---|---|---|---|
| Lower Bound | Upper Bound | |||
| ANN | 0.955 | 0.016 | 0.924 | 0.986 |
| LR | 0.874 | 0.026 | 0.823 | 0.925 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, D.; Dong, W.; Guan, H.; Yakupu, A.; Wang, H.; Chen, L.; Lu, S.; Tang, J. CT-Angiography-Based Outcome Prediction on Diabetic Foot Ulcer Patients: A Statistical Learning Approach. Diagnostics 2022, 12, 1076. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12051076
Zhang D, Dong W, Guan H, Yakupu A, Wang H, Chen L, Lu S, Tang J. CT-Angiography-Based Outcome Prediction on Diabetic Foot Ulcer Patients: A Statistical Learning Approach. Diagnostics. 2022; 12(5):1076. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12051076
Chicago/Turabian StyleZhang, Di, Wei Dong, Haonan Guan, Aobuliaximu Yakupu, Hanqi Wang, Liuping Chen, Shuliang Lu, and Jiajun Tang. 2022. "CT-Angiography-Based Outcome Prediction on Diabetic Foot Ulcer Patients: A Statistical Learning Approach" Diagnostics 12, no. 5: 1076. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12051076