
The Effectiveness and Tolerability of a Very Low-Volume Bowel Preparation for Colonoscopy Compared to Low and High-Volume Polyethylene Glycol-Solutions in the Real-Life Setting

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Study Population and Characteristics
3.2. Bowel Cleansing Efficacy
3.3. Predictors of Overall Cleansing Success and High-Quality Cleansing of the Right Colon
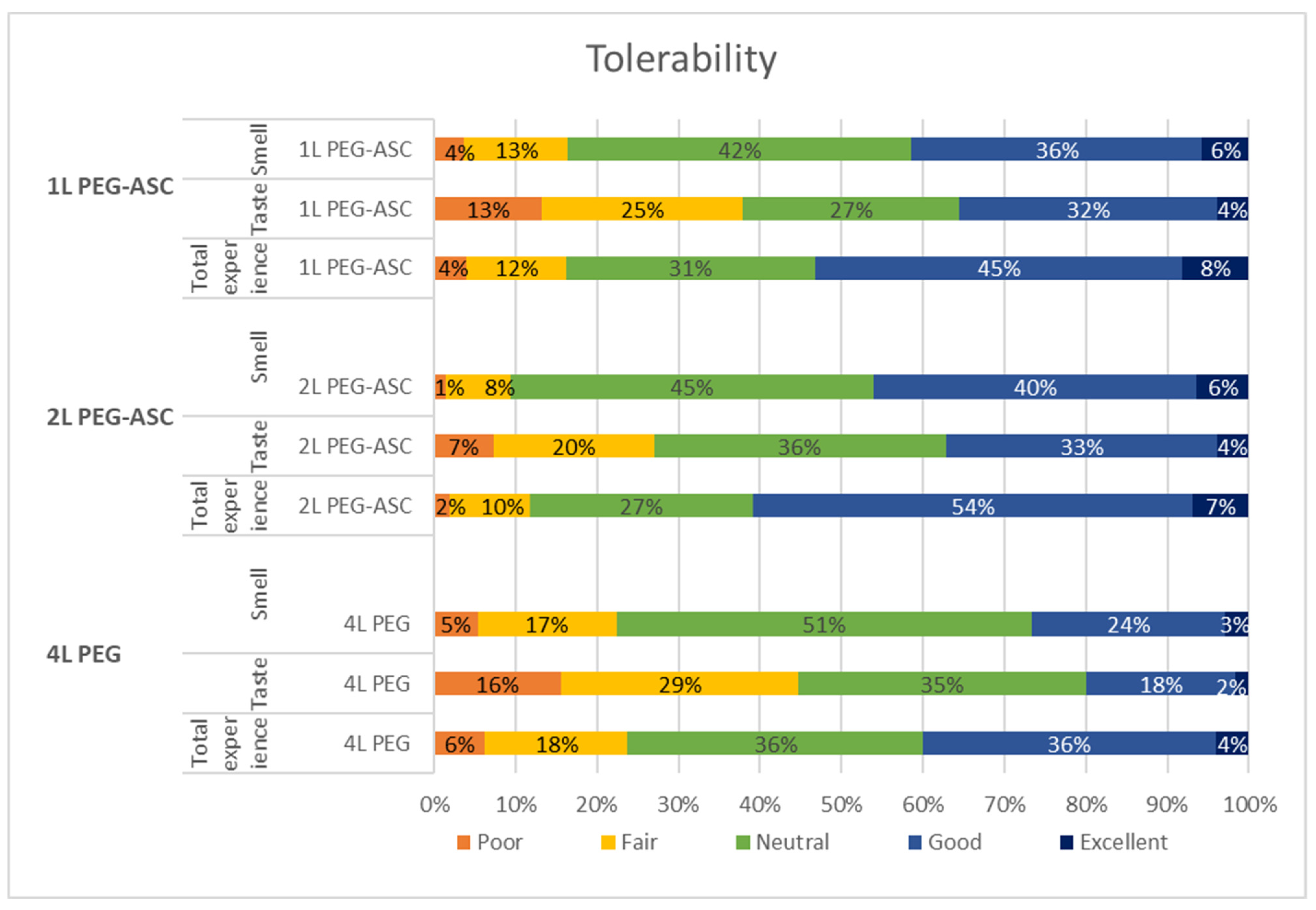
3.4. Adherence and Tolerability
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Örebro | Karlskoga | Malmö | Linköping | Stockholm GMC | Stockholm Ersta | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age | 60 (22–85) | 61 (21–89) | 62 (21–91) | 55 (18–85) | 54 (18–84) | 59 (19–89) | ||||||
| Gender m/f | 66/68 | 57/59 | 88/109 | 91/118 | 108/109 | 99/95 | ||||||
| CIR | 134/144 (93%) | 118/129 (92%) | 186/197 (94%) | 201/211 (95%) | 208/217 (96%) | 180/197 (92%) | ||||||
| Movprep (n = 104) | Plenvu (n = 37) | Laxabon (n = 46) | Plenvu (n = 75) | Laxabon (n = 100) | Plenvu (n = 97) | Vistaprep (n = 101) | Plenvu (n = 109) | Vistaprep (n = 117) | Plenvu (n = 100) | Movprep (n = 93) | Plenvu (n = 100) | |
| Smell | 4.0 (3.0–4.0) | 3.0 (3.0–4.0) | 3.0 (2.0–3.0) | 3.0 (3.0–4.0) ** | 3.0 (2.0–3.0) | 4.0 (3.0–4.0) *** | 3.0 (3.0–4.0) | 4.0 (3.0–4.0) | 3.0 (3.0–4.0) | 3.0 (3.0–4.0) | 3.0 (3.0–4.0) | 4.0 (3.0–4.0) |
| Taste | 3.0 (2.0–4.0) | 3.0 (2.0–4.0) | 3.0 (2.0–4.0) | 3.0 (2.0–4.0) | 3 (1.5–3.0) | 3.0 (2.0–4.0) | 3.0 (2.0–4.0) | 3.0 (2.0–4.0) | 3.0 (2.0–3.0) | 3.0 (2.0–4.0) | 3.0 (3.0–4.0) | 3.0 (2.0–4.0) |
| Overall experience | 4.0 (3.0–4.0) | 4.0 (3.0–4.0) | 3.0 (3.0–4.0) | 4.0 (3.0–4.0) * | 4.0 (3.0–4.0) | 4.0 (3.0–4.0) | 3.0 (3.0–4.0) | 4.0 (3.0–4.0) | 3.0 (2.0–4.0) | 4.0 (3.0–4.0) *** | 4.0 (3.0–4.0) | 4.0 (3.0–4.0) |
| Ingestion of all laxative | 104 (95%) | 37 (93%) | 40 (89%) | 71 (95%) | 85 (86%) | 90 (93%) | 82 (81%) | 97 (88%) | 100 (86%) | 92 (92%) | 89 (96%) | 87 (88%) |
| Nausea | 27 (25%) | 17 (43%) | 16 (35%) | 34 (45%) | 36 (36%) | 38 (39%) | 34 (34%) | 55 (50%) * | 48 (41%) | 42 (42%) | 18 (20%) | 37 (38%) * |
| Vomiting | 4 (4%) | 8 (20%) ** | 4 (9%) | 9 (12%) | 9 (9%) | 10 (10%) | 2 (2%) | 15 (14%) ** | 9 (8%) | 10 (10%) | 4 (4%) | 8 (8%) |
| BBPS Right | 2.5 (0.7) | 3.0 (0.2) *** | 2.5 (0.5) | 2.7 (0.6) * | 2.6 (0.6) | 2.7 (0.5) | 2.5 (0.6) | 2.8 (0.5) *** | 2.6 (0.5) | 2.7 (0.6) | 2.3 (0.7) | 2.6 (0.6) *** |
| BBPS Transverse | 2.6 (0.7) | 3.0 (0.0) *** | 2.6 (0.5) | 2.7 (0.7) | 2.7 (0.5) | 2.8 (0.4) | 2.7 (0.5) | 2.8 (0.5) | 2.7 (0.5) | 2.8 (0.5) | 2.4 (0.6) | 2.7 (0.5) *** |
| BBPS Left | 2.6 (0.7) | 3.0 (0.2) *** | 2.5 (0.5) | 2.6 (0.7) | 2.7 (0.6) | 2.7 (0.5) | 2.6 (0.5) | 2.8 (0.6) * | 2.7 (0.5) | 1.8 (0.5) | 2.3 (0.6) | 2.7 (0.5) *** |
| BBPS Total | 7.6 (2.0) | 8.9 (0.3) *** | 7.3 (1.9) | 7.7 (2.4) | 8.1 (1.4) | 8.3 (1.3) | 7.8 (1.2) | 8.4 (1.2) *** | 8.0 (1.4) | 8.3 (1.5) | 6.9 (1.8) | 8.2 (1.3) *** |
| BBPS ≥ 6 | 102 (94%) | 40 (100%) | 45 (98%) | 17 (93%) | 96 (96%) | 96 (99%) | 97 (96%) | 107 (97%) | 116 (99%) | 97 (97%) | 89 (96%) | 97 (97%) |
| BBPS = 9 | 54 (54%) | 36 (92%) | 19 (42%) | 49 (67%) ** | 61 (65%) | 69 (73%) | 37 (39%) | 79 (75%) *** | 68 (58%) | 73 (73%) * | 30 (35%) | 64 (68%) *** |
| BBPS Right = 3 | 64 (63%) | 37 (95%) *** | 20 (46%) | 53 (74%) ** | 64 (68%) | 72 (76%) | 47 (50%) | 87 (83%) *** | 71 (61%) | 76 (76%) * | 31 (37%) | 66 (69%) *** |
| CIR | 95 (91%) | 36 (97%) | 44 (96%) | 67 (92%) | 93 (93%) | 93 (96%) | 95 (62%) | 105(96%) | 114 (97%) | 94 (94%) | 80 (94%) | 94 (94%) |
References
- Bechtold, M.L.; Mir, F.; Puli, S.R.; Nguyen, D.L. Optimizing bowel preparation for colonoscopy: A guide to enhance quality of visualization. Ann. Gastroenterol. 2016, 29, 137–146. [Google Scholar] [CrossRef] [PubMed]
- Brenner, H.; Stock, C.; Hoffmeister, M. Effect of screening sigmoidoscopy and screening colonoscopy on colorectal cancer incidence and mortality: Systematic review and meta-analysis of randomised controlled trials and observational studies. BMJ 2014, 348, g2467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baxter, N.N.; Warren, J.L.; Barrett, M.J.; Stukel, T.A.; Doria-Rose, V.P. Association between colonoscopy and colorectal cancer mortality in a US cohort according to site of cancer and colonoscopist specialty. J. Clin. Oncol. 2012, 30, 2664–2669. [Google Scholar] [CrossRef] [PubMed]
- Clark, B.T.; Rustagi, T.; Laine, L. What level of bowel prep quality requires early repeat colonoscopy: Systematic review and meta-analysis of the impact of preparation quality on adenoma detection rate. Am. J. Gastroenterol. 2014, 109, 1714–1723, quiz 1724. [Google Scholar] [CrossRef] [Green Version]
- Sulz, M.C.; Kröger, A.; Prakash, M.; Manser, C.N.; Heinrich, H.; Misselwitz, B. Meta-Analysis of the Effect of Bowel Preparation on Adenoma Detection: Early Adenomas Affected Stronger than Advanced Adenomas. PLoS ONE 2016, 11, e0154149. [Google Scholar] [CrossRef] [Green Version]
- Clark, B.T.; Protiva, P.; Nagar, A.; Imaeda, A.; Ciarleglio, M.M.; Deng, Y.; Laine, L. Quantification of Adequate Bowel Preparation for Screening or Surveillance Colonoscopy in Men. Gastroenterology 2016, 150, 396–405. [Google Scholar] [CrossRef] [Green Version]
- Clark, B.T.; Laine, L. High-quality Bowel Preparation Is Required for Detection of Sessile Serrated Polyps. Clin. Gastroenterol. Hepatol. 2016, 14, 1155–1162. [Google Scholar] [CrossRef] [Green Version]
- Hsu, C.M.; Lin, W.P.; Su, M.Y.; Chiu, C.T.; Ho, Y.P.; Chen, P.C. Factors that influence cecal intubation rate during colonoscopy in deeply sedated patients. J. Gastroenterol. Hepatol. 2012, 27, 76–80. [Google Scholar] [CrossRef]
- Radaelli, F.; Meucci, G.; Sgroi, G.; Minoli, G. Technical performance of colonoscopy: The key role of sedation/analgesia and other quality indicators. Am. J. Gastroenterol. 2008, 103, 1122–1130. [Google Scholar] [CrossRef]
- Aslinia, F.; Uradomo, L.; Steele, A.; Greenwald, B.D.; Raufman, J.P. Quality assessment of colonoscopic cecal intubation: An analysis of 6 years of continuous practice at a university hospital. Am. J. Gastroenterol. 2006, 101, 721–731. [Google Scholar] [CrossRef]
- Bugajski, M.; Wieszczy, P.; Hoff, G.; Rupinski, M.; Regula, J.; Kaminski, M.F. Modifiable factors associated with patient-reported pain during and after screening colonoscopy. Gut 2018, 67, 1958–1964. [Google Scholar] [CrossRef] [PubMed]
- Yadlapati, R.; Johnston, E.R.; Gregory, D.L.; Ciolino, J.D.; Cooper, A.; Keswani, R.N. Predictors of Inadequate Inpatient Colonoscopy Preparation and Its Association with Hospital Length of Stay and Costs. Dig. Dis. Sci. 2015, 60, 3482–3490. [Google Scholar] [CrossRef] [PubMed]
- Rex, D.K.; Imperiale, T.F.; Latinovich, D.R.; Bratcher, L.L. Impact of bowel preparation on efficiency and cost of colonoscopy. Am. J. Gastroenterol. 2002, 97, 1696–1700. [Google Scholar] [CrossRef] [PubMed]
- Kaminski, M.F.; Thomas-Gibson, S.; Bugajski, M.; Bretthauer, M.; Rees, C.J.; Dekker, E.; Hoff, G.; Jover, R.; Suchanek, S.; Ferlitsch, M.; et al. Performance measures for lower gastrointestinal endoscopy: A European Society of Gastrointestinal Endoscopy (ESGE) Quality Improvement Initiative. Endoscopy 2017, 49, 378–397. [Google Scholar]
- Martel, M.; Barkun, A.N.; Menard, C.; Restellini, S.; Kherad, O.; Vanasse, A. Split-Dose Preparations Are Superior to Day-Before Bowel Cleansing Regimens: A Meta-analysis. Gastroenterology 2015, 149, 79–88. [Google Scholar] [CrossRef] [Green Version]
- Shah, H.; Desai, D.; Samant, H.; Davavala, S.; Joshi, A.; Gupta, T.; Abraham, P. Comparison of split-dosing vs non-split (morning) dosing regimen for assessment of quality of bowel preparation for colonoscopy. World J. Gastrointest. Endosc. 2014, 6, 606–611. [Google Scholar] [CrossRef]
- Spadaccini, M.; Frazzoni, L.; Vanella, G.; East, J.; Radaelli, F.; Spada, C.; Fuccio, L.; Benamouzig, R.; Bisschops, R.; Bretthauer, M.; et al. Efficacy and Tolerability of High- vs Low-Volume Split-Dose Bowel Cleansing Regimens for Colonoscopy: A Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2020, 18, 1454–1465.e14. [Google Scholar] [CrossRef]
- DiPalma, J.A.; Marshall, J.B. Comparison of a new sulfate-free polyethylene glycol electrolyte lavage solution versus a standard solution for colonoscopy cleansing. Gastrointest. Endosc. 1990, 36, 285–289. [Google Scholar] [CrossRef]
- Wirström, G.; Lindfors, T.; Lindfors, P. Patient Satisfaction and Efficiency of Sulphate-Free High-Volume Makrogol Laxative Compared to Standard High-Volume Makrogol Laxative as Preparation to Colonoscopy, a Pseudo-Randomized Controlled Study; Abstract: A-946-0128-02233, UEG Week 2018; 2018; Available online: https://0-doi-org.brum.beds.ac.uk/10.1177/2050640618792832 (accessed on 16 March 2022).
- Marmo, R.; Rotondano, G.; Riccio, G.; Marone, A.; Bianco, M.A.; Stroppa, I.; Caruso, A.; Pandolfo, N.; Sansone, S.; Gregorio, E.; et al. Effective bowel cleansing before colonoscopy: A randomized study of split-dosage versus non-split dosage regimens of high-volume versus low-volume polyethylene glycol solutions. Gastrointest. Endosc. 2010, 72, 313–320. [Google Scholar] [CrossRef]
- Ell, C.; Fischbach, W.; Bronisch, H.J.; Dertinger, S.; Layer, P.; Rünzi, M.; Schneider, T.; Kachel, G.; Grüger, J.; Köllinger, M.; et al. Randomized trial of low-volume PEG solution versus standard PEG + electrolytes for bowel cleansing before colonoscopy. Am. J. Gastroenterol. 2008, 103, 883–893. [Google Scholar] [CrossRef]
- Yi, L.J.; Tian, X.; Shi, B.; Chen, H.; Liu, X.L.; Pi, Y.P.; Chen, W.Q. Low-Volume Polyethylene Glycol Improved Patient Attendance in Bowel Preparation Before Colonoscopy: A Meta-Analysis With Trial Sequential Analysis. Front. Med. 2019, 6, 92. [Google Scholar] [CrossRef]
- Maida, M.; Sinagra, E.; Morreale, G.C.; Sferrazza, S.; Scalisi, G.; Schillaci, D.; Ventimiglia, M.; Macaluso, F.S.; Vettori, G.; Conoscenti, G.; et al. Effectiveness of very low-volume preparation for colonoscopy: A prospective, multicenter observational study. World J. Gastroenterol. 2020, 26, 1950–1961. [Google Scholar] [CrossRef] [PubMed]
- Baile-Maxia, S.; Amlani, B.; Martínez, R.J. Bowel-cleansing efficacy of the 1L polyethylene glycol-based bowel preparation NER1006 (PLENVU) in patient subgroups in two phase III trials. Ther. Adv. Gastroenterol. 2021, 14, 17562848211020286. [Google Scholar] [CrossRef] [PubMed]
- Clayton, L.B.; Tayo, B.; Halphen, M.; Kornberger, R. Novel 1 L polyethylene glycol-based bowel preparation (NER1006): Proof of concept assessment versus standard 2 L polyethylene glycol with ascorbate—A randomized, parallel group, phase 2, colonoscopist-blinded trial. BMC Gastroenterol. 2019, 19, 79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Epstein, M.; Halonen, J.; Sharma, P. Bowel preparation with 1L polyethylene glycol and ascorbate NER1006 doubles the chance to detect three or more adenomas in overweight or obese males. Endosc. Int. Open 2021, 9, E1324–E1334. [Google Scholar] [CrossRef]
- Kang, S.H.; Jeen, Y.T.; Lee, J.H.; Yoo, I.K.; Lee, J.M.; Kim, S.H.; Choi, H.S.; Kim, E.S.; Keum, B.; Lee, H.S.; et al. Comparison of a split-dose bowel preparation with 2 liters of polyethylene glycol plus ascorbic acid and 1 liter of polyethylene glycol plus ascorbic acid and bisacodyl before colonoscopy. Gastrointest. Endosc. 2017, 86, 343–348. [Google Scholar] [CrossRef]
- Bisschops, R.; Manning, J.; Clayton, L.B.; Ng Kwet Shing, R.; Álvarez-González, M. Colon cleansing efficacy and safety with 1 L NER1006 versus 2 L polyethylene glycol + ascorbate: A randomized phase 3 trial. Endoscopy 2019, 51, 60–72. [Google Scholar] [CrossRef]
- Frazzoni, L.; Spada, C.; Radaelli, F.; Mussetto, A.; Laterza, L.; La Marca, M.; Piccirelli, S.; Cortellini, F.; Rondonotti, E.; Paci, V.; et al. 1L- vs. 4L-Polyethylene glycol for bowel preparation before colonoscopy among inpatients: A propensity score-matching analysis. Dig. Liver Dis. 2020, 52, 1486–1493. [Google Scholar] [CrossRef]
- Kim, S.H.; Kim, E.R.; Kim, K.; Kim, T.J.; Hong, S.N.; Chang, D.K.; Kim, Y.H. Combination of bisacodyl suppository and 1 L polyethylene glycol plus ascorbic acid is a non-inferior and comfortable regimen compared to 2 L polyethylene glycol plus ascorbic acid. Dig. Endosc. 2020, 32, 600–607. [Google Scholar] [CrossRef]
- Kwon, J.E.; Lee, J.W.; Im, J.P.; Kim, J.W.; Kim, S.H.; Koh, S.J.; Kim, B.G.; Lee, K.L.; Kim, S.G.; Kim, J.S.; et al. Comparable Efficacy of a 1-L PEG and Ascorbic Acid Solution Administered with Bisacodyl versus a 2-L PEG and Ascorbic Acid Solution for Colonoscopy Preparation: A Prospective, Randomized and Investigator-Blinded Trial. PLoS ONE 2016, 11, e0162051. [Google Scholar] [CrossRef]
- Hong, S.N.; Lee, C.K.; Im, J.P.; Choi, C.H.; Byeon, J.S.; Cho, Y.S.; Jung, S.A.; Kim, T.I.; Jeen, Y.T. Efficacy and safety of split-dose bowel preparation with 1 L polyethylene glycol and ascorbate compared with 2 L polyethylene glycol and ascorbate in a Korean population: A phase IV, multicenter, randomized, endoscopist-blinded study. Gastrointest. Endosc. 2022, 95, 500–511.e2. [Google Scholar] [CrossRef] [PubMed]
- Cash, B.D.; Moncrief, M.B.C.; Epstein, M.S.; Poppers, D.M. Patient experience with NER1006 as a bowel preparation for colonoscopy: A prospective, multicenter US survey. BMC Gastroenterol. 2021, 21, 70. [Google Scholar] [CrossRef] [PubMed]
- Lai, E.J.; Calderwood, A.H.; Doros, G.; Fix, O.K.; Jacobson, B.C. The Boston bowel preparation scale: A valid and reliable instrument for colonoscopy-oriented research. Gastrointest. Endosc. 2009, 69 Pt 2, 620–625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doubeni, C.A.; Corley, D.A.; Quinn, V.P.; Jensen, C.D.; Zauber, A.G.; Goodman, M.; Johnson, J.R.; Mehta, S.J.; Becerra, T.A.; Zhao, W.K.; et al. Effectiveness of screening colonoscopy in reducing the risk of death from right and left colon cancer: A large community-based study. Gut 2018, 67, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Oh, C.H.; Lee, C.K.; Kim, J.W.; Shim, J.J.; Jang, J.Y. Suboptimal Bowel Preparation Significantly Impairs Colonoscopic Detection of Non-polypoid Colorectal Neoplasms. Dig. Dis. Sci. 2015, 60, 2294–2303. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, B.C.; Calderwood, A.H. Measuring bowel preparation adequacy in colonoscopy-based research: Review of key considerations. Gastrointest. Endosc. 2020, 91, 248–256. [Google Scholar] [CrossRef]
- Hassan, C.; Manning, J.; Álvarez González, M.A.; Sharma, P.; Epstein, M.; Bisschops, R. Improved detection of colorectal adenomas by high-quality colon cleansing. Endosc. Int. Open 2020, 8, E928–E937. [Google Scholar] [CrossRef]
- Pohl, J.; Halphen, M.; Kloess, H.R.; Fischbach, W. Impact of the quality of bowel cleansing on the efficacy of colonic cancer screening: A prospective, randomized, blinded study. PLoS ONE 2015, 10, e0126067. [Google Scholar] [CrossRef] [Green Version]
- DeMicco, M.P.; Clayton, L.B.; Pilot, J.; Epstein, M.S. Novel 1 L polyethylene glycol-based bowel preparation NER1006 for overall and right-sided colon cleansing: A randomized controlled phase 3 trial versus trisulfate. Gastrointest. Endosc. 2018, 87, 677–687.e3. [Google Scholar] [CrossRef] [Green Version]
- Manning, J.; Halonen, J.; Cheriyamkunnel, S.J.; Álvarez-González, M.A. 1L NER1006 can improve rates of adequate and high-quality bowel cleansing in the right colon: A post hoc analysis of two randomised clinical trials. BMC Gastroenterol. 2022, 22, 35. [Google Scholar] [CrossRef]
- Waldmann, E.; Penz, D.; Majcher, B.; Zagata, J.; Šinkovec, H.; Heinze, G.; Dokladanska, A.; Szymanska, A.; Trauner, M.; Ferlitsch, A.; et al. Impact of high-volume, intermediate-volume and low-volume bowel preparation on colonoscopy quality and patient satisfaction: An observational study. United Eur. Gastroenterol. J. 2019, 7, 114–124. [Google Scholar] [CrossRef] [PubMed]
- Harewood, G.C.; Wiersema, M.J.; Melton, L.J., 3rd. A prospective, controlled assessment of factors influencing acceptance of screening colonoscopy. Am. J. Gastroenterol. 2002, 97, 3186–3194. [Google Scholar] [CrossRef] [PubMed]
- Yuan, X.; Zhang, Z.; Xie, J.; Zhang, Y.; Xu, L.; Wang, W.; Xu, L. Comparison of 1L Adjuvant Auxiliary Preparations with 2L Solely Polyethylene Glycol plus Ascorbic Acid Regime for Bowel Cleaning: A Meta-analysis of Randomized, Controlled Trials. Biomed. Res. Int. 2021, 2021, 6638858. [Google Scholar] [CrossRef]
- Maida, M.; Macaluso, F.S.; Sferrazza, S.; Ventimiglia, M.; Sinagra, E. Effectiveness and safety of NER1006 versus standard bowel preparations: A meta-analysis of randomized phase-3 clinical trials. Dig. Liver Dis. 2020, 52, 833–839. [Google Scholar] [CrossRef] [PubMed]
- Schreiber, S.; Baumgart, D.C.; Drenth, J.P.H.; Filip, R.S.; Clayton, L.B.; Hylands, K.; Repici, A.; Hassan, C. Colon cleansing efficacy and safety with 1 L NER1006 versus sodium picosulfate with magnesium citrate: A randomized phase 3 trial. Endoscopy 2019, 51, 73–84. [Google Scholar] [CrossRef] [PubMed]
- Radaelli, F. The paradox of the novel 1 L polyethylene glycol bowel preparation: Efficacy, not tolerability, is the great new! Endoscopy 2019, 51, 7–9. [Google Scholar] [CrossRef]
- Oliveira, A.; Mascarenhas-Saraiva, M. Tolerance and efficiency of a novel low-volume PEG + Ascorbate (NER1006) preparation in the elderly: A real-life single center study. Endoscopy 2019, 51, 25. [Google Scholar]
- Hassan, C.; East, J.; Radaelli, F.; Spada, C.; Benamouzig, R.; Bisschops, R.; Bretthauer, M.; Dekker, E.; Dinis-Ribeiro, M.; Ferlitsch, M.; et al. Bowel preparation for colonoscopy: European Society of Gastrointestinal Endoscopy (ESGE) Guideline—Update 2019. Endoscopy 2019, 51, 775–794. [Google Scholar] [CrossRef] [Green Version]
- Gandhi, K.; Tofani, C.; Sokach, C.; Patel, D.; Kastenberg, D.; Daskalakis, C. Patient Characteristics Associated With Quality of Colonoscopy Preparation: A Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2018, 16, 357–369. [Google Scholar] [CrossRef]


| Overall (n 1098) | 1L PEG-ASC (n 523) | 2L PEG-ASC (n 204) | 4L PEG (n 371) | p-Value 1L vs. 2L PEG-ASC | p-Value 1L PEG-ASC vs. 4L PEG | |
|---|---|---|---|---|---|---|
| Age (mean, min-max, SD) | 58 (18–91, 16.9) | 57 (18–91, 17.4) | 60 (19–89, 16.4) | 59 (19–90, 16.5) | 0.034 | 0.241 |
| Age < 65 year | 612 (56%) | 301 (58%) | 105 (52%) | 206 (56%) | 0.212 | 0.381 |
| Age ≥ 65 year | 482 (44%) | 219 (44%) | 98 (48%) | 165 (44%) | 0.232 | 0.356 |
| Male | 503 (48%) | 230 (46%) | 103 (54%) | 170 (47%) | 0.051 | 0.618 |
| Smell (median, pctl) | 3.0 (3.0–4.0) | 3.5 (3.0–4.0) | 3.0 (3.0–4.0) | 3.0 (3.0–4.0) | 0.342 | <0.001 |
| Taste (median, pctl) | 3.0 (2.0–4.0) | 3.0 (2.0–4.0) | 3.0 (2.0–4.0) | 3.0 (2.0–3.0) | 0.647 | <0.001 |
| Overall experience (median, pctl) | 4.0 (3.0–4.0) | 4.0 (3.0–4.0) | 4.0 (3.0–4.0) | 3.0 (3.0–4.0) | 0.065 | <0.001 |
| Ingestion of all bowel preparation | 978 (90%) | 474 (91%) | 195 (96%) | 312 (85%) | 0.037 | 0.003 |
| ≥1L additional fluids | 691 (63%) | 371 (71%) | 164 (81%) | 159 (43%) | 0.009 | <0.001 |
| Nausea | 404 (37%) | 223 (43%) | 45 (22%) | 136 (37%) | <0.001 | 0.059 |
| Vomiting | 92 (8%) | 60 (12%) | 8 (4%) | 11 (5%) | 0.002 | 0.011 |
| BBPS Right (mean, SD) | 2.6 (0.6) | 2.7 (0.5) | 2.4 (0.7) | 2.6 (0.6) | <0.001 | <0.001 |
| BBPS Transverse (mean, SD) | 2.7 (0.5) | 2.8 (0.5) | 2.5 (0.7) | 2.7 (0.5) | <0.001 | 0.018 |
| BBPS Left (mean, SD) | 2.7 (0.6) | 2.8 (0.5) | 2.5 (0.6) | 2.7 (0.5) | <0.001 | 0.015 |
| BBPS Total (mean, SD) | 7.9 (1.6) | 8.3 (1.5) | 7.3 (2.0) | 7.9 (1.4) | <0.001 | <0.001 |
| BBPS ≥ 6 | 1062 (97%) | 508 (97%) | 193 (95%) | 361 (97%) | 0.100 | 0.877 |
| BBPS = 9 | 642 (61%) | 370 (73%) | 84 (45%) | 188 (53%) | <0.001 | <0.001 |
| BBPS Right = 3 | 692 (66%) | 391 (77%) | 95 (51%) | 206 (58%) | <0.001 | <0.001 |
| Cecal intubation rate | 1020 (94%) | 489 (95%) | 177(90%) | 354 (95%) | 0.024 | 0.576 |
| Incomplete due to inadequate laxation | 21 (1.9) | 11 (2.1%) | 3 (1.5%) | 7 (1.9%) | 0.577 | 0.820 |
| Incomplete due to technical reasons | 21 (1.9) | 8 (1.5%) | 5 (2.5%) | 8 (2.2%) | 0.400 | 0.486 |
| Incomplete due to other reasons | 19 (1.7) | 5 (1.0%) | 12 (5.9%) | 2 (0.5%) | <0.001 | 0.486 |
| (A) | ||||
|---|---|---|---|---|
| Univariate | Multivariate | |||
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Age ≥ 65 | 0.34 (0.16–0.69) | 0.003 | 0.36 (0.17–0.75) | 0.006 |
| Gender (male) | 1.57 (0.78–3.15) | 0.206 | 0.61 (0.30–1.23) | 0.166 |
| 1L PEG-ASC | Ref | Ref | ||
| 2L PEG-ASC | 0.52 (0.23–1.15) | 0.105 | 0.51 (0.23–1.14) | 0.099 |
| 4L PEG | 1.07 (0.47–2.4) | 0.877 | 1.20 (0.52–2.80) | 0.667 |
| (B) | ||||
| Univariate | Multivariate | |||
| OR (95% CI) | p-Value | OR (95% CI) | OR (95% CI) | |
| Age ≥ 65 | 0.73 (0.57–0.93) | 0.012 | 0.74 (0.57–0.97) | 0.027 |
| Gender (male) | 1.18 (0.92–1.53) | 0.192 | 1.13 (0.87–1.47) | 0.351 |
| 1L PEG-ASC | Ref | Ref | ||
| 2L PEG-ASC | 0.30 (0.21–0.42) | <0.001 | 0.31 (0.22–0.44) | <0.001 |
| 4L PEG | 0.41 (0.31–0.54) | <0.001 | 0.42 (0.31–0.56) | <0.001 |
| (C) | ||||
| Univariate | Multivariate | |||
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Age ≥ 65 | 0.74 (0.58–0.96) | 0.024 | 0.77 (0.59–1.01) | 0.057 |
| Gender (male) | 1.14 (0.88–1.48) | 0.311 | 1.10 (0.83–1.42) | 0.541 |
| 1L PEG-ASC | Ref | Ref | ||
| 2L PEG-ASC | 0.30 (0.21–0.43) | <0.001 | 0.31 (0.22–0.45) | <0.001 |
| 4L PEG | 0.41 (0.30–0.54) | <0.001 | 0.41 (0.30–0.55) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bednarska, O.; Nyhlin, N.; Schmidt, P.T.; Johansson, G.W.; Toth, E.; Lindfors, P. The Effectiveness and Tolerability of a Very Low-Volume Bowel Preparation for Colonoscopy Compared to Low and High-Volume Polyethylene Glycol-Solutions in the Real-Life Setting. Diagnostics 2022, 12, 1155. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12051155
Bednarska O, Nyhlin N, Schmidt PT, Johansson GW, Toth E, Lindfors P. The Effectiveness and Tolerability of a Very Low-Volume Bowel Preparation for Colonoscopy Compared to Low and High-Volume Polyethylene Glycol-Solutions in the Real-Life Setting. Diagnostics. 2022; 12(5):1155. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12051155
Chicago/Turabian StyleBednarska, Olga, Nils Nyhlin, Peter Thelin Schmidt, Gabriele Wurm Johansson, Ervin Toth, and Perjohan Lindfors. 2022. "The Effectiveness and Tolerability of a Very Low-Volume Bowel Preparation for Colonoscopy Compared to Low and High-Volume Polyethylene Glycol-Solutions in the Real-Life Setting" Diagnostics 12, no. 5: 1155. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12051155