
Hepatocellular Carcinoma with Gastrointestinal Involvement: A Systematic Review

 ,
,  ,
,
Abstract
:1. Introduction
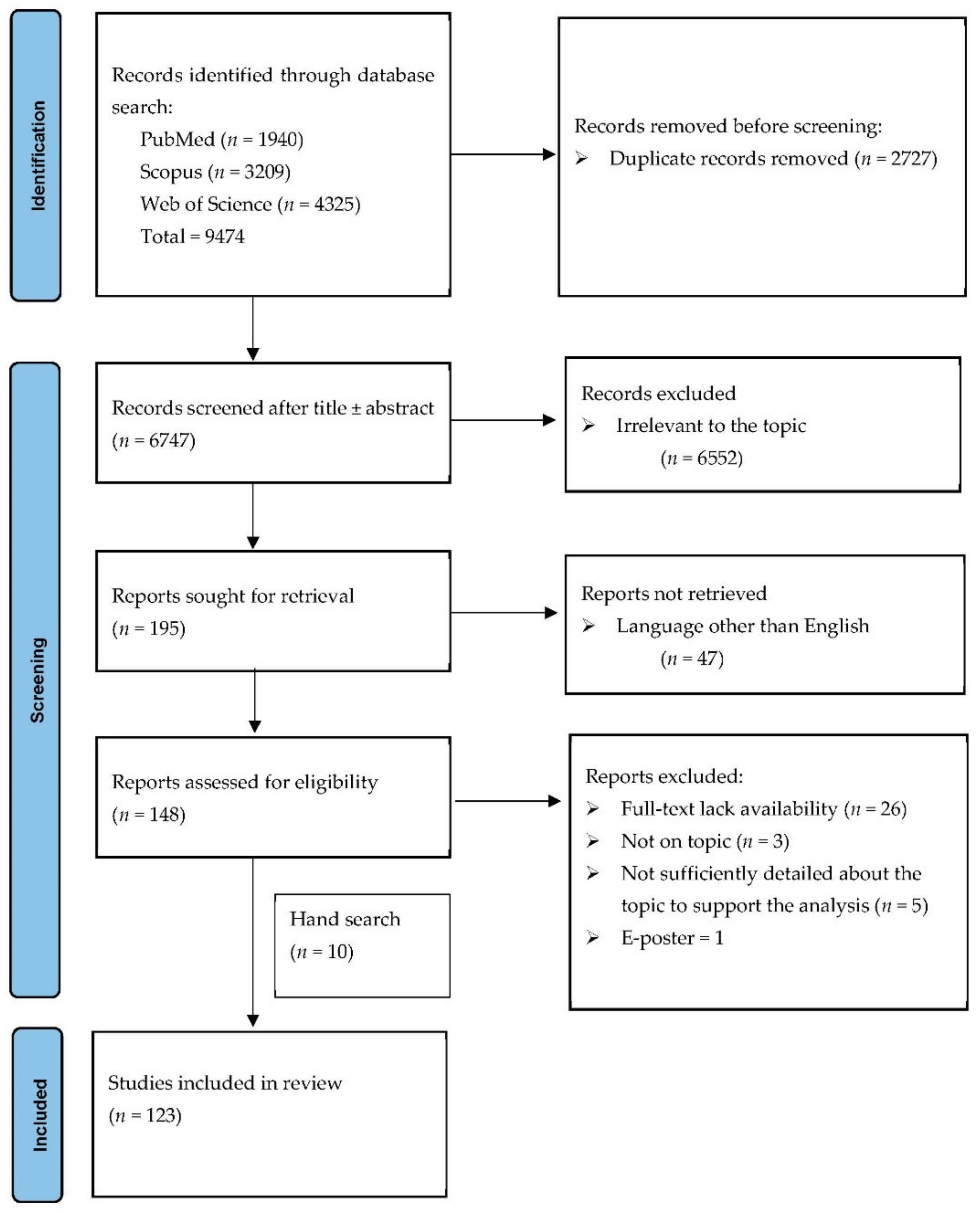
2. Materials and Methods
2.1. Data Sources
2.2. Inclusion and Exclusion Criteria
2.3. Search Strategy
3. Results
3.1. Publication Characteristics
3.2. Patient Characteristics
3.3. Etiology
3.4. Clinical Findings in the Study Population
3.5. Previous Treatment for Hepatocellular Carcinoma
3.6. Involved GI Site and Presumed Mode of Involvement
3.7. Clinical Presentation
3.8. Diagnosis of GI Lesions
3.9. Prognosis of Gastrointestinal Involvement in Patients with HCC
4. Discussion
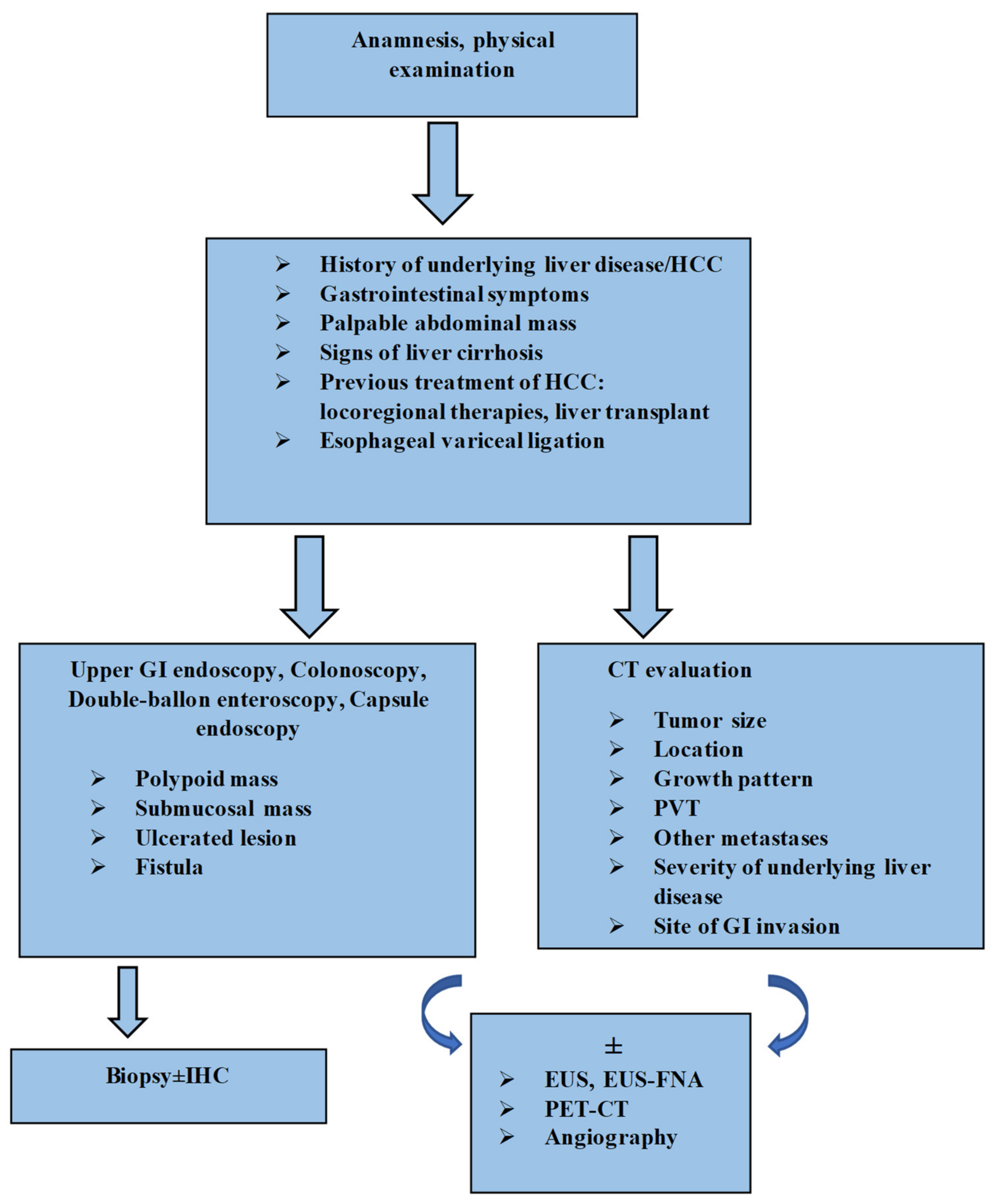
Algorithm of Diagnosis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Terada, T.; Maruo, H. Unusual extrahepatic metastatic sites from hepatocellular carcinoma. Int. J. Clin. Exp. Pathol. 2013, 6, 816–820. [Google Scholar] [PubMed]
- Sawabe, M.; Nakamura, T.; Kanno, J.; Kasuga, T. Analysis of morphological factors of hepatocellular carcinoma in 98 autopsy cases with respect to pulmonary metastasis. Pathol. Int. 1987, 37, 1389–1404. [Google Scholar] [CrossRef] [PubMed]
- Katyal, S.; Oliver, J.H., 3rd; Peterson, M.S.; Ferris, J.V.; Carr, B.S.; Baron, R.L. Extrahepatic metastases of hepatocellular carcinoma. Radiology 2000, 216, 698–703. [Google Scholar] [CrossRef]
- Natsuizaka, M.; Omura, T.; Akaike, T.; Kuwata, Y.; Yamazaki, K.; Sato, T.; Karino, Y.; Toyota, J.; Suga, T.; Asaka, M. Clinical features of hepatocellular carcinoma with extrahepatic metastases. J. Gastroenterol. Hepatol. 2005, 20, 1781–1787. [Google Scholar] [CrossRef]
- Chen, L.-T.; Chen, C.-Y.; Jan, C.-M.; Wang, W.-M.; Lan, T.-S.; Hsieh, M.-Y.; Liu, G.-C. Gastrointestinal Tract Involvement in Hepatocellular Carcinoma: Clinical, Radiological and Endoscopic Studies. Endoscopy 1990, 22, 118–123. [Google Scholar] [CrossRef]
- Lin, C.; Cheng, J.; Lai, K.; Lo, G.; Hsu, P.; Chan, H.; Hsu, J.; Wang, Y.; Pan, H.; Tseng, H. Gastrointestinal metastasis in hepatocellular carcinoma: Radiological and endoscopic studies of 11 cases. J. Gastroenterol. Hepatol. 2000, 15, 536–541. [Google Scholar] [CrossRef]
- Park, M.-S.; Kim, K.W.; Yu, J.-S.; Kim, M.-J.; Yoon, S.-W.; Chung, K.-W.; Lee, J.T.; Yoo, H.S. Radiologic Findings of Gastrointestinal Tract Involvement in Hepatocellular Carcinoma. J. Comput. Assist. Tomogr. 2002, 26, 95–101. [Google Scholar] [CrossRef]
- Fujii, K.; Nagino, M.; Kamiya, J.; Uesaka, K.; Sano, T.; Yuasa, N.; Oda, K.; Nimura, Y. Complete resection of hepatocellular carcinoma with direct invasion to the stomach remnant. J. Hepatobiliary Pancreat. Surg. 2004, 11, 441–444. [Google Scholar] [CrossRef]
- Lin, T.-L.; Yap, A.Q.; Wang, J.-H.; Chen, C.-L.; Iyer, S.G.; Low, J.-K.; Lin, C.-C.; Li, W.-F.; Chen, T.-Y.; Bora, D.; et al. Long term survival in patients with hepatocellular carcinoma directly invading the gastrointestinal tract: Case reports and literature review. Surg. Oncol. 2011, 20, e207–e214. [Google Scholar] [CrossRef]
- Kato, Y.; Matsubara, K.; Akiyama, Y.; Hattori, H.; Hirata, A.; Yamamoto, T.; Suzuki, F.; Ohtaka, H.; Sugiura, Y.; Kitajima, M. Direct biliopancreatoduodenal invasion by hepatocellular carcinoma: Report of the first resected case and review of the literature. Int. J. Clin. Oncol. 2010, 16, 421–427. [Google Scholar] [CrossRef] [PubMed]
- Harada, J.-I.; Matsutani, T.; Hagiwara, N.; Kawano, Y.; Matsuda, A.; Taniai, N.; Nomura, T.; Uchida, E. Metastasis of Hepatocellular Carcinoma to the Esophagus: Case Report and Review. Case Rep. Surg. 2018, 2018, 8685371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, Y.-M.; Cao, Y.-S.; Wu, Z.; Huang, R.; Shen, Z.-L. Colon metastasis from hepatocellular carcinoma: A case report and literature review. World J. Surg. Oncol. 2020, 18, 189. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Mu, M.; Liang, P.; Yu, X.; Cheng, Z. Colonic metastasis from hepatocellular carcinoma after treated by ablation and transarterial chemoembolization manifested by intestinal obstruction: A case report and review of the literature. J. Cancer Res. Ther. 2021, 17, 814–817. [Google Scholar] [CrossRef] [PubMed]
- Ding, J.; Wen, Z. Survival improvement and prognosis for hepatocellular carcinoma: Analysis of the SEER database. BMC Cancer 2021, 21, 1157. [Google Scholar] [CrossRef]
- Hashimoto, M.; Watanabe, G.; Matsuda, M.; Yamamoto, T.; Tsutsumi, K.; Tsurumaru, M. Case Report: Gastrointestinal bleeding from a hepatocellular carcinoma invading the transverse colon. J. Gastroenterol. Hepatol. 1996, 11, 765–767. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 88, 105906. [Google Scholar] [CrossRef]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetc, R.; Currie, M.; Lisy, K.; Qureshi, R.; Mattis, P.; et al. Chapter 7: Systematic reviews of etiology and risk. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020; Available online: https://synthesismanual.jbi.global (accessed on 22 December 2021).
- Sohn, D.; Valensi, Q.; Bryk, D. Hepatoma metastasizing to the esophagus. JAMA 1965, 194, 910–912. [Google Scholar] [CrossRef]
- Hiraoka, T.; Iwai, K.; Yamashita, R.; Tada, I.; Miyauchi, Y. Metastases from hepatocellular carcinoma in sclerosed oesophageal varices in cirrhotic patients. Br. J. Surg. 1986, 73, 932. [Google Scholar] [CrossRef]
- Kume, K.; Murata, I.; Yoshikawa, I.; Kanagawa, K.; Otsuki, M. Polypoid Metastatic Hepatocellular Carcinoma of the Esophagus Occurring After Endoscopic Variceal Band Ligation. Endoscopy 2000, 32, 419–421. [Google Scholar] [CrossRef]
- Sohara, N.; Takagi, H.; Yamada, T.; Ichikawa, T.; Abe, T.; Itoh, H.; Mori, M. Esophageal metastasis of hepatocellular carcinoma. Gastrointest. Endosc. 2000, 51, 739–741. [Google Scholar] [CrossRef] [PubMed]
- Tsubouchi, E.; Hirasaki, S.; Kataoka, J.; Hidaka, S.; Kajiwara, T.; Yamauchi, Y.; Masumoto, T.; Hyodo, I. Unusual Metastasis of Hepatocellular Carcinoma to the Esophagus. Intern. Med. 2005, 44, 444–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yan, S.-L.; Hung, Y.-H.; Yang, T.-H. Metastatic hepatocellular carcinoma of the esophagus: An unusual cause of upper gastrointestinal bleeding. Endoscopy 2007, 39, E257–E258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, L.-Y.; Fan, M.; Fan, J.; Wang, J.; Xu, X.-L.; Jiang, G.-L. Metastatic hepatocellular carcinoma in the esophagus following liver transplantation. Liver Transplant. 2008, 14, 1680–1682. [Google Scholar] [CrossRef]
- Choi, C.S.; Kim, H.C.; Kim, T.H.; Seo, G.S.; Kim, K.H.; Cho, E.Y.; Seo, S.O.; Oh, H.J.; Choi, S.C. Does the endoscopic finding of esophageal metastatic hepatocellular carcinoma progress from submucosal mass to polypoid shape? Gastrointest. Endosc. 2008, 68, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Hsu, K.-F.; Hsieh, T.-Y.; Yeh, C.-L.; Shih, M.-L.; Hsieh, C.-B. Polypoid esophageal and gastric metastases of recurrent hepatocellular carcinoma after liver transplantation. Endoscopy 2009, 41, E82–E83. [Google Scholar] [CrossRef] [Green Version]
- Kahn, J.; Kniepeiss, D.; Langner, C.; Wagner, D.; Iberer, F.; Tscheliessnigg, K. Oesophageal metastases of hepatocellular carcinoma after liver transplantation. Transpl. Int. 2010, 23, 438–439. [Google Scholar] [CrossRef]
- Boonnuch, W.; Akaraviputh, T.; Nino, C.; Yiengpruksawan, A.; Christiano, A.A. Successful treatment of esophageal metastasis from hepatocellular carcinoma using the da Vinci robotic surgical system. World J. Gastrointest. Surg. 2011, 3, 82–85. [Google Scholar] [CrossRef]
- Škurla, B.; Mlinarić, A.; Nadalin, S.; Katičić, M.; Naumovski-Mihalić, S. Esophageal metastases of hepatocellular carcinoma following liver transplantation. Int. J. Case Rep. Images 2010, 1, 7–11. [Google Scholar] [CrossRef]
- Fukatsu, H.; Miura, S.; Kishida, H.; Takagi, S.; Morishita, H.; Uchino, K.; Fujisawa, M. Gastrointestinal: Esophageal metastasis from hepatocellular carcinoma. J. Gastroenterol. Hepatol. 2012, 27, 1536. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.-X.; Jeng, L.-B.; Lin, Y.-S.; Lu, T.-Y.; Kao, P.-Y.; Fang, H.-Y. A Mimicking Esophageal Cancer After Liver Transplant for Hepatocellular Carcinoma: A Rare Posttransplant Metastasis. Exp. Clin. Transplant. 2016, 14, 571–574. [Google Scholar] [CrossRef] [PubMed]
- Kongkam, P. Esophageal Metastatic Sub-mucosal Lesion of Hepatocellular Carcinoma Diagnosed by EUS. Gastroenterol. Hepatol. Open Access 2018, 9, 282. [Google Scholar] [CrossRef] [Green Version]
- Bonboire, R.; Miscu, C.; Yengue, P.; Maes, B.; Patris, A.; Gallez, J.-F. Gastrointestinal tract involvement in hepatocellular carcinoma: Two cases illustrating duodenal and oesophageal invasion. Acta Gastro Enterol. Belg. 2021, 84, 656–658. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, S.K.; Bhakta, D.; Thosani, N.; Ertan, A. Hepatocellular carcinoma masquerading as nodular Barrett’s esophagus. Gastrointest. Endosc. 2021, 93, 1182–1183. [Google Scholar] [CrossRef]
- Shiota, T.; Watanabe, A.; Mitani, K.; Ito, T.; Tobe, K.; Nagashima, H. Long-term survival in a case of hepatocellular carcinoma. Acta Med. Okayama 1983, 37, 73–78. [Google Scholar]
- Makino, H.; Takazakura, E.; Nakamura, S.; Kobayashi, K.; Hattori, N.; Nonomura, A.; Ohta, G. Hepatocellular carcinoma with metastatic gastric cancer simulating Borrmann type 2 and hyper-lipidemia. Acta Pathol. Jpn. 1986, 36, 577–586. [Google Scholar]
- De Nardi, P.; Braga, M.; Zerbi, A.; Sassi, I.; Mangili, F.; Cristallo, M.; Di Carlo, V. Bleeding Gastric Polyposis-Like Metastases of Hepatocellular Carcinoma. Dig. Surg. 1992, 9, 105–108. [Google Scholar] [CrossRef]
- Nicoll, A.J.; Ireton, H.J.C.; Crotty, B. Gastrointestinal bleeding from hepatocellular carcinoma invading the stomach. J. Gastroenterol. Hepatol. 1994, 9, 533–535. [Google Scholar] [CrossRef]
- Maruyama, A.; Murabayashi, K.; Hayashi, M.; Nakano, H.; Isaji, S.; Uehara, S.; Kusuda, T.; Miyahara, S.; Kondo, A.; Nakano, H.; et al. Hepatocellular carcinoma complicated by gastrointestinal hemorrhage caused by direct tumor invasion of stomach. J. Hepato-Biliary Pancreat. Surg. 1999, 6, 90–93. [Google Scholar] [CrossRef]
- Srivastava, D.N.; Gandhi, D.; Julka, P.K.; Tandon, R.K. Gastrointestinal hemorrhage in hepatocellular carcinoma: Management with transhepatic arterioembolization. Abdom. Imaging 2000, 25, 380–384. [Google Scholar] [CrossRef]
- Wang, M.-H.; Wu, M.-S.; Wang, H.-P.; Change, Y.-L.; Lin, J.-T. Endoscopic manifestations of metastatic hepatocellular carcinoma to the stomach: Report of two cases. Gastrointest. Endosc. 2000, 52, 273–275. [Google Scholar] [CrossRef] [PubMed]
- Inoue, H.; Sawada, Y.; Ochiai, K.; Honda, H.; Murayama, J.; Kudo, Y.; Nakashima, Y.; Sagihara, N.; Miyatani, H.; Nakamura, I.; et al. Hepatocellular Carcinoma with Direct Invasion to the Stomach. Intern. Med. 2007, 46, 845–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ong, J.C.; Chow, P.K.; Chan, W.-H.; Chung, A.Y.; Thng, C.H.; Wong, W.-K. Hepatocellular carcinoma masquerading as a bleeding gastric ulcer: A case report and a review of the surgical management. World J. Gastroenterol. 2007, 13, 4523–4525. [Google Scholar] [CrossRef] [PubMed]
- Kimura, K.; Miura, H.; Saito, S.; Suzaki, A.; Kondo, K.; Hamada, T.; Kitamura, S.; Yamada, H. Hepatocellular Carcinoma with Direct Invasion to the Stomach Causing Gastrointestinal Hemorrhage. Intern. Med. 2008, 47, 671–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korkolis, D.P.; Aggeli, C.; Plataniotis, G.D.; Gontikakis, E.; Zerbinis, H.; Papantoniou, N.; Xinopoulos, D.; Apostolikas, N.; Vassilopoulos, P.P. Successful en bloc resection of primary hepatocellular carcinoma directly invading the stomach and pancreas. World J. Gastroenterol. 2009, 15, 1134–1137. [Google Scholar] [CrossRef] [PubMed]
- Hu, M.-L.; Tai, W.-C.; Chuah, S.-K.; Chiu, Y.-C.; Wu, K.-L.; Chou, Y.-P.; Kuo, C.-M.; Hu, T.-H.; Chiu, K.-W. Gastric metastasis of hepatocellular carcinoma via a possible existing retrograde hematogenous pathway. J. Gastroenterol. Hepatol. 2010, 25, 408–412. [Google Scholar] [CrossRef]
- Park, H.; Kim, S.U.; Choi, J.; Park, J.Y.; Ahn, S.H.; Han, K.-H.; Chon, C.Y.; Park, Y.N.; Kim, Y. Hepatogastric fistula caused by direct invasion of hepatocellular carcinoma after transarterial chemoembolization and radiotherapy. Korean J. Hepatol. 2010, 16, 401–404. [Google Scholar] [CrossRef]
- Tan, W.J.; Chia, C.S.; Ong, H.S. A rare cause of gastrointestinal haemorrhage: Gastric invasion by hepatocellular carcinoma. J. Surg. Case Rep. 2013, 2013, rjs050. [Google Scholar] [CrossRef] [Green Version]
- Sayana, H.; Yousef, O.; Clarkston, W.K. Massive upper gastrointestinal hemorrhage due to invasive hepatocellular carcinoma and hepato-gastric fistula. World J. Gastroenterol. 2013, 19, 7472–7475. [Google Scholar] [CrossRef]
- Okay, E.; Sarı, A.; Odabasioglu, H.; Uygun, K.; Sarisoy, T.; Gürbüz, Y.; Sari, A.; Uygun, K. Hepatocellular carcinoma presenting as a huge intra-abdominal mass: A case report. Turk. J. Gastroenterol. 2014, 25, 330–332. [Google Scholar] [CrossRef] [Green Version]
- Inagaki, Y.; Shiraki, K.; Takei, Y. Gastric Metastasis of Hepatocellular Carcinoma Presenting as Hematemesis. Clin. Gastroenterol. Hepatol. 2014, 12, A16–A17. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.-D.; Wu, J.; Yang, H.-G.; Chen, Y.; Zhang, C.-W.; Zhao, D.-J.; Hu, Z.-M. Rare cause of upper gastrointestinal bleeding owing to hepatic cancer invasion: A case report. World J. Gastroenterol. 2014, 20, 12704–12708. [Google Scholar] [CrossRef] [PubMed]
- Grover, I.; Ahmad, N.; Googe, A.B. Hepatogastric fistula following transcatheter arterial chemoembolization of hepatocellular carcino-ma. Case Rep. Gastroenterol. 2014, 8, 286–290. [Google Scholar] [CrossRef]
- Li, L.; Zhang, W.; Meng, F.; Ma, X.; Shen, L.; Jin, B.; Li, H.; Han, J.; Zhou, G.; Liu, S. Gastric Metastasis of Hepatocellular Carcinoma with Gastrointestinal Bleeding After Liver Transplant: A Case Report. Transplant. Proc. 2015, 47, 2544–2547. [Google Scholar] [CrossRef] [PubMed]
- Hot, S.; Yeşiltaş, M.; Gökçek, B.; Eğin, S.; Şengiz, S. Massive and life-threatening upper gastrointestinal bleeding due to invasive hepatocellular carcinoma: A case report. Int. J. Surg. Case Rep. 2016, 26, 69–72. [Google Scholar] [CrossRef] [Green Version]
- Haruki, K.; Misawa, T.; Gocho, T.; Saito, R.; Shiba, H.; Akiba, T.; Yanaga, K. Hepatocellular carcinoma with gastric metastasis treated by simultaneous hepatic and gastric resection: Report of a case. Clin. J. Gastroenterol. 2016, 9, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.; Wei, S.; Liu, B.; Wu, X.; Feng, Y.; Luo, C.; Ju, Y.; Liang, J. Effect of immune suppression on metastasis in a patient with hepatocellular carcinoma metastasized to the colon and stomach: A case report. Exp. Ther. Med. 2016, 11, 1741–1747. [Google Scholar] [CrossRef] [Green Version]
- Hakim, M.S.A.; Azmi, A.N.; Jayalakshmi, P.; Mahadeva, S. Gastric Metastasis from Hepatocellular Carcinoma: A Rare Manifestation. J. Gastrointest. Cancer 2017, 49, 346–348. [Google Scholar] [CrossRef]
- Xiao, W.; Peng, L.; Yu, K.; Li, Y. Gastric metastasis of recurrent hepatocellular carcinoma: A case report and literature review. J. Cancer Res. Ther. 2018, 14, S1230–S1232. [Google Scholar] [CrossRef] [PubMed]
- Kasi, M.; Rashid, S.; Wallace, S.A.J.; Sujendran, V.; Griffiths, B.; Butler, A.; Gibbs, P.; Sreedharan, L.; Zaitoun, A.M.; Venkatachalapathy, S.; et al. Seeding of hepatocellular carcinoma into the stomach wall following endoscopic ultrasound and fine-needle aspiration biopsy. Oxf. Med. Case Rep. 2018, 2018, omy039. [Google Scholar] [CrossRef]
- Sakumura, M.; Tajiri, K.; Sugiyama, T. Gastric Metastasis of Hepatocellular Carcinoma Mimicking Early Gastric Cancer. Clin. Gastroenterol. Hepatol. 2018, 16, e99–e100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bale, A.; Shetty, S.; Shetty, A.; Balaraju, G.; Pai, C.G. Upper Gastrointestinal Bleed Due to Invasive Hepatocellular Carcinoma and Hepato-Gastric Fistula. J. Clin. Exp. Hepatol. 2018, 8, 104–105. [Google Scholar] [CrossRef]
- Imai, M.; Ishikawa, T.; Okoshi, M.; Tomiyoshi, K.; Kojima, Y.; Horigome, R.; Nozawa, Y.; Sano, T.; Iwanaga, A.; Honma, T.; et al. Hemorrhagic Gastric Metastasis from Hepatocellular Carcinoma Successfully Treated Using Coil Embolization of the Left Gastric Artery. Intern. Med. 2019, 58, 2179–2183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Da Costa, P.M.; Luis, R.; Lopes, J. Hepatocellular Carcinoma Invading the Gastric Antrum. Clin. Gastroenterol. Hepatol. 2018, 17, e102–e103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, R.; Song, J.; Kim, S.B. Concurrent hepatocellular carcinoma metastasis to stomach, colon, and brain: A case report. World J. Clin. Cases 2020, 8, 3534–3541. [Google Scholar] [CrossRef] [PubMed]
- Abouzied, M.M.; Fathala, A.; AlMuhaideb, A.; Almanea, H.; Al-Sugair, A.S.; AlSkaff, R.; Al-Qahtani, M.H. Gastric wall metastases from hepatocellular carcinoma: Case report and review of the literature. Radiol. Case Rep. 2020, 16, 550–554. [Google Scholar] [CrossRef]
- Eskarous, H.; Patel, D.; Geme, B.; Krishnamurthy, M. Hepatocellular Carcinoma with Gastric Metastasis. ACG Case Rep. J. 2022, 9, e00750. [Google Scholar] [CrossRef]
- Arima, K.; Suga, M.; Ikeda, N.; Takahashi, T.; Nakata, M.; Shibata, K.; Kobayashi, T.; Yabana, T.; Yachi, A.; Wakabayashi, J. Hepatocellular Carcinoma with Metastasis to the Duodenum: A Case Report. Dig. Endosc. 1992, 4, 62–67. [Google Scholar] [CrossRef]
- Moriura, S.; Ikeda, S.; Ikezawa, T.; Naiki, K.; Sakai, T.; Yokochi, K.; Kuroda, M. Hepatocellular Carcinoma Invading the Duodenum: Combined Resection of the Lateral Duodenum and Repair with a Pedicled Gastric Flap. Dig. Surg. 1995, 12, 136–139. [Google Scholar] [CrossRef]
- Okusaka, T.; Okada, S.; Ishii, H.; Nagahama, H.; Yoshimori, M.; Yamasaki, S.; Takayasu, K.; Kakizoe, T.; Ochiai, A.; Shimoda, T. Hepatocellular Carcinoma With Gastrointestional Hemorrhage Caused by Direct Tumor Invasion to the Duodenum. Jpn. J. Clin. Oncol. 1997, 27, 343–345. [Google Scholar] [CrossRef] [Green Version]
- Hung, H.-C.; Huang, Y.-S.; Lin, C.-C.; Chao, Y.; Chi, K.-H.; Yen, S.-H.; Chang, F.-Y. CASE REPORT: Radiotherapy in the treatment of duodenal bleeding due to hepatocellular carcinoma invasion. J. Gastroenterol. Hepatol. 1998, 13, 1143–1145. [Google Scholar] [CrossRef] [PubMed]
- Farrell, R.; Morrin, M.; Lewis, D.; Chuttani, R.; Pleskow, D. EUS features of duodenal invasion secondary to hepatocellular carcinoma: Case report. Gastrointest. Endosc. 1999, 49, 384–387. [Google Scholar] [CrossRef]
- Del Natale, M.; Druez, P.; Brenard, R. Fistulization of a hepatocellular carcinoma into the duodenum. J. Hepatol. 2001, 34, 172. [Google Scholar] [CrossRef]
- Cho, A.; Ryu, M.; Ochiai, T. Successful resection, using pancreas-sparing duodenectomy, of extrahepatically growing hepatocellular carcinoma associated with direct duodenal invasion. J. Hepato-Biliary-Pancreat. Surg. 2002, 9, 393–396. [Google Scholar] [CrossRef] [PubMed]
- Ohnishi, S.; Hatanaka, K.; Nakanishi, M.; Hige, S.; Asaka, M. Massive Invasion of Hepatocellular Carcinoma to the Duodenum: Successful Treatment of Gastrointestinal Haemorrhage with Transcatheter Arterial Embolisation. Clin. Oncol. 2004, 16, 157. [Google Scholar] [CrossRef] [PubMed]
- Uehara, K.; Hasegawa, H.; Ogiso, S.; Sakamoto, E.; Ohira, S.; Igami, T.; Mori, T. Skip lymph node metastases from a small hepatocellular carcinoma with difficulty in preoperative diagnosis. J. Gastroenterol. Hepatol. 2003, 18, 345–349. [Google Scholar] [CrossRef] [PubMed]
- Chung, C.; Al Ali, J.; Owen, D.A.; Weiss, A.A.; Yoshida, E.M.; Tai, I.T. A rare case of isolated duodenal metastases from hepatocellular carcinoma associated with p53 and ki-67 expression: A case report. Cases J. 2009, 2, 9344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurtz, L.E.; Miah, A.R. Infiltrating hepatocellular carcinoma into the duodenum presenting with upper gastrointestinal bleeding. Endoscopy 2009, 41, E308. [Google Scholar] [CrossRef]
- Liang, J.-D.; Chen, C.-H.; Hsu, S.-J.; Sheu, J.-C.; Yang, P.-M.; Lee, H.-S.; Lee, C.-Z.; Huang, G.-T. Hepatocellular carcinoma with duodenal invasion and metastasis. J. Gastroenterol. Hepatol. 2011, 27, 677–683. [Google Scholar] [CrossRef]
- Kim, J.N.; Lee, H.S.; Kim, S.Y.; Kim, J.H.; Jung, S.W.; Koo, J.S.; Yim, H.J.; Lee, S.W.; Choi, J.H.; Kim, C.D.; et al. Endoscopic Treatment of Duodenal Bleeding Caused by Direct Hepatocellular Carcinoma Invasion with an Ethanol Injection. Gut Liver 2012, 6, 122–125. [Google Scholar] [CrossRef]
- Sauer, B.G.; Dustin, S.M.; Caldwell, S.H. Liver Invasion of the Duodenum Due to Hepatocellular Carcinoma. Clin. Gastroenterol. Hepatol. 2012, 10, A25. [Google Scholar] [CrossRef] [PubMed]
- Arima, K.; Chikamoto, A.; Hashimoto, D.; Kaida, T.; Higashi, T.; Taki, K.; Takeyama, H.; Okabe, H.; Nitta, H.; Hayashi, H.; et al. Hepatology: Hepatocellular carcinoma with duodenal metastasis. J. Gastroenterol. Hepatol. 2015, 30, 1115. [Google Scholar] [CrossRef] [PubMed]
- Kashani, A.; Nissen, N.N.; Guindi, M.; Jamil, L.H. Metastatic Periampullary Tumor from Hepatocellular Carcinoma Presenting as Gastrointestinal Bleeding. Case Rep. Gastrointest. Med. 2015, 2015, 732140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, I.-C.; Tai, C.-M.; Tseng, C.-M. Duodenal invasion of hepatocellular carcinoma following transarterial chemoembolization. Dig. Liver Dis. 2018, 50, 618. [Google Scholar] [CrossRef]
- Ito, T.; Hirose, T.; Matsumoto, A.; Yogo, A.; Okuno, T.; Doi, R. Hepatocellular carcinoma with duodenal invasion resected subsequent to multimodal therapies: A case report. Int. J. Surg. Case Rep. 2019, 60, 348–352. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.H.; Lo, E.Y.J.; Lee, K.F.; Chong, C.C.N.; Lai, P.B.-S. An unusual cause of upper gastrointestinal bleeding due to recurrent hepatocellular carcinoma: A case report. Int. J. Surg. Case Rep. 2020, 70, 83–86. [Google Scholar] [CrossRef]
- Wu, Y.-H.; Hsu, W.-F.; Yang, C.-Y.; Chang, K.-P. Gastrointestinal bleeding caused by hepatocellular carcinoma in a rare case of direct invasion to the duodenum. Dig. Liver Dis. 2020, 53, 1201–1202. [Google Scholar] [CrossRef]
- Sawada, K.; Fujiya, M.; Nakajima, S.; Okumura, T. Endoscopic findings of hepatocellular carcinoma invading the duodenum. Jpn. J. Clin. Oncol. 2021, 51, 1689–1690. [Google Scholar] [CrossRef]
- Lee, Y.J.; Kim, J.H.; Song, H.-Y.; Park, J.-H.; Na, H.K.; Kim, P.H.; Fan, Y. Hepatocellular Carcinoma Complicated by Gastroduodenal Obstruction: Palliative Treatment with Metallic Stent Placement. Cardiovasc. Interv. Radiol. 2011, 35, 1129–1135. [Google Scholar] [CrossRef]
- Tsujimoto, M.; Aozasa, K.; Nakajima, Y.; Kariya, M. Hepatocellular carcinoma with sarcomatous proliferation showing an unusual and wide-spread metastasis. Pathol. Int. 1984, 34, 839–845. [Google Scholar] [CrossRef]
- Narita, T.; Nakazawa, H.; Hizawa, Y.; Ishidoya, T.; Kudo, H. Hepatocellular carcinoma with unusual metastasis to the small intestine. Pathol. Int. 1993, 43, 779–782. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, A.; Takeda, R.; Yamamoto, H.; Utsunomiya, H.; Okamura, R.; Kataoka, M.; Mukaihara, S.; Yamaoka, Y. Extrahepatic large hepatocellular carcinoma with peritoneal dissemination: Multimodal treatment, including four surgical operations. J. Hepato-Biliary-Pancreatic Surg. 2000, 7, 339–344. [Google Scholar] [CrossRef] [PubMed]
- Byun, J.R.; Cho, S.H.; Yang, D.H.; Kim, Y.K.; Ju, J.K.; Choi, S.K.; Chung, I.J. Ileovesical Fistula Caused by Hepatocellular Carcinoma. Korean J. Intern. Med. 2005, 20, 76–79. [Google Scholar] [CrossRef]
- Kim, H.S.; Shin, J.W.; Kim, G.Y.; Kim, Y.M.; Cha, H.J.; Jeong, Y.K.; Du Jeong, I.; Bang, S.-J.; Kim, D.H.; Park, N.H. Metastasis of hepatocellular carcinoma to the small bowel manifested by intussusception. World J. Gastroenterol. 2006, 12, 1969–1971. [Google Scholar] [CrossRef]
- Iwaki, K.; Ohta, M.; Ishio, T.; Kai, S.; Iwashita, Y.; Shibata, K.; Himeno, K.; Seike, M.; Fujioka, T.; Kitano, S. Metastasis of hepatocellular carcinoma to spleen and small intestine. J. Hepato-Biliary-Pancreatic Surg. 2008, 15, 213–219. [Google Scholar] [CrossRef]
- Choi, J.-H.; Kim, T.H.; Choi, K.H.; Oh, H.J. Small intestinal perforation caused by metastatic tumor necrosis after sorafenib (Nexavar®) therapy for advanced hepatocellular carcinoma. Int. Cancer Conf. J. 2012, 1, 155–158. [Google Scholar] [CrossRef] [Green Version]
- Kunizaki, M.; Hidaka, S.; Isomoto, H.; Takeshita, H.; Nanashima, A.; Sawai, T.; Yasutake, T.; Nagayasu, T. Diagnosis of small-bowel metastasis of hepatocellular carcinoma by double-balloon enteroscopy. Int. J. Surg. Case Rep. 2012, 3, 263–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Igawa, A.; Oka, S.; Tanaka, S.; Nakano, M.; Aoyama, T.; Watari, I.; Aikata, H.; Arihiro, K.; Chayama, K. Small Bowel Metastasis of Hepatocellular Carcinoma Detected by Capsule Endoscopy. Case Rep. Gastroenterol. 2013, 7, 492–497. [Google Scholar] [CrossRef] [PubMed]
- Kanazawa, M.; Sugaya, T.; Tominaga, K.; Takahashi, F.; Takenaka, K.; Nakano, M.; Hiraishi, H. Jejunal Metastasis from Hepatocellular Carcinoma. Intern Med. 2018, 57, 947–950. [Google Scholar] [CrossRef] [Green Version]
- Shelat, V.G.; Giron, D.M.; Oo, A.M. Acute haemoperitoneum due to small bowel metastases from hepatocellular carcinoma in a long term survivor following previous rupture. Ann. Hepato-Biliary Pancreat. Surg. 2018, 22, 416–418. [Google Scholar] [CrossRef] [Green Version]
- Sun, W.-C.; Tsai, T.-J.; Tsai, W.-L.; Cheng, J.-S.; Chen, W.-C. Metastatic hepatocellular carcinoma of small bowel presenting as GI bleeding. Gastrointest. Endosc. 2018, 88, 774–775. [Google Scholar] [CrossRef] [PubMed]
- Mashiko, T.; Masuoka, Y.; Nakano, A.; Tsuruya, K.; Hirose, S.; Hirabayashi, K.; Kagawa, T.; Nakagohri, T. Intussusception due to hematogenous metastasis of hepatocellular carcinoma to the small intestine: A case report. World J. Gastroenterol. 2020, 26, 6698–6705. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, N.; Tajiri, K.; Futsukaichi, Y.; Tanaka, S.; Murayama, A.; Entani, T.; Kobayashi, S.; Takahashi, K.; Fujii, T.; Imura, J.; et al. Perforation of the Small Intestine after Introduction of Lenvatinib in a Patient with Advanced Hepatocellular Carcinoma. Case Rep. Gastroenterol. 2020, 14, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Fukui, H.; Kashiwagi, T.; Shirai, Y.; Matsuda, Y.; Kawata, S.; Nishimura, T.; Kozuka, T. Metastasis of Hepatocellular Carcinoma to the Colon Demonstrated by Tc-99m PMT Scintigraphy. Clin. Nucl. Med. 1993, 18, 512–515. [Google Scholar] [CrossRef] [PubMed]
- Cosenza, C.A.; Sher, L.S.; Poletti, B.J.; Tschirhart, D.; Noguchi, H.; Hoffman, A.L.; Lopez, R.R.; Lugo, D.; Rojter, S.E.; Makowka, L. Metastasis of hepatocellular carcinoma to the right colon manifested by gastrointestinal bleeding. Am. Surg. 1999, 65, 218–221. [Google Scholar] [PubMed]
- Kurachi, K.; Suzuki, S.; Yokoi, Y.; Okumura, T.; Inaba, K.; Igarashi, T.; Takehara, Y.; Konno, H.; Baba, S.; Nakamura, S. A 5-year survivor after resection of peritoneal metastases from pedunculated-type hepatocellular carcinoma. J. Gastroenterol. 2002, 37, 571–574. [Google Scholar] [CrossRef]
- Zech, C.J.; Bilzer, M.; Mueller-Lisse, U.G.; Steitz, H.O.; Haraida, S.; Reiser, M.F.; Zech, M.C.J. Perforation of the colon: A rare complication of hepatocellular carcinoma. Acta Radiol. 2006, 47, 538–542. [Google Scholar] [CrossRef]
- Tapuria, N.; Sinha, C.K.; Michael, N.; Fisher, P.W. Haematogenous metastasis to ascending colon in a patient with hepatocellular carcinoma and autoimmune hepatitis. Eur. J. Gastroenterol. Hepatol. 2007, 19, 607–609. [Google Scholar] [CrossRef]
- Kaibori, M.; Morita, M.; Tagami, S.; Uchida, Y.; Tanaka, H.; Yoshioka, K.; Takahashi, Y.; Sakaida, N.; Uemura, Y.; Seki, T.; et al. Cutaneous and Colonic Metastases After Resection of Hepatocellular Carcinoma. Am. J. Dig. Dis. 2007, 52, 1114–1117. [Google Scholar] [CrossRef]
- Ng, D.S.C.; Chok, K.S.H.; Law, W.-L.; Collins, R.J.; Fan, S.-T. Long-term survival after resection of extrahepatic recurrence of hepatocellular carcinoma at the right colon. Int. J. Color. Dis. 2007, 22, 1411–1412. [Google Scholar] [CrossRef]
- Hirashita, T.; Ohta, M.; Iwaki, K.; Kai, S.; Shibata, K.; Sasaki, A.; Nakashima, K.; Kitano, S. Direct invasion to the colon by hepatocellular carcinoma: Report of two cases. World J Gastroenterol. 2008, 14, 4583–4585. [Google Scholar] [CrossRef] [PubMed]
- Nozaki, Y.; Kobayashi, N.; Shimamura, T.; Akiyama, T.; Inamori, M.; Iida, H.; Endo, H.; Fujita, K.; Yoneda, M.; Takahashi, H.; et al. Colonic Metastasis from Hepatocellular Carcinoma: Manifested by Gastrointestinal Bleeding. Am. J. Dig. Dis. 2008, 53, 3265–3266. [Google Scholar] [CrossRef] [PubMed]
- Yoo, D.-J.; Chung, Y.-H.; Lee, Y.-S.; Kim, S.E.; Jin, Y.-J.; Lee, Y.M.; Kim, M.-J. Sigmoid colon metastasis from hepatocellular carcinoma. Korean J. Hepatol. 2010, 16, 397–400. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.-F.; Chou, J.-W.; Lai, H.-C. A Rare Cause of Bloody Stools in a 57-Year-Old Woman With Hepatocellular Carcinoma. Gastroenterology 2011, 140, e5–e6. [Google Scholar] [CrossRef]
- Shih, Y.J.; Hsu, K.F.; Yu, J.C.; Chan, D.C.; Hsieh, C.B. Synchronous hepatocellular carcinoma and sigmoid colon metastasis present-ing as liver and intra-abdominal abscesses. Acta Gastroenterol. Belg. 2012, 75, 278–279. [Google Scholar]
- Haga, Y.; Chiba, T.; Ohira, G.; Kanai, F.; Yokota, H.; Motoyama, T.; Ogasawara, S.; Suzuki, E.; Ooka, Y.; Tawada, A.; et al. Simultaneous Resection of Disseminated Hepatocellular Carcinoma and Colon Cancer. Case Rep. Gastroenterol. 2013, 7, 37–43. [Google Scholar] [CrossRef]
- Sun, L.-H.; Han, H.-Q.; Wang, P.-Z.; Tian, W.-J. Emergency caudate lobectomy for ruptured hepatocellular carcinoma with multiple primary cancers. World J. Gastroenterol. 2013, 19, 418–421. [Google Scholar] [CrossRef]
- Ou, T.-M.; Tsai, W.-C.; Hsieh, T.-Y.; Shih, Y.-L. Hepatocellular carcinoma with colonic metastasis. Singap. Med. J. 2014, 55, e93–e95. [Google Scholar] [CrossRef] [Green Version]
- Imada, S.; Noura, S.; Ohue, M.; Shingai, T.; Sueda, T.; Gotoh, K.; Yamada, T.; Tomita, Y.; Yano, M.; Ishikawa, O. Recurrence of hepatocellular carcinoma presenting as an asymptomatic appendiceal tumor: Report of a case. Surg. Today 2012, 43, 685–689. [Google Scholar] [CrossRef]
- Kohli, R.; Purysko, A.S.; John, B.V. Hematochezia From Metastasis of Hepatocellular Carcinoma to Colon in a Patient Who Underwent Liver Transplantation. Clin. Gastroenterol. Hepatol. 2014, 12, A23–A24. [Google Scholar] [CrossRef]
- Zhu, X.; Lou, Z.; He, J.; Sui, J.; Ma, J.; Gong, H.; Zhang, W. Hematogenous transverse colon metastasis from primary hepatocellular carcinoma. Int. J. Color. Dis. 2015, 31, 1241–1242. [Google Scholar] [CrossRef] [PubMed]
- Mitsialis, V.; Lee, L.S. Metastasis of Hepatocellular carcinoma to Distal colon Associated With Inferior Mesenteric Arteriovenous Fistula and Tumor Thrombus: A case Report. Am. J. Gastroenterol. 2018, 113, 916–918. [Google Scholar] [CrossRef] [PubMed]
- Repullo, D.; Diaz, M.; Holbrechts, S.; Gomez-Galdon, M.; Van Gestel, D.; Bohlok, A.; Liberale, G.; Donckier, V. Unusual presentation of a hepatocellular carcinoma as a potential late side effect of radiotherapy in a patient treated for Wilms tumor in childhood. World J. Surg. Oncol. 2018, 16, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tagliabue, F.; Burati, M.; Chiarelli, M.; Marando, A.; De Simone, M.; Cioffi, U. Left colonic metastasis from primary hepatocellular carcinoma: A case report. World J. Clin. Cases 2019, 7, 2044–2048. [Google Scholar] [CrossRef] [PubMed]
- Van Pham, B.; Phan, H.H.; Le Ngo, L.; Nguyen, H.T.T.; Van Le, K.; Dinh, T.C.; Bac, N.D.; Toi, C.D. A Rare Colonic Metastasis Case from Hepatocellular Carcinoma. Open Access Maced. J. Med Sci. 2019, 7, 4368–4371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soni, A.; Malhi, N.S. Lower Gastrointestinal Bleeding: Liver Rams into Gut! GE-Port. J. Gastroenterol. 2018, 26, 218–220. [Google Scholar] [CrossRef] [Green Version]
- Miyauchi, W.; Yamamoto, M.; Masahiro, M.; Shishido, Y.; Miyatani, K.; Matsunaga, T.; Sakamoto, T.; Fujiwara, Y. Colonic metastasis of hepatocellular carcinoma with repeated retroperitoneal bleeding: A case report. Surg. Case Rep. 2021, 7, 261. [Google Scholar] [CrossRef]
- Liu, K.-W.; Chen, H.-P.; Yang, C.-H. Rectal metastasis following radiofrequency ablation for hepatocellular carcinoma. Formos. J. Surg. 2013, 46, 140–143. [Google Scholar] [CrossRef] [Green Version]
- Nielsen, J.A.; Putcha, R.V.; Roberts, C.A. The increasing incidence of remote metastasis: A case report of metastatic hepatocellular carcinoma to the rectosigmoid. Tumori J. 2014, 100, e31–e34. [Google Scholar] [CrossRef]
- Ikeda, A.; Nagayama, S.; Yamamoto, N.; Akiyoshi, T.; Konishi, T.; Fujimoto, Y.; Fukunaga, Y.; Ishikawa, Y.; Ueno, M. A rare case of hepatocellular carcinoma metastasizing hematogenously to the rectum. Int. Cancer Conf. J. 2016, 5, 168–173. [Google Scholar] [CrossRef]
- Pasini, F.; Serenari, M.; Cucchetti, A.; Ercolani, G. Treatment options for recurrence of hepatocellular carcinoma after surgical resection: Review of the literature and current recommendations for management. Hepatoma Res. 2020, 6, 26. [Google Scholar] [CrossRef]
- Cardarelli-Leite, L.; Hadjivassiliou, A.; Klass, D.; Chung, J.; Ho, S.G.F.; Lim, H.J.; Kim, P.T.W.; Mujoomdar, A.; Liu, D.M. Current locore-gional therapies and treatment strategies in hepatocellular carcinoma. Curr. Oncol. 2020, 27 (Suppl. S3), S144–S151. [Google Scholar] [CrossRef] [PubMed]
- Okuda, K.; Moriyama, M.; Yasumoto, M.; Jinnouchi, S.; Shimokawa, Y.; Nakayama, T.; Kanda, Y.; Fukyuama, Y.; Musha, H.; Kuratomi, S.; et al. Roentgenologic demonstration of spontaneous reversal of portal blood flow in cirrhosis and primary carcinoma of the liver. Am. J. Roentgenol. 1973, 119, 419–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Author | Year | Type of Paper | Segment of GI Tract Involved | No. of Patients Reported | Age | Gender | Etiology | Localization of HCC | Dimension of HCC (cm) | Previous Treatment for HCC | PVT | AFP (ng/mL) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sohn, D. et al. [19] | 1965 | Case report | esophagus | 1 | 74 | M | N/A | LHL | 6 | none | yes | N/A |
| Hiraoka, T. et al. [20] | 1986 | Case report | esophageal varices | 2 | 55 | M | N/A | RHL, LHL | 1 | none | yes | N/A |
| esophageal varices | 62 | M | N/A | RHL | N/A | none | yes | N/A | ||||
| Kume, K. et al. [21] | 2000 | Case report | esophagus | 1 | 56 | M | HBV | RHL, LHL | N/A | TACE | yes | 12.200 |
| Sohara, N. et al. [22] | 2000 | Case report | esophagus | 2 | 54 | M | HCV | RHL | N/A | TAI, PEI | yes | 7820 |
| esophagus | 56 | M | UK | RHL | N/A | TAI, external beam radiotherapy | yes | 990 | ||||
| Tsubouchi, E. et al. [23] | 2005 | Case report | esophagus + stomach | 1 | 63 | M | HCV | RHL, LHL | 3; 2 | PEI, IHAC | no | 596.09 |
| Yan, S.L. et al. [24] | 2007 | Editorial material | esophagus | 1 | 53 | M | HBV | LHL | N/A | None | yes | 17.036 |
| Xie, L.Y. et al. [25] | 2008 | Case report | esophagus | 1 | 50 | M | HBV | RHL | N/A | LT, TACE, systemic chemotherapy | yes | N/A |
| Choi, C.S. et al. [26] | 2008 | Case report | esophagus | 1 | 66 | M | UK | RHL, LHL | N/A | TACE, external beam radiotherapy | yes | 3.47 |
| Hsu, K.F. et al. [27] | 2009 | Editorial material | esophagus + gastric cardia | 1 | 54 | M | HBV | N/A | N/A | LT, TACE, systemic chemotherapy | no | N/A |
| Kahn, J. et al. [28] | 2009 | Letter to editor | esophagus | 1 | 55 | M | HCV | RHL, LHL | N/A | LT, TACE | yes | 1426 |
| Boonnuch, W. et al. [29] | 2011 | Case report | esophagus | 1 | 59 | M | N/A | No tumor reccurence | N/A | LT | no | 510 |
| Skurla, B. et al. [30] | 2010 | Case report | esophagus | 1 | 56 | M | alcohol | RHL, LHL | N/A (at the moment of esophageal metastasis diagnosis) | LT | yes | NR |
| Fukatsu, H. et al. [31] | 2012 | Case report | esophagus | 1 | 63 | M | NA | RHL, LHL | N/A | TACE, RFA | yes | N/A |
| Chen, J.X. et al. [32] | 2016 | Case report | esophagus | 1 | 44 | M | alcohol | NA | N/A | LT, TACE | no | 17.62 |
| Harada, J.-i. et al. [12] | 2018 | Case report | esophagus | 1 | 71 | M | HBV | RHL, LHL * | N/A | surgical resection | no | 1800 |
| Kongkam, P. et al. [33] | 2018 | Case report | esophagus | 1 | 59 | M | N/A | NA | N/A | LT | no | 258.3 |
| Boinboire, R. et al. [34] | 2021 | Case report | esophagus | 1 | 66 | M | alcohol | RHL, LHL | N/A | surgical resection, RFA | no | NR |
| Subramanian, S.K. et al. [35] | 2021 | Editorial material | esophagus | 1 | 53 | M | alcohol | No tumor recurrence in the liver | 5; 10 | systemic chemotherapy | no | NR |
| Shiota, T. et al. [36] | 1983 | Case report | stomach | 1 | 56 | M | UK | RHL, LHL | 5; 10 | systemic chemotherapy | no | NR |
| Makino, H. et al. [37] | 1986 | Case report | stomach | 1 | 69 | M | UK | RHL, LHL | N/A | none | yes | 1,136,000 |
| Chen, L.T. et al. [6] | 1990 | Retrospective analysis study | stomach | 3 | 48 | M | HBV | LHL | 17 | surgical resection | UK | N/A |
| 86 | M | UK | RHL, LHL | 25 | none | yes | 221.920 | |||||
| 59 | M | HBV | RHL | 18 | TAE, IHAC | no | 51.270 | |||||
| De Nardi, P. et al. [38] | 1992 | Case report | stomach | 1 | 60 | M | UK | RHL | No tumor recurrence in the liver | surgical resection | yes | 24,000 |
| Nicoll, A.J. et al. [39] | 1994 | Case report | stomach | 1 | 61 | M | UK | N/A | N/A | systemic chemotherapy | no | 6526 |
| Maruyama, A. et al. [40] | 1999 | Case report | stomach | 1 | 65 | M | HCV | RHL, LHL | N/A | TAE, IHAC, radiotherapy | no | NR |
| Srivastava, D.N. et al. [41] | 2000 | Case series | stomach | 1 | 58 | M | HCV | LHL | N/A | N/A | N/A | N/A |
| Wang, M.H. et al. [42] | 2000 | Case report | stomach | 2 | 57 | F | HBV | LHL | N/A | surgical resection, TACE | no | elevated |
| 58 | M | HBV | LHL | N/A | surgical resection | no | N/A | |||||
| Lin, C.P. et al. [7] | 2000 | Retrospective analysis study | stomach | 5 | 53 | M | HCV | RHL, LHL | 9 | none | yes | 719.110 |
| stomach | 66 | M | HBV | LHL | 12 | surgical resection | UK | 1159 | ||||
| stomach | 60 | M | HCV | RHL, LHL | 14 | none | yes | 136.070 | ||||
| stomach | 69 | M | UK | RHL, LHL | 14 | surgical resection, TACE | no | 50 | ||||
| stomach | 63 | M | HBV | RHL, LHL | 9 | none | no | 2432 | ||||
| Fujii, K. et al. [9] | 2004 | Case report | stomach + jejunum | 1 | 61 | M | alcohol | LHL | 10; 2 | none | no | 19.675 |
| Inoue, H. et al. [43] | 2006 | Case report | stomach | 1 | 71 | M | HCV | LHL | 5 | IHAC | yes | 45.630 |
| Ong, J.C.A. et al. [44] | 2007 | Case report | stomach | 1 | 67 | M | HBV | LHL | 10 | none | No | NA |
| Kimura, K. et al. [45] | 2008 | Case report | stomach | 1 | 54 | M | HBV | LHL | 7.5 | TAE | no | NR |
| Korkolis, D.P. et al. [46] | 2009 | Case report | stomach | 1 | 70 | M | HBV | LHL | 15 | none | no | 2.1 |
| Hu, M.L. et al. [47] | 2009 | Retrospective analysis study | stomach | 7 | 48 | M | HBV, alcohol | LHL | 12 | TAE | yes | 969 |
| stomach | 54 | M | HBV | LHL | 6 | TAE | yes | >87.500 | ||||
| stomach | 68 | M | HBV | RHL, LHL | N/A ** | none | yes | 440 | ||||
| stomach | 62 | M | HBV | RHL | 7 | TAE | yes | 2 | ||||
| stomach | 50 | M | HBV + HCV + HDV + alcohol | RHL, LHL | N/A ** | TAE | no | 218 | ||||
| stomach | 51 | M | HBV + alcohol | LHL | 14 | TAE | yes | 6398 | ||||
| stomach | 71 | M | HBV + alcohol | RHL, LHL | 8; 6 | TAE | yes | 34.706 | ||||
| Park, H. et al. [48] | 2010 | Case report | stomach | 1 | 63 | M | HBV | RHL, LHL | 8; 3 | TACE | no | 50.202 |
| Lin, T.L. et al. [10] | 2011 | Case report | stomach | 1 | 57 | M | HBV | LHL | 9 | TAE | no | NA |
| Tan, W.J. et al. [49] | 2013 | Case report | stomach | 1 | 76 | F | cryptogenic liver cirrhosis | NA ** | NA | none | no | >60.500 |
| Sayana, H. et al. [50] | 2013 | Case report | stomach | 1 | 36 | M | HBV + HCV | LHL | 19 | TACE, sorafenib | no | 7.6 |
| Okay, E. et al. [51] | 2014 | Case report | stomach + transverse colon | 1 | 44 | M | HBV | LHL | 28 | none | no | >350.000 |
| Inagaki, Y. et al. [52] | 2014 | Case report-Image of the month | stomach | 1 | 62 | M | HCV | N/A | N/A | TACE, RFA | N/A | 6404 |
| Wu, W.D. et al. [53] | 2014 | Case report | stomach | 1 | 75 | M | HBV | LHL | N/A | surgical resection, TACE | no | NR |
| Grover, I. et al. [54] | 2014 | Case report | stomach | 1 | 51 | M | HBV | LHL | 11.5 | TACE | no | elevated |
| Li, L. et al. [55] | 2015 | Case report | stomach | 1 | 43 | M | HBV | N/A | N/A | LT | no | 191 |
| Hot, S. et al. [56] | 2016 | Case report | stomach | 1 | 62 | M | alcohol | hepatic hilum | 13 | none | no | 2.82 |
| Haruki, K. et al. [57] | 2016 | Case report | stomach | 1 | 73 | M | UK | LHL | 17 | none | no | N/A |
| Wu, D. et al. [58] | 2016 | Case report | stomach + colon | 1 | 54 | M | N/A | RHL | 4 | surgical resection | N/A | N/A |
| Abdul Hakim, M.S. et al. [59] | 2017 | Case report | stomach + duodenum | 1 | 73 | M | N/A | RHL | N/A | RFA | no | 124.800 |
| Peng, L. et al. [60] | 2018 | Case report | stomach | 1 | 22 | M | HBV | RHL, LHL | 8; 1.5 | surgical resection | no | >1200 |
| Kasi, M. et al. [61] | 2018 | Case report | stomach | 1 | 43 | M | HBV | caudate lobe | 3 | LT, TACE | no | 69 |
| Sakumura, M. et al. [62] | 2018 | Editorial material | stomach | 1 | 68 | F | HBV | N/A | N/A | TACE | yes | N/A |
| Bale, A. et al. [63] | 2018 | Editorial material | stomach | 1 | 69 | M | NAFLD | LHL | N/A | TACE | no | N/A |
| Imai, M. et al. [64] | 2019 | Case report | stomach | 1 | 62 | M | alcohol | RHL, LHL | 17; 6 | TACE | yes | 56.388 |
| Marques da Costa, P. et al. [65] | 2019 | Editorial material | stomach + duodenum | 1 | 81 | F | HCV | RHL | N/A | none | no | N/A |
| Kim, R. et al. [66] | 2020 | Case report | stomach + ascending colon | 1 | 75 | M | alcohol | N/A | N/A | surgical resection, TACE | no | NR (2.3) |
| Abouzied, M.M. et al. [67] | 2021 | Case report | stomach | 1 | 69 | M | N/A | RHL | 10 | surgical resection | no | NR (3.3) |
| Eskarous, H. et al. [68] | 2022 | Case report | stomach | 1 | 82 | F | NA | RHL | N/A | surgical resection | N/A | N/A |
| Chen, L.-T. et al. [6] | 1990 | Retrospective analysis study | duodenum | 4 | 56 | M | HBV | RHL | 22 | none | UK | 3200 |
| 56 | M | UK | RHL | 6 | TAE | no | >700 | |||||
| 54 | M | HBV | LHL | 8 | TAE, radiotherapy | yes | 10 | |||||
| 34 | M | HBV | RHL | NA | systemic chemotherapy | UK | 15,435 | |||||
| Arima, K. et al. [69] | 1992 | Case report | duodenum | 1 | 61 | M | NA | RHL | 3 | surgical resection, systemic chemotherapy | yes | N/A |
| Moriura, S. et al. [70] | 1995 | Case report | duodenum | 1 | 57 | M | UK | hepatic hilum | 7 | none | no | NA |
| Okusaka, T. et al. [71] | 1997 | Case report | duodenum | 1 | 60 | M | alcohol | N/A ** | 11 | surgical resection, TAE, PEI | no | NA |
| Hung, H.C. et al. [72] | 1998 | Case report | duodenum + stomach | 1 | 58 | M | HBV | RHL | 4 | surgical resection, TAE, systemic chemotherapy | no | 20,799 |
| Farrell, R. et al. [73] | 1999 | Case report | duodenum | 1 | 53 | M | HCV | N/A ** | 8 | surgical resection | no | 5 |
| Srivastava, D.N. et al. [41] | 2000 | Case series | duodenum | 1 | 48 | M | N/A | RHL | N/A | none | N/A | N/A |
| Lin, C.P. et al. [7] | 2000 | Retrospective analysis study | duodenum | 3 | 64 | M | HBV | RHL, LHL | 10 | none | yes | 252 |
| duodenum + transverse colon | 67 | M | HBV | RHL, LHL | 15 | none | yes | 12,420 | ||||
| duodenum | 56 | M | HBV | LHL | 12 | none | yes | <3 | ||||
| Del Natale, M. et al. [74] | 2001 | Case report | duodenum | 1 | 67 | M | alcohol | N/A | N/A | TACE | yes | 24,935 |
| Cho, A. et al. [75] | 2002 | Case report | duodenum | 1 | 50 | M | HBV | RHL | 22 | none | no | 3477 |
| Ohnishi, S. et al. [76] | 2003 | Letter to the editor | duodenum | 1 | 73 | M | N/A | RHL | 9 | surgical resection, TAE, RFA, PEI, radiotherapy | no | N/A |
| Uehara, K. et al. [77] | 2003 | Case report | duodenum | 1 | 62 | M | HCV | RHL | 1 | none | N/A | 2000 |
| Chung, C. et al. [78] | 2009 | Case report | duodenum | 1 | 53 | F | HCV, alcohol | N/A | N/A ** | none | yes | NR |
| Kurtz, L.E. et al. [79] | 2009 | Editorial material | duodenum | 1 | 78 | F | HCV | RHL | 8.5 | RFA, sorafenib | no | N/A |
| Kato, Y. et al. [11] | 2011 | Case report | duodenum | 1 | 63 | M | UK | RHL | 25; 2 | none | no | 848 |
| Lin, T.L. et al. [10] | 2011 | Review | duodenum | 1 | 72 | M | HBV | RHL | 4.5 | PEI, RAE, surgical resection | no | N/A |
| Liang, J.D. et al. [80] | 2011 | Retrospective analysis study | duodenum-19 duodenum + stomach-1 duodenum + colon-1 | 21 | 62.5 | M-17; F-4 | HBV-12; HCV-7; HBV + HCV-2; alcohol-2 | LHL, RHL-3; RHL-7; LHL-4; peritoneum-1; lymph node -1; no recurrent liver tumor = 1; NA = 4 | 8.6 | none-4; surgical resection-3; surgical resection + TACE-7; surgical resection + TACE + PEI-1; TACE + RFA-1; TACE-4; TACE + PEI-1 | yes-3; no-18 | 8051.6 |
| Kim, J.N. et al. [81] | 2012 | Case report | duodenum | 1 | 57 | M | UK | LHL | N/A | TACE | yes | N/A |
| Sauer, B.G. et al. [82] | 2012 | Editorial material | duodenum | 1 | 68 | M | N/A | N/A | N/A | TACE, radiotherapy, systemic chemotherapy | N/A | N/A |
| Arima, K. et al. [83] | 2015 | Case report | duodenum | 1 | 76 | F | HCV | RHL | 6 | surgical resection | yes | 34,428 |
| Kashani, A. et al. [84] | 2015 | Case report | duodenum | 1 | 62 | M | HCV | N/A ** | N/A | TACE | no | N/A |
| Lin, I.C. et al. [85] | 2017 | Editorial material | duodenum | 1 | 83 | M | N/A | RHL | N/A | TACE | N/A | N/A |
| Ito, T. et al. [86] | 2019 | Case report | duodenum | 1 | 65 | M | HCV | N/A | 10 | TACE, sorafenib | no | 13,300 |
| Liu, Y.H. et al. [87] | 2020 | Case report | duodenum | 1 | 62 | M | HBV | RHL | 2.4 | RFA, surgical resection | no | NR |
| Wu, Y.H. et al. [88] | 2021 | Case report | duodenum | 1 | 80 | F | N/A | N/A | 25 | none | N/A | N/A |
| Bonboire, R. et al. [34] | 2021 | Case report | duodenum | 1 | 67 | M | alcohol | RHL | 79 | none | no | 269 |
| Sawada, K. et al. [89] | 2021 | Editorial material | duodenum | 1 | 72 | M | alcohol | caudate lobe | N/A | TACE | no | N/A |
| Lee, Y.J. et al. [90] | 2021 | Retrospective analysis study | duodenum-3 stomach-1 duodenum + stomach-3 | 7 | 59.71 *** | M-7 | HBV-6 UK-1 | N/A | N/A | TACE, PEIT-4 TACE, RT-2 | N/A | N/A |
| Tsujimoto, M. et al. [91] | 1984 | Case report | intestinal tract | 1 | 62 | M | alcohol | RHL | 14 | none | N/A | N/A |
| Chen, L.T. et al. [6] | 1990 | Retrospective analysis study | jejunum | 1 | 36 | M | HBV | RHL | NA | hepatic arterial ligation | UK | 309 |
| Narita, T. et al. [92] | 1993 | Case report | small bowel-mostly ileum + stomach | 1 | 73 | F | HBV | RHL | 6 | TAE | no | 16,000 |
| Tanaka, A. et al. [93] | 2000 | Case report | ileum | 1 | 52 | M | HBV | Peritoneum+ small intestine **** | N/A | TACE, surgical resection, systemic chemotherapy, hyperthermia | no | 1160 |
| Byun, J.R. et al. [94] | 2005 | Case report | ileum | 1 | 27 | M | none | RHL, caudate lobe | 2.4; 3.4; 4.5 | TACE | yes | 6050 |
| Kim, H.S. et al. [95] | 2006 | Case report | jejunum | 1 | 65 | M | HBV | N/A | N/A | none | N/A | 629 |
| Iwaki, K. et al. [96] | 2008 | Case report | jejunum | 1 | 60 | M | HCV | N/A | N/A | surgical resection, TACE, RFA | no | N/A ***** |
| Choi, J.H. et al. [97] | 2012 | Case report | jejunum | 1 | 54 | M | HBV | N/A | N/A | sorafenib, surgical resection | yes | N/A |
| Kunizaki, M. et al. [98] | 2012 | Case report | small bowel | 1 | 60 | M | HBV | N/A | N/A | TACE, RFA | no | 1345 |
| Igawa, A. et al. [99] | 2013 | Case report | ileum | 1 | 60 | M | HBV | N/A | N/A | sorafenib | yes | 86.5 |
| Kanazawa, M. et al. [100] | 2018 | Case report | jejunum | 1 | 76 | M | alcohol | N/A | N/A | surgery, TACE, sorafenib | N/A | N/A |
| Shelat, V.G. et al. [101] | 2018 | Case report | jejunum | 1 | 75 | M | HBV | N/A | N/A | surgical resection | no | N/A |
| Sun, W.C. et al. [102] | 2018 | Editorial material | ileum | 1 | 72 | M | N/A | N/A | N/A | TACE, RFA | N/A | N/A |
| Mashiko, T. et al. [103] | 2020 | Case report | ileum | 1 | 71 | M | HBV | RHL | N/A | surgical resection, sorafenib | no | N/A |
| Suzuki, N. et al. [104] | 2020 | Case report | small bowel | 1 | 75 | M | alcohol | LHL, caudate lobe ****** | 2 | Lenvatinib, RFA, surgical resection | no | 2.2 |
| Fukui, H. et al. [105] | 1993 | Case report | ascending colon | 1 | 57 | M | HCV | RHL | N/A | surgical resection, TAE | no | 7 |
| Hashimoto, M. et al. [16] | 1996 | Case report | transverse colon | 1 | 72 | F | HCV | RHL | 4.5 | TAE | no | 33 |
| Cosenza, C.A. et al. [106] | 1989 | Case report | duodenum (inflammatory adhesions) + ascending colon | 1 | 82 | F | HCV | RHL | NA | surgical resection, systemic chemotherapy, cryoablation | no | 19 |
| Srivastava, D.N. et al. [41] | 2000 | Case series | transverse colon | 1 | 32 | M | HBV | LHL | N/A | no | no | N/A |
| Lin, C.P. et al. [7] | 2000 | Retrospective analysis study | colon | 3 | 59 | M | HCV | RHL | 8 | TAE | yes | 3319 |
| 69 | M | HBV | RHL, LHL | 20 | none | no | 698.346 | |||||
| 63 | M | UK | RHL, LHL | 20 | none | yes | 46 | |||||
| Kurachi, K. et al. [107] | 2002 | Case report | colon | 1 | 43 | M | UK | LHL | 12 | PEIT, surgical resection | no | 3 |
| Zech, C.J. et al. [108] | 2006 | Case report | ascending colon | 1 | 57 | M | HBV + HCV | RHL | N/A | TACE | no | N/A |
| Tapuria, N. et al. [109] | 2006 | Case report | ascending colon | 1 | 67 | M | autoimmune cirrhosis | RHL, LHL | N/A | none | yes | 20.9 |
| Kaibori, M. et al. [110] | 2007 | Case report | descending colon | 1 | 61 | M | HCV | RHL, LHL | 2; 1.5 | TAE, PEI, surgical resection | N/A | N/A |
| Ng, D.S.C. et al. [111] | 2007 | Case report | ascending and hepatic flexure of the colon | 1 | 35 | M | HBV | RHL | 12 | surgical resection | no | 7 |
| Hirashita, T. et al. [112] | 2008 | Case report | transverse colon | 2 | 79 | M | HCV | caudate lobe | 7.5 | TACE | no | 331 |
| hepatic flexure of colon | 69 | M | HCV | RHL | 5.5 | TACE, RFA | no | 370 | ||||
| Nozaki, Y. et al. [113] | 2008 | Letter to the editor | ascending colon | 1 | 69 | M | N/A | LHL | N/A | surgical resection | no | 686 |
| Yoo, D.J. et al. [114] | 2010 | Case report | sigmoid colon | 1 | 47 | M | HBV | RHL | 1.7 | TACE | no | NR |
| Huang, S.F. et al. [115] | 2011 | Editorial material | rectum | 1 | 57 | F | HCV | RHL | 3.8; 1.5 | RFA | no | 800 |
| Shih, Y.J. et al. [116] | 2012 | Letter to the editor | sigmoid colon | 1 | 50 | M | UK | RHL | 7; 6 | none | no | NR |
| Haga, Y. et al. [117] | 2013 | Case report | cecum | 1 | 75 | F | HCV | RHL | 3.8; 1.5 | RFA | no | 800 |
| Sun, L.H. et al. [118] | 2013 | Case report | ascending colon | 1 | 72 | F | NA | caudate lobe | 6 | none | no | N/A |
| Imada, S. et al. [119] | 2013 | Case report | appendix | 1 | 66 | M | N/A | N/A | N/A | surgical resection, TAE | no | 37 |
| Ou, T.M. et al. [120] | 2014 | Case report | ascending colon + rectum | 1 | 62 | M | HBV | RHL, LHL | N/A | surgical resection, RFA, PEI, stereotactic radiosurgery, TACE | N/A | N/A |
| Kohli, R. et al. [121] | 2014 | Editorial material | splenic flexure of the colon | 1 | 50 | F | cryptogenic cirrhosis | RHL | 1.5 | LT, Yttrium-90 radioembolization | N/A | 43 |
| Zhu, X. et al. [122] | 2016 | Letter to the editor | transverse colon | 1 | 47 | M | HBV | No tumor recurrence | 1.8 | surgical resection, TACE, TAE | no | NR |
| Mitsialis, V. et al. [123] | 2018 | Letter to the editor | sigmoid colon | 1 | 67 | F | N/A | N/A | N/A | TACE, surgical resection | yes | N/A |
| Repullo, D. et al. [124] | 2018 | Case report | hepatic flexure of the colon | 2 | 49 | M | UK | RHL | 10 | none | NR | NR |
| Tagliabue, F. et al. [125] | 2019 | Case report | sigmoid colon | 1 | 70 | M | HBV | RHL | N/A | TACE | no | 3 |
| Pham, B.V. et al. [126] | 2019 | Case report | sigmoid colon | 1 | 60 | M | HBV | RHL, LHL | 4.1 | TACE | no | 9.48 |
| Soni, A. et al. [127] | 2019 | Case report | hepatic flexure | 1 | 65 | M | HCV | RHL, LHL | 12 | none | N/A | 633 |
| Yu, Y.M. et al. [13] | 2020 | Case report | sigmoid colon | 1 | 60 | M | HBV | RHL | N/A | resection, TACE, RFA, PRFA, sorafenib, regorafenib, immunotherapy | no | 21,000 |
| Mu, M. et al. [14] | 2021 | Case report | hepatic flexure | 1 | 86 | M | HBV | RHL | 7 | TACE, ablation | no | NR |
| Miyauchi, T. et al. [128] | 2021 | Case report | colon | 1 | 80 | M | HBV | RHL | N/A | TACE, surgical resection, RFA | no | N/A |
| Park, M.S. et al. [8] | 2002 | Retrospective analysis study | duodenum-4, colon-3, stomach-10, stomach and colon-1 | 18 | 58 | M-15, F-3 | N/A | 11-LHL, 5-RHL, 2-LHL, RHL | mean ≈ 6 | 2-surgical resection, 10-none, 6-NA | yes = 10; no = 8 | N/A |
| Liu, K.W. et al. [129] | 2013 | Case report | rectum | 1 | 71 | M | HBV | RHL | 1.5 cm No liver tumor recurrence | RFA | no | 11 |
| Nielsen, J.A. et al. [130] | 2014 | Case report | rectosigmoid | 1 | 51 | M | HBV | N/A | N/A | surgical resection | no | N/A |
| Ikeda, A. et al. [131] | 2016 | Case report | rectum | 1 | 82 | F | HCV | RHL, LHL | 3.5; 2.5;1 | RFA, TACE | N/A | 3024 |
| Author | Clinical Presentation | Route of Involvement | Imagistic Methods Used for the Diagnosis of GI Involvement | Endoscopic Aspect | Method of Histopathological Diagnosis | IHC | Survival Period (Months) |
|---|---|---|---|---|---|---|---|
| Sohn, D. et al. [19] | anorexia, weight loss | hematogenous, trans-lymphatic | UGI | not done | NA | no | 7 |
| Hiraoka, T. et al. [20] | hematemesis | hematogenous | autopsy | not done | autopsy | no | post-mortem diagnosis |
| NA | hematogenous | autopsy | not done | autopsy | no | post-mortem diagnosis | |
| Kume, K. et al. [21] | dysphagia, tarry tools | hematogenous | EGD, CT | polypoid lesion | autopsy | no | 2 |
| Sohara, N. et al. [22] | melena | hematogenous | EGD | submucosal tumor | EGD + autopsy | no | 1 |
| hematemesis | hematogenous | EGD | polypoid lesion | autopsy | no | 6 | |
| Tsubouchi, E. et al. [23] | epigastric discomfort | hematogenous + direct invasion | EGD, EUS, CT | polypoid lesion | EGD | yes | 3 |
| Yan, S.L. et al. [24] | melena | hematogenous | EGD | polypoid lesion | EGD | yes | 1 |
| Xie, L.Y. et al. [25] | dysphagia, odynophagia | hematogenous | EGD, CT | polypoid lesion | EGD | yes | alive at eight-month follow-up |
| Choi, C.S. et al. [27] | hematemesis | hematogenous | EGD, EUS | submucosal mass polypoid | EGD | yes | 7 |
| Hsu, K.F. et al. [26] | hematemesis, tarry stools | hematogenous | EGD | polypoid | EGD | yes | 4 |
| Kahn, J. et al. [28] | dysphagia | undetermined | EGD | polypoid (submucosal) | EGD | yes | 9 |
| Boonnuch, W. et al. [29] | dysphagia | hematogenous | UGI series, EGD, EUS, CT, PET-CT | extrinsic compression | resected specimen | no | N/A |
| Skurla, B. et al. [30] | intermittent GI bleeding, anemia | hematogenous | EGD | flat and polypoid lesions | EGD | no | alive at two-month follow-up |
| Fukatsu, H. et al. [31] | progressive anemia | hematogenous | EGD | polypoid/submucosal mass | EGD | yes | 1 |
| Chen, J.X. et al. [32] | nausea, abdominal discomfort, dysphagia, tarry tools | undetermined-possible translymphatic | EGD, PET-CT, CT | ulcerative mass | EGD | no | 1 |
| Harada, J. et al. [12] | asymptomatic (increased AFP) | undetermined * | EGD, CT, UGI series | polypoid lesion | EGD + resected specimen | yes | 2 |
| Kongkam, P. et al. [33] | asymptomatic ** | hematogenous | EUS, PET-CT | not seen | EUS-FNA | no | 20 |
| Boinboire, R. et al. [34] | dysphagia | direct invasion from right atrium mass | EGD, CT | exophytic mass | EGD | yes | alive at fifteen-month follow-up |
| Subramanian, S.K. et al. [35] | hematemesis, melena | N/A | EDS, EUS | nodule | resected specimen | no | alive at five-month follow-up |
| Shiota, T. et al. [36] | hematemesis, melena, anasarca | direct invasion | autopsy | not done | autopsy | no | post-mortem diagnosis |
| Makino, H. et al. [37] | epigastralgia | hematogenous | EGD | Bormann type 2 tumor | autopsy | yes | 2 months + 10 days |
| Chen, L.T. et al. [6] | hematemesis | undetermined | EGD | ulcerated submucosal tumor | EGD | no | 1 |
| bloody stool | hematogenous | EGD, CT, UGI series | Borman III-like- ulcer | EGD | no | 1 | |
| fecal occult blood test+ | direct invasion | EGD, CT | ulcerated submucosal tumor | EGD | no | 2 | |
| De Nardi, P. et al. [38] | anorexia, weakness, weight loss, melena | hematogenous | EGD | polyps | EGD + resected specimen | yes | 20 |
| Nicoll, A.J. et al. [39] | melena, hematemesis, syncope | direct invasion | EGD | protuberant gastric nodule | resected specimen | yes | alive at seven-month follow-up |
| Maruyama, A. et al. [40] | melena | direct invasion | EGD, CT, UGI series | ulceration | resected specimen | no | 5 |
| Srivastava, D.N. et al. [41] | hematemesis | direct invasion | EGD, Angio-CT | ulcerative lesion | none | no | death on the same day as diagnosis |
| Wang, M.H. et al. [42] | tarry stools | undetermined-possible direct invasion | EGD | ulcerated, submucosal tumor | EGD | yes | N/A |
| bloody sputum | undetermined-possible direct invasion | EGD | ulcerated, submucosal tumor | EGD | no | 1 | |
| Lin, C.P. et al. [7] | nausea, vomiting, fecal occult blood test+ | direct invasion | EGD | submucosal tumor | EGD | no | 0.7 |
| melena, abdominal fullness | undetermined | CT | not done | none | no | 9.7 | |
| RUQ + epigastric pain | hematogenous | EGD | ulcerative tumor | EGD | no | 1.8 | |
| melena | direct invasion | EGD | submucosal tumor | EGD | no | 4.7 | |
| hematemesis, melena | direct invasion | EGD, CT | penetrated ulcer | none | no | 1.6 | |
| Fujii, K. et al. [9] | anemia | direct invasion | EGD | ulcerative tumor | resected specimen | no | 32 |
| Inoue, H. et al. [43] | LUQ pain, weight loss | translymphatic (direct invasion from an enlarged lymph node) | EGD, CT | protruding, necrotic tumor | EGD | yes | NA |
| Ong, J.C. et al. [44] | epigastric pain, dizziness, dyspnea, GI bleeding | direct invasion | EGD | ulcer (bleeding) | resected specimen | no | alive at two-year-and-nine-month follow-up |
| Kimura, K. et al. [45] | progressive anemia, posprandial epigastric pressure, hematemesis | direct invasion | EGD, CT | extrinsic compression | EGD | no | 2 |
| Korkolis, D.P. et al. [46] | upper abdominal pain, gastric outlet obstruction | direct invasion | EGD, CT | protrusive, infiltrating tumor | resected specimen | no | alive at sixteen-month follow-up |
| Hu, M.L. et al. [47] | NA | hematogenous | EGD | ulcerative mass | EGD | no | N/A |
| NA | hematogenous | EGD | ulcerative mass | EGD | no | N/A | |
| NA | hematogenous | EGD | ulcerative mass | EGD | no | N/A | |
| NA | hematogenous | EGD | ulcerative mass | EGD | no | N/A | |
| NA | hematogenous | EGD | ulcerative mass | EGD | no | N/A | |
| NA | hematogenous | EGD | ulcerative mass | EGD | no | N/A | |
| NA | hematogenous | EGD | ulcer with irregular margin | EGD | no | N/A | |
| Park, H. et al. [48] | dysphagia, postprandial epigastric pain, hematemesis | direct invasion | EGD, CT | fistula | EGD | no | 0.5 |
| Lin, T.L. et al. [10] | NA | direct invasion | EGD, CT | ulcerative tumor | resected specimen | no | >80 |
| Tan, W.J. et al. [49] | melena, hematemesis, abdominal distension, nausea, epigastric pain | direct invasion | EGD, EUS, CT | ulcer | none | no | N/A |
| Sayana, H. et al. [50] | hematemesis, melena | direct invasion | EGD, CT | fistula | none | no | alive at six months after diagnosis |
| Okay, E. et al. [51] | dyspnea, abdominal distension, nausea, vomiting, abdominal pain, fever, weight loss | direct invasion | intraoperative diagnosis | not done | resected specimen | yes | 12 |
| Inagaki, Y. et al. [52] | hematemesis | hematogenous | EGD, CT | polypoid lesions | autopsy | no | 1 |
| Wu, W.D. et al. [53] | GI bleeding | direct invasion | EGD, MRI | mass mimicking gastric cancer | resected specimen | yes | alive at twelve-month follow-up |
| Grover, I. et al. [54] | melena, hematemesis | direct invasion | EGD, CT | fistula | no | no | N/A |
| Li, L. et al. [55] | melena | translymphatic | EGD, CT | (polypoid) cauliflower like- mass | EGD | yes | 4 |
| Hot, S. et al. [56] | GI bleeding | direct invasion | EGD, CT | ulcerated mass | resected specimen + EGD | yes | <1 m |
| Haruki, K. et al. [57] | epigastric pain | hematogenous | EGD, CT, MRI | submucosal tumor | resected specimen | no | alive at thirteen-month follow-up |
| Wu, D. et al. [58] | melena, anemia | undetermined | EGD, colonoscopy | N/A | resected specimen | no | 50 |
| Abdul Hakim, M.S. et al. [59] | anemia, melena | hematogenous | EGD | fungating, nodular mass | EGD | yes | 1 |
| Peng, L. et al. [60] | hepatalgia, asthenia | undetermined * | EGD, CT | protrusion like stromal tumor | resected specimen | yes | alive at six-month follow-up |
| Kasi, M. et al. [61] | anemia | needle track seeding (EUS) | EGD, MRI, PET-CT | polypoid, ulcerated mass | EGD + resected specimen | yes | N/A |
| Sakumura, M. et al. [62] | anemia, leg numbness | hematogenous | EGD | polyp | EGD | yes | N/A |
| Bale, A. et al. [63] | upper GI bleeding | undetermined | EGD, CT | fistula | none | no | N/A |
| Imai, M. et al. [64] | anemia | hematogenous | EGD | elevated lesion | EGD | yes | 5 |
| Marques da Costa, P. et al. [65] | abdominal pain, melena | direct invasion | EGD, CT | lobulated mass | EGD | yes | <1 (0.75) |
| Kim, R. et al. [66] | dyspnea, melena | hematogenous | EGD, CT, colonoscopy | fungating mass-stomach; ulcerofungating tumor—ascending colon | EGD + colonoscopy+ surgical resection | yes | 1.5 |
| Abouzied, M.M. et al. [67] | weakness, anemia | probably hematogenous | MRI, EGD, PET-CT | polyps | EGD | no | alive at 15-month follow-up |
| Eskarous, H. et al. [68] | dysphagia | N/A | EGD | polyps | EGD | yes | N/A |
| Chen, L.T. et al. [6] | nausea, vomiting, fecal occult blood test+ | direct invason | EGD | polypoid (cauliflower tumor) | EGD | no | <1 (0.75) |
| melena | direct invasion | EGD, celiac angiography, CT | ulcerated, submucosal tumor | none | no | 1 | |
| epigastric pain, fecal occult blood test+ | direct invasion | EGD, UGI series, | penetrating ulcer | none | no | 4 | |
| melena | direct invasion | EGD, CT, UGI series | polypoid (cauliflower tumor) | EGD | no | 2 | |
| Arima, K. et al. [69] | hematemesis, melena | hematogenous | EGD | Bormann 2 type elevation with large tumor | EGD + autopsy | no | 17 |
| Moriura, S. et al. [70] | anemia | direct invasion | EGD, UGI series | ulcer | EGD + resected specimen | no | alive at 22-month follow-up |
| Okusaka, T. et al. [71] | GI bleeding, abdominal pain | direct invasion | autopsy | duodenum not analysed at EGD | autopsy | no | post-mortem diagnosis |
| Hung, H.-C. et al. [72] | abdominal pain, tarry stools | direct invasion | EGD, CT | ulcerative mass | EGD | no | 6 |
| Farell, R. et al. [73] | GI bleeding, lethargy | direct invasion | EGD, EUS | persistent nodular ulcer | EGD-not suggestive | no | N/A |
| Srivastava, D.N. et al. [41] | GI bleeding | direct invasion | EGD | ulcerative mass | EGD | no | 2 |
| Lin, C.P. et al. [7] | RUQ pain, fecal occult blood test+ | hematogenous | EGD | ulcerative tumor | EGD | no | 2.2 |
| RUQ pain, fecal occult blood test+ | direct invasion | CT | not done | none | no | 1.5 | |
| GI bleeding | direct invasion | EGD, CT | ulcerative tumor | EGD | no | 3 | |
| Del Natale, M. et al. [74] | abdominal pain, asthenia, dyspnea, anemia | direct invasion | EGD, CT | fistula | no | no | N/A |
| Cho, A. et al. [75] | palpable abdominal tumor, vomiting | direct invasion | CT, EGD | submucosal tumor | resected specimen | no | N/A |
| Ohnishi, S. et al. [76] | hematemesis | direct invasion | CT, EGD, UGI series | obstruction by the invading tumor | autopsy | no | 2 |
| Uehara, K. et al. [77] | no symptoms described | compression of a lymph node metastasis | CT, upper roentgenography | normal duodenal mucosa | none | no | Alive—no signs of recurrence at 22-month follow-up |
| Chung, C. et al. [78] | melena, abdominal pain | undetermined * | EGD | ulcerative tumor + nodule resembeling liver parenchyma | EGD | yes | 7 |
| Kurtz, L.E. et al. [79] | melena, anemia | direct invasion | EGD. CT | infiltrating mass | none | no | N/A |
| Kato, Y. et al. [11] | painful epigastric mass | direct invasion | UGI series | not done | resected specimen | yes | 8 |
| Liang, J.D. et al. [80] | GI bleeding-17, abdominal pain-2, anemia-1 | direct invasion-14; undetermined-1; metastases-6, (hematogeneous/translymphatic-5, peritoneal spreading-1) | CT-4; EGD-4; intraoperative diagnosis-1; CT + EGD-12; UGI series-2 | ulceration-13; tumor mass-10; fistula-1 | EGD-2; resected specimen-7; none-12 | no | mean 10.5 |
| Lin, T.L. et al. [10] | tarry stools | direct invasion | CT, EGD | ulcerative mass | resected specimen | no | >68 |
| Kim, J.N. et al. [81] | melena, dyspnea | direct invasion | CT, EGD | protrusive mass | EGD | no | 3 |
| Sauer, B.G. et al. [82] | GI bleeding, nausea, vomiting | direct invasion | EGD, CT | large mass (liver) penetrating the pyloric channel causing gastric obstruction | EGD | yes | 1 |
| Arima, K. et al. [83] | N/A | hematogenous | CTHA, CTAP | not done | resected specimen | no | N/A |
| Kashani, A. et al. [84] | fatigue, GI bleeding | spread of HCC tumoral cells after biliary interventions | EGD, MRI | periampullary mass | EGD | yes | few months |
| Lin, I.C. et al. [85] | melena | direct invasion | EGD, CT | mass | EGD | no | N/A |
| Ito, T. et al. [86] | anemia | direct invasion | EGD, CT | ulcerative lesion | EGD + resected specimen | no | alive at three-year follow-up |
| Liu, Y.H. et al. [87] | hematemesis, tarry stools | direct invasion | EGD, CT | ulcer | resected specimen | no | alive at seven-year follow-up |
| Wu, Y.H. et al. [88] | tarry stools | direct invasion | EGD, EUS | ulcerative mass | EGD | yes | N/A |
| Bonboire, R. et al. [34] | melena | direct invasion | EGD, abdominal arteriography, CT | submucosal mass | no | no | 6 |
| Sawada, K. et al. [89] | hematemesis | direct invasion | EGD, CT | ulcer-ulcerative lesion-submucosal tumor-like ulcer | EGD | yes | 7.5 |
| Lee, Y.J. et al. [90] | nausea, vomiting, dysphagia | direct invasion-4 translymphatic-extraluminal compression due to metastatic lymph nodes/3 | EGD | ulcerative mass-4 submucosal tumor-3 | N/A | N/A | <2 months |
| Tsujimoto, M. et al. [91] | abdominal pain, vomiting, abdominal fullness | hematogenous | autopsy | not done | autopsy | yes | post-mortem diagnosis |
| Chen, L.T. et al. [6] | melena | hematogenous | superior mesenteric angiography | not done | laparotomy | no | 0.5 |
| Narita, T. et al. [92] | N/A | hematogenous | autopsy | not done | autopsy | no | post-mortem diagnosis |
| Tanaka, A. et al. [93] | increased AFP, palpable mass | peritoneal spread | intraoperative diagnosis | not done | resected specimen | no | 15 |
| Byun, J.R. et al. [94] | dysuria, fecaluria | peritoneal spread | CT, barium study | not done | resected specimen | no | N/A |
| Kim, H.S. et al. [95] | abdominal pain, nausea, vomiting | hematogenous | CT, US, intraoperative diagnosis | not done | resected specimen | yes | N/A |
| Iwaki, K. et al. [96] | asymptomatic | hematogenous | intraoperative diagnosis | not done | resected specimen | yes | alive at twenty-one months |
| Choi, J.H. et al. [97] | abdominal pain, abdominal distension | hematogenous | intraoperative diagnosis | not done | resected specimen | no | 1 |
| Kunizaki, M. et al. [98] | fatigue, anemia, melena | hematogenous | double-balloon enteroscopy | protruding lesion | double balloon enteroscopy + resected specimen | yes | N/A |
| Igawa, A. et al. [99] | melena, anemia | hematogenous | capsule endoscopy, double-balloon enteroscopy | polypoid lesion | double-balloon enteroscopy | yes | 2 |
| Kanazawa, M. et al. [100] | melena, light-headedness | undetermined | capsule endoscopy, double-balloon enteroscopy | mass lesion | double-balloon enteroscopy | yes | 0.5 |
| Shelat, V.G. et al. [101] | abdominal pain, vomiting, diarrhea | peritoneal spreading | CT | not done | resected specimen | yes | alive at eight-month follow-up |
| Sun, W.C. et al. [102] | melena | metastasis *** | single balloon retrograde enteroscopy | protrusive mass | single-balloon enteroscopy | no | N/A |
| Mashiko, T. et al. [103] | abdominal pain, vomiting | hematogenous | CT | not done | resected specimen | yes | alive at eighty-two-month follow-up |
| Suzuki, N. et al. [104] | abdominal pain | hematogenous | intraoperative diagnosis | not done | resected specimen | no | alive at two-month follow-up |
| Fukui, H. et al. [105] | asymptomatic | possible hematogenous | CT, colonoscopy, scintigraphy Tc-99 MPT | elevated lesion | colonoscopy | no | N/A |
| Hashimoto, M. et al. [16] | melena | direct invasion | colonoscopy, lower GI series superior mesenteric angiography | ulcerations | colonoscopy + resected specimen | no | N/A |
| Cosenza, C.A. et al. [106] | weakness, fatigue, rectorrhagia | duodenum-direct invasion, colon-hematogenous | colonoscopy, lower GI series | polypoid mass | colonoscopy | no | N/A |
| Srivastava, D.N. et al. [41] | bloody stools | direct invasion | angio-CT | not done | none | no | 0.75 |
| Lin, C.P. et al. [7] | bloody stools | direct invasion | colonoscopy, CT | polypod tumor | colonoscopy | no | 1.2 |
| Lin, C.P. et al. [7] | epigastric pain, fecal occult blood test+ | direct invasion | CT, superior mesenteric angiography | not done | none | no | 4.7 |
| Lin, C.P. et al. [7] | bloody stools | direct invasion | CT, superior mesenteric angiography | not seen | none | no | 4 |
| Kurachi, K. et al. [107] | epigastric discomfort | peritoneal spread | intraoperative diagnosis | not done | resected specimen | no | alive at five-year-and-nine-month follow-up |
| Zech, C.J. et al. [108] | abdominal pain, fever, hemorrhagic diarrhea | direct invasion | CT, colonoscopy | inflammatory mucosal lesions | resected specimen | no | N/A |
| Tapuria, N. et al. [109] | rectorrhagia, anemia | hematogenous | CT, colonoscopy | obstructing tumor | colonoscopy | yes | few months |
| Kaibori, M. et al. [110] | melena | metastasis *** | intraoperative diagnosis | not done | resected specimen | no | 5 |
| Ng, D.S.C. et al. [111] | rectorrhagia | hematogenous | colonoscopy | fungating tumor | colonoscopy + resected specimen | no | alive at more than five years |
| Hirashita, T. et al. [112] | epigastric pain | direct invasion | CT | not done | resected specimen | no | 6 |
| melena, abdominal distension | direct invasion | colonoscopy, CT | lobulated tumor | resected specimen | no | 1 | |
| Nozaki, Y. et al. [113] | abdominal pain, hematochezia | metastasis *** | colonoscopy | erosive tumor lesion | colonoscopy | no | 1 |
| Yoo, D.J. et al. [114] | abdominal pain | hematogenous | colonoscopy, CT | bulging mass | resected specimen | yes | alive at four-month follow-up |
| Huang, S.F. et al. [115] | bloody stools | metastasis *** | colonoscopy | soft-tissue-like lesion | resected specimen | yes | N/A |
| Shih, Y.J. et al. [116] | abdominal pain, fever | hematogenous | CT | not done | resected specimen | no | 6 |
| Haga, Y. et al. [117] | abdominal pain, vomiting | peritoneal spreading | CT | not seen | resected specimen | no | N/A |
| Sun, L.H. et al. [118] | abdominal pain | hematogenous | CT | not done | resected specimen | yes | 8 |
| Imada, S. et al. [119] | asymptomatic | hematogenous | US, CT, MRI, CT, PET-CT | normal aspect | resected specimen | yes | alive at 20-month follow-up |
| Ou, T.M. et al. [120] | tenesmus | hematogenous | colonoscopy | polyps | resected specimen | no | 1 |
| Kohli, R. et al. [121] | hematochezia | hematogenous | colonoscopy | friable, necrotic lesion | colonoscopy | no | N/A |
| Zhu, X. et al. [122] | fecal occult blood test+ | hematogenous | colonoscopy | mass | resected specimen | yes | 12 |
| Mitsialis, V. et al. [123] | abdominal pain, diarrhea, hematochezia | hematogenous | colonoscopy | ulceration | resected specimen | no | N/A |
| Repullo, D. et al. [124] | abdominal pain, fever, weight loss | direct invasion | colonoscopy, CT | resected specimen | no | N/A | |
| Tagliabue, F. et al. [125] | GI bleeding | hematogenous | colonoscopy, CT | mass | resected specimen | yes | N/A |
| Pham, B.V. et al. [126] | tenesmus, abdominal pain | hematogenous | colonoscopy, CT | mass | resected specimen | yes | N/A |
| Soni, A. et al. [127] | rectorrhagia, anemia | direct invasion | colonoscopy, CT | ulcerated lesion | colonoscopy | no | at diagnosis |
| YU, Y.M. et al. [13] | hematochezia | hematogenous | colonoscopy, CT | protuberant mass | resected specimen | yes | alive at three-month follow-up |
| Mu, M. et al. [14] | abdominal pain, nausea, vomiting | direct invasion | MRI | not seen | resected specimen | no | 10 |
| Miyauchi, T. et al. [128] | abdominal pain, fever | hematogenous | CT | not done | resected specimen | no | 30 |
| Park, M.S. et al. [8] | GI bleeding-3; lower GI bleeding-1; epigastric discomfort (pain, nausea, vomiting)-9, palpable mass-5 | direct invasion-12; hematogenous-3; undetermined-2; peritoneal spreading-1 | CT-13, CT + UGI series-5, endoscopy = 13 | N/A | EGD-13; resected specimen-5 | no | lost to follow up- 12 patients; 2 months- 3 patients; alive- 3 patients. |
| Liu, K.W. et al. [129] | tenesmus | direct seeding after RFA | CT | not seen | resected specimen | yes | 19 |
| Nielsen, J.A. et al. [130] | abdominal pain, diarrhea | hematogenous | colonoscopy | mass | colonoscopy | yes | N/A |
| Ikeda, A. et al. [131] | bloody stools | hematogenous | colonoscopy, lower GI series, CT | protruding tumor | resected specimen, colonoscopy-not conclusive | yes | 5 |
| Risk Factor | n (%) |
|---|---|
| HBV | 76 (38.57%) |
| HCV | 35 (17.76%) |
| Alcohol | 15 (7.61%) |
| HBV + HCV | 4 (2.03%) |
| HBV, Alcohol | 3 (1.52%) |
| HCV, Alcohol | 1 (0.50%) |
| HBV + HCV + HVD + Alcohol | 1 (0.50%) |
| NAFLD | 1 (0.50%) |
| Autoimmune | 1 (0.50%) |
| Cryptogenic | 2 (1.01%) |
| Unknown | 19 (9.64%) |
| Not specified | 39 (23.35%) |
| Size of HCC (n = 92 Hepatic Nodules) | [Mean ± SD] 8.66 ± 6. 22 cm |
|---|---|
| Localization of HCC (n = 158) | |
| RHL | 62 (31.47%) |
| LHL | 43 (21.82%) |
| LHL, RHL | 38 (19.28%) |
| Caudate lobe | 4 (2.03%) |
| Peritoneum | 2 (1.01%) |
| Lymph nodes | 1 (0.50%) |
| LHL, caudate lobe | 1 (0.50%) |
| RHL, caudate lobe | 1 (0.50%) |
| Hepatic hilum | 2 (1.01%) |
| No tumor recurrence | 4 (2.03%) |
| Portal vein thrombosis | |
| Present | 55 (27.91%) |
| Absent | 109 (55.32%) |
| Not available | 33 (16.75%) |
| AFP | Mean = 15,366.18 ng/mL |
| Methods of Treatment | n (%) |
|---|---|
| TACE | 65 (32.99%) |
| Surgical resection | 57 (28.93%) |
| TAE | 23 (11.67%) |
| Radiofrequency ablation | 20 (10.15%) |
| Liver transplant | 11 (5.58%) |
| Systemic chemotherapy | 11 (5.58%) |
| Targeted molecular therapies | 9 (4.56%) |
| Percutaneous ethanol injection | 14 (7.10%) |
| Radiotherapy | 8 (4.06%) |
| Intra-arterial chemotherapy | 4 (2.03%) |
| Immunotherapy | 1 (0.50%) |
| Yttrium-90 radioembolization | 1 (0.50%) |
| Hepatic arterial ligation | 1 (0.50%) |
| Ultrasound guided percutaneous microwave ablation | 1 (0.50%) |
| Crioablation | 1 (0.50%) |
| None | 53 (26.90%) |
| N/A | 7 (3.55%) |
| GI Site Involved by HCC (n = 197) | n (%) |
|---|---|
| Stomach | 55 (27.91%) |
| Duodenum | 55 (27.91%) |
| Colon | 32 (16.24%) |
| Esophagus | 18 (8.92%) |
| Small bowel | 14 (9.13%) |
| Esophaghus + Stomach | 2 (1.01%) |
| Stomach + colon | 4 (2.03%) |
| Stomach + duodenum | 7 (3.55%) |
| Stomach + small bowel | 2 (1.01%) |
| Duodenum + Colon | 3 (1.52%) |
| Rectum | 3 (1.52%) |
| Rectosigmoid | 1 (0.50%) |
| Rectum and colon | 1 (0.50%) |
| Involvement route | |
| Direct invasion | 87 (44.16%) |
| Hematogenous route | 63 (31.97%) |
| Translymphatic route | 6 (3.04%) |
| Peritoneal spreading | 7 (3.55%) |
| Iatrogenic | 3 (1.52%) |
| Direct invasion + Hematogenous route | 2 (1.19%) |
| Hematogenous + translymphatic route | 1 (0.50%) |
| Metastasis (hematogenous or translymphatic) | 17 (8.62%) |
| Undetermined | 9 (4.56%) |
| N/A | 2 (1.19%) |
| Symptom | n (%) |
|---|---|
| GI bleeding | 98 (49.74%) |
| Abdominal pain | 53 (26.90%) |
| Nausea/Vomiting | 29 (14.72%) |
| Dysphagia | 15 (7.61%) |
| Anemia | 10 (5.07%) |
| Fecal occult blood+ | 8 (4.06%) |
| Gatric outlet obstruction | 8 (0.50%) |
| Palpable abdominal mass | 7 (3.55%) |
| Weight loss | 5 (2.53%) |
| Dyspnea | 5 (2.53%) |
| Abdominal distension | 5 (2.53%) |
| Fever | 5 (2.53%) |
| Fatigue | 4 (2.03%) |
| Diarrhea | 4 (2.03%) |
| Abdominal fulness | 2 (1.01%) |
| Tenesmus | 2 (1.01%) |
| Anorexia | 1 (0.50%) |
| Anasarca | 1 (0.50%) |
| Syncope | 1 (0.50%) |
| Dizziness | 1 (0.50%) |
| Asymptomatic | 4 (2.03%) |
| Not available | 11 (5.58%) |
| Diagnostics Tools | n (%) |
|---|---|
| Upper GI endoscopy | 47 (23.85%) |
| Upper GI endoscopy, CT | 55 (27.91%) |
| CT | 13 (6.59%) |
| Lower GI endoscopy, CT | 10 (5.07%) |
| Lower GI endoscopy | 8 (4.06%) |
| CT, upper GI series | 7 (3.55%) |
| Upper GI endsocopy, CT, upper GI series | 5 (2.53%) |
| Upper GI endoscopy, EUS | 4 (2.03%) |
| Upper GI series | 4 (2.03%) |
| Double baloon/single baloon enteroscopy | 3 (1.52%) |
| CT, superior mesenteric angiography | 2 (1.01%) |
| Capsule endoscopy + double ballon enteroscopy | 2 (1.01%) |
| Upper GI endoscopy, MRI, PET-CT | 2 (1.01%) |
| Lower GI endoscopy, lower GI series | 2 (1.01%) |
| Upper GI endoscopy, EUS, CT | 2 (1.01%) |
| Upper GI endoscopy, MRI | 2 (1.01%) |
| Upper GI endoscopy, upper GI series | 2 (1.01%) |
| Upper GI series, upper GI endoscopy, EUS, CT, PET-CT | 1 (0.50%) |
| EUS, PET-CT | 1 (0.50%) |
| Upper GI endoscopy, MRI, CT | 1 (0.50%) |
| MRI | 1 (0.59%) |
| Upper GI endoscopy, lower GI endoscopy, CT | 1 (0.50%) |
| Upper GI endoscopy, lower GI endoscopy | 1 (0.50%) |
| Upper GI endsoscopy, celiac angiography, CT | 1 (0.50%) |
| Upper GI endoscopy, CTA | 1 (0.50%) |
| CT, CTA | 1 (0.50%) |
| CTA | 1 (0.59%) |
| CT, lower GI endoscopy + Tc-99 m PMT Scintigraphy | 1 (0.50%) |
| CT, lower GI endsocopy, lower GI series | 1 (0.50%) |
| Lower GI endoscopy, lower GI series, superior mesenteric angiography | 1 (0.50%) |
| Superior mesenteric angiography | 1 (0.50%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Urhut, C.M.; Sandulescu, L.D.; Streba, L.; Iovanescu, V.F.; Sandulescu, S.M.; Danoiu, S. Hepatocellular Carcinoma with Gastrointestinal Involvement: A Systematic Review. Diagnostics 2022, 12, 1270. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12051270
Urhut CM, Sandulescu LD, Streba L, Iovanescu VF, Sandulescu SM, Danoiu S. Hepatocellular Carcinoma with Gastrointestinal Involvement: A Systematic Review. Diagnostics. 2022; 12(5):1270. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12051270
Chicago/Turabian StyleUrhut, Cristiana Marinela, Larisa Daniela Sandulescu, Liliana Streba, Vlad Florin Iovanescu, Sarmis Marian Sandulescu, and Suzana Danoiu. 2022. "Hepatocellular Carcinoma with Gastrointestinal Involvement: A Systematic Review" Diagnostics 12, no. 5: 1270. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12051270