
Association between Fibrinogen-to-Albumin Ratio and Prognosis of Hospitalized Patients with COVID-19: A Systematic Review and Meta-Analysis

 , , ,
, , ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Literature Search
2.2. Study Sreening
2.3. Data Collection
2.4. Definitions and Outcomes
2.5. Risk of Bias Assessment for the Included Studies
2.6. Data Synthesis and Analysis
3. Results
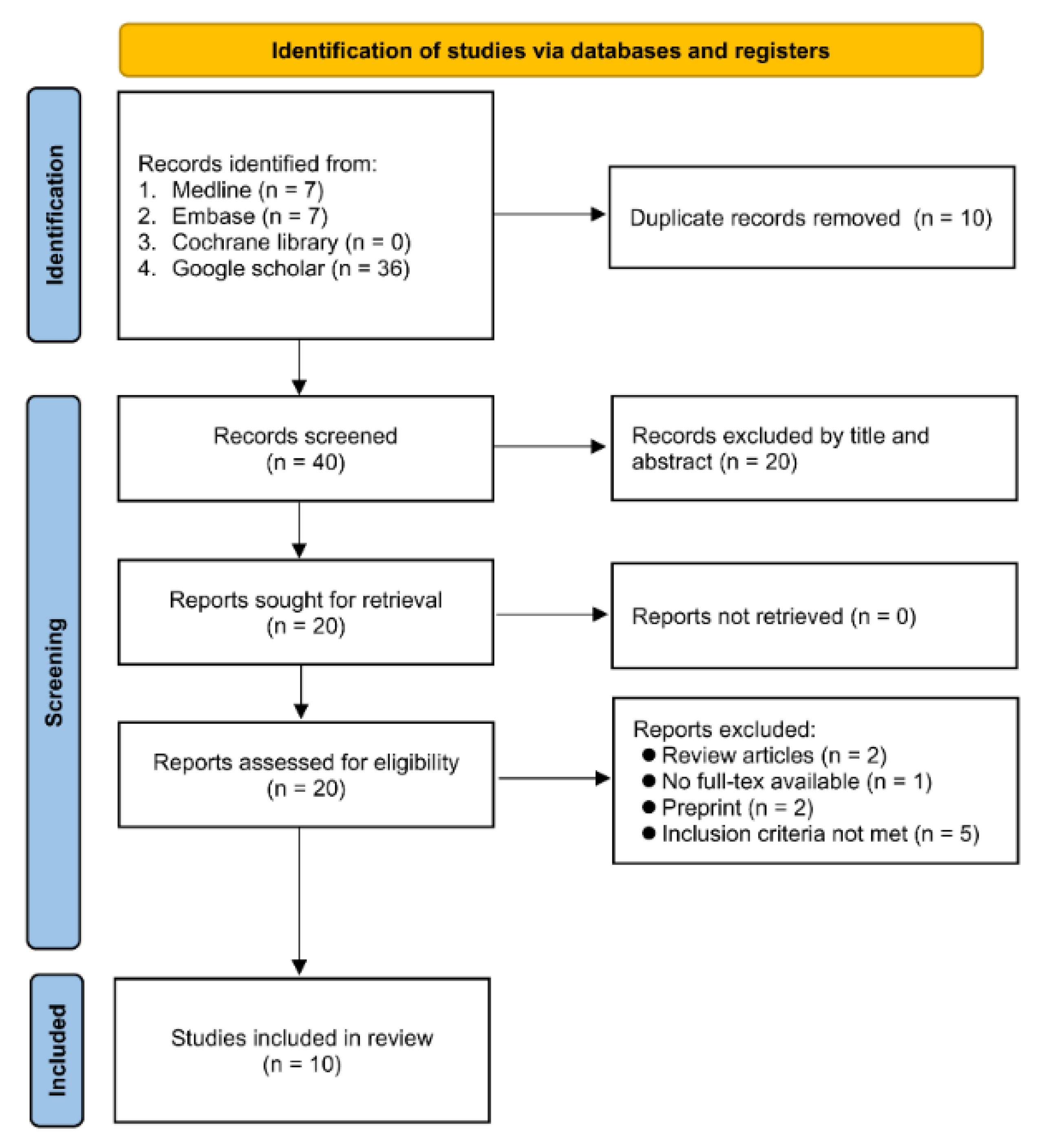
3.1. Study Selection
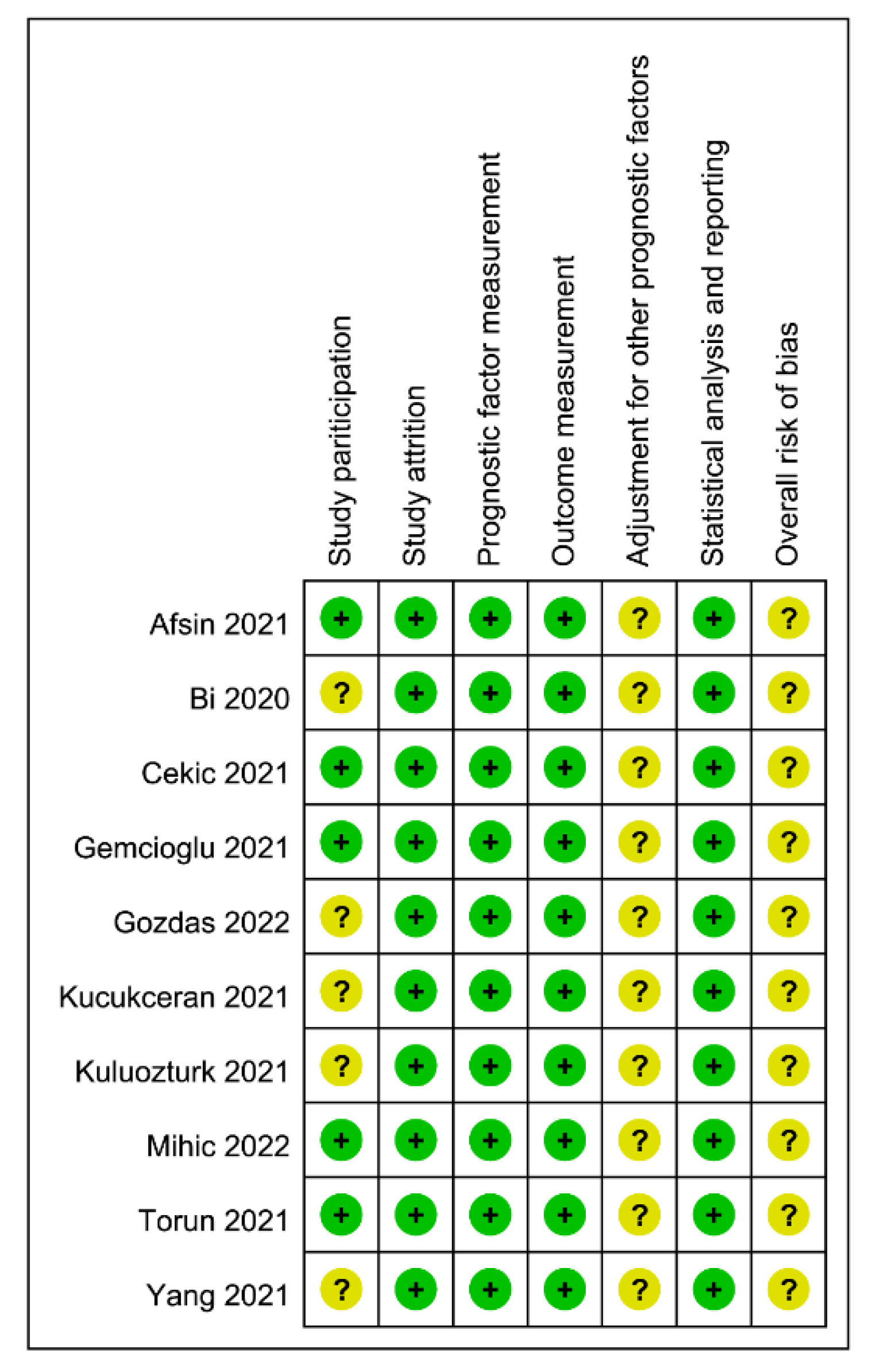
3.2. Characteristics of Studies and Risk of Bias
3.3. Data Analysis
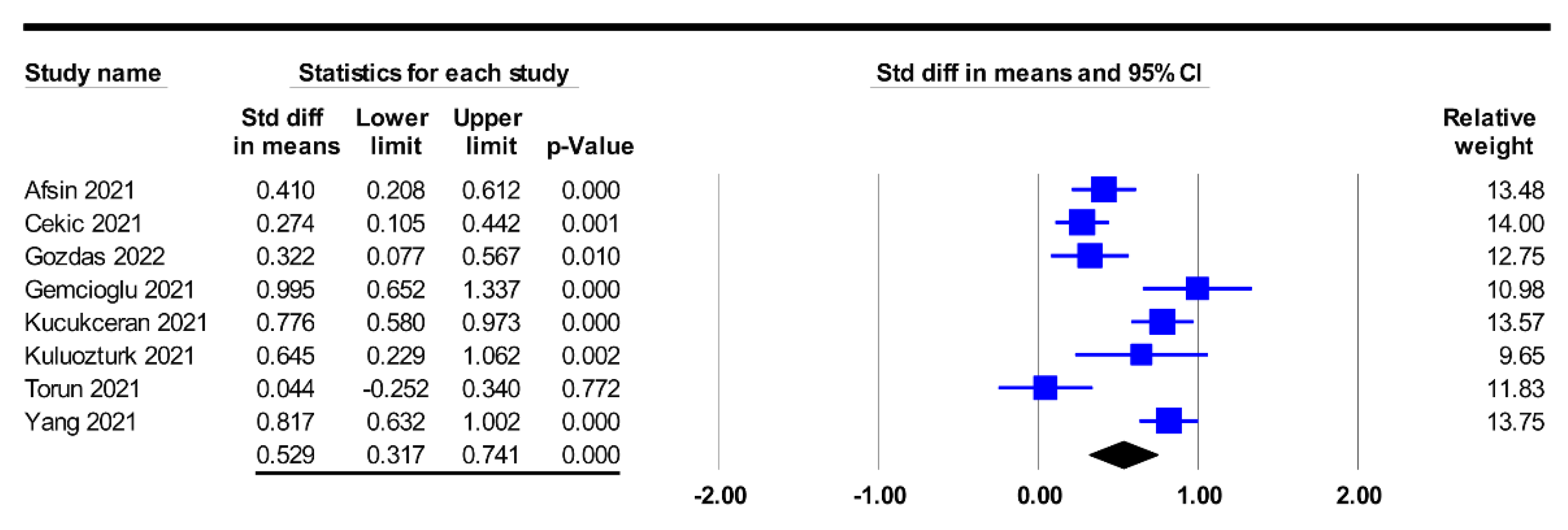
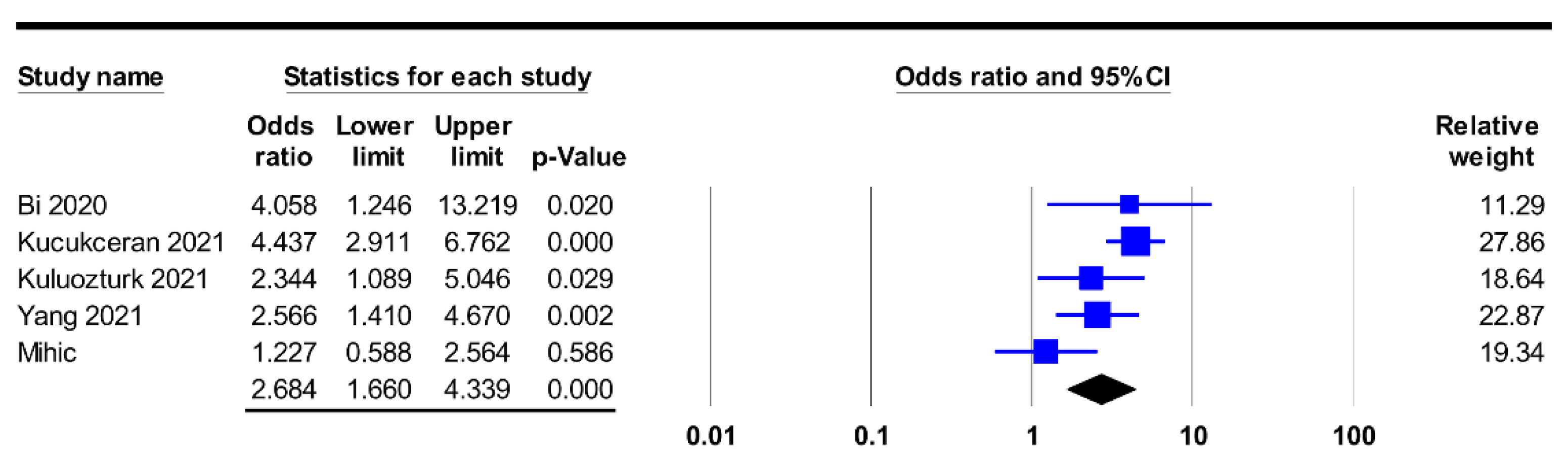
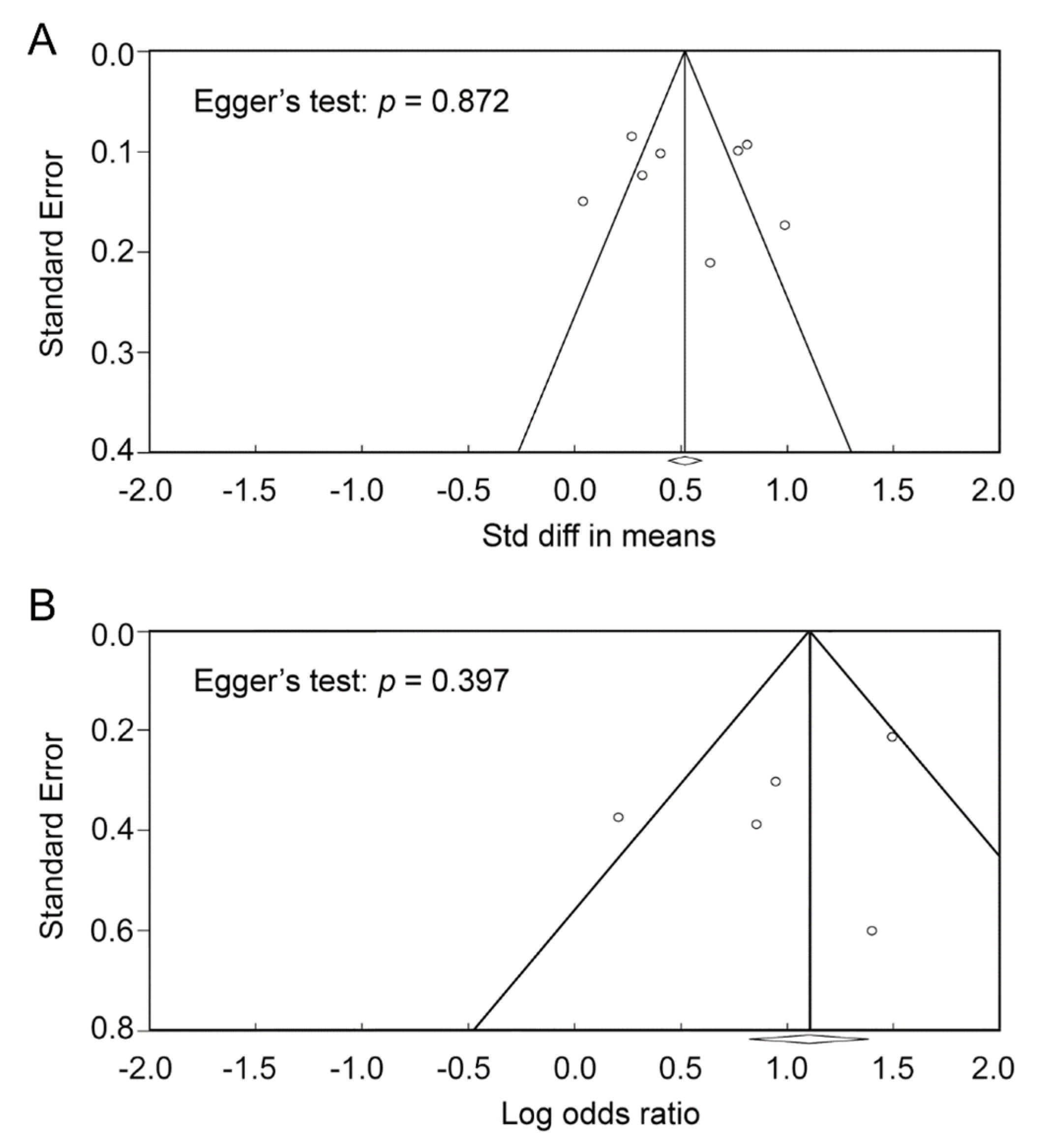
3.3.1. Association of Fibrinogen-to-Albumin Ratio with Prognosis
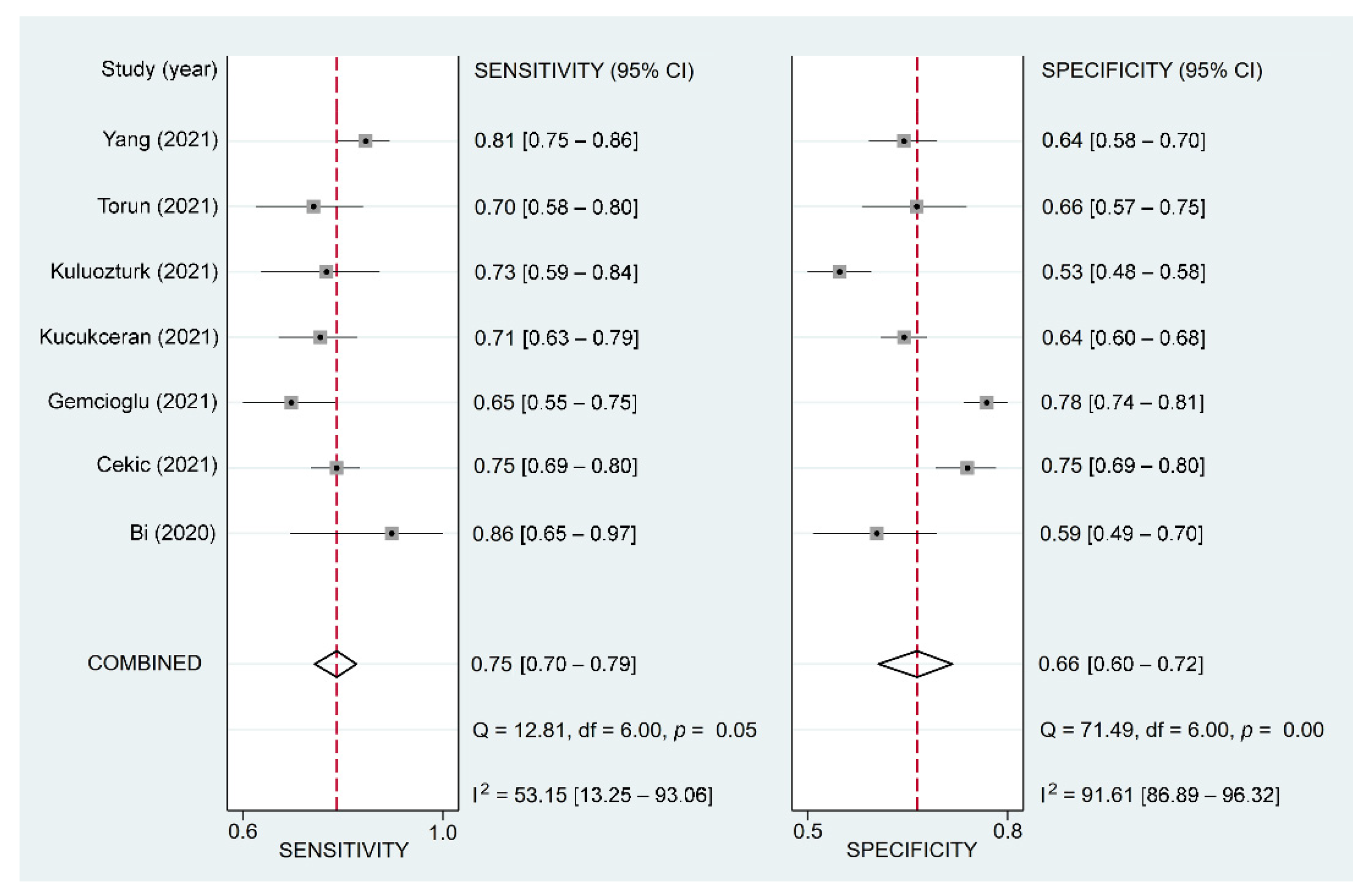
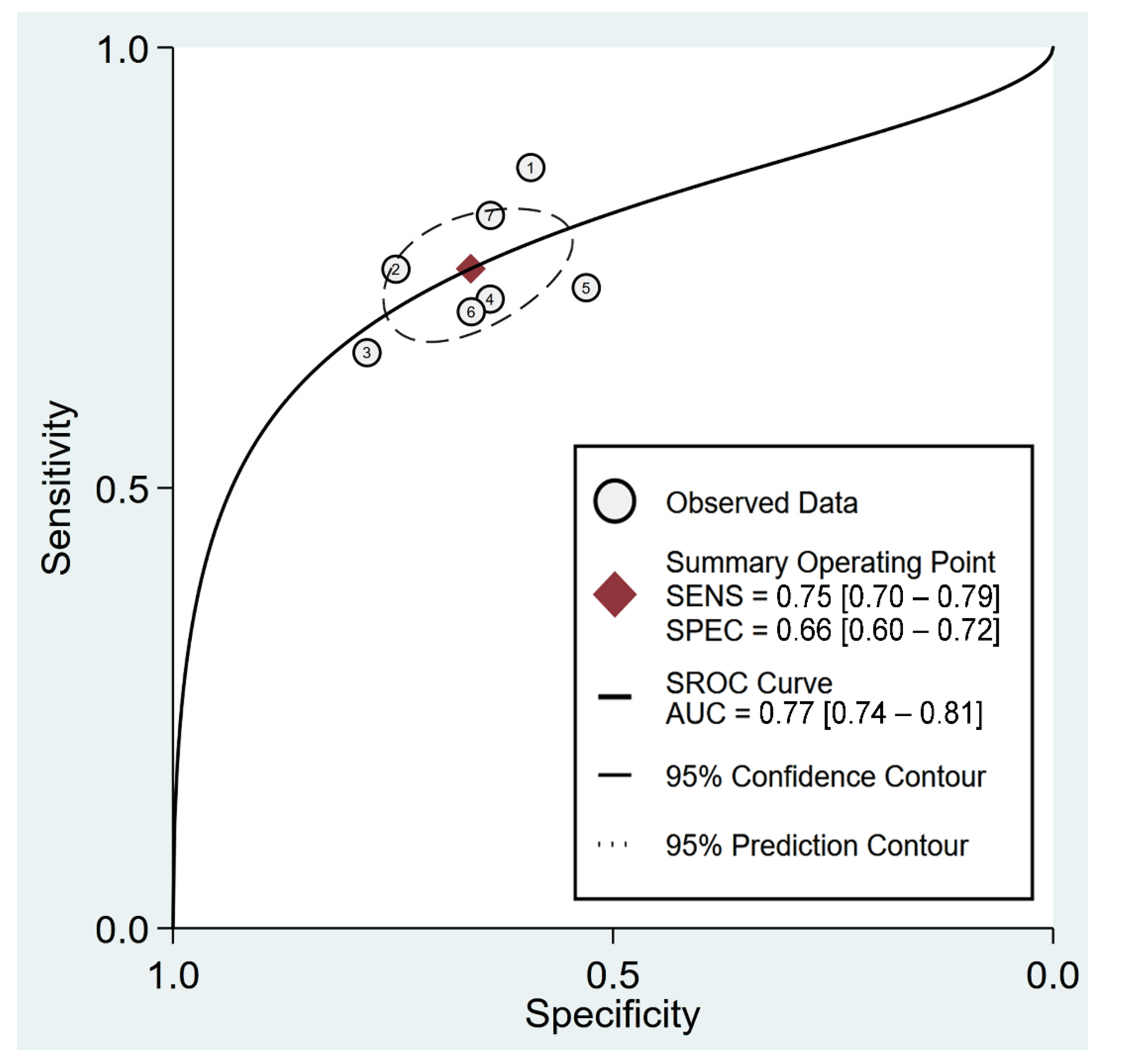
3.3.2. The Use of Fibrinogen-to-Albumin Ratio for Predicting Poor Prognosis: Pooled Sensitivity/Specificity Estimates and sROC
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chang, D.; Chang, X.; He, Y.; Tan, K.J.K. The determinants of COVID-19 morbidity and mortality across countries. Sci. Rep. 2022, 12, 5888. [Google Scholar] [CrossRef] [PubMed]
- Perico, L.; Benigni, A.; Casiraghi, F.; Ng, L.F.P.; Renia, L.; Remuzzi, G. Immunity, endothelial injury and complement-induced coagulopathy in COVID-19. Nat. Rev. Nephrol. 2021, 17, 46–64. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Cao, B. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Reddy, S.G.K.; Mantena, M.; Garlapati, S.K.P.; Manohar, B.P.; Singh, H.; Bajwa, K.S.; Tiwari, H. COVID-2019-2020-2021: Systematic Review and Meta-Analysis. J. Pharm. Bioallied. Sci. 2021, 13, S921. [Google Scholar]
- Laino, M.E.; Ammirabile, A.; Lofino, L.; Lundon, D.J.; Chiti, A.; Francone, M.; Savevski, V. Prognostic findings for ICU admission in patients with COVID-19 pneumonia: Baseline and follow-up chest CT and the added value of artificial intelligence. Emerg. Radiol. 2022, 29, 243–262. [Google Scholar] [CrossRef]
- Hu, H.; Pan, H.; Li, R.; He, K.; Zhang, H.; Liu, L. Increased Circulating Cytokines Have a Role in COVID-19 Severity and Death With a More Pronounced Effect in Males: A Systematic Review and Meta-Analysis. Front. Pharmacol. 2022, 13, 802228. [Google Scholar] [CrossRef]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Tan, W. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Hajiasgharzadeh, K.; Jafarlou, M.; Mansoori, B.; Dastmalchi, N.; Baradaran, B.; Khabbazi, A. Inflammatory reflex disruption in COVID-19. Clin. Exp. Neuroimmunol. 2022. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Peng, Z. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Xu, X.W.; Wu, X.X.; Jiang, X.G.; Xu, K.J.; Ying, L.J.; Ma, C.L.; Li, L.J. Clinical findings in a group of patients infected with the 2019 novel coronavirus (SARS-Cov-2) outside of Wuhan, China: Retrospective case series. Bmj 2020, 368, m606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bi, X.; Su, Z.; Yan, H.; Du, J.; Wang, J.; Chen, L.; Li, J. Prediction of severe illness due to COVID-19 based on an analysis of initial Fibrinogen to Albumin Ratio and Platelet count. Platelets 2020, 31, 674–679. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Plebani, M.; Henry, B.M. Thrombocytopenia is associated with severe coronavirus disease 2019 (COVID-19) infections: A meta-analysis. Clin. Chim. Acta 2020, 506, 145–148. [Google Scholar] [CrossRef] [PubMed]
- Göbel, K.; Eichler, S.; Wiendl, H.; Chavakis, T.; Kleinschnitz, C.; Meuth, S.G. The coagulation factors fibrinogen, thrombin, and factor XII in inflammatory disorders—A systematic review. Front. Immunol. 2018, 9, 1731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brunclikova, M.; Simurda, T.; Zolkova, J.; Sterankova, M.; Skornova, I.; Dobrotova, M.; Kubisz, P. Heterogeneity of Genotype-Phenotype in Congenital Hypofibrinogenemia—A Review of Case Reports Associated with Bleeding and Thrombosis. J. Clin. Med. 2022, 11, 1083. [Google Scholar] [CrossRef]
- Li, Q.; Cao, Y.; Chen, L.; Wu, D.; Yu, J.; Wang, H.; Hu, Y. Hematological features of persons with COVID-19. Leukemia 2020, 34, 2163–2172. [Google Scholar] [CrossRef]
- Wool, G.D.; Miller, J.L. The Impact of COVID-19 Disease on Platelets and Coagulation. Pathobiology 2021, 88, 15–27. [Google Scholar] [CrossRef]
- Hariyanto, T.I.; Japar, K.V.; Kwenandar, F.; Damay, V.; Siregar, J.I.; Lugito, N.P.H.; Kurniawan, A. Inflammatory and hematologic markers as predictors of severe outcomes in COVID-19 infection: A systematic review and meta-analysis. Am. J. Emerg. Med. 2021, 41, 110–119. [Google Scholar] [CrossRef]
- Eckart, A.; Struja, T.; Kutz, A.; Baumgartner, A.; Baumgartner, T.; Zurfluh, S.; Schuetz, P. Relationship of Nutritional Status, Inflammation, and Serum Albumin Levels During Acute Illness: A Prospective Study. Am. J. Med. 2020, 133, 713–722.e7. [Google Scholar] [CrossRef]
- Xiao, L.; Jia, Y.; Wang, X.; Huang, H. The impact of preoperative fibrinogen-albumin ratio on mortality in patients with acute ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention. Clin. Chim. Acta 2019, 493, 8–13. [Google Scholar] [CrossRef]
- Tan, Z.; Zhang, M.; Han, Q.; Wen, J.; Luo, K.; Lin, P.; Fu, J. A novel blood tool of cancer prognosis in esophageal squamous cell carcinoma: The Fibrinogen/Albumin Ratio. J. Cancer 2017, 8, 1025–1029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Vong, T.; Yanek, L.R.; Wang, L.; Yu, H.; Fan, C.; Zhou, E.; Mullin, G.E. Malnutrition Increases Hospital Length of Stay and Mortality among Adult Inpatients with COVID-19. Nutrients 2022, 14, 1310. [Google Scholar] [CrossRef] [PubMed]
- Afşin, A.; Tibilli, H.; Hoşoğlu, Y.; Asoğlu, R.; Süsenbük, A.; Markirt, S.; Tuna, V.D. Fibrinogen-to-albumin ratio predicts mortality in COVID-19 patients admitted to the intensive care unit. Adv. Respir. Med. 2021, 89, 557–564. [Google Scholar] [CrossRef] [PubMed]
- Çekiç, D.; Emir Arman, M.; Cihad Genc, A.; İşsever, K.; Yıldırım, İ.; Bilal Genc, A.; Yaylacı, S. Predictive role of FAR ratio in COVID-19 patients. Int. J. Clin. Pract. 2021, 75, e14931. [Google Scholar] [CrossRef]
- Gómez, C.A.; Sun, C.K.; Tsai, I.T.; Chang, Y.P.; Lin, M.C.; Hung, I.Y.; Hung, K.C. Mortality and risk factors associated with pulmonary embolism in coronavirus disease 2019 patients: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 16025. [Google Scholar] [CrossRef]
- Hung, K.C.; Ho, C.N.; Chen, I.W.; Hung, I.Y.; Lin, M.C.; Lin, C.M.; Sun, C.K. The impact of aminophylline on incidence and severity of post-dural puncture headache: A meta-analysis of randomised controlled trials. Anaesth. Crit. Care Pain Med. 2021, 40, 100920. [Google Scholar] [CrossRef]
- Hayden, J.A.; van der Windt, D.A.; Cartwright, J.L.; Côté, P.; Bombardier, C. Assessing bias in studies of prognostic factors. Ann. Intern. Med. 2013, 158, 280–286. [Google Scholar] [CrossRef]
- Hung, K.C.; Wang, L.K.; Lin, Y.T.; Yu, C.H.; Chang, C.Y.; Sun, C.K.; Chen, J.Y. Association of preoperative vitamin D deficiency with the risk of postoperative delirium and cognitive dysfunction: A meta-analysis. J. Clin. Anesth. 2022, 79, 110681. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. Bmj 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Takwoingi, Y.; Riley, R.D.; Deeks, J.J. Meta-analysis of diagnostic accuracy studies in mental health. Evid. Based Ment. Health 2015, 18, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Gemcioglu, E.; Davutoglu, M.; Catalbas, R.; Karabuga, B.; Kaptan, E.; Aypak, A.; Ates, I. Predictive values of biochemical markers as early indicators for severe COVID-19 cases in admission. Future Virol. 2021, 16, 353–367. [Google Scholar] [CrossRef]
- Gozdas, H.T.; Kayis, S.A.; Damarsoy, T.; Ozsari, E.; Turkoglu, M.; Yildiz, I.; Demirhan, A. Multi-inflammatory Index as a Novel Mortality Predictor in Critically Ill COVID-19 Patients. J. Intensive Care Med. 2022, 08850666221100411. [Google Scholar] [CrossRef]
- Küçükceran, K.; Ayranci, M.K.; Girişgin, A.S.; Koçak, S. Predictive value of D-dimer/albumin ratio and fibrinogen/albumin ratio for in-hospital mortality in patients with COVID-19. Int. J. Clin. Pract. 2021, 75, e14263. [Google Scholar] [CrossRef]
- Kuluöztürk, M.; Deveci, F.; Turgut, T.; Öner, Ö. The Glasgow Prognostic Score and fibrinogen to albumin ratio as prognostic factors in hospitalized patients with COVID-19. Expert Rev. Respir. Med. 2021, 15, 1061–1068. [Google Scholar] [CrossRef]
- Mihić, D.; Maričić, L.; Tolj, I.; Loinjak, D.; Sušić, L.; Begić, I. Prognostic significance inflammatory scoring systems in critically ill patients with COVID-19 infection. Med. Jadertina 2022, 52, 5–12. [Google Scholar]
- Torun, A.; Çakırca, T.D.; Çakırca, G.; Portakal, R.D. The value of C-reactive protein/albumin, fibrinogen/albumin, and neutrophil/lymphocyte ratios in predicting the severity of COVID-19. Revista da Associação Médica Brasileira 2021, 67, 431–436. [Google Scholar] [CrossRef]
- Yang, R.; Gui, X.; Ke, H.; Gao, S.; Luo, M.; Xiong, Y. The indicative role of markers for liver injury on the severity and prognosis of coronavirus disease 2019 patients. Eur. J. Gastroenterol. Hepatol. 2021, 33, e176–e182. [Google Scholar] [CrossRef]
- McGovern, J.; Al-Azzawi, Y.; Kemp, O.; Moffitt, P.; Richards, C.; Dolan, R.D.; Maguire, D. The relationship between frailty, nutritional status, co-morbidity, CT-body composition and systemic inflammation in patients with COVID-19. J. Transl. Med. 2022, 20, 98. [Google Scholar] [CrossRef]
- Cvachovec, K.; Horácek, M.; Vislocký, I. A retrospective survey of fibrinolysis as an indicator of poor outcome after cardiopulmonary bypass and a possible early sign of systemic inflammation syndrome. Eur. J. Anaesthesiol. 2000, 17, 173–176. [Google Scholar] [CrossRef]
- Tousoulis, D.; Papageorgiou, N.; Androulakis, E.; Briasoulis, A.; Antoniades, C.; Stefanadis, C. Fibrinogen and cardiovascular disease: Genetics and biomarkers. Blood Rev. 2011, 25, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Karahan, O.; Yavuz, C.; Kankilic, N.; Demirtas, S.; Tezcan, O.; Caliskan, A.; Mavitas, B. Simple blood tests as predictive markers of disease severity and clinical condition in patients with venous insufficiency. Blood Coagul. Fibrinolysis 2016, 27, 684–690. [Google Scholar] [CrossRef] [PubMed]
- Simurda, T.; Asselta, R.; Zolkova, J.; Brunclikova, M.; Dobrotova, M.; Kolkova, Z.; Kubisz, P. Congenital Afibrinogenemia and Hypofibrinogenemia: Laboratory and Genetic Testing in Rare Bleeding Disorders with Life-Threatening Clinical Manifestations and Challenging Management. Diagnostics 2021, 11, 2140. [Google Scholar] [CrossRef]
- Simurda, T.; Vilar, R.; Zolkova, J.; Ceznerova, E.; Kolkova, Z.; Loderer, D.; Kubisz, P. A Novel Nonsense Mutation in FGB (c.1421G>A; p.Trp474Ter) in the Beta Chain of Fibrinogen Causing Hypofibrinogenemia with Bleeding Phenotype. Biomedicines 2020, 8, 605. [Google Scholar] [CrossRef] [PubMed]
- Nugroho, J.; Wardhana, A.; Mulia, E.P.; Maghfirah, I.; Rachmi, D.A.; A’Yun, M.Q.; Septianda, I. Elevated fibrinogen and fibrin degradation product are associated with poor outcome in COVID-19 patients: A meta-analysis. Clin. Hemorheol. Microcirc. 2021, 77, 221–231. [Google Scholar] [CrossRef] [PubMed]
- Cabrerizo, S.; Cuadras, D.; Gomez-Busto, F.; Artaza-Artabe, I.; Marín-Ciancas, F.; Malafarina, V. Serum albumin and health in older people: Review and meta analysis. Maturitas 2015, 81, 17–27. [Google Scholar] [CrossRef]
- Chen, C.; Wang, S.; Chen, J.; Liu, X.; Zhang, M.; Wang, X.; Si, M. Escin suppresses HMGB1-induced overexpression of aquaporin-1 and increased permeability in endothelial cells. FEBS Open Bio. 2019, 9, 891–900. [Google Scholar] [CrossRef] [Green Version]
- Cao, B.; Jing, X.; Liu, Y.; Wen, R.; Wang, C. Comparison of laboratory parameters in mild vs. severe cases and died vs. survived patients with COVID-19: Systematic review and meta-analysis. J. Thorac. Dis. 2022, 14, 1478–1487. [Google Scholar] [CrossRef]
- Stavileci, B.; Ereren, E.; Özdemir, E.; Özdemir, B.; Cengiz, M.; Enar, R. The impact of daily troponin I and D-dimer serum levels on mortality in COVID-19 pneumonia patients. Cardiovasc. J. Afr. 2022, 33, 1–7. [Google Scholar] [CrossRef]
- Fathalla, L.A.; Kamal, L.M.; Salaheldin, O.; Khalil, M.A.; Kamel, M.M.; Fahim, H.H.; El-Meligui, Y.M. Laboratory biomarker predictors for disease progression and outcome among Egyptian COVID-19 patients. Int. J. Immunopathol. Pharmacol. 2022, 36, 3946320221096207. [Google Scholar] [CrossRef]
- Sahu, B.R.; Kampa, R.K.; Padhi, A.; Panda, A.K. C-reactive protein: A promising biomarker for poor prognosis in COVID-19 infection. Clin. Chim. Acta 2020, 509, 91–94. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Zhang, F.; Hu, W.; Chen, Q.; Li, C.; Wu, L.; Yue, J. Laboratory markers associated with COVID-19 progression in patients with or without comorbidity: A retrospective study. J. Clin. Lab. Anal. 2021, 35, e23644. [Google Scholar] [CrossRef]
- Tirupathi, R.; Muradova, V.; Shekhar, R.; Salim, S.A.; Al-Tawfiq, J.A.; Palabindala, V. COVID-19 disparity among racial and ethnic minorities in the US: A cross sectional analysis. Travel Med. Infect. Dis. 2020, 38, 101904. [Google Scholar] [CrossRef] [PubMed]
- Mackey, K.; Ayers, C.K.; Kondo, K.K.; Saha, S.; Advani, S.M.; Young, S.; Kansagara, D. Racial and Ethnic Disparities in COVID-19-Related Infections, Hospitalizations, and Deaths: A Systematic Review. Ann. Intern. Med. 2021, 174, 362–373. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Zhou, H.; Zhou, Y.; Wu, X.; Zhao, Y.; Lu, Y.; Wang, Y. Risk factors associated with disease severity and length of hospital stay in COVID-19 patients. J. Infect. 2020, 81, e95–e97. [Google Scholar] [CrossRef] [PubMed]
- Qian, Z.; Li, Z.; Peng, J.; Gao, Q.; Cai, S.; Xu, X. Association between hypertension and prognosis of patients with COVID-19: A systematic review and meta-analysis. Clin. Exp. Hypertens. 2022, 44, 451–458. [Google Scholar] [CrossRef] [PubMed]
- Kastora, S.; Patel, M.; Carter, B.; Delibegovic, M.; Myint, P.K. Impact of diabetes on COVID-19 mortality and hospital outcomes from a global perspective: An umbrella systematic review and meta-analysis. Endocrinol. Diabetes Metab. 2022, 5, e00338. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) | Population | Age (Years) | Male (%) | n | Outcome | Cut-Off Value for F/A Ratio | Country |
|---|---|---|---|---|---|---|---|
| Afsin (2021) | ICU patients | 71 vs. 72 | 50 vs. 58 | 386 | Mortality | NA | Turkey |
| Bi (2020) | Hospitalized patients | 54 vs. 44 | 59 vs. 56 | 113 | Severity | 9 | China |
| Cekic (2021) | Medical and ICU patients | 60 vs. 71 | 55 vs. 65 | 590 | Mortality | 13 | Turkey |
| Gemcioglu (2021) | Hospitalized patients | 68 vs. 42 | 55 vs. 53 | 301 | Severity | 10.2 | Turkey |
| Gozdas (2022) | ICU patients | 76 vs. 65 | 60 vs. 57 | 348 | Mortality | NA | Turkey |
| Kucukceran (2021) | Patient admitted to ED | 61 vs. 76 | 62 vs. 51 | 717 | Mortality | 11 | Turkey |
| Kuluozturk (2021) | Hospitalized patients | 65 vs. 54 | 64 vs. 58 | 400 | Mortality | 14 | Turkey |
| Mihic (2022) | ICU patients | 69 vs. 66 | NA | 137 | Mortality | NA | Croatia |
| Torun (2021) | Hospitalized patients | 62 vs. 60 | 54 vs. 47 | 188 | Severity | 11.4 | Turkey |
| Yang (2021) | Hospitalized patients | 61 vs. 53 | 54 vs. 44 | 495 | Severity | 12 | China |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hung, K.-C.; Huang, Y.-T.; Chang, Y.-J.; Yu, C.-H.; Wang, L.-K.; Wu, C.-Y.; Liu, P.-H.; Chiu, S.-F.; Sun, C.-K. Association between Fibrinogen-to-Albumin Ratio and Prognosis of Hospitalized Patients with COVID-19: A Systematic Review and Meta-Analysis. Diagnostics 2022, 12, 1678. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12071678
Hung K-C, Huang Y-T, Chang Y-J, Yu C-H, Wang L-K, Wu C-Y, Liu P-H, Chiu S-F, Sun C-K. Association between Fibrinogen-to-Albumin Ratio and Prognosis of Hospitalized Patients with COVID-19: A Systematic Review and Meta-Analysis. Diagnostics. 2022; 12(7):1678. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12071678
Chicago/Turabian StyleHung, Kuo-Chuan, Yen-Ta Huang, Ying-Jen Chang, Chia-Hung Yu, Li-Kai Wang, Chung-Yi Wu, Ping-Hsin Liu, Sheng-Fu Chiu, and Cheuk-Kwan Sun. 2022. "Association between Fibrinogen-to-Albumin Ratio and Prognosis of Hospitalized Patients with COVID-19: A Systematic Review and Meta-Analysis" Diagnostics 12, no. 7: 1678. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12071678