
Serum Periostin May Help to Identify Patients with Poor Collaterals in the Hyperacute Phase of Ischemic Stroke

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
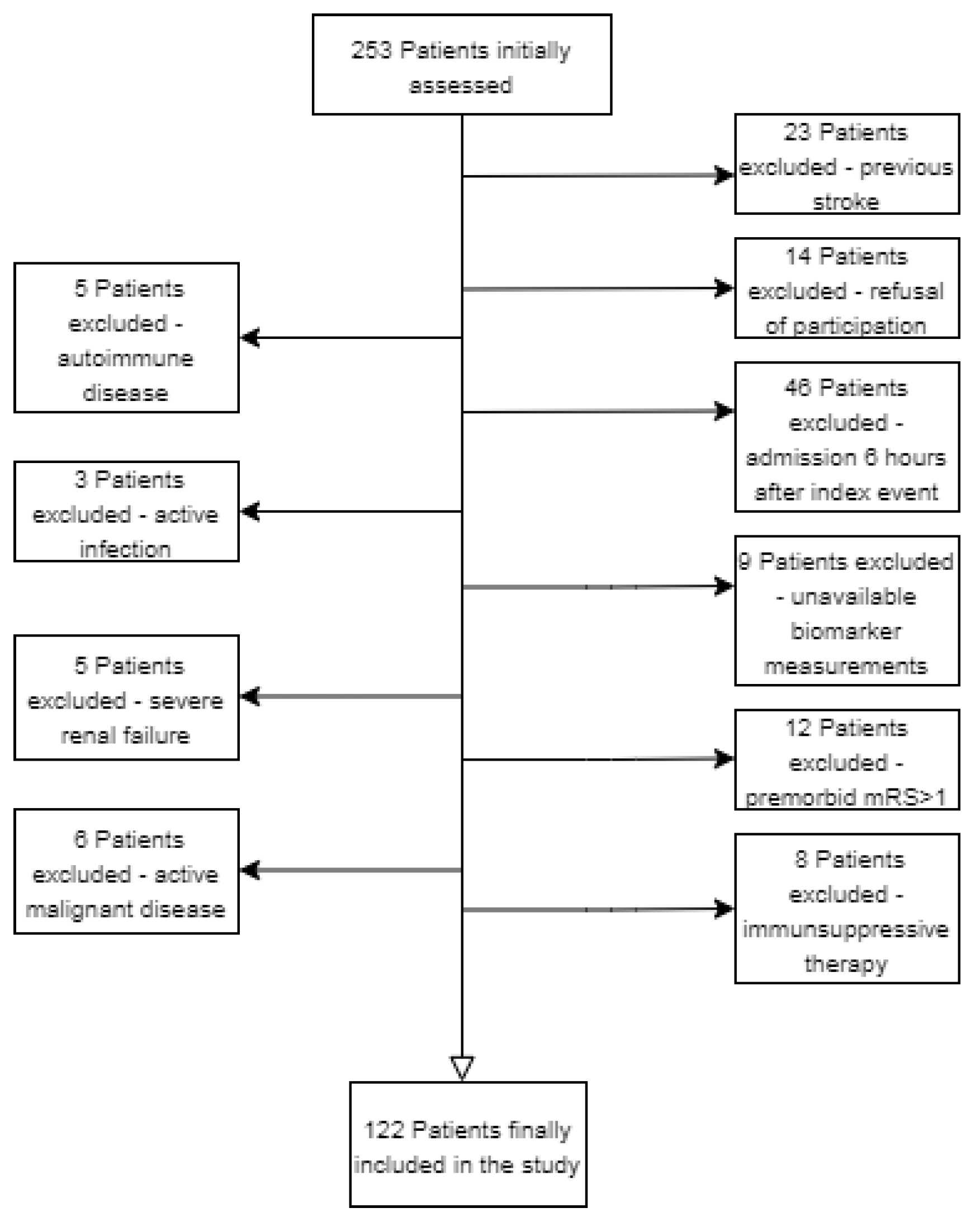
2.1. Participants
2.2. Clinical Protocol
2.3. Laboratory Analysis
2.4. Statistical Analysis
3. Results
3.1. Clinical Characteristics
3.2. Admission Periostin Level, Comorbidities and Outcome
3.3. Variables Associated with Poor Collaterals
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Donnan, G.A.; Fisher, M.; Macleod, M.; Davis, S.M. Stroke. Lancet 2008, 371, 1612–1623. [Google Scholar] [CrossRef]
- Jin, R.; Yang, G.; Li, G. Inflammatory mechanisms in ischemic stroke: Role of inflammatory cells. J. Leukoc. Biol. 2010, 87, 779–789. [Google Scholar] [CrossRef] [PubMed]
- Järveläinen, H.; Sainio, A.; Koulu, M.; Wight, T.N.; Penttinen, R. Extracellular Matrix Molecules: Potential Targets in Pharmacotherapy. Pharmacol. Rev. 2009, 61, 198–223. [Google Scholar] [CrossRef] [PubMed]
- Liu, A.Y.; Zheng, H.; Ouyang, G. Periostin, a multifunctional matricellular protein in inflammatory and tumor microenvironments. Matrix Biol. 2014, 37, 150–156. [Google Scholar] [CrossRef]
- Kühn, B.; Del Monte, F.; Hajjar, R.J.; Chang, Y.S.; Lebeche, D.; Arab, S.; Keating, M.T. Periostin induces proliferation of differentiated cardiomyocytes and promotes cardiac repair. Nat. Med. 2007, 13, 962–969. [Google Scholar] [CrossRef]
- Izuhara, K.; Conway, S.J.; Moore, B.B.; Matsumoto, H.; Holweg, C.T.J.; Matthews, J.G.; Arron, J.R. Roles of Periostin in Respiratory Disorders. Am. J. Respir. Crit. Care Med. 2016, 193, 949–956. [Google Scholar] [CrossRef]
- Conway, S.J.; Izuhara, K.; Kudo, Y.; Litvin, J.; Markwald, R.; Ouyang, G.; Arron, J.; Holweg, C.T.J.; Kudo, A. The role of periostin in tissue remodeling across health and disease. Cell. Mol. Life Sci. 2014, 71, 1279–1288. [Google Scholar] [CrossRef]
- Dorn, G.W., 2nd. Periostin and myocardial repair, regeneration, and recovery. N. Engl. J. Med. 2007, 357, 1552–1554. [Google Scholar] [CrossRef]
- Shimamura, M.; Taniyama, Y.; Katsuragi, N.; Koibuchi, N.; Kyutoku, M.; Sato, N.; Allahtavakoli, M.; Wakayama, K.; Nakagami, H.; Morishita, R. Role of central nervous system periostin in cerebral ischemia. Stroke 2012, 43, 1108–1114. [Google Scholar] [CrossRef]
- Luo, W.; Wang, H.; Hu, J. Increased concentration of serum periostin is associated with poor outcome of patients with aneurysmal subarachnoid hemorrhage. J. Clin. Lab. Anal. 2018, 32, e22389. [Google Scholar] [CrossRef]
- He, X.; Bao, Y.; Shen, Y.; Wang, E.; Hong, W.; Ke, S.; Jin, X. Longitudinal evaluation of serum periostin levels in patients after large-artery atherosclerotic stroke: A prospective observational study. Sci. Rep. 2018, 8, 11729. [Google Scholar] [CrossRef] [PubMed]
- Seker, F.; Potreck, A.; Möhlenbruch, M.; Bendszus, M.; Pham, M. Comparison of four different collateral scores in acute ischemic stroke by CT angiography. J. Neurointerv. Surg. 2016, 8, 1116–1118. [Google Scholar] [CrossRef] [PubMed]
- Dehkharghani, S.; Bammer, R.; Straka, M.; Bowen, M.; Allen, J.W.; Rangaraju, S.; Kang, J.; Gleason, T.; Brasher, C.; Nahab, F. Performance of CT ASPECTS and Collateral Score in Risk Stratification: Can Target Perfusion Profiles Be Predicted without Perfusion Imaging? AJNR 2016, 37, 1399–1404. [Google Scholar] [CrossRef] [PubMed]
- Nannoni, S.; Sirimarco, G.; Cereda, C.W.; Lambrou, D.; Strambo, D.; Eskandari, A.; Mosimann, P.J.; Wintermark, M.; Michel, P. Determining factors of better leptomeningeal collaterals: A study of 857 consecutive acute ischemic stroke patients. J. Neurol. 2019, 266, 582–588. [Google Scholar] [CrossRef]
- Raza, S.A.; Barreira, C.M.; Rodrigues, G.M.; Frankel, M.R.; Haussen, D.C.; Nogueira, R.G.; Rangaraju, S. Prognostic importance of CT ASPECTS and CT perfusion measures of infarction in anterior emergent large vessel occlusions. J. Neurointerv. Surg. 2019, 11, 670–674. [Google Scholar] [CrossRef]
- Nogueira, R.G.; Jadhav, A.P.; Haussen, D.C.; Bonafe, A.; Budzik, R.F.; Bhuva, P.; Yavagal, D.R.; Ribo, M.; Cognard, C.; Hanel, R.; et al. Thrombectomy 6 to 24 Hours after Stroke with a Mismatch between Deficit and Infarct. NEJM 2018, 378, 11–21. [Google Scholar] [CrossRef]
- Albers, G.W.; Marks, M.P.; Kemp, S.; Christensen, S.; Tsai, J.P.; Ortega-Gutierrez, S.; McTaggart, R.A.; Torbey, M.T.; Kim-Tenser, M.; Leslie-Mazwi, T.; et al. Thrombectomy for Stroke at 6 to 16 Hours with Selection by Perfusion Imaging. NEJM 2018, 378, 708–718. [Google Scholar] [CrossRef]
- Matsunaga, E.; Nambu, S.; Oka, M.; Tanaka, M.; Taoka, M.; Iriki, A. Periostin, a neurite outgrowth-promoting factor, is expressed at high levels in the primate cerebral cortex. Dev. Growth Differ. 2015, 57, 200–208. [Google Scholar] [CrossRef]
- Ma, S.M.; Chen, L.X.; Lin, Y.F.; Yan, H.; Lv, J.W.; Xiong, M.; Li, J.; Cheng, G.Q.; Yang, Y.; Qiu, Z.L.; et al. Periostin Promotes Neural Stem Cell Proliferation and Differentiation following Hypoxic-Ischemic Injury. PLoS ONE 2015, 10, e0123585. [Google Scholar] [CrossRef]
- Dong, X.Q.; Yu, W.H.; Du, Q.; Wang, H.; Zhu, Q.; Yang, D.B.; Che, Z.H.; Shen, Y.F.; Jiang, L. Serum periostin concentrations and outcomes after severe traumatic brain injury. Clin. Chim. Acta 2017, 471, 298–303. [Google Scholar] [CrossRef]
- Ji, W.J.; Chou, X.M.; Wu, G.Q.; Shen, Y.F.; Yang, X.G.; Wang, Z.F.; Lan, L.X.; Shi, X.G. Association between serum periostin concentrations and outcome after acute spontaneous intracerebral hemorrhage. Clin. Chim. Acta 2017, 474, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Latroche, C.; Weiss-Gayet, M.; Muller, L.; Gitiaux, C.; Leblanc, P.; Liot, S.; Ben-Larbi, S.; Abou-Khalil, R.; Verger, N.; Bardot, P.; et al. Coupling between Myogenesis and Angiogenesis during Skeletal Muscle Regeneration Is Stimulated by Restorative Macrophages. Stem Cell Rep. 2017, 9, 2018–2033. [Google Scholar] [CrossRef] [PubMed]
- Jiang, W.; Hu, W.; Ye, L.; Tian, Y.; Zhao, R.; Du, J.; Shen, B.; Wang, K. Contribution of Apelin-17 to Collateral Circulation Following Cerebral Ischemic Stroke. Transl. Stroke Res. 2019, 10, 298–307. [Google Scholar] [CrossRef] [PubMed]
- Turc, G.; Bhogal, P.; Fischer, U.; Khatri, P.; Lobotesis, K.; Mazighi, M.; Schellinger, P.D.; Toni, D.; De Vries, J.; White, P.; et al. European Stroke Organisation (ESO)—European Society for Minimally Invasive Neurological Therapy (ESMINT) Guidelines on Mechanical Thrombectomy in Acute Ischemic Stroke. J. Neurointerv. Surg. 2019, 11, 535–538. [Google Scholar] [CrossRef]
- Liu, L.; Kawakita, F.; Fujimoto, M.; Nakano, F.; Imanaka-Yoshida, K.; Yoshida, T.; Suzuki, H. Role of Periostin in Early Brain Injury After Subarachnoid Hemorrhage in Mice. Stroke 2017, 48, 1108–1111. [Google Scholar] [CrossRef]
- Lux, D.; Alakbarzade, V.; Bridge, L.; Clark, C.; Clarke, B.; Zhang, L.; Khan, U.; Pereira, A.C. The association of neutrophil-lymphocyte ratio and lymphocyte-monocyte ratio with 3-month clinical outcome after mechanical thrombectomy following stroke. J. Neuroinflamm. 2020, 17, 60. [Google Scholar] [CrossRef]
- Molnar, T.; Papp, V.; Banati, M.; Szereday, L.; Pusch, G.; Szapary, L.; Bogar, L.; Illes, Z. Relationship between C-reactive protein and early activation of leukocytes indicated by leukocyte antisedimentation rate (LAR) in patients with acute cerebrovascular events. Clin. Hemorheol. Microcirc. 2010, 44, 183–192. [Google Scholar] [CrossRef]
- Mael-Ainin, M.; Abed, A.; Conway, S.J.; Dussaule, J.-C.; Chatziantoniou, C. Inhibition of periostin expression protects against the development of renal inflammation and fibrosis. J. Am. Soc. Nephrol. 2014, 25, 1724–1736. [Google Scholar] [CrossRef]
- Liu, W.; Zi, M.; Tsui, H.; Chowdhury, S.K.; Zeef, L.; Meng, Q.J.; Travis, M.; Prehar, S.; Berry, A.; Hanley, N.A.; et al. A novel immunomodulator, FTY-720 reverses existing cardiac hypertrophy and fibrosis from pressure overload by targeting NFAT (nuclear factor of activated T-cells) signaling and periostin. Circ. Heart Fail. 2013, 6, 833–844. [Google Scholar] [CrossRef]
- Wu, H.; Xie, J.; Li, G.N.; Chen, Q.H.; Li, R.; Zhang, X.L.; Kang, L.N.; Xu, B. Possible involvement of TGF-β/periostin in fibrosis of right atrial appendages in patients with atrial fibrillation. Int. J. Clin. Exp. Pathol. 2015, 8, 6859–6869. [Google Scholar]
- Azharuddin, M.; Adil, M.; Ghosh, P.; Kapur, P.; Sharma, M. Periostin as a novel biomarker of cardiovascular disease: A systematic evidence landscape of preclinical and clinical studies. J. Evid. Based Med. 2019, 12, 325–336. [Google Scholar] [CrossRef] [PubMed]
- Csecsei, P.; Pusch, G.; Ezer, E.; Berki, T.; Szapary, L.; Illes, Z.; Molnar, T. Relationship between Cardiac Troponin and Thrombo-Inflammatory Molecules in Prediction of Outcome after Acute Ischemic Stroke. J. Stroke Cerebrovasc. Dis. 2018, 27, 951–956. [Google Scholar] [CrossRef] [PubMed]
- Rudilosso, S.; Rodríguez-Vázquez, A.; Urra, X.; Arboix, A. The Potential Impact of Neuroimaging and Translational Research on the Clinical Management of Lacunar Stroke. Int. J. Mol. Sci. 2022, 23, 1497. [Google Scholar] [CrossRef] [PubMed]
- Segers, V.F.M.; Brutsaert, D.L.; De Keulenaer, G.W. Cardiac Remodeling: Endothelial Cells Have More to Say Than Just NO. Front. Physiol. 2018, 9, 382. [Google Scholar] [CrossRef] [PubMed]
- Schranz, D.; Molnar, T.; Erdo-Bonyar, S.; Simon, D.; Berki, T.; Nagy, C.; Czeiter, E.; Buki, A.; Lenzser, G.; Csecsei, P. Increased level of LIGHT/TNFSF14 is associated with survival in aneurysmal subarachnoid hemorrhage. Acta Neurol. Scand. 2021, 143, 530–537. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total (n = 122) | Favorable * Outcome (n = 59) | Unfavorable * Outcome (n = 63) | p-Value |
|---|---|---|---|---|
| Age, y, median (IQR) | 71 (63–79) | 71 (62–77) | 73 (64–79) | 0.127 |
| Male, n (%) | 74 (60.7%) | 35 (59.3%) | 39 (61.9%) | 0.770 |
| Hypertension, n (%) | 100 (82%) | 48 (81.4%) | 52 (82.5%) | 0.865 |
| Diabetes, n (%) | 35 (28.7%) | 17 (28.8%) | 18 (28.6%) | 0.976 |
| Smoking, n (%) | 52 (38%) | 19 (32.2%) | 33 (52.4%) | 0.024 * |
| Atrial fibrillation, n (%) | 34 (27.9%) | 7 (11.9%) | 27 (42.9%) | <0.001 * |
| Large artery atherosclerosis, n (%) | 59 (48.4%) | 35 (59.3%) | 24 (38.1%) | 0.029 |
| Lacunar, n (%) | 23 (18.9%) | 13 (22%) | 10 (15.8%) | 0.385 |
| Other, n (%) | 4 (3.3%) | 3 (5.1%) | 1 (1.6%) | 0.278 |
| Undetermined, n (%) | 2 (1.5%) | 1 (1.7%) | 1 (1.7%) | 0.899 |
| GCS, median (IQR) | 15 (12–15) | 15 (15) | 14 (11–15) | <0.001 * |
| NIHSS, median (IQR) | 8 (5–16) | 6 (4–8) | 13 (8–19) | <0.001 * |
| SBP, median (IQR) | 150 (130–170) | 148 (130–170) | 160 (138–180) | 0.237 |
| DBP, median (IQR) | 84 (80–94) | 82 (80–90) | 86 (80–100) | 0.463 |
| ASPECTs, median (IQR) | 9 (7–10) | 10 (9–10) | 8 (6–9) | <0.001 * |
| WBC, median (IQR) | 8.4 (6.9–10.7) | 7.7 (9–10) | 8.8 (7–11) | 0.264 |
| NLR, median (IQR) | 2.9 (2–5.6) | 2.5 (1.7) | 3.6 (2.5–7.3) | 0.002 * |
| platelet, median (IQR) | 242 (188–306) | 245 (196–300) | 238 (185–305) | 0.625 |
| creatinine, median (IQR) | 86 (73–102) | 83 (70–97) | 87 (74–104) | 0.411 |
| glucose, median (IQR) | 7.2 (6.2–8.9) | 6.8 (5.9–8.1) | 7.8 (6.8–9) | 0.004 * |
| CRP, median (IQR) | 3.7 (1.4–9.5) | 2.6 (1.4–5.4) | 5.1 (1.7–16) | 0.042 * |
| Thrombectomy, n (%) | 29 (23.8) | 14 (23.7) | 15 (23.8) | 0.856 |
| Intravenous tPA, n (%) | 51 (41.8) | 28 (47.5) | 23 (36.5) | 0.190 |
| Thrombectomy plus intravenous tPA, n (%) | 17 (13.9) | 6 (10.2) | 11 (17.5) | 0.260 |
| Conservative, n (%) | 25 (20.5) | 11 (18.6) | 14 (22.2) | 0.658 |
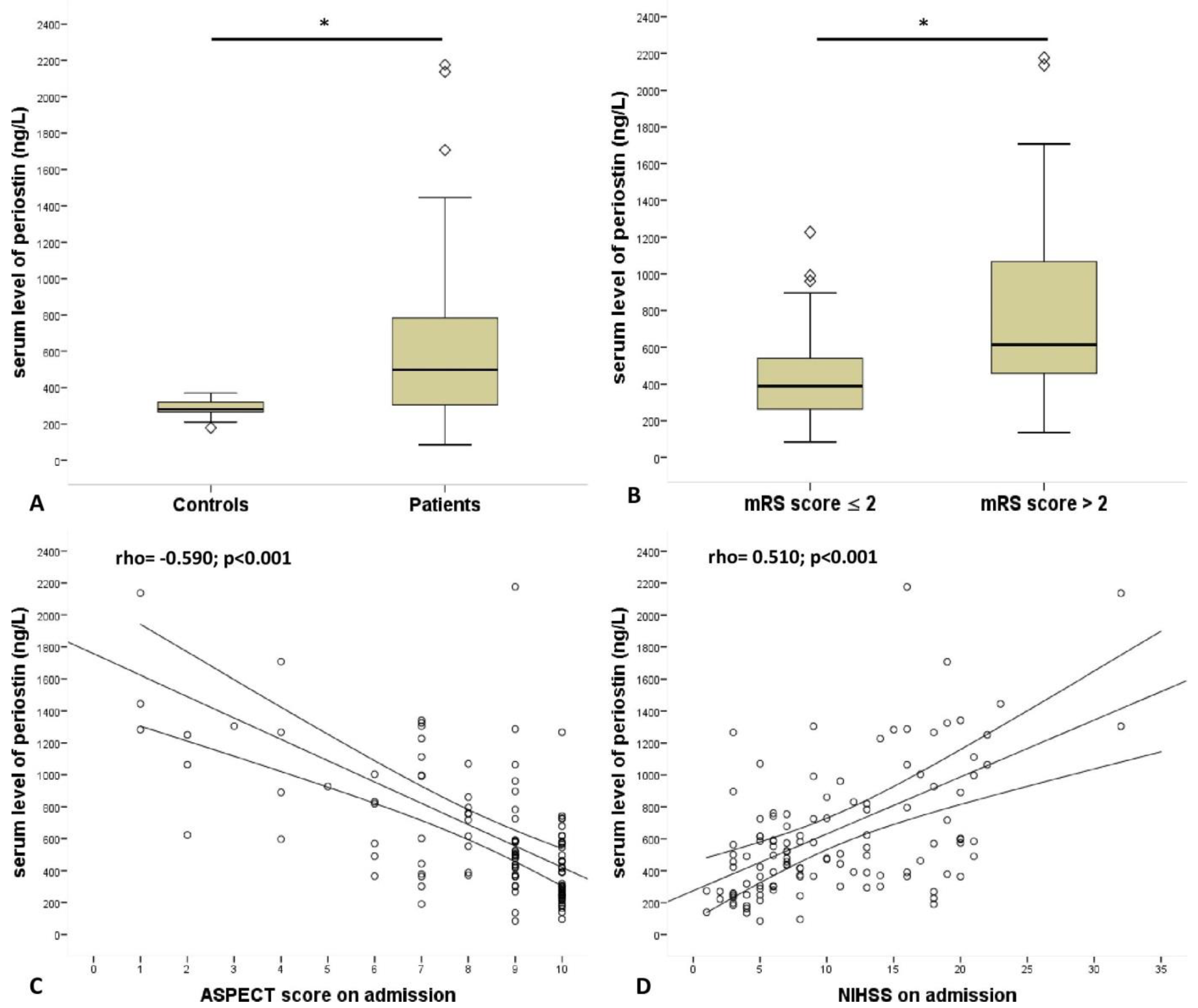
| serum level of periostin, median (IQR), ng/L | 462 (297–735) | 390 (260–563) | 615 (443–1070) | <0.001 * |
| Variable | Spearman Correlation Coefficient (r) | p-Value |
|---|---|---|
| Atrial fibrillation | 0.335 | <0.001 |
| Systolic blood pressure | 0.068 | 0.459 |
| Diastolic blood pressure | 0.119 | 0.193 |
| Glasgow Coma Scale | −0.308 | <0.001 |
| ASPECT score | −0.590 | <0.001 |
| White blood cell count, G/L | 0.239 | 0.01 |
| Neutrophil-lymphocyte ratio | 0.328 | <0.001 |
| Creatinine, µmol/L | 0.277 | 0.003 |
| C-reactive protein, mg/L | 0.285 | 0.002 |
| Glucose, mmol/L | 0.257 | 0.007 |
| Platelet, G/L | −0.059 | 0.534 |
| Carbamide, mmol/L | 0.245 | 0.01 |
| Odds Ratio | 95% CI | p-Value | |
|---|---|---|---|
| periostin | 15.532 | 0.995–0.998 | <0.001 |
| Model 1 | 6.339 | 0.995–0.999 | 0.012 |
| Model 2 | 5.917 | 0.993–0.999 | 0.015 |
| Model 3 | 5.911 | 0.990–0.999 | 0.015 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spantler, D.; Csecsei, P.; Borocz, K.; Berki, T.; Zavori, L.; Schwarcz, A.; Lenzser, G.; Molnar, T. Serum Periostin May Help to Identify Patients with Poor Collaterals in the Hyperacute Phase of Ischemic Stroke. Diagnostics 2022, 12, 1942. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12081942
Spantler D, Csecsei P, Borocz K, Berki T, Zavori L, Schwarcz A, Lenzser G, Molnar T. Serum Periostin May Help to Identify Patients with Poor Collaterals in the Hyperacute Phase of Ischemic Stroke. Diagnostics. 2022; 12(8):1942. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12081942
Chicago/Turabian StyleSpantler, Dora, Peter Csecsei, Katalin Borocz, Timea Berki, Laszlo Zavori, Attila Schwarcz, Gabor Lenzser, and Tihamer Molnar. 2022. "Serum Periostin May Help to Identify Patients with Poor Collaterals in the Hyperacute Phase of Ischemic Stroke" Diagnostics 12, no. 8: 1942. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12081942