
Comparison of Diagnostic Performance of Ultrasonography and Magnetic Resonance Enterography in the Assessment of Active Bowel Lesions in Patients with Crohn’s Disease: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Study Selection
2.3. Data Extraction and Quality Assessment
2.4. Data Synthesis and Analysis
2.5. Meta-Regression Analyses
3. Results
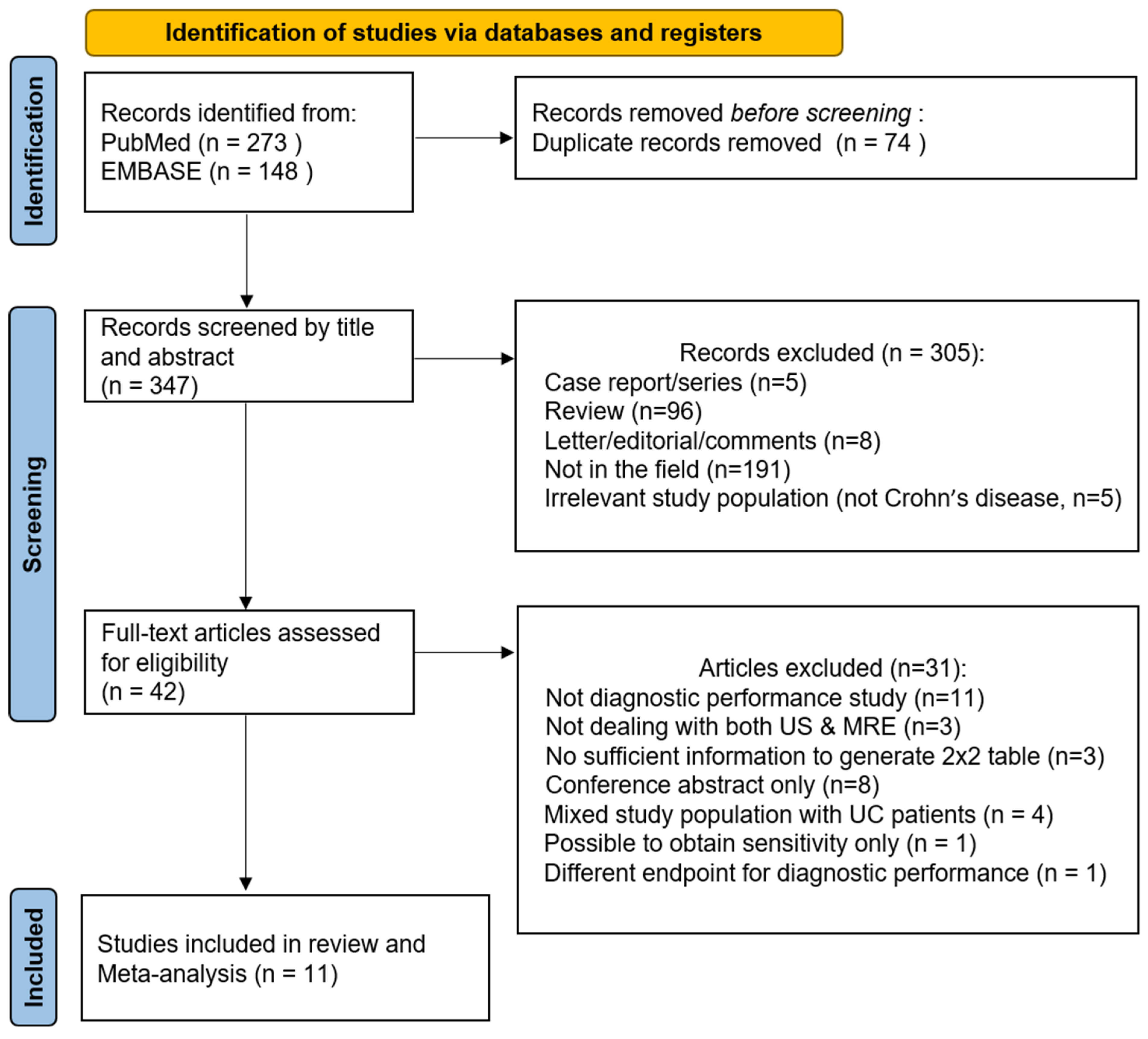
3.1. Literature Search
3.2. Characteristics of the Studies and the Included Patients
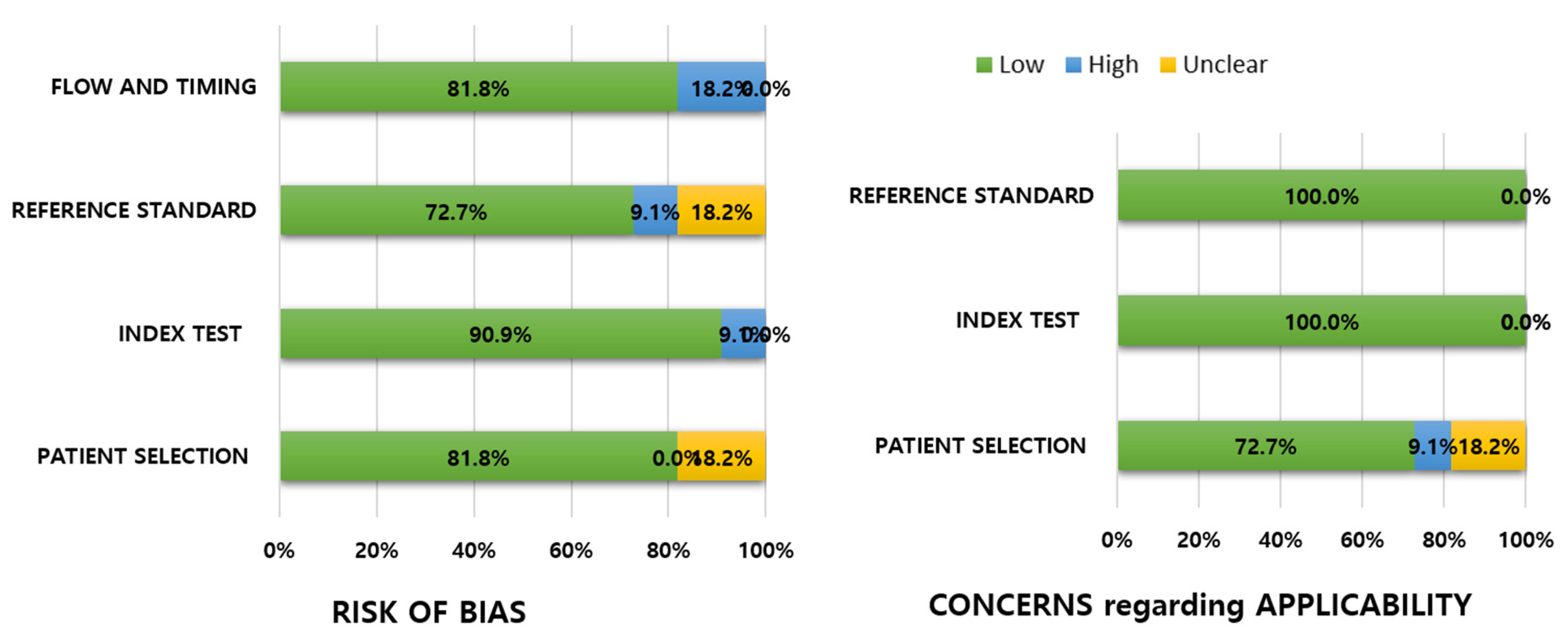
3.3. Quality of Studies
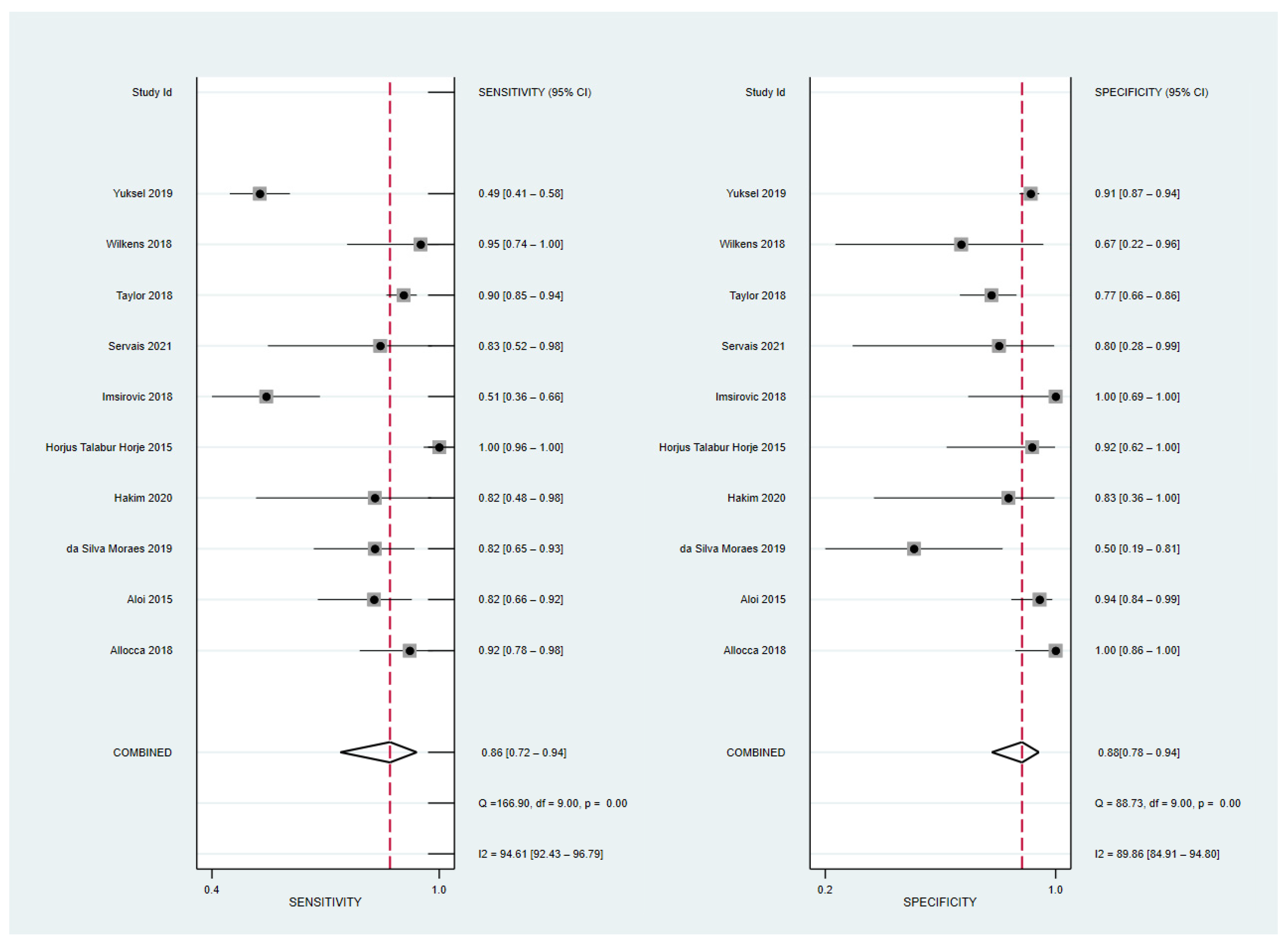
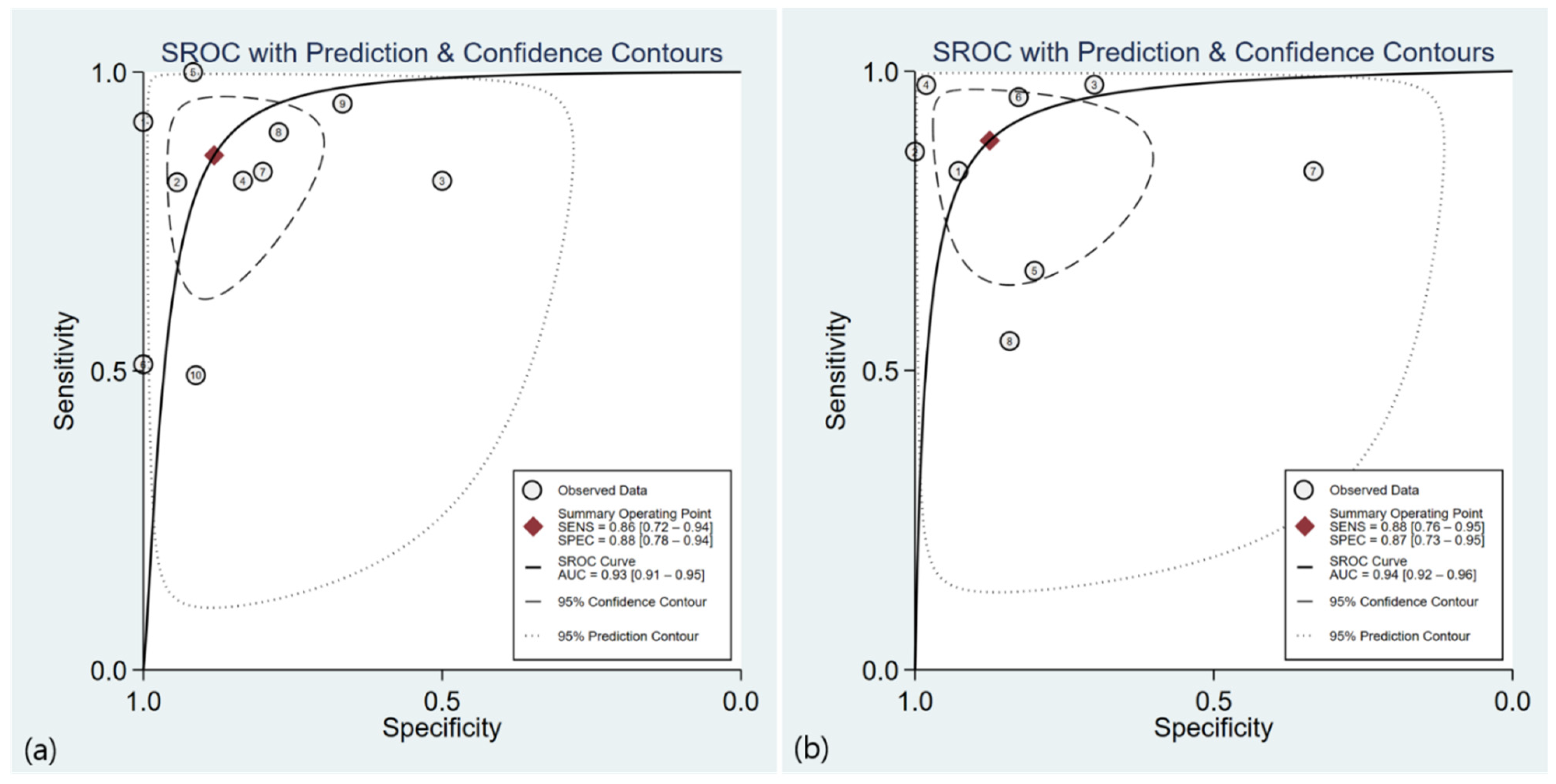
3.4. Diagnostic Performance of US
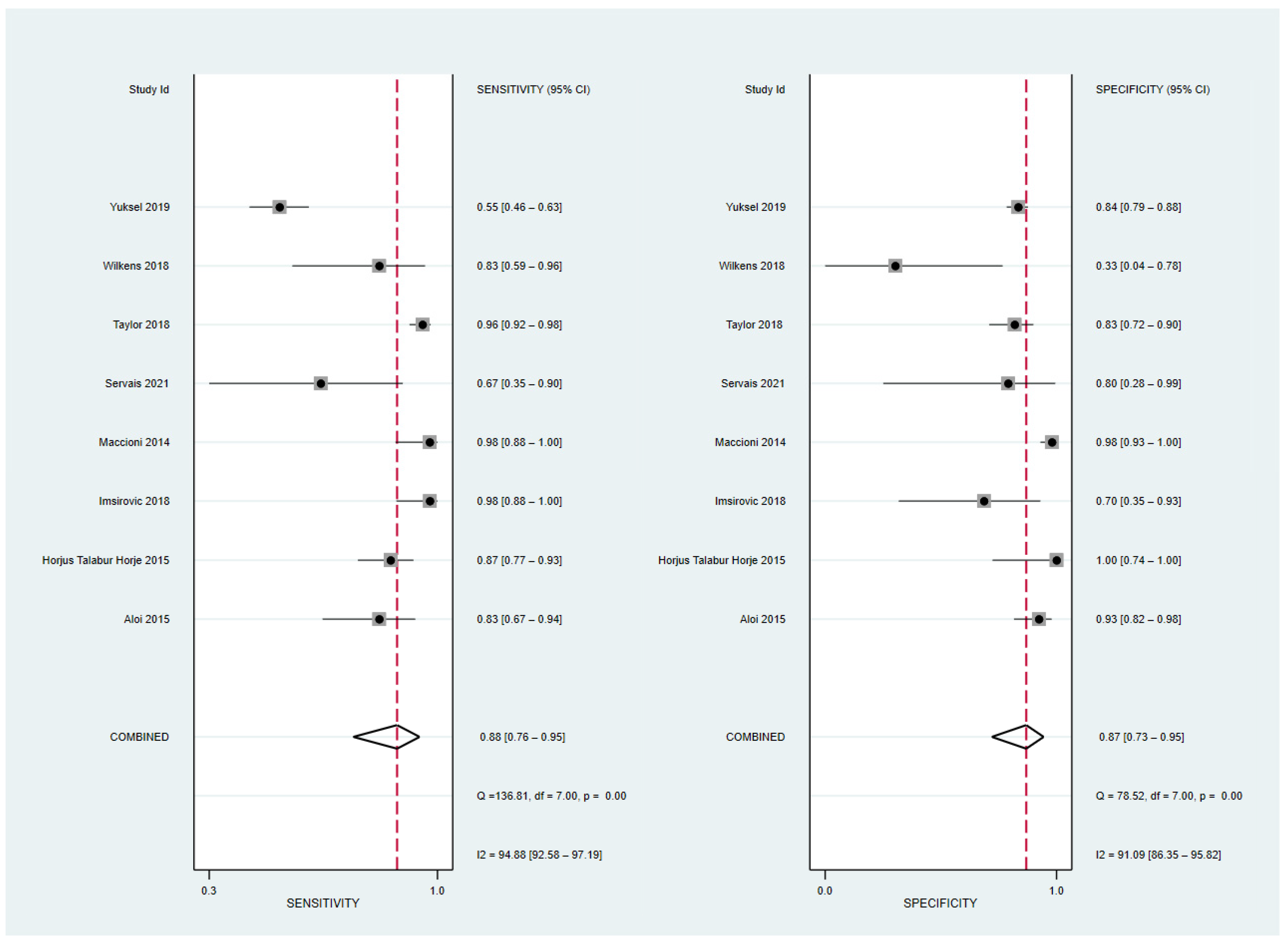
3.5. Diagnostic Performance of MRE
3.6. Meta-Regression Analyses
3.7. Comparison of Diagnostic Performance of US and MRE in Diagnosing Active Bowel Lesions
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Panes, J.; Bouhnik, Y.; Reinisch, W.; Stoker, J.; Taylor, S.A.; Baumgart, D.C.; Danese, S.; Halligan, S.; Marincek, B.; Matos, C.; et al. Imaging techniques for assessment of inflammatory bowel disease: Joint ECCO and ESGAR evidence-based consensus guidelines. J. Crohns Colitis 2013, 7, 556–585. [Google Scholar] [CrossRef] [PubMed]
- Sauer, C.G.; Kugathasan, S.; Martin, D.R.; Applegate, K.E. Medical radiation exposure in children with inflammatory bowel disease estimates high cumulative doses. Inflamm. Bowel Dis. 2011, 17, 2326–2332. [Google Scholar] [CrossRef] [PubMed]
- Qiu, Y.; Mao, R.; Chen, B.L.; Li, X.H.; He, Y.; Zeng, Z.R.; Li, Z.-P.; Chen, M.-H. Systematic review with meta-analysis: Magnetic resonance enterography vs. computed tomography enterography for evaluating disease activity in small bowel Crohn’s disease. Aliment. Pharmacol. Ther. 2014, 40, 134–146. [Google Scholar] [CrossRef]
- Liu, W.; Liu, J.; Xiao, W.; Luo, G. A Diagnostic Accuracy Meta-analysis of CT and MRI for the Evaluation of Small Bowel Crohn Disease. Acad. Radiol. 2017, 24, 1216–1225. [Google Scholar] [CrossRef] [PubMed]
- Minordi, L.M.; Larosa, L.; Papa, A.; Cimino, G.; Bevere, A.; Brizi, M.G.; Manfredi, R. A review of Magnetic Resonance Enterography classification and quantitative evaluation of active disease in patients with Crohn’s disease. Clin. Imaging 2021, 69, 50–62. [Google Scholar] [CrossRef] [PubMed]
- Mainenti, P.P.; Castiglione, F.; Rispo, A.; Laccetti, E.; Guarino, S.; Romeo, V.; Testa, A.; Pace, L.; Maurea, S. MR-enterography in Crohn’s disease: What MRE mural parameters are associated to one-year therapeutic management outcome? Br. J. Radiol. 2021, 94, 20200844. [Google Scholar] [CrossRef]
- Stenczel, N.D.; Purcarea, M.R.; Tribus, L.C.; Oniga, G.H. The role of the intestinal ultrasound in Crohn’s disease diagnosis and monitoring. J. Med. Life 2021, 14, 310–315. [Google Scholar] [CrossRef]
- Pascu, M.; Roznowski, A.B.; Müller, H.P.; Adler, A.; Wiedenmann, B.; Dignass, A.U. Clinical relevance of transabdominal ultrasonography and magnetic resonance imaging in patients with inflammatory bowel disease of the terminal ileum and large bowel. Inflamm. Bowel Dis. 2004, 10, 373–382. [Google Scholar] [CrossRef]
- Miao, Y.M.; Koh, D.M.; Amin, Z.; Healy, J.C.; Chinn, R.J.S.; Zeegen, R.; Westaby, D. Ultrasound and Magnetic Resonance Imaging Assessmentof Active Bowel Segments in Crohn’s Disease. Clin. Radiol. 2002, 57, 913–918. [Google Scholar] [CrossRef]
- McInnes, M.D.F.; Moher, D.; Thombs, B.D.; McGrath, T.A.; Bossuyt, P.M.; Clifford, T.; Cohen, J.F.; Deeks, J.J.; Gatsonis, C.; Hooft, L.; et al. Preferred Reporting Items for a Systematic Review and Meta-analysis of Diagnostic Test Accuracy Studies: The PRISMA-DTA Statement. JAMA 2018, 319, 388–396. [Google Scholar] [CrossRef]
- Leeflang, M.M.; Deeks, J.J.; Takwoingi, Y.; Macaskill, P. Cochrane diagnostic test accuracy reviews. Syst. Rev. 2013, 2, 82. [Google Scholar] [CrossRef] [PubMed]
- Trikalinos, T.A.; Balion, C.M.; Coleman, C.I.; Griffith, L.; Santaguida, P.L.; Vandermeer, B.; Fu, R. Meta-Analysis of Test Performance When There Is a “Gold Standard”. In Methods Guide for Medical Test Reviews; Chang, S.M., Matchar, D.B., Smetana, G.W., Umscheid, C.A., Eds.; AHRQ Methods for Effective Health Care: Rockville, MD, USA, 2012. [Google Scholar]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.G.; Sterne, J.A.C.; Bossuyt, P.M. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Kim, K.W.; Choi, S.H.; Huh, J.; Park, S.H. Systematic Review and Meta-Analysis of Studies Evaluating Diagnostic Test Accuracy: A Practical Review for Clinical Researchers-Part II. Statistical Methods of Meta-Analysis. Korean J. Radiol. 2015, 16, 1188–1196. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.W.; Lee, J.; Choi, S.H.; Huh, J.; Park, S.H. Systematic Review and Meta-Analysis of Studies Evaluating Diagnostic Test Accuracy: A Practical Review for Clinical Researchers-Part I. General Guidance and Tips. Korean J. Radiol. 2015, 16, 1175–1187. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Allocca, M.; Fiorino, G.; Bonifacio, C.; Furfaro, F.; Gilardi, D.; Argollo, M.; Peyrin-Biroulet, L.; Danese, S. Comparative Accuracy of Bowel Ultrasound Versus Magnetic Resonance Enterography in Combination with Colonoscopy in Assessing Crohn’s Disease and Guiding Clinical Decision-making. J. Crohns Colitis 2018, 12, 1280–1287. [Google Scholar] [CrossRef]
- Aloi, M.; Di Nardo, G.; Romano, G.; Casciani, E.; Civitelli, F.; Oliva, S.; Viola, F.; Maccioni, F.; Gualdi, G.; Cucchiara, S. Magnetic resonance enterography, small-intestine contrast US, and capsule endoscopy to evaluate the small bowel in pediatric Crohn’s disease: A prospective, blinded, comparison study. Gastrointest. Endosc. 2015, 81, 420–427. [Google Scholar] [CrossRef]
- da Silva Moraes, A.C.; de Freitas Moraes, G.; de Araújo, A.L.E.; Luiz, R.R.; Elia, C.; Carneiro, A.J.; de Souza, H.S.P. Abdominal ultrasonography with color Doppler analysis in the assessment of ileal Crohn’s disease: Comparison with magnetic resonance enterography. Intest. Res. 2019, 17, 227–236. [Google Scholar] [CrossRef]
- Hakim, A.; Alexakis, C.; Pilcher, J.; Tzias, D.; Mitton, S.; Paul, T.; Saxena, S.; Pollok, R.; Kumar, S. Comparison of small intestinal contrast ultrasound with magnetic resonance enterography in pediatric Crohn’s disease. JGH Open 2020, 4, 126–131. [Google Scholar] [CrossRef]
- Horje, C.S.H.T.; Bruijnen, R.; Roovers, L.; Groenen, M.J.; Joosten, F.B.; Wahab, P.J. Contrast Enhanced Abdominal Ultrasound in the Assessment of Ileal Inflammation in Crohn’s Disease: A Comparison with MR Enterography. PLoS ONE 2015, 10, e0136105. [Google Scholar]
- Imsirovic, B.; Zerem, E.; Guso, E.; Djedovic, M.; Cengic, A.; Baljic, R.; Merhemic, Z.; Efendic, A. Comparison of conventional ultrasound and contrast enhanced magnetic resonance (MR) enterography in evaluation patients with Crohn’s disease. Acta Inform. Med. 2018, 26, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Maccioni, F.; Al Ansari, N.; Mazzamurro, F.; Civitelli, F.; Viola, F.; Cucchiara, S.; Catalano, C. Detection of Crohn disease lesions of the small and large bowel in pediatric patients: Diagnostic value of MR enterography versus reference examinations. Am. J. Roentgenol. 2014, 203, W533–W542. [Google Scholar] [CrossRef] [PubMed]
- Servais, L.; Boschetti, G.; Meunier, C.; Gay, C.; Cotte, E.; Francois, Y.; Rozieres, A.; Fontaine, J.; Cuminal, L.; Chauvenet, M.; et al. Intestinal Conventional Ultrasonography, Contrast-Enhanced Ultrasonography and Magnetic Resonance Enterography in Assessment of Crohn’s Disease Activity: A Comparison with Surgical Histopathology Analysis. Dig. Dis. Sci. 2022, 67, 2492–2502. [Google Scholar] [CrossRef]
- Taylor, S.A.; Mallett, S.; Bhatnagar, G.; Baldwin-Cleland, R.; Bloom, S.; Gupta, A.; Hamlin, P.J.; Hart, A.L.; Higginson, A.; Jacobs, I.; et al. Diagnostic accuracy of magnetic resonance enterography and small bowel ultrasound for the extent and activity of newly diagnosed and relapsed Crohn’s disease (METRIC): A multicentre trial. Lancet Gastroenterol. Hepatol. 2018, 3, 548–558. [Google Scholar] [CrossRef]
- Wilkens, R.; Hagemann-Madsen, R.H.; Peters, D.A.; Nielsen, A.H.; Nørager, C.B.; Glerup, H.; Krogh, K. Validity of Contrast-enhanced Ultrasonography and Dynamic Contrast-enhanced MR Enterography in the Assessment of Transmural Activity and Fibrosis in Crohn’s Disease. J. Crohns Colitis 2018, 12, 48–56. [Google Scholar] [CrossRef]
- Yuksel, I.; Kilincalp, S.; Coskun, Y.; Akinci, H.; Hamamci, M.; Alkan, A. Diagnostic accuracy of intestinal ultrasound and magnetic resonance enterography for the detection of endoscopy-based disease activity in ileocolonic Crohn’s disease. Eur. J. Gastroenterol. Hepatol. 2019, 31, 809–816. [Google Scholar] [CrossRef]
- Dong, J.; Wang, H.; Zhao, J.; Zhu, W.; Zhang, L.; Gong, J.; Li, Y.; Gu, L.; Li, J. Ultrasound as a diagnostic tool in detecting active Crohn’s disease: A meta-analysis of prospective studies. Eur. Radiol. 2014, 24, 26–33. [Google Scholar] [CrossRef]
- Ahmed, O.; Rodrigues, D.M.; Nguyen, G.C. Magnetic Resonance Imaging of the Small Bowel in Crohn’s Disease: A Systematic Review and Meta-Analysis. Can. J. Gastroenterol. Hepatol. 2016, 2016, 7857352. [Google Scholar] [CrossRef]
- Chavoshi, M.; Mirshahvalad, S.A.; Kasaeian, A.; Djalalinia, S.; Kolahdoozan, S.; Radmard, A.R. Diagnostic Accuracy of Magnetic Resonance Enterography in the Evaluation of Colonic Abnormalities in Crohn’s Disease: A Systematic Review and Meta-Analysis. Acad. Radiol. 2021, 28 (Suppl. 1), S192–S202. [Google Scholar] [CrossRef]
- Giles, E.; Barclay, A.R.; Chippington, S.; Wilson, D.C. Systematic review: MRI enterography for assessment of small bowel involvement in paediatric Crohn’s disease. Aliment. Pharmacol. Ther. 2013, 37, 1121–1131. [Google Scholar] [CrossRef]
- Travis, S.P.; Stange, E.F.; Lemann, M.; Oresland, T.; Chowers, Y.; Forbes, A.; D’Haens, G.; Kitis, G.; Cortot, A.; Prantera, C.; et al. European evidence based consensus on the diagnosis and management of Crohn’s disease: Current management. Gut 2006, 55 (Suppl. 1), i16–i35. [Google Scholar] [CrossRef] [PubMed]
- Biondi, M.; Bicci, E.; Danti, G.; Flammia, F.; Chiti, G.; Palumbo, P.; Bruno, F.; Borgheresi, A.; Grassi, R.; Grassi, F.; et al. The Role of Magnetic Resonance Enterography in Crohn’s Disease: A Review of Recent Literature. Diagnostics 2022, 12, 1236. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Montpetit, E.; Ripollés, T.; Martinez-Pérez, M.J.; Vizuete, J.; Martín, G.; Blanc, E. Ultrasound findings of Crohn’s disease: Correlation with MR enterography. Abdom. Radiol. 2021, 46, 156–167. [Google Scholar] [CrossRef] [PubMed]
- Panés, J.; Bouzas, R.; Chaparro, M.; García-Sánchez, V.; Gisbert, J.P.; de Guereñu, B.M.; Mendoza, J.L.; Paredes, J.M.; Quiroga, S.; Ripollés, T.; et al. Systematic review: The use of ultrasonography, computed tomography and magnetic resonance imaging for the diagnosis, assessment of activity and abdominal complications of Crohn’s disease. Aliment. Pharmacol. Ther. 2011, 34, 125–145. [Google Scholar] [CrossRef] [PubMed]
- Kopylov, U.; Yung, D.E.; Engel, T.; Vijayan, S.; Har-Noy, O.; Katz, L.; Oliva, S.; Avni, T.; Battat, R.; Eliakim, R.; et al. Diagnostic yield of capsule endoscopy versus magnetic resonance enterography and small bowel contrast ultrasound in the evaluation of small bowel Crohn’s disease: Systematic review and meta-analysis. Dig. Liver Dis. 2017, 49, 854–863. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, J.G.; Fidler, J.L.; Bruining, D.H.; Huprich, J.E. New concepts in intestinal imaging for inflammatory bowel diseases. Gastroenterology 2011, 140, 1795–1806. [Google Scholar] [CrossRef]
- Aaltonen, G.; Keränen, I.; Carpelan-Holmström, M.; Savolainen, R.; Lindén, R.; Lepistö, A. Intra-Abdominal Adhesions Make the Interpretation of Magnetic Resonance Enterography in Crohn’s Disease More Difficult. Dig. Surg. 2017, 34, 30–35. [Google Scholar] [CrossRef]
- Ma, X.; Li, Y.; Jia, H.; Zhang, J.; Wang, G.; Liu, X.; Song, Y. Contrast-enhanced ultrasound in the diagnosis of patients suspected of having active Crohn’s disease: Meta-analysis. Ultrasound Med. Biol. 2015, 41, 659–668. [Google Scholar] [CrossRef]
- Cammarota, T.; Sarno, A.; Robotti, D.; Bonenti, G.; Debani, P.; Versace, K.; Astegiano, M.; Pera, A. US evaluation of patients affected by IBD: How to do it, methods and findings. Eur. J. Radiol. 2009, 69, 429–437. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Study Design | Study Region | No. of Patients (n) | No. of Lesions (n) | Method of Analyses | Study Population | Crohn’s Disease status |
|---|---|---|---|---|---|---|---|
| Allocca et al. (2018) [17] | Prospective | Milano, Italy | 60 | Per-patient | Adult > 18 y | Confirmed | |
| Aloi et al. (2015) [18] | Prospective | Rome, Italy | 25 | 91 | Per-segment | Pediatrics | confirmed + suspected |
| da Silva Moraes et al. (2019) [19] | Prospective | Rio de Janeiro, Brazil | 43 | Per-patient | Adult | Confirmed | |
| Hakim et al. (2020) [20] | Retrospective | London, UK | 17 | Per-patient | Pediatrics | Confirmed | |
| Horjus et al. (2015) [21] | Prospective | Arnhem, Netherland | 105 | Per-patient | Adult | confirmed active | |
| Imsirovic et al. (2018) [22] | Prospective | Bosnia and Herzegovina | 55 | Per-patient | Adult | Suspected | |
| Maccioni et al. (2014) [23] | Prospective | Rome, Italy | 50 | 150 | Per-segment | Pediatrics | Confirmed |
| Servais et al. (2021) [24] | Prospective | Lyon, France | 17 | Per-patient | Adult > 18 y | Confirmed | |
| Taylor et al. (2018) [25] | Prospective | London, UK | 284 | Per-patient | Adult > 16 y | Newly diagnosed + relapsed | |
| Wilkens et al. (2018) [26] | Prospective | Silkeborg, Denmark | 25 | Per-patient | Adult > 18 y | Confirmed | |
| Yuksel et al. (2019) [27] | Prospective | Ankara, Turkey | 71 | 426 | Per-segment | Adult | Confirmed |
| Author | Index Test | US Probe | Comparator | MR Magnet T | Blinding | Reference Standards | Outcome Variable |
|---|---|---|---|---|---|---|---|
| Allocca 2018 [17] | US | 1–5 MHz (convex), 4–8 MHz (linear) | 1.5 | yes | Colonoscopy + MRE | active disease in terminal ileum and colon | |
| Aloi 2015 [18] | SICUS | 3.5 MHz (convex), 5 MHz (linear) | MRE | 1.5 | yes | Panel consensus dx + Colonoscopy | active small bowel disease |
| da Silva Moraes 2019 [19] | US | 10–12 MHz(linear), 5–10 MHz(convex) | Clinical HBI | 1.5 | yes | MRE | active ileal disease |
| Hakim 2020 [20] | SICUS | 3–9 MHz (convex) 6–11 MHz (linear) | 1.5 | NR | MRE | active small bowel lesion | |
| Horjus 2015 [21] | CEUS using Sonovue | 7.5 MHz (linear) | MRE | 1.5 | yes | Colonoscopy | active bowel lesion in terminal ileum |
| Imsirovic 2018 [22] | US | 3.5 MHz (convex), 7 MHz (linear) | MRE | 1.5 | NR | Colonoscopy + pathology | bowel wall thickening in terminal ileum and colon |
| Maccioni 2014 [23] | MRE | 7.5 MHz (linear) | 1.5 | yes | HRUS+ colonoscopy | localization of active small bowel lesion | |
| Servais 2021 [24] | US | 14 MHz (linear) 6 MHz(convex) | MRE | 1.5 | yes | Pathology | severe active small bowel lesion |
| Taylor 2018 [25] | US | 2–5 MHz(convex), >5 MHz (linear) | MRE | 1.5/3 | yes | Panel consensus dx | active small bowel disease |
| Wilkens 2018 [26] | US | 9 L4 probe (linear) | MRE | 1.5 | yes | Pathology | ulcer in small bowel |
| Yuksel 2019 [27] | US | 3.5–5.5 MHz 7–12 MHz (linear) | MRE | 1.5 | yes | Colonoscopy | bowel wall thickening in terminal ileum and colon |
| Covariate | Subgroup | No. of Studies | Meta-Analytic Summary Estimates | |||
|---|---|---|---|---|---|---|
| Sensitivity (95% CI) | p Value | Specificity (95% CI) | p Value | |||
| Study design | Prospective | 9 | 86% (75,97) | 0.63 | 88% (80,96) | 0.66 |
| Retrospective | 1 | 84% (44,100) | 85% (50,100) | |||
| Total no. of patients | ≥30 | 6 | 85% (71,99) | 0.94 | 89% (79,98) | 0.56 |
| <30 | 4 | 88% (73,100) | 87% (72,100) | |||
| Study region | Europe | 7 | 91% (85,97) | 0.002 * | 88% (76,94) | 0.38 |
| Not Europe | 3 | 61% (40,83) | 85% (71,100) | |||
| Study population | Adult | 8 | 87% (76,98) | 0.92 | 87% (77,96) | 0.58 |
| Pediatrics | 2 | 82% (68,90) | 93% (83,97) | |||
| Crohn’s disease status | Confirmed CD | 7 | 90% (80,99) | 0.14 | 85% (75,95) | 0.38 |
| Including suspected CD | 3 | 71% (50,86) | 94% (86,98) | |||
| Reference standards | Including MRE | 3 | 87% (80,94) | 0.82 | 85% (68,100) | 0.99 |
| Others | 7 | 86% (73,98) | 89% (80,97) | |||
| Type of US | Conventional US | 7 | 83% (67,92) | 0.26 | 85% (60,95) | 0.36 |
| SICUS/CEUS | 3 | 95% (60,100) | 93% (84,97) | |||
| Type of US probe | Both linear and convex | 8 | 79% (68,90) | 0.01 * | 89% (81,97) | 0.68 |
| Linear | 2 | 99% (97,100) | 84% (60,95) | |||
| Method of outcome analysis | Per patient | 8 | 90% (82,98) | 0.11 | 83% (73,94) | 0.97 |
| Per segment | 2 | 67% (32,100) | 93% (86,100) | |||
| Lesion location | Small bowel | 7 | 91% (85,98) | 0.01 * | 83% (71,94) | 0.19 |
| Small and large bowels | 3 | 67% (43,91) | 96% (90,100) | |||
| Outcome variable | Combined features | 7 | 90% (84,97) | 0.01 * | 87% (77,97) | 0.92 |
| One feature | 3 | 67% (41,92) | 90% (78,100) | |||
| Covariate | Subgroup | No. of Studies | Meta-Analytic Summary Estimates | |||
|---|---|---|---|---|---|---|
| Sensitivity (95% CI) | p Value | Specificity (95% CI) | p Value | |||
| Total no. of patients | ≥30 | 5 | 92% (76,98) | 0.26 | 91% (77,97) | 0.31 |
| <30 | 3 | 80% (69,88) | 78% (39,95) | |||
| Study region | Europe | 6 | 90% (81,95) | 0.62 | 90% (70,97) | 0.41 |
| Not Europe | 2 | 87% (32,99) | 84% (79,87) | |||
| Study population | Adult | 6 | 87% (70,95) | 0.46 | 83% (79,87) | 0.0002 * |
| Pediatrics | 2 | 93% (74,98) | 96% (91,99) | |||
| Crohn’s disease status | Confirmed CD | 6 | 87% (70,95) | 0.45 | 88% (67,96) | 0.89 |
| Including suspected CD | 2 | 93% (74,98) | 88% (67,96) | |||
| Reference standards | Others | 7 | 86% (76,96) | 0.42 | 84% (80,88) | 0.001 * |
| Including US | 1 | 98% (93,100) | 98% (96,100) | |||
| Type of US | Conventional US | 6 | 90% (72,97) | 0.68 | 83% (63,94) | 0.17 |
| SICUS/CEUS | 2 | 86% (78,91) | 94% (85,98) | |||
| Type of US probe | Both linear and convex | 5 | 86% (66,96) | 0.53 | 85% (81,88) | 0.46 |
| Linear | 3 | 90% (80,96) | 94% (36,100) | |||
| Method of Outcome analysis | Per patient | 5 | 90% (80,99) | 0.41 | 75% (61,90) | 0.48 |
| Per segment | 3 | 85% (68,100) | 93% (88,99) | |||
| Lesion location | Small bowel | 6 | 90% (81,99) | 0.61 | 90% (80,100) | 0.45 |
| Small and large bowels | 2 | 84% (62,100) | 81% (54,100) | |||
| Outcome | Combined features (active inflammation) | 5 | 90% (81,99) | 0.36 | 94% (88,99) | 0.01 * |
| One feature (bowel wall thickening/ulcer) | 3 | 84% (67,100) | 70% (47,93) | |||
| Author | US | MRE | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| TP | TN | FP | FN | Sensitivity (95% CI) | Specificity (95% CI) | TP | TN | FP | FN | Sensitivity (95% CI) | Specificity (95% CI) | |
| Aloi et al. [18] | 31 | 50 | 3 | 7 | 81% (65,92) | 94% (84,98) | 30 | 51 | 4 | 6 | 83% (67,93) | 92% (82,98) |
| Horjus_Talabur et al. [21] | 82 | 11 | 1 | 0 | 100% (95,100) | 91% (61,99) | 71 | 12 | 0 | 11 | 86% (77,93) | 100% (73,100) |
| Imsirovic et al. [22] | 23 | 10 | 0 | 22 | 51% (35,66) | 100% (69,100) | 44 | 7 | 3 | 1 | 97% (88,99) | 70% (34,93) |
| Servais et al. [24] | 10 | 4 | 1 | 2 | 83% (52,98) | 80% (28,99) | 8 | 4 | 1 | 4 | 66% (34,90) | 80% (28,99) |
| Taylor et al. [25] | 188 | 58 | 17 | 21 | 90% (85,93) | 77% (66,86) | 200 | 62 | 13 | 9 | 95% (92,98) | 82% (72,90) |
| Wilkens et al. [26] | 18 | 4 | 2 | 1 | 94% (74,99) | 66% (22,95) | 15 | 2 | 4 | 3 | 83% (58,96) | 33% (43,77) |
| Yuksel et al. [27] | 70 | 259 | 25 | 72 | 49% (40,57) | 91% (87,94) | 78 | 239 | 45 | 64 | 54% (46,63) | 84% (79,88) |
| Higgins I2 for study heterogeneity | 92.1% | 79.8% | 88.1% | 72.5% | ||||||||
| Summary estimate using the bivariate model | 86% a (65,96) | 87% b (78,93) | 86% a (72,93) | 84% b (72,90) | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, D.I.; You, M.-W.; Park, S.H.; Seo, M.; Park, S.J. Comparison of Diagnostic Performance of Ultrasonography and Magnetic Resonance Enterography in the Assessment of Active Bowel Lesions in Patients with Crohn’s Disease: A Systematic Review and Meta-Analysis. Diagnostics 2022, 12, 2008. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12082008
Lee DI, You M-W, Park SH, Seo M, Park SJ. Comparison of Diagnostic Performance of Ultrasonography and Magnetic Resonance Enterography in the Assessment of Active Bowel Lesions in Patients with Crohn’s Disease: A Systematic Review and Meta-Analysis. Diagnostics. 2022; 12(8):2008. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12082008
Chicago/Turabian StyleLee, Da In, Myung-Won You, So Hyun Park, Mirinae Seo, and Seong Jin Park. 2022. "Comparison of Diagnostic Performance of Ultrasonography and Magnetic Resonance Enterography in the Assessment of Active Bowel Lesions in Patients with Crohn’s Disease: A Systematic Review and Meta-Analysis" Diagnostics 12, no. 8: 2008. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12082008