
Interstitial Lung Fibrosis Following COVID-19 Pneumonia

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Demographic and Biological Parameters
2.2. Imaging Parameters
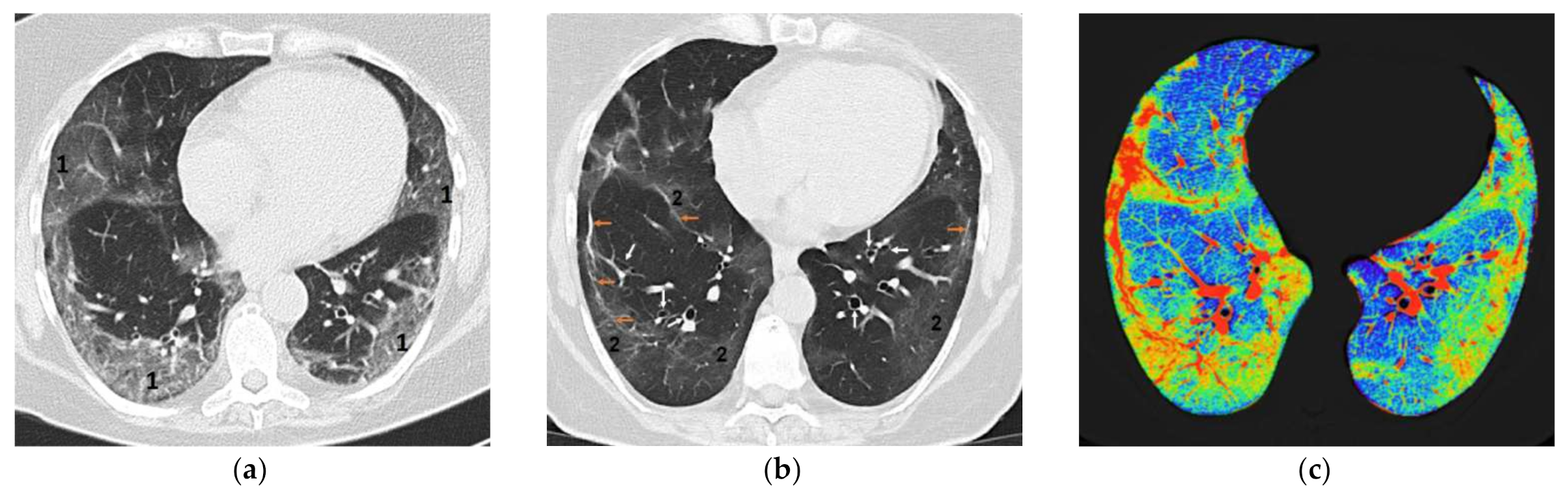
2.3. The Optimization Method in the Evaluation of Pulmonary Fibrosis Following COVID-19 Pneumonia by Quantitative Analysis
2.4. Identification of the Risk Factors/Predictors for Pulmonary Fibrosis in Patients with SARS-CoV-2 Infection
2.5. Characterization of the Impact of Pulmonary Fibrosis on the Symptomatology of Patients with COVID-19 after Release from the Hospital
3. Results
3.1. Quantitative Analysis of Pulmonary Fibrosis (Changes Registered at Three Months Follow-Up)
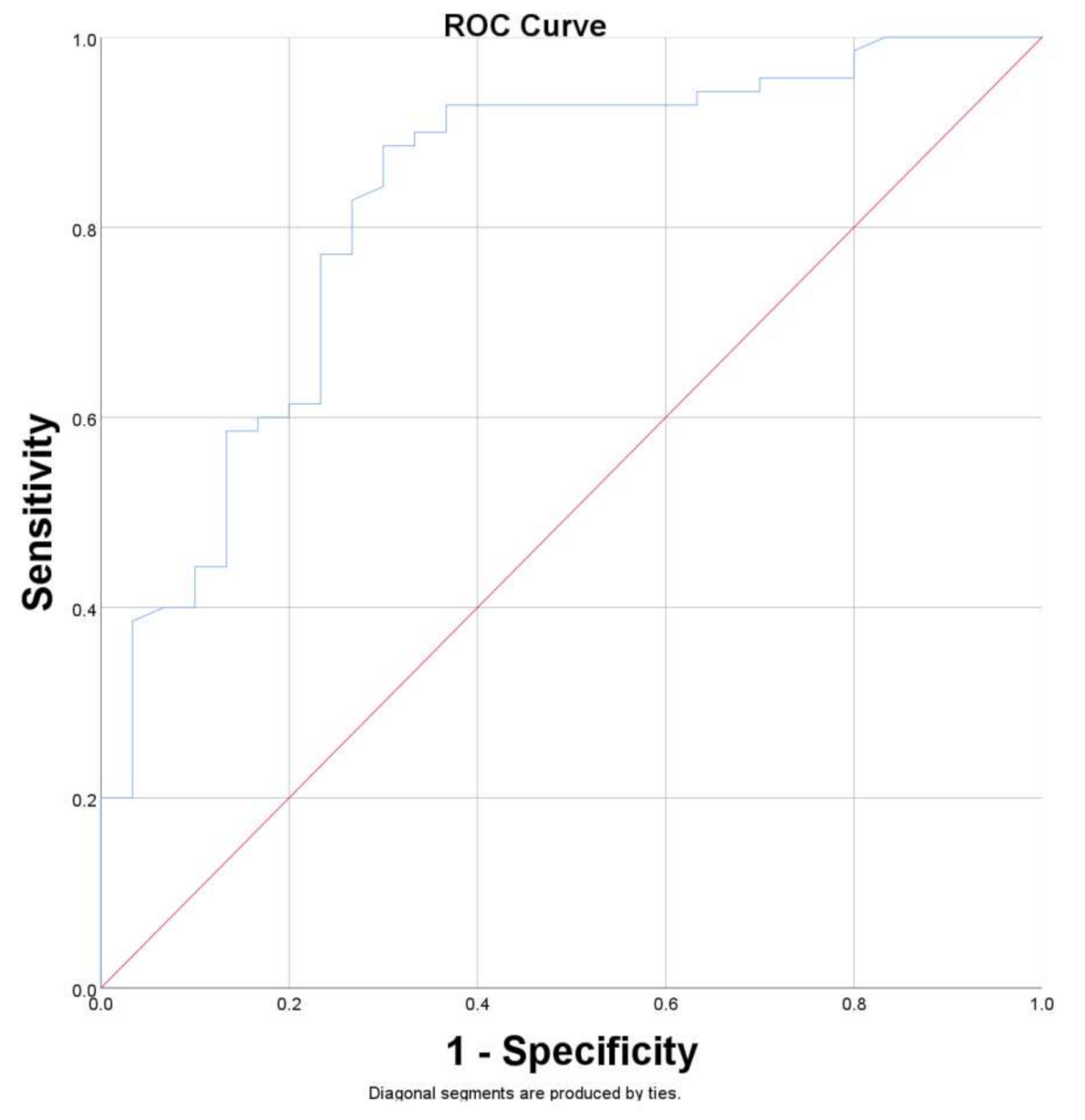
3.2. Risk Factors/Predictors for Pulmonary Fibrosis
3.3. Pulmonary Fibrosis and Symptomatology
4. Discussion
4.1. Mechanisms of Post-COVID-19 Lung Fibrosis
4.2. Evaluation of Pulmonary Fibrosis Following COVID-19 Pneumonia
4.3. Risk Factors/Predictors for Pulmonary Fibrosis in Patients with SARS-CoV-2 Infection
4.4. Impact of Pulmonary Fibrosis on the Symptomatology of Patients with COVID-19 after Release from the Hospital
4.5. Treatment of Post-COVID-19 Pulmonary Fibrosis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.M.; Lau, E.H.Y.; Wong, J.Y.; et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Ruan, F.; Huang, M.; Liang, L.; Huang, H.; Hong, Z.; Yu, J.; Kang, M.; Song, Y.; Xia, J.; et al. SARS-CoV-2 viral load in upper respiratory specimens of infected patients. N. Engl. J. Med. 2020, 382, 1177–1179. [Google Scholar] [CrossRef] [PubMed]
- Tung-Chen, Y.; Algora-Martín, A.; Rodríguez-Roca, S.; de Santiago, A.D. COVID-19 multisystemic inflammatory syndrome in adults: A not to be missed diagnosis. BMJ Case Rep. 2021, 14, e241696. [Google Scholar] [CrossRef] [PubMed]
- Aslan, A.; Aslan, C.; Zolbanin, N.M.; Jafari, R. Acute respiratory distress syndrome in COVID-19: Possible mechanisms and therapeutic management. Pneumonia 2021, 13, 14. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Paulson, K.R.; Pease, S.A.; Watson, S.; Comfort, H.; Zheng, P.; Aravkin, A.Y.; Bisignano, C.; Barber, R.M.; Alam, T.; et al. Estimating excess mortality due to the COVID-19 pandemic: A systematic analysis of COVID-19-related mortality, 2020–2021. Lancet 2022, 399, 1513–1536. [Google Scholar] [CrossRef]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef]
- Montani, D.; Savale, L.; Beurnier, A.; Colle, R.; Noël, N.; Pham, T.; Monnet, X.; Humbert, M. Multidisciplinary approach for post-acute COVID-19 syndrome: Time to break down the walls. Eur. Respir. J. 2021, 58, 2101090. [Google Scholar] [CrossRef]
- Amin, B.J.H.; Kakamad, F.H.; Ahmed, G.S.; Ahmed, S.F.; Abdulla, B.A.; Mohammed, S.H.; Mikael, T.M.; Salih, R.Q.; Ali, R.K.; Salh, A.M.; et al. Post COVID-19 pulmonary fibrosis; a meta-analysis study. Ann. Med. Surg. 2022, 77. [Google Scholar] [CrossRef]
- Rai, D.K.; Kumar, S.; Sahay, N. Post-COVID-19 pulmonary fibrosis: A case series and review of literature. J. Fam. Med. Prim. Care 2021, 10, 2028–2031. [Google Scholar] [CrossRef]
- Aul, R.; Gates, J.; Draper, A.; Dunleavy, A.; Ruickbie, S.; Meredith, H.; Walters, N.; van Zeller, C.; Taylor, V.; Bridgett, M.; et al. Complications after discharge with COVID-19 infection and risk factors associated with development of post-COVID pulmonary fibrosis. Respir. Med. 2021, 188, 106602. [Google Scholar] [CrossRef]
- Zou, J.N.; Sun, L.; Wang, B.R.; Zou, Y.; Xu, S.; Ding, Y.J.; Shen, L.J.; Huang, W.C.; Jiang, X.J.; Chen, S.M. The characteristics and evolution of pulmonary fibrosis in COVID-19 patients as assessed by AI-assisted chest HRCT. PLoS ONE 2021, 16, e0248957. [Google Scholar] [CrossRef] [PubMed]
- Wilson, M.S.; Wynn, T.A. Pulmonary fibrosis: Pathogenesis, etiology and regulation. Mucosal Immunol. 2009, 2, 103–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balestro, E.; Calabrese, F.; Turato, G.; Lunardi, F.; Bazzan, E.; Marulli, G.; Biondini, D.; Rossi, E.; Sanduzzi, A.; Rea, F.; et al. Immune Inflammation and Disease Progression in Idiopathic Pulmonary Fibrosis. PLoS ONE 2016, 11, e0154516. [Google Scholar] [CrossRef] [PubMed]
- Raghu, G.; Collard, H.R.; Egan, J.J.; Martinez, F.J.; Behr, J.; Brown, K.K.; Colby, T.V.; Cordier, J.-F.; Flaherty, K.R.; Lasky, J.A.; et al. An Official ATS/ERS/JRS/ALAT Statement: Idiopathic Pulmonary Fibrosis: Evidence-based Guidelines for Diagnosis and Management. Am. J. Respir. Crit. Care Med. 2011, 183, 788–824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hobbs, S.; Chung, J.; Leb, J.; Kaproth-Joslin, K.; Lynch, D. Practical Imaging Interpretation in Patients Suspected of Having Idiopathic Pulmonary Fibrosis: Official Recommendations from the Radiology Working Group of the Pulmonary Fibrosis Foundation. Radiol. Cardiothorac. Imaging 2021, 3, e200279. [Google Scholar] [CrossRef] [PubMed]
- Battista, G.; Sassi, C.; Zompatori, M.; Palmarini, D.; Canini, R. Ground-glass opacity: Interpretation of high resolution CT findings. La Radiol. Med. 2004, 106, 425–442. [Google Scholar]
- Hansell, D.M.; Bankier, A.A.; MacMahon, H.; McLoud, T.C.; Müller, N.L.; Remy, J. Fleischner Society: Glossary of Terms for Thoracic Imaging. Radiology 2008, 246, 697–722. [Google Scholar] [CrossRef] [Green Version]
- National Institutes of Health (NIH). COVID-19 Treatment Guidelines, Clinical Spectrum of SARS-CoV-2 Infection. 2021. Available online: https://www.covid19treatmentguidelines.nih.gov/overview/clinical-spectrum/ (accessed on 4 June 2022).
- Anghel, A.-M.; Niculae, C.-M.; Manea, E.-D.; Lazar, M.; Popescu, M.; Damalan, A.-C.; Bel, A.-A.; Nedelcu, I.-M.; Patrascu, R.-E.; Hristea, A. The Impact of Tocilizumab on Radiological Changes Assessed by Quantitative Chest CT in Severe COVID-19 Patients. J. Clin. Med. 2022, 11, 1247. [Google Scholar] [CrossRef]
- Leach, H.G.; Chrobak, I.; Han, R.; Trojanowska, M. Endothelial Cells Recruit Macrophages and Contribute to a Fibrotic Milieu in Bleomycin Lung Injury. Am. J. Respir. Cell Mol. Biol. 2013, 49, 1093–1101. [Google Scholar] [CrossRef] [Green Version]
- Prasse, A.; Pechkovsky, D.V.; Toews, G.B.; Jungraithmayr, W.; Kollert, F.; Goldmann, T.; Vollmer, E.; Müller-Quernheim, J.; Zissel, G. A Vicious Circle of Alveolar Macrophages and Fibroblasts Perpetuates Pulmonary Fibrosis via CCL18. Am. J. Respir. Crit. Care Med. 2006, 173, 781–792. [Google Scholar] [CrossRef] [Green Version]
- Kawata, M.; Koinuma, D.; Ogami, T.; Umezawa, K.; Iwata, C.; Watabe, T.; Miyazono, K. TGF-β-induced epithelial-mesenchymal transition of A549 lung adenocarcinoma cells is enhanced by pro-inflammatory cytokines derived from RAW 264.7 macrophage cells. J. Biochem. 2011, 151, 205–216. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.K.; Kugler, M.C.; Wolters, P.J.; Robillard, L.; Galvez, M.G.; Brumwell, A.N.; Sheppard, D.; Chapman, H.A. Alveolar epithelial cell mesenchymal transition develops in vivo during pulmonary fibrosis and is regulated by the extracellular matrix. Proc. Natl. Acad. Sci. USA 2006, 103, 13180–13185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delpino, M.V.; Quarleri, J. SARS-CoV-2 Pathogenesis: Imbalance in the renin-angiotensin system favors lung fibrosis. Front. Cell Infect. Microbiol. 2020, 10, 340. [Google Scholar] [CrossRef] [PubMed]
- Udwadia, Z.; Koul, P.; Richeldi, L. Post-COVID lung fibrosis: The tsunami that will follow the earthquake. Lung India 2021, 38, S41–S47. [Google Scholar] [CrossRef] [PubMed]
- Suh, Y.J.; Hong, H.; Ohana, M.; Bompard, F.; Revel, M.-P.; Valle, C.; Gervaise, A.; Poissy, J.; Susen, S.; Hékimian, G.; et al. Pulmonary Embolism and Deep Vein Thrombosis in COVID-19: A Systematic Review and Meta-Analysis. Radiology 2021, 298, E70–E80. [Google Scholar] [CrossRef] [PubMed]
- Tran, S.; Ksajikian, A.; Overbey, J.; Li, P.; Li, Y. Pathophysiology of Pulmonary Fibrosis in the Context of COVID-19 and Implications for Treatment: A Narrative Review. Cells 2022, 11, 2489. [Google Scholar] [CrossRef]
- Liu, M.; Lv, F.; Huang, Y.; Xiao, K. Follow-up study of the chest CT characteristics of COVID-19 survivors seven months after recovery. Front. Med. 2021, 8, 636298. [Google Scholar] [CrossRef]
- Nabahati, M.; Ebrahimpour, S.; Khaleghnejad Tabari, R.; Mehraeen, R. Post-COVID-19 pulmonary fibrosis and its predictive factors: A prospective study. Egypt. J. Radiol. Nucl. Med. 2021, 52, 248. [Google Scholar] [CrossRef]
- Bazdyrev, E.; Rusina, P.; Panova, M.; Novikov, F.; Grishagin, I.; Nebolsin, V. Lung Fibrosis after COVID-19: Treatment Prospects. Pharmaceuticals 2021, 14, 807. [Google Scholar] [CrossRef]
- Zhao, Y.-M.; Shang, Y.-M.; Song, W.-B.; Li, Q.-Q.; Xie, H.; Xu, Q.-F.; Jia, J.-L.; Li, L.-M.; Mao, H.-L.; Zhou, X.-M.; et al. Follow-up study of the pulmonary function and related physiological characteristics of COVID-19 survivors three months after recovery. eClinicalMedicine 2020, 25, 100463. [Google Scholar] [CrossRef]
- American Thoracic Society. Idiopathic pulmonary fibrosis: Diagnosis and treatment. International consensus statement. Am. J. Respir. Crit. Care Med. 2000, 161, 646–664. [Google Scholar] [CrossRef] [Green Version]
- Tung, K.T.; Wells, A.U.; Rubens, M.B.; Kirk, J.M.; du Bois, R.M.; Hansell, D.M. Accuracy of the typical computed tomographic appearances of fibrosingalveolitis. Thorax 1993, 48, 334–338. [Google Scholar] [CrossRef] [Green Version]
- Grenier, P.; Valeyre, D.; Cluzel, P.; Brauner, M.W.; Lenoir, S.; Chastang, C. Chronic diffuse interstitial lung disease: Diagnostic value of chest radiography and high-resolution CT. Radiology 1991, 179, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Hunninghake, G.W.; Lynch, D.A.; Galvin, J.R.; Gross, B.H.; Müller, N.; Schwartz, D.A.; King, T.E., Jr.; Lynch, J.P., 3rd; Hegele, R.; Waldron, J.; et al. Radiologic findings are strongly associated with a pathologic diagnosis of usual interstitial pneumonia. Chest 2003, 124, 1215–1223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kizer, J.; Zisman, D.; Blumenthal, N.; Kotloff, R.M.; Kimmel, S.E.; Strieter, R.M.; Arcasoy, S.M.; Ferrari, V.A.; Hansen-Flaschen, J. Association between pulmonary fibrosis and coronary artery disease. Arch. Int. Med. 2004, 164, 551–556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansell, D.M.; Goldin, J.G.; King, T.E., Jr.; Lynch, D.A.; Richeldi, L.; Wells, A.U. CT staging and monitoring of fi brotic interstitial lung diseases in clinical practice and treatment trials: A Position Paper from the Fleischner Society. Lancet 2015, 3, 483–496. [Google Scholar]
- Hunninghake, G.W.; Zimmerman, M.B.; Schwartz, D.A.; King, T.E., Jr.; Lynch, J.; Hegele, R.; Waldron, J.; Colby, T.; Müller, N.; Lynch, D.; et al. Utility of a lung biopsy for the diagnosis of idiopathic pulmonary fibrosis. Am. J. Respir. Crit. Care Med. 2001, 164, 193–196. [Google Scholar] [CrossRef] [Green Version]
- Swensen, S.J.; Aughenbaugh, G.L.; Myers, J.L. Diffuse lung disease: Diagnostic accuracy of CT in patients undergoing surgical biopsy of the lung. Radiology 1997, 205, 229–234. [Google Scholar] [CrossRef]
- Flaherty, K.R.; Toews, G.B.; Travis, W.D.; Colby, T.V.; Kazerooni, E.A.; Gross, B.H.; Jain, A.; Strawderman, R.L.; Paine, R.; Flint, A.; et al. Clinical significance of histological classification of idiopathic interstitial pneumonia. Eur. Respir. J. 2002, 19, 275–283. [Google Scholar] [CrossRef] [Green Version]
- Yu, M.; Liu, Y.; Xu, D.; Zhang, R.; Lan, L.; Xu, H. Prediction of the Development of Pulmonary Fibrosis Using Serial Thin-Section CT and Clinical Features in Patients Discharged after Treatment for COVID-19 Pneumonia. Korean J. Radiol. 2020, 21, 746–755. [Google Scholar] [CrossRef]
- Huang, W.; Wu, Q.; Chen, Z.; Xiong, Z.; Wang, K.; Tian, J.; Zhang, S. The potential indicators for pulmonary fibrosis in survivors of severe COVID-19. J. Infect. 2020, 82, e5–e7. [Google Scholar] [CrossRef] [PubMed]
- Patil, S.V.; Gondhali, G.; Patil, R. POST-COVID-19 LUNG FIBROSIS: STUDY OF 600 CASES IN TERTIARY CARE SETTING IN INDIA. Eur. Respir. J. 2021, 58, PA3776. [Google Scholar] [CrossRef]
- Gordon, A.C.; Mouncey, P.R.; Al-Beidh, F.; Rowan, K.M.; Nichol, A.D.; Arabi, Y.M.; Annane, D.; Beane, A.; van Bentum-Puijk, W.; Berry, L.R.; et al. Interleukin-6 receptor antagonists in critically ill patients with COVID-19. N Engl. J. Med. 2021, 384, 1491–1502. [Google Scholar] [PubMed]
- Mach, W.J.; Thimmesch, A.R.; Pierce, J.T.; Pierce, J.D. Consequences of hyperoxia and the toxicity of oxygen in the lung. Nurs. Res.Pract. 2011, 2011, 260482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vasarmidi, E.; Tsitoura, E.; Spandidos, D.A.; Tzanakis, N.; Antoniou, K.M. Pulmonary fibrosis in the aftermath of the COVID-19 era. Exp. Ther. Med. 2020, 20, 2557–2560. [Google Scholar] [CrossRef]
- Guler, S.A.; Ebner, L.; Beigelman, C.; Bridevaux, P.-O.; Brutsche, M.; Clarenbach, C.; Garzoni, C.; Geiser, T.K.; Lenoir, A.; Mancinetti, M.; et al. Pulmonary function and radiological features four months after COVID-19: First results from the national prospective observational Swiss COVID-19 lung study. Eur. Respir. J. 2021, 57, 2003690. [Google Scholar] [CrossRef] [PubMed]
- Stratan, L.; Tiliscan, C.; Arama, V.; Lazar, M.; Visan, A.; Ganea, O.; Trifonescu, M.I.; Arama, S.S.; Ion, D. COVID-19 associated coagulopathy is correlated with increased age and markers of inflammation response. Rev. Romana Med. Lab. 2021, 29, 387–394. [Google Scholar] [CrossRef]
- Han, X.; Fan, Y.; Alwalid, O.; Li, N.; Jia, X.; Yuan, M.; Li, Y.; Cao, Y.; Gu, J.; Wu, H.; et al. Six-month Follow-up Chest CT Findings after Severe COVID-19 Pneumonia. Radiology 2021, 299, E177–E186. [Google Scholar] [CrossRef]
- Arnold, D.T.; Hamilton, F.W.; Milne, A.; Morley, A.J.; Viner, J.; Attwood, M.; Noel, A.; Gunning, S.; Hatrick, J.; Hamilton, S.; et al. Patient outcomes after hospitalisation with COVID-19 and implications for follow-up: Results from a prospective UK cohort. Thorax 2020, 76, 399–401. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Brancatella, A.; Ricci, D.; Viola, N.; Sgrò, D.; Santini, F.; Latrofa, F. Subacute Thyroiditis After Sars-COV-2 Infection. J. Clin. Endocrinol. Metab. 2020, 105, 2367–2370. [Google Scholar] [CrossRef] [PubMed]
- Rubino, F.; Amiel, S.A.; Zimmet, P.; Alberti, G.; Bornstein, S.; Eckel, R.H.; Mingrone, G.; Boehm, B.; Cooper, M.E.; Chai, Z.; et al. New-Onset Diabetes in Covid-19. N. Engl. J. Med. 2020, 383, 789–790. [Google Scholar] [CrossRef] [PubMed]
- Chippa, V.; Aleem, A.; Anjum, F. Post Acute Coronavirus (COVID-19) Syndrome. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Chopra, V.; Flanders, S.A.; O’Malley, M.; Malani, A.N.; Prescott, H.C. Sixty-Day Outcomes Among Patients Hospitalized with COVID-19. Ann. Intern. Med. 2021, 174, 576–578. [Google Scholar] [CrossRef] [PubMed]
- Rai, D.K.; Sharma, P.; Kumar, R. Post covid 19 pulmonary fibrosis. Is it real threat? Indian, J. Tuberc. 2020, 68, 330–333. [Google Scholar] [CrossRef]
- Baldi, B.G.; Tanni, S.E. Pulmonary fibrosis and follow-up of COVID-19 survivors: An urgent need for clarification. J. Bras. Pneumol. 2021, 47, e20210213. [Google Scholar] [CrossRef]
- Mattos-Silva, P.; Felix, N.S.; Silva, P.L.; Robba, C.; Battaglini, D.; Pelosi, P.; Rocco, P.R.M.; Cruz, F.F. Pros and cons of corticosteroid therapy for COVID-19 patients. Respir. Physiol. Neurobiol. 2020, 280, 103492. [Google Scholar] [CrossRef]
- Batiha, G.E.-S.; Al-Gareeb, A.I.; Saad, H.M.; Al-Kuraishy, H.M. COVID-19 and corticosteroids: A narrative review. Inflammopharmacology 2022, 30, 1189–1205. [Google Scholar] [CrossRef]
- Collins, B.F.; Raghu, G. Antifibrotic therapy for fibrotic lung disease beyond idiopathic pulmonary fibrosis. Eur. Respir. Rev. 2019, 28, 190022. [Google Scholar] [CrossRef]
- Li, Y.; Li, H.; Liu, S. Pirfenidone ameliorates lipopolysaccharide-induced pulmonary inflammation and fibrosis by blocking NLRP3 inflammasome activation. Mol. Immunol. 2018, 99, 134–144. [Google Scholar] [CrossRef]
- George, P.M.; Wells, A.U.; Jenkins, R.G. Pulmonary fibrosis and COVID-19: The potential role for antifibrotic therapy. Lancet Respir. Med. 2020, 8, 807–815. [Google Scholar] [CrossRef]
- la Garza, C.E.M.-D.; Flores-Torres, A.S.; García-Hernández, M.; Castro-Corona, M.D.L. Diethylcarbamazine as potential treatment of COVID-19 lung fibrosis. Med. Hypotheses 2022, 160, 110774. [Google Scholar] [CrossRef] [PubMed]
- Enomoto, T.; Usuki, J.; Azuma, A.; Nakagawa, T.; Kudoh, S. Diabetes mellitus may increase risk for idiopathic pulmonary fibrosis. Chest 2003, 123, 2007–2011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartelius, H.; Gaub, J.; Ingemann Jensen, L.; Jensen, J.; Faber, V. Computed tomography of the lungs in acquired immunodeficiency syndrome. An early indicator of interstitial pneumonia. Acta Radiol. 1988, 29, 641–644. [Google Scholar] [CrossRef] [PubMed]
- Wahidi, M.M.; Speer, M.C.; Steele, M.P.; Brown, K.K.; Schwarz, M.I.; Schwartz, D.A. Familial pulmonary fibrosis in the United States. Chest 2002, 121, 30S. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameter | Admission DateMedian [Q1, Q3] | Follow-Up (3 Months) Median [Q1, Q3] | Control Group Median [Q1, Q3] | p-Value Admission vs. Follow-Up | p-Value Follow-Up vs. Control |
|---|---|---|---|---|---|
| C reactive protein (mg/L) | 43.9 [12.8, 89.9] | 3.35 [1.85, 6,49] | 2.8 [2.3, 3.6] | <0.001 | 0.794 |
| Erythrocyte Sedimentation Ratio (mm/h) | 45.8 [18.9, 60.7] | 15 [12, 17] | 14 [11, 16] | <0.001 | 0.570 |
| Fibrinogen (mg/dL) | 479 [368.8, 609.5] | 344 [307, 413.5] | 303.5 [244, 340.25] | <0.001 | 0.007 |
| Lactate dehydrogenase (U/L) | 279.2 [230.7, 365.1] | 188 [168, 214] | 180.5 [160, 197.75] | <0.001 | 0.419 |
| Alanine transaminase (U/L) | 42.2 [28, 57.6] | 37.5 [32, 47.7] | 36 [31.5, 39.5] | <0.001 | 0.151 |
| Creatine kinase (U/L) | 112.5 [48, 166.7] | 71.5 [36.7, 182] | 75 [41, 127] | 0.222 | 0.144 |
| Erythrocytes (×106/µL) | 4.68 [4.2, 5] | 4.7 [4.3, 5.1] | 4.64 [4.28, 5] | 0.665 | 0.519 |
| Leukocytes (×103/µL) | 6.6 [5.3, 10] | 7.1 [5.8, 9.1] | 6.6 [5.5, 9.1] | 0.096 | 0.644 |
| Lymphocytes (×103/µL) | 1 [0.6, 1.6] | 1.5 [1.1, 2.1] | 1.5 [1.3, 2] | 0.746 | 0.998 |
| Neutrophils (×103/µL) | 4.9 [3.4, 7.5] | 4.1 [3.2, 4.5] | 4.1 [3.2, 4.4] | <0.001 | 0.925 |
| Ly/Ne ratio | 0.2 [0,1, 0,4] | 0.4 [0.3, 0.5] | 0.4 [0.3, 0.5] | 0.383 | 0.9 |
| Platelets (×103/µL) | 203.3 [150.7, 256] | 223 [173.5, 301.7] | 225 [186, 280.5] | 0.614 | 0.937 |
| Ferritin (ng/mL) | 667.1 [319.4,1236.6] | 285 [150, 409.6] | 238 [150, 373.6] | <0.001 | 0.603 |
| D-dimers (ng/mL) | 204 [148.5, 287.2] | 210 [154, 283.5] | 201 [153.2, 257] | 0.111 | 0.658 |
| IL-1 (pg/mL) | 4.19 [0.2, 14.2] | 3.7 [0.4, 9.8] | 2.6 [0.3, 5.8] | 0.058 | 0.763 |
| IL-6 (pg/mL) | 68.6 [34.3, 249.1] | 8.7 [4.4, 24.2] | 5.1 [3.3, 7] | <0.001 | 0.814 |
| Parameter | Admission Date | Follow-Up (3 Months) | Control Group | p-ValueAdmission vs. Follow-Up | p-Value Follow-Up vs. Control |
|---|---|---|---|---|---|
| Affected pulmonary lobes (n, median, Q1, Q3) | 5 [4, 5] | 2.7 [0, 5] | 0 | <0.001 | <0.001 |
| Consolidation (%, median, Q1, Q3) | 1 [0.7, 1.7] | 0.7 [0.5, 0.9] | 0.6 [0.5, 0.7] | <0.001 | 0.252 |
| Mixed lesions (%, median, Q1, Q3) | 2.6 [1.4, 3.9] | 1.2 [1, 1.5] | 0.8 [0.7, 0.9] | <0.001 | 0.068 |
| Interstitial lesions (%, median, Q1, Q3) | 32.2 [23.3, 45.5] | 17.3 [14, 27] | 9 [7.7, 10.5] | <0.001 | <0.001 |
| Normal pulmonary densities (%, median, Q1, Q3) | 58.6 [44.4, 67.9] | 72.9 [66.4, 75] | 77.4 [75.9, 80.9] | 0.001 | <0.001 |
| Total pulmonary lesions (%, median, Q1, Q3) | 36.3 [25.3, 53] | 19.4 [15.7, 28.7] | 10.3 [9, 12.05] | <0.001 | <0.001 |
| Parameter | Spearman’s Rho | p-Value | OR [CI] | Risk of Fibrosis |
|---|---|---|---|---|
| Age | 130 | 0.198 | ||
| CRP | 0.252 | 0.02 | 1.015 [1.002, 1.028] | 1.5% * |
| ESR | 0.422 | <0.001 | 1.057 [1.021, 1.094] | 5.7% * |
| Fibrinogen | 0.192 | 0.06 | ||
| LDH | 0.204 | 0.05 | 1.005 [1, 1.01] | 0.5% * |
| Alanine transaminase | 0.135 | 0.19 | ||
| Creatine kinase | −0.74 | 0.47 | ||
| Erythrocytes | 0.007 | 0.94 | ||
| Leukocytes | 0.122 | 0.234 | ||
| Lymphocytes | 0.102 | 0.321 | ||
| Neutrophils | 0.076 | 0.457 | ||
| Ly/Ne ratio | 0.052 | 0.615 | ||
| Ferritin | −0.077 | 0.518 | ||
| Platelets | 0.152 | 0.137 | ||
| D-dimers | 0.12 | 0.25 | ||
| IL-1 | −0.206 | 0.302 | ||
| IL-6 | 0.192 | 0.145 | ||
| Duration of hospitalization | 0.249 | 0.012 | 1.06 [1.008, 1.115] | 6% * |
| Duration of antiviral treatment | 0.246 | 0.019 | 1.089 [0.957, 1.239] | − |
| Number of affected pulmonary lobes | 0.252 | 0.012 | 1.82 [1.175, 2.818] | 82% * |
| Percent of alveolar consolidation | 0.389 | <0.001 | 1.124 [0.776, 1.628] | − |
| Percent of mixed pulmonary lesions | 0.357 | <0.001 | 1.089 [0.917, 1.295] | − |
| Percent of interstitial pulmonary lesions | 0.519 | <0.001 | 1.122 [1.065, 1.183] | 12.2% * |
| Percent of normal lung densities | −0.478 | <0.001 | 0.924 [0.888, 0.761] | 8.6% # |
| Total pulmonary lung lesions | 0.480 | <0.001 | 1.081 [1.04, 1.124] | 8.1% * |
| Predictor | AUC | Std Error | p-Value | CI 95% | |
|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||
| CRP | 0.672 | 0.06 | 0.021 | 0.547 | 0.797 |
| ESR | 0.787 | 0.07 | 0.001 | 0.649 | 0.925 |
| LDH | 0.629 | 0.06 | 0.05 | 0.509 | 0.749 |
| Duration of hospitalization | 0.656 | 0.06 | 0.014 | 0.537 | 0.774 |
| Duration of antiviral treatment | 0.653 | 0.07 | 0.023 | 0.519 | 0.786 |
| Number of affected pulmonary lobes | 0.630 | 0.06 | 0.041 | 0.503 | 0.756 |
| Percent of alveolar consolidation | 0.745 | 0.06 | <0.001 | 0.622 | 0.868 |
| Percent of mixed pulmonary lesions | 0.725 | 0.06 | <0.001 | 0.597 | 0.853 |
| Percent of interstitial pulmonary lesions | 0.827 | 0.04 | <0.001 | 0.736 | 0.918 |
| Percent of normal lung densities | 0.801 | 0.05 | <0.001 | 0.691 | 0.911 |
| Total pulmonary lung lesions | 0.803 | 0.05 | <0.001 | 0.695 | 0.910 |
| Variable | B | S.E. | Wald | p | OR | 95% CI for OR | |
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| ESR | 0.034 | 0.023 | 2.165 | 0.141 | 1.035 | 0.989 | 1.083 |
| Duration of hospitalization | 0.082 | 0.055 | 2.198 | 0.138 | 1.086 | 0.974 | 1.21 |
| Duration of antiviral treatment | 0.36 | 0.199 | 3.264 | 0.071 | 1.433 | 0.970 | 2.118 |
| Percent of alveolar consolidation | −2.524 | 1.120 | 5.076 | 0.024 | 0.08 | 0.009 | 0.720 |
| Percent of interstitial pulmonary lesions | 0.391 | 0.176 | 4.913 | 0.027 | 1.478 | 1.046 | 2.089 |
| Constant | −9.789 | 4.092 | 5.722 | 0.017 | 0 | ||
| Parameter | Number of Patients (n,%) | Spearman’s Rho | p-Value |
|---|---|---|---|
| Fatigue | 32 (32%) | 0.449 | <0.001 |
| Shortness of breath | 20 (20%) | 0.327 | 0.001 |
| Chest pain | 11 (11%) | 0.091 | 0.365 |
| Cough | 16 (16%) | 0.286 | 0.004 |
| Memory loss and concentration problems | 11 (11%) | 0.230 | 0.021 |
| Insomnia | 16 (16%) | 0.048 | 0.634 |
| Palpitations | 11 (11%) | 0.021 | 0.834 |
| Dizziness | 13 (13%) | 0.253 | 0.011 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lazar, M.; Barbu, E.C.; Chitu, C.E.; Tiliscan, C.; Stratan, L.; Arama, S.S.; Arama, V.; Ion, D.A. Interstitial Lung Fibrosis Following COVID-19 Pneumonia. Diagnostics 2022, 12, 2028. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12082028
Lazar M, Barbu EC, Chitu CE, Tiliscan C, Stratan L, Arama SS, Arama V, Ion DA. Interstitial Lung Fibrosis Following COVID-19 Pneumonia. Diagnostics. 2022; 12(8):2028. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12082028
Chicago/Turabian StyleLazar, Mihai, Ecaterina Constanta Barbu, Cristina Emilia Chitu, Catalin Tiliscan, Laurentiu Stratan, Sorin Stefan Arama, Victoria Arama, and Daniela Adriana Ion. 2022. "Interstitial Lung Fibrosis Following COVID-19 Pneumonia" Diagnostics 12, no. 8: 2028. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12082028