
Volumetric Flow Assessment in Extracranial Arteries in Patients with 70–99% Internal Carotid Artery Stenosis
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Cerebral Blood Flow Volume in the Whole Study Group (53 Patients)
- 26/53, 49%—patients with significant volumetric flow compensation (CBF values exceeding the proposed reference values: average + standard deviation);
- 17/53, 32%—patients with mild compensation (in the presence of major reduction in the flow in one of carotid arteries, the increase in the other vessels allows the CBF to be maintained within the proposed standards);
- 10/53, 19%—patients with no compensation (CBF lower than the proposed reference value: average—standard deviation).
3.2. Cerebral Blood Flow Volume in the Whole Study Group (53 Patients)
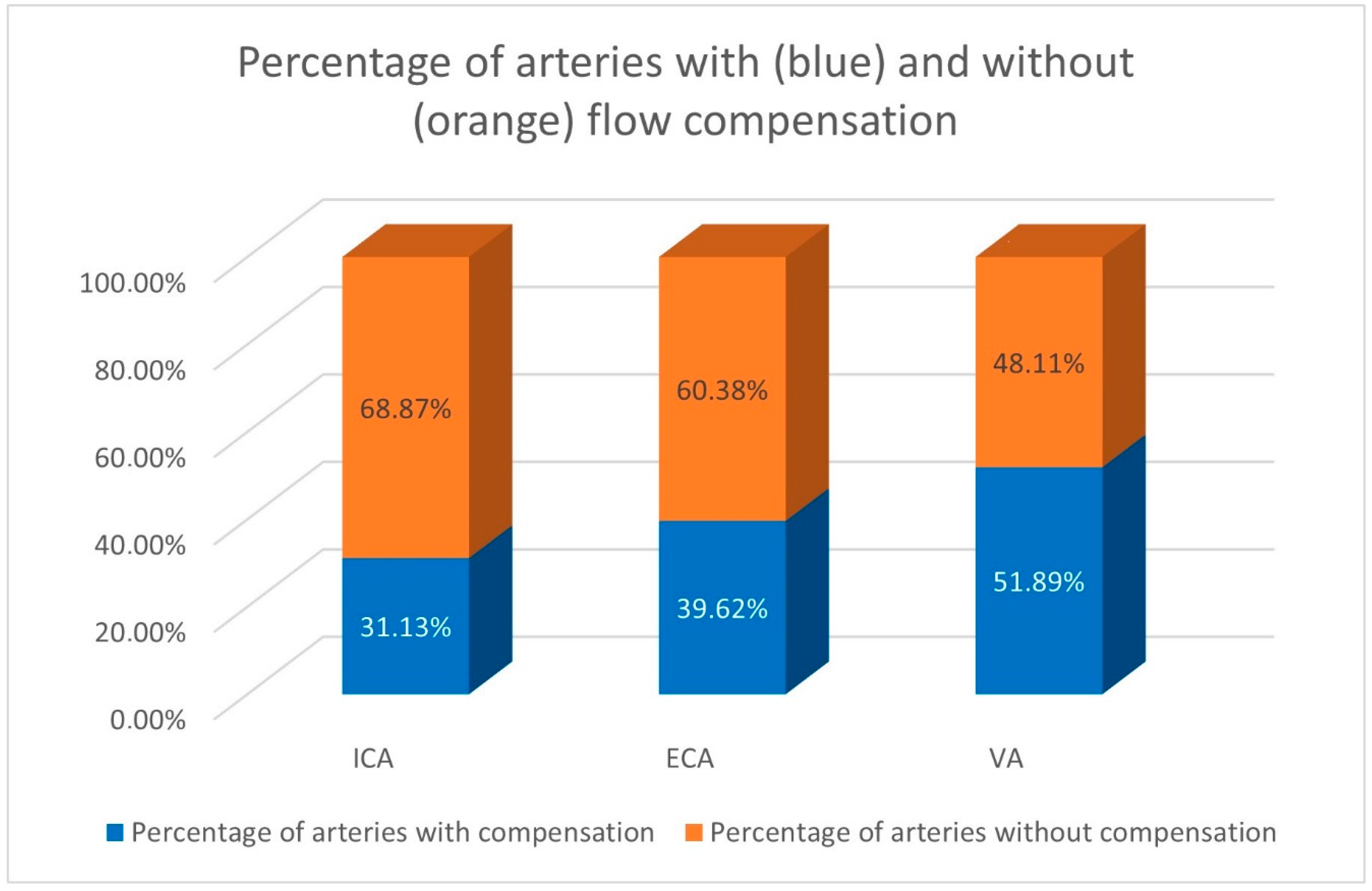
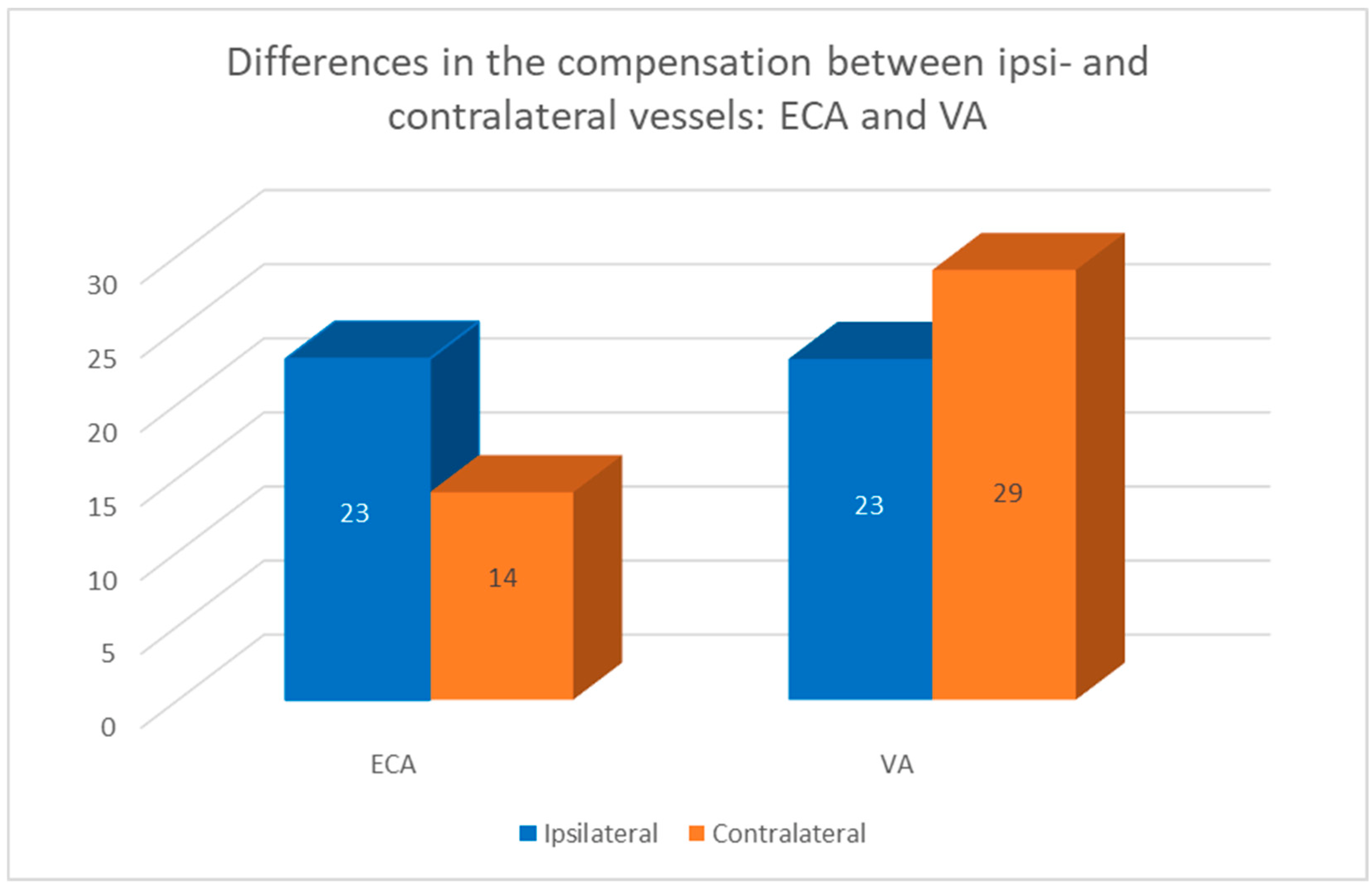
3.3. The Pathways of Volumetric Flow Compensation in the Extracranial Arteries
- 31 contralateral ICA;
- 29 contralateral VA;
- 23 ipsilateral ECA;
- 23 ipsilateral VA;
- 14 contralateral ECA.
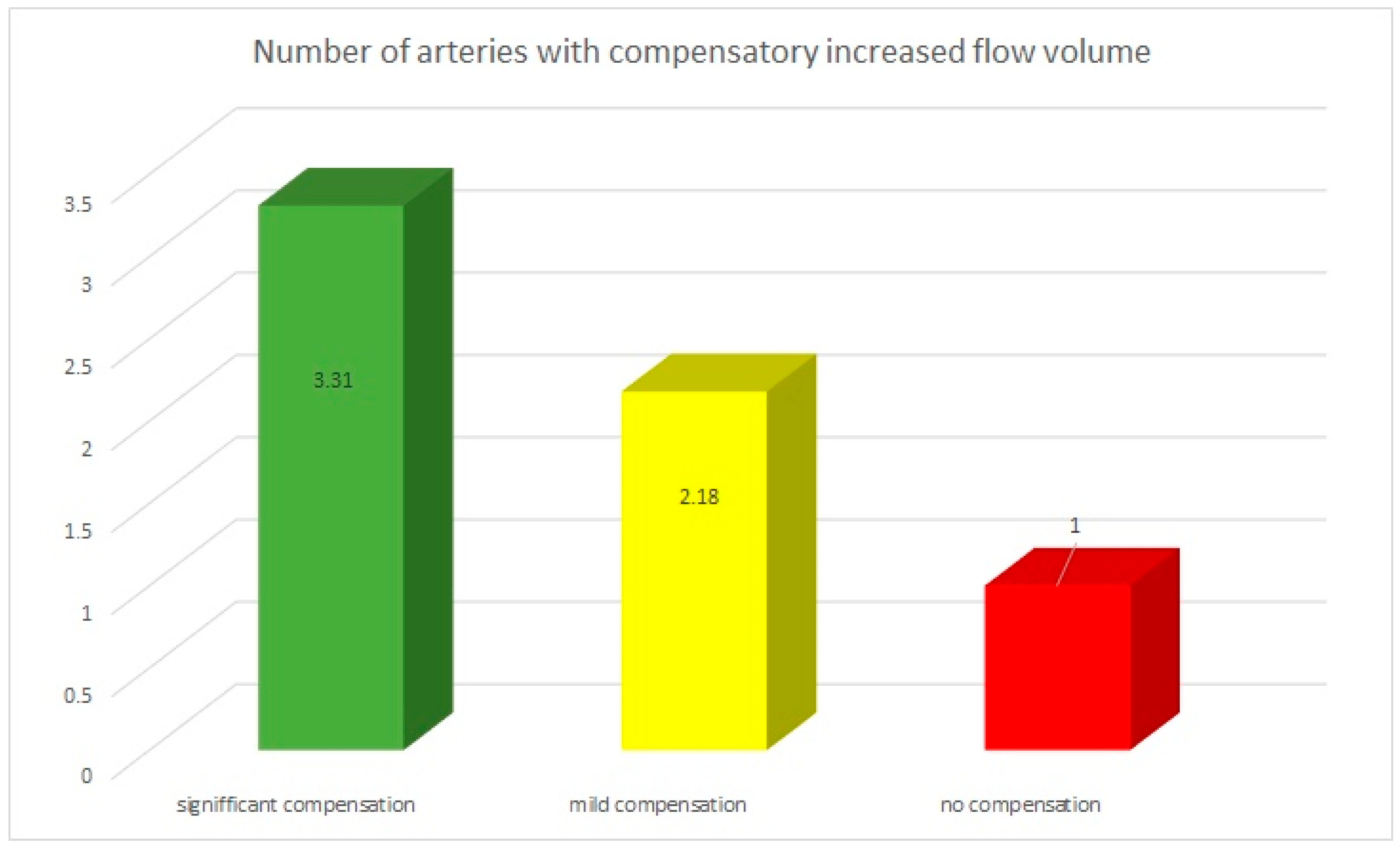
3.4. The Multivessel Character of Volumetric Flow Compensation
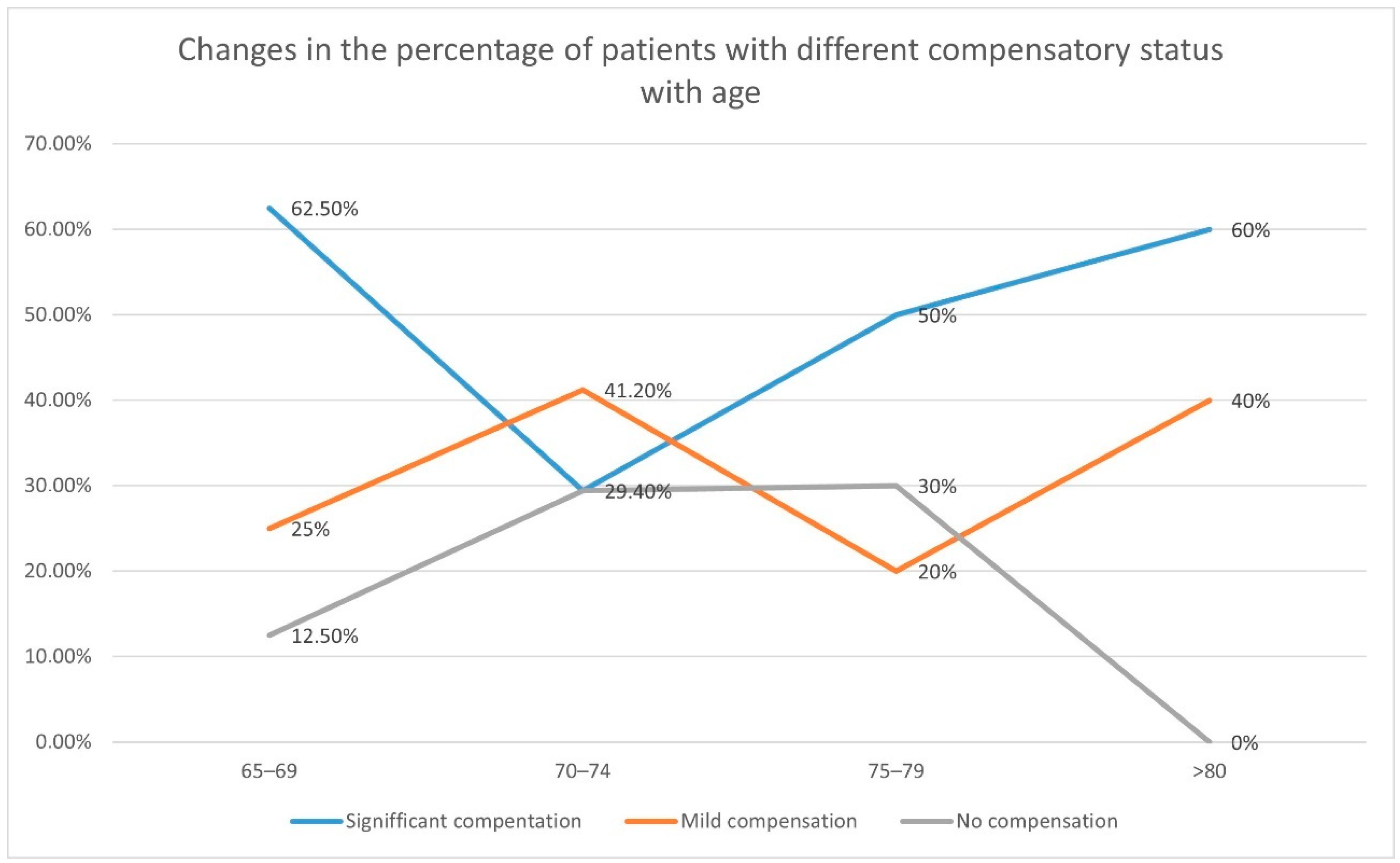
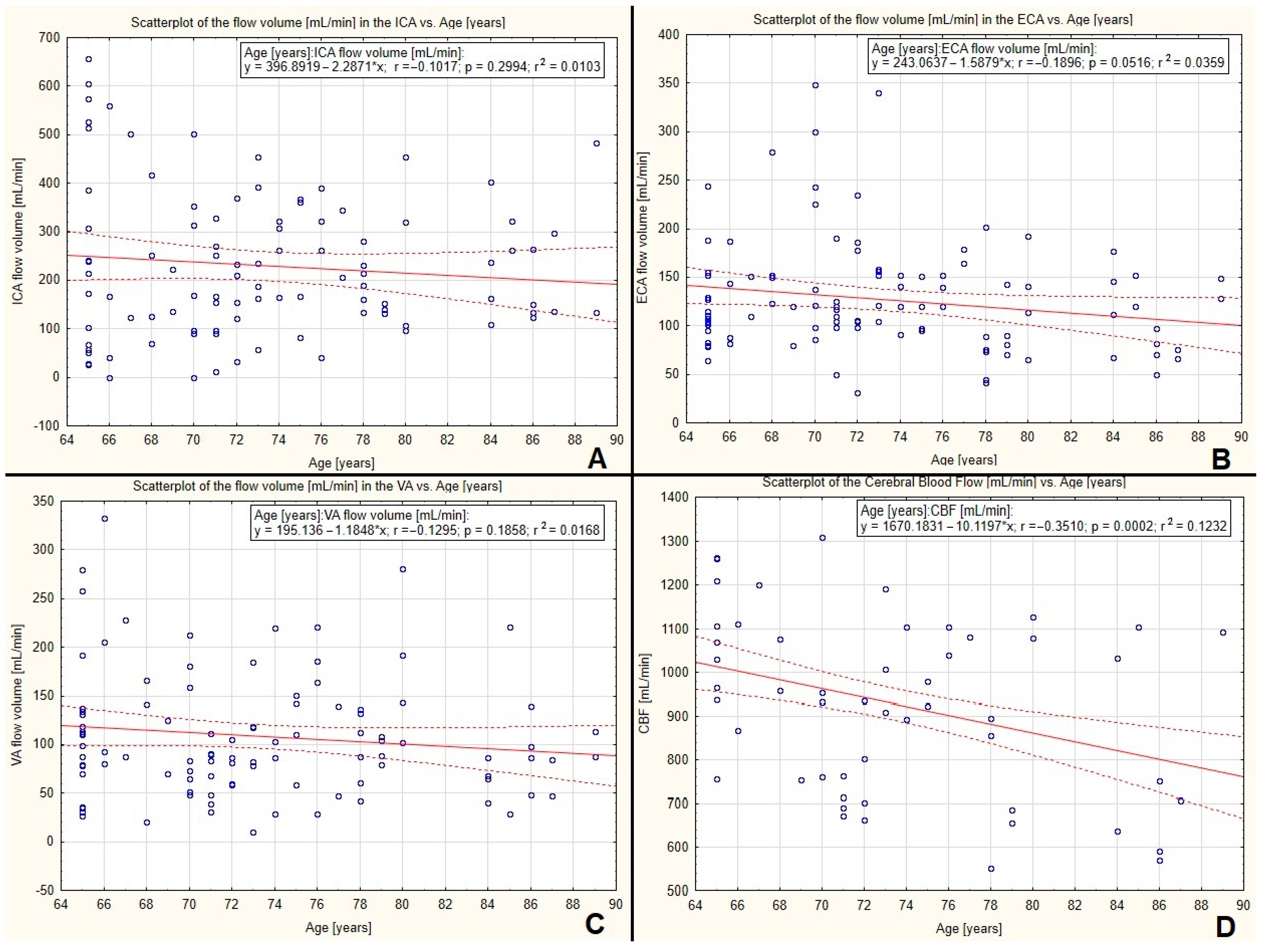
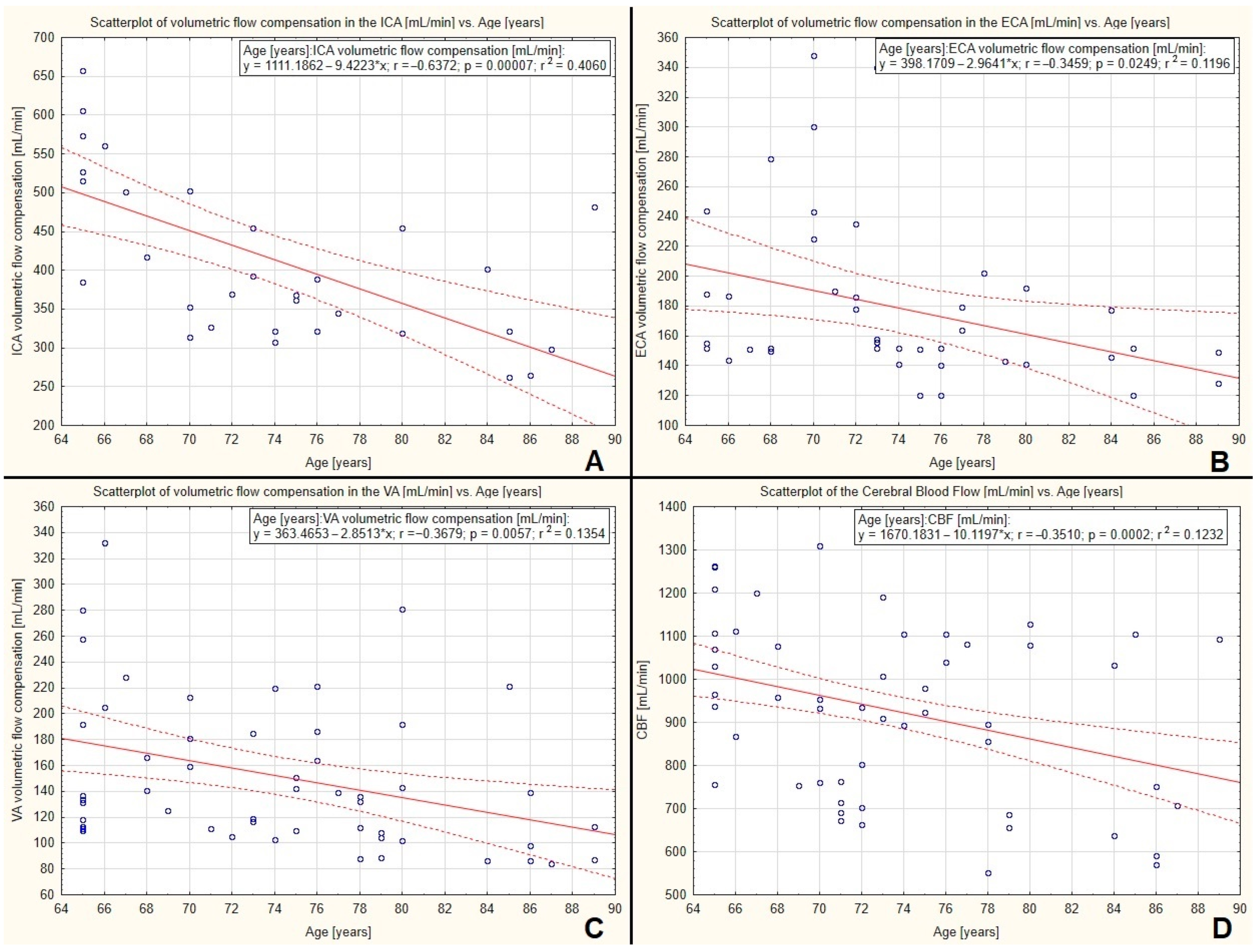
3.5. The Correlation between Volumetric Flow Compensation, Cerebral Blood Flow Volume, and Age
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Sigvant, B.; Wiberg-Hedman, K.; Bergqvist, D.; Rolandsson, O.; Andersson, B.; Persson, E.; Wahlberg, E. A population-based study of peripheral arterial disease prevalence with special focus on critical limb ischemia and sex differences. J. Vasc. Surg. 2007, 45, 1185–1191. [Google Scholar] [CrossRef] [PubMed]
- Sigvant, B.; Lundin, F.; Wahlberg, E. The Risk of Disease Progression in Peripheral Arterial Disease is Higher than Expected: A Meta-Analysis of Mortality and Disease Progression in Peripheral Arterial Disease. Eur. J. Vasc. Endovasc. Surg. 2016, 51, 395–403. [Google Scholar] [CrossRef] [PubMed]
- American Heart Association, Global Burden of Disease—2021 Statistical Fact Sheet. Available online: https://professional.heart.org/-/media/PHD-Files-2/Science-News/2/2021-Heart-and-Stroke-Stat-Update/2021_Stat_Update_factsheet_Global_Burden_of_Disease.pdf (accessed on 9 June 2022).
- Aboyans, V.; Ricco, J.B.; Bartelink, M.L.; Björck, M.; Brodmann, M.; Cohnert, T.; Collet, J.P.; Czerny, M.; De Carlo, M.; Debus, S. Editor’s Choice—2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS). Eur. J. Vasc. Endovasc. Surg. 2018, 55, 305–368. [Google Scholar] [CrossRef]
- Sobczyk, O.; Sam, K.; Mandell, D.M.; Crawley, A.P.; Venkatraghavan, L.; McKetton, L.; Poublanc, J.; Duffin, J.; Fisher, J.A.; Mikulis, D.J. Cerebrovascular Reactivity Assays Collateral Function in Carotid Stenosis. Front. Physiol. 2020, 11, 1031. [Google Scholar] [CrossRef] [PubMed]
- Bang, O.Y.; Saver, J.L.; Buck, B.H.; Alger, J.R.; Starkman, S.; Ovbiagele, B.; Kim, D.; Jahan, R.; Duckwiler, G.R.; Yoon, S.R.; et al. Impact of collateral flow on tissue fate in acute ischaemic stroke. J. Neurol. Neurosurg. Psychiatry 2008, 79, 625–629. [Google Scholar] [CrossRef] [PubMed]
- Sheth, S.A.; Sanossian, N.; Hao, Q.; Starkman, S.; Ali, L.K.; Kim, O.; Gonzalez, N.R.; Tateshima, S.; Jahan, R.; Duckwiler, G.R.; et al. Collateral flow as causative of good outcomes in endovascular stroke therapy. J. NeuroInterv. Surg. 2014, 8, 2–7. [Google Scholar] [CrossRef] [PubMed]
- Tan, B.; Wan-Yee, K.; Paliwal, P.; Gopinathan, A.; Nadarajah, M.; Ting, E.; Venketasubramanian, N.; Seet, R.C.; Chan, B.P.; Teoh, H.L.; et al. Good Intracranial Collaterals Trump Poor ASPECTS (Alberta Stroke Program Early CT Score) for Intravenous Thrombolysis in Anterior Circulation Acute Ischemic Stroke. Stroke 2016, 47, 2292–2298. [Google Scholar] [CrossRef]
- Elwertowski, M.; Leszczyński, J.; Kaszczewski, P.; Lamparski, K.; YeeHo, S.S.; Gałązka, Z. The importance of bloodflow volume in the brain-supplying arteries for the clinical management—the impact of collateral circulation. J. Ultrason. 2018, 18, 112–119. [Google Scholar] [CrossRef]
- Kaszczewski, P.; Elwertowski, M.; Leszczynski, J.; Ostrowski, T.; Galazka, Z. Volumetric Carotid Flow Characteristics in Doppler Ultrasonography in Healthy Population Over 65 Years Old. J. Clin. Med. 2020, 9, 1375. [Google Scholar] [CrossRef]
- Kaszczewski, P.; Elwertowski, M.; Leszczyński, J.; Ostrowski, T.; Gałązka, Z. CAR 5. Carotid flow volume measurement in Doppler ultrasound as a new look at the diagnosis of internal carotid artery stenosis. J. Vasc. Surg. 2019, 70, e162. [Google Scholar] [CrossRef]
- Kaszczewski, P.; Elwertowski, M.; Leszczyński, J.; Ostrowski, T.; Gałązka, Z. Volumetric Flow Assessment in Doppler Ultra- sonography in Risk Stratification of Patients with In-ternal Carotid Stenosis and Occlusion. J. Clin. Med. 2022, 11, 531. [Google Scholar] [CrossRef]
- Kaszczewski, P.; Elwertowski, M.; Leszczyński, J.; Ostrowski, T.; Kaszczewska, J.; Gałązka, Z. Intracranial Flow Volume Estimation in Patients with Internal Carotid Artery Occlusion. Diagnostics 2022, 12, 766. [Google Scholar] [CrossRef] [PubMed]
- Leszczyński, J.; Kaszczewski, P.; Elwertowski, M.; Stępkowski, K.; Maciąg, R.; Elwertowska, A.; Gałązka, Z. Volumetic Flow Changes in Extracranial Arteries in a Symptomatic Patient with Significant Bilateral Carotid Artery Stenosis: A Case Study and Literature Review. Am. J. Case Rep. 2020, 21, e927202. [Google Scholar] [CrossRef] [PubMed]
- Grant, E.G.; Benson, C.B.; Moneta, G.L.; Alexandrov, A.V.; Baker, J.D.; Bluth, E.I.; Carroll, B.A.; Eliasziw, M.; Gocke, J.; Hertzberg, B.S.; et al. Carotid Artery Stenosis: Gray-Scale and Doppler US Diagnosis—Society of Radiologists in Ultrasound Consensus Conference. Radiology 2003, 229, 340–346. [Google Scholar] [CrossRef] [PubMed]
- Von Reutern, G.M.; Goertler, M.W.; Bornstein, N.M.; Sette, M.D.; Evans, D.H.; Goertler, M.W.; Hetzel, A.; Kaps, M.; Perren, F.; Razumovky, A.; et al. Grading carotid stenosis using ultrasonic methods. Stroke 2012, 43, 916–921. [Google Scholar] [CrossRef]
- Arning, C.; Widder, B.; von Reutern, G.M.; Stiegler, H.; Görtler, M. Revision of DEGUM ultrasound criteria for grading internal carotid artery stenoses and transfer to NASCET measurement. Ultraschall Med. 2010, 31, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Mokhber, N.; Shariatzadeh, A.; Avan, A.; Saber, H.; Babaei, G.S.; Chaimowitz, G.; Azarpazhooh, M.R. Cerebral blood flow changes during aging process and in cognitive disorders: A review. Neuroradiol. J. 2021, 34, 300–307. [Google Scholar] [CrossRef]
- Udomphorn, Y.; Armstead, W.M.; Vavilala, M.S. Cerebral Blood Flow and Autoregulation After Pediatric Traumatic Brain Injury. Pediatr. Neurol. 2008, 38, 225–234. [Google Scholar] [CrossRef]
- Vavilala, M.S.; A Lee, L.; Lam, A.M. Cerebral blood flow and vascular physiology. Anesthesiol. Clin. N. Am. 2002, 20, 247–264. [Google Scholar] [CrossRef]
- Peters, R. Ageing and the brain. Postgrad. Med. J. 2006, 82, 84–88. [Google Scholar] [CrossRef]
- Scheel, P.; Ruge, C.; Petruch, U.R.; Schoning, M. Color Duplex Measurement of Cerebral Blood Flow Volume in Healthy Adults. Stroke 2000, 31, 147–150. [Google Scholar] [CrossRef]
- Buijs, P.C.; Krabbe-Hartkamp, M.J.; Bakker, C.J.; De Lange, E.; Ramos, L.M.; Breteler, M.; Mali, W.P. Effect of age on cerebral blood flow: Measurement with ungated two-dimensional phase-contrast MR angiography in 250 adults. Radiology 1998, 209, 667–674. [Google Scholar] [CrossRef] [PubMed]
- Kashimada, A.; Machida, K.; Honda, N.; Mamiya, T.; Takahashi, T.; Kamano, T.; Osada, H. Measurement of cerebral blood flow with two-dimensional cine phase-contrast mR imaging: Evaluation of normal subjects and patients with vertigo. Radiat. Med. 1995, 13, 95–102. [Google Scholar] [PubMed]
- Gupta, A.; Chazen, J.; Hartman, M. Cerebrovascular Reserve and Stroke Risk in Patients with Carotid Stenosis or Occlusion: A Systematic Review and Meta-Analysis. J. Vasc. Surg. 2013, 57, 1720. [Google Scholar] [CrossRef]
- Chuang, Y.M.; Liu, C.Y.; Pan, P.J.; Lin, C.P. Posterior communicating artery hypoplasia as a risk factor for acute ischemic stroke in the absence of carotid artery occlusion. J. Clin. Neurosci. 2008, 15, 1376–1381. [Google Scholar] [CrossRef] [PubMed]
- Shahan, C.P.; Gray, R.I.; Croce, M.A.; Fabian, T.C. Impact of circle of Willis anatomy in traumatic blunt cerebrovascular injury-related stroke. Trauma Surg. Acute Care Open 2017, 2, e000086. [Google Scholar] [CrossRef]
- Van Seeters, T.; Biessels, G.J.; Kappelle, L.J.; van der Graaf, Y.; Velthuis, B.K. Determinants of leptomeningeal collateral flow in stroke patients with a middle cerebral artery occlusion. Neuroradiology 2016, 58, 969–977. [Google Scholar] [CrossRef]
- Van Seeters, T.; Hendrikse, J.; Biessels, G.J.; Velthuis, B.K.; Mali, W.P.; Kappelle, L.J.; van der Graaf, Y. Completeness of the circle of Willis and risk of ischemic stroke in patients without cerebrovascular disease. Neuroradiology 2015, 57, 1247–1251. [Google Scholar] [CrossRef]
- Eldrea, H.; Arben, R.; Gabran, S. Anatomical variations of circle of Willis in adult human brains: A case control study in Albania. Manag. Health 2014, 18, 33–35. [Google Scholar]
- Badacz, R.; Przewłocki, T.; Karch, I.; Pieniazek, P.; Rosławiecka, A.; Mleczko, S.; Brzychczy, A.; Trystuła, M.; Zmudka, K.; Kabłak-Ziembicka, A. Low prevalence of collateral cerebral circulation in the circle of Willis in patients with severe carotid artery stenosis and recent ischemic stroke. Adv. Interv. Cardiol. 2015, 4, 312–317. [Google Scholar] [CrossRef]
- Oumer, M.; Alemayehu, M.; Muche, A. Association between circle of Willis and ischemic stroke: A systematic review and meta-analysis. BMC Neurosci. 2021, 22, 3. [Google Scholar] [CrossRef] [PubMed]
- Jongen, L.; van der Worp, H.; Waaijer, A.; van der Graaf, Y.; Mali, W. Interrelation between the Degree of Carotid Stenosis, Collateral Circulation and Cerebral Perfusion. Cerebrovasc. Dis. 2010, 30, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Myrcha, P.; Lewczuk, A.; Jakuciński, M.; Kozak, M.; Siemieniuk, D.; Rózan’ski, D.; Koziorowski, D.; Woz´niak, W. The Anatomy of the Circle of Willis Is Not a Strong Enough Predictive Factor for the Prognosis of Cross-Clamping Intolerance during Carotid Endarterectomy. J. Clin. Med. 2020, 9, 3913. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, S. A Comprehensive Study of the Anatomical Variations of the Circle of Willis in Adult Human Brains. J. Clin. Diagn. Res. 2013, 7, 2423–2427. [Google Scholar] [CrossRef] [PubMed]
- De Silva, K.R.D.; Silva, R.; Gunasekera, W.S.L.; Jeyesekera, R.W. Prevalence of typical circle of Willis and the variation in the anterior communicating artery: A study of a Sri Lankan population. Ann. Indian Acad. Neurol. 2009, 12, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Fawcett, E.; Blachford, J.V. The Circle of Willis: An Examination of 700 Specimens. J. Anat. Physiol. 1905, 40, 63–70. [Google Scholar]
- Vrselja, Z.; Brkic, H.; Mrdenovic, S.; Radic, R.; Curic, G. Function of Circle of Willis. J. Cereb. Blood Flow Metab. 2014, 34, 578–584. [Google Scholar] [CrossRef]
- Lattanzi, S.; Carbonari, L.; Pagliariccio, G.; Bartolini, M.; Cagnetti, C.; Viticchi, G.; Buratti, L.; Provinciali, L.; Silvestrini, M. Neurocognitive functioning and cerebrovascular reactivity after carotid endarterectomy. Neurology 2018, 90, e307–e315. [Google Scholar] [CrossRef]
- Lattanzi, S.; Carbonari, L.; Pagliariccio, G.; Cagnetti, C.; Luzzi, S.; Bartolini, M.; Buratti, L.; Provinciali, L.; Silvestrini, M. Predictors of cognitive functioning after carotid revascularization. J. Neurol. Sci. 2019, 405, 116435. [Google Scholar] [CrossRef]
- Kaszczewski, P. Peripheral: “A Novel Approach in the Assessment of the Influence of Internal Carotid Stenosis Treatment on Cerebral Blood Flow Volume Changes in Doppler Ultrasonography”; Charing Cross International Symposium: London, UK, 2022. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Female | Male | Total | |
|---|---|---|---|
| Number of patients | 17 | 36 | 53 |
| Mean age±std. dev. | 73.9 ± 7.5 years old | 73.2 ± 6.8 years old | 73.4 ± 7 years old |
| Number of patients with LICA stenosis | 5 | 11 | 16 |
| Number of patients with RICA stenosis | 10 | 21 | 31 |
| Number of patients with bilateral ICA stenosis | 2 | 4 | 6 |
| Age: 65–69 | 5 | 11 | 16 |
| Age: 70–74 | 5 | 12 | 17 |
| Age: 75–79 | 3 | 7 | 10 |
| Age: 80+ | 4 | 6 | 10 |
| Age Group | 65–69 | 70–74 | 75–80 | >80 |
|---|---|---|---|---|
| CBF Proposed reference value [mL/min] | 898.5 ± 119.1 | 838.5 ± 148.9 | 805.1 ± 99.3 | 685.7 ± 112.3 |
| RICA [mL/min] | 271.1 ± 63.6 | 236.0 ± 66.1 | 234.8 ± 62.3 | 202.3 ± 38.4 |
| RECA [mL/min] | 106.1 ± 35.0 | 103.7 ± 33.2 | 94.0 ± 24.14 | 83.1 ± 36.3 |
| RVA [mL/min] | 58.7 ± 29.1 | 60.2 ± 26.7 | 62.3 ± 28.4 | 55.7 ± 24.1 |
| LICA [mL/min] | 276.4 ± 57.5 | 239.8 ± 42.4 | 245.5 ± 32.3 | 204.4 ± 47.0 |
| LECA [mL/min] | 101.4 ± 30.9 | 104.7 ± 32.5 | 89.0 ± 21.9 | 79.0 ± 33.7 |
| LVA [mL/min] | 84.9 ± 33.0 | 80.4 ± 29.8 | 70.0 ± 21.5 | 58.8 ± 13.0 |
| Age/Flow Compensation | Significant Compensation | Mild Compensation—Flow Volume within Reference Value | No Compensation—Decreased Flow Volume |
|---|---|---|---|
| Whole study group | 26/53 (49%) | 17/53 (32%) | 10/53 (19%) |
| 65–69 | 10/16 (62.5%) | 4/16 (25%) | 2/16 (12.5%) |
| 70–74 | 5/17 (29.4%) | 7/17 (41.2%) | 5/17 (29.4%) |
| 75–79 | 5/10 (50%) | 2/10 (20%) | 3/10 (30%) |
| ≥80 | 6/10 (60%) | 4/10 (40%) | 0/10 (0%) |
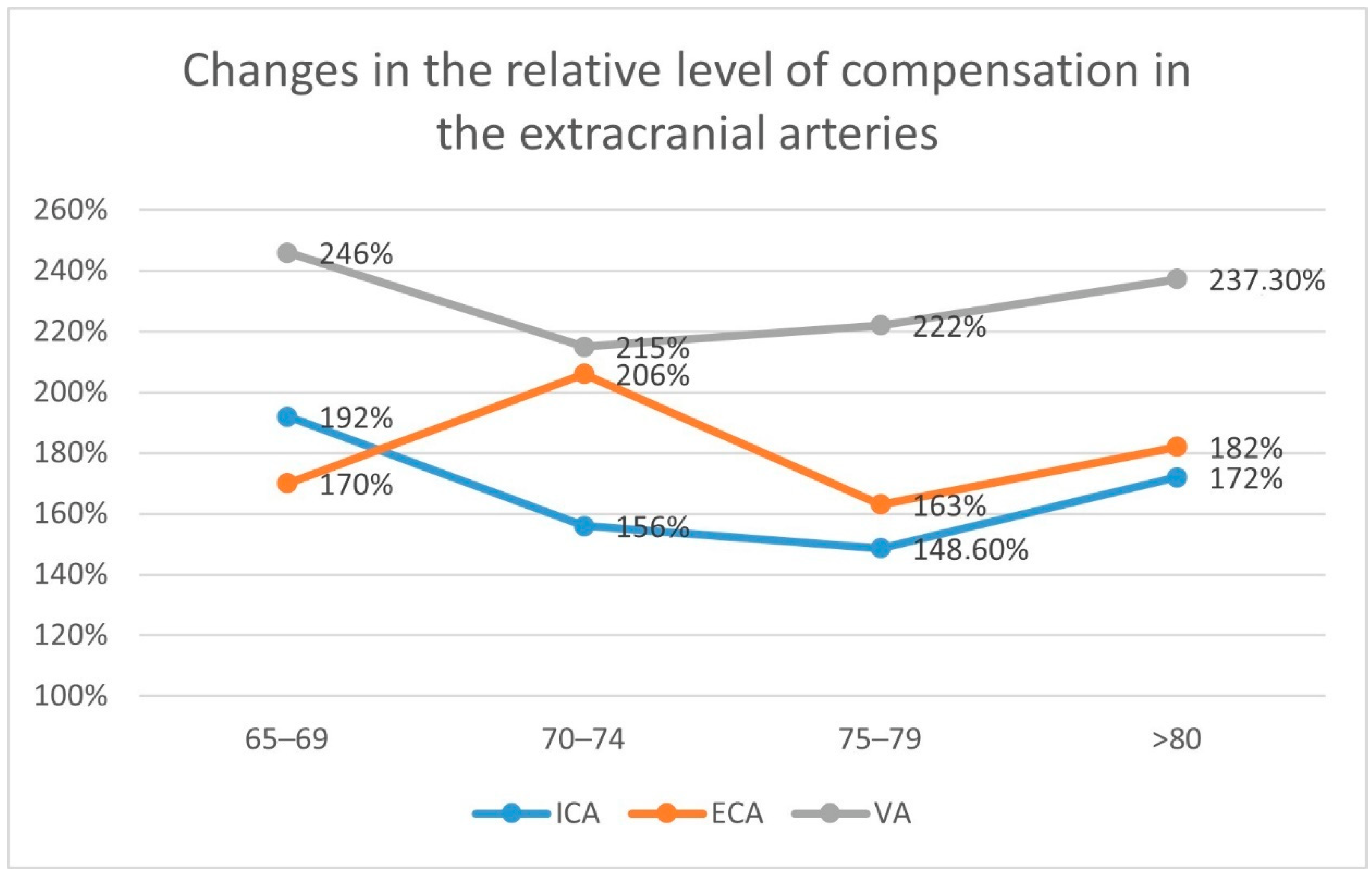
| Age Group | Artery | Compensation Average ± std. dev. [mL/min] | Reference [mL/min] | p < 0.005 | Flow Difference [mL/min] | Relative Flow Increase |
|---|---|---|---|---|---|---|
| 65–69 | ICA | 525.7 ± 81.4 | 273.8 ± 60.5 | yes | 251.9 | 192% |
| ECA | 176.8 ± 50.3 | 103.6 ± 32.9 | yes | 73.8 | 170% | |
| VA | 176.7 ± 68.1 | 71.8 ± 32.3 | yes | 104.9 | 246% | |
| 70–74 | ICA | 370.9 ± 67.7 | 237.9 ± 54.3 | yes | 133 | 156% |
| ECA | 214.6 ± 70.6 | 104.2 ± 32.7 | yes | 110.4 | 206% | |
| VA | 151.3 ± 45.9 | 70.3 ± 28.8 | yes | 81 | 215% | |
| 75–79 | ICA | 356.8 ± 25.5 | 240.1 ± 47.3 | yes | 116.7 | 148.60% |
| ECA | 149.1 ± 27.1 | 91.5 ± 23 | yes | 57.6 | 163% | |
| VA | 134.4 ± 37.6 | 60.5 ± 25 | yes | 73.9 | 222% | |
| >80 | ICA | 350.4 ± 85.2 | 203.2 ± 42.7 | yes | 147.2 | 172.00% |
| ECA | 150.6 ± 23.8 | 81 ± 35 | yes | 69.6 | 186% | |
| VA | 136.0 ± 63.7 | 57.3 ± 18.5 | yes | 78.7 | 237.30% |
| Age Group | Number of Patients | Stenosis | Contralateral ICA | Contralateral ECA | Contralateral VA | Ipsilateral ECA | Ipsilateral VA |
|---|---|---|---|---|---|---|---|
| 65–69 | 6 | RICA | 5/6 (83%) | 0/6 (0%) | 6/6 (100%) | 2/6 (33%) | 2/6 (33%) |
| 7 | LICA | 6/7 (86%) | 1/7 (14%) | 3/7 (43%) | 4/7 (57%) | 6/7 (86%) | |
| 70–74 | 14 | RICA | 8/14 (57%) | 4/14 (29%) | 5/14 (36%) | 5/14 (36%) | 2/14 (14%) |
| 2 | LICA | 1/2 (50%) | 1/2 (50%) | 1/2 (50%) | 2/2 (100%) | 2/2 (100%) | |
| 75–79 | 5 | RICA | 2/5 (40%) | 2/5 (40%) | 4/5 (80%) | 1/5 (20%) | 2/5 (40%) |
| 5 | LICA | 3/5 (60%) | 3/5 (60%) | 3/5 (60%) | 4/5 (80%) | 5/5 (100%) | |
| >80 | 6 | RICA | 5/6 (83%) | 2/6 (33%) | 6/6 (100%) | 3/6 (50%) | 3/6 (50%) |
| 2 | LICA | 1/2 (50%) | 1/2 (50%) | 1/2 (50%) | 2/2 (100%) | 1/2 (50%) |
| Age Group | Number of Patients | Stenosis | LECA | LVA | RECA | RVA |
|---|---|---|---|---|---|---|
| 65–69 | 3 | Bliateral | 2 | 1 | 1 | 2 |
| 70–74 | 1 | Bilateral | 1 | 0 | 1 | 0 |
| 75–79 | 0 | Bilateral | - | - | - | - |
| >80 | 2 | Bilateral | 0 | 0 | 0 | 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaszczewski, P.; Elwertowski, M.; Leszczyński, J.; Ostrowski, T.; Kaszczewska, J.; Brzeziński, T.; Jarosz, D.; Świeczkowski-Feiz, S.; Gałązka, Z. Volumetric Flow Assessment in Extracranial Arteries in Patients with 70–99% Internal Carotid Artery Stenosis. Diagnostics 2022, 12, 2216. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12092216
Kaszczewski P, Elwertowski M, Leszczyński J, Ostrowski T, Kaszczewska J, Brzeziński T, Jarosz D, Świeczkowski-Feiz S, Gałązka Z. Volumetric Flow Assessment in Extracranial Arteries in Patients with 70–99% Internal Carotid Artery Stenosis. Diagnostics. 2022; 12(9):2216. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12092216
Chicago/Turabian StyleKaszczewski, Piotr, Michał Elwertowski, Jerzy Leszczyński, Tomasz Ostrowski, Joanna Kaszczewska, Tomasz Brzeziński, Daniel Jarosz, Siavash Świeczkowski-Feiz, and Zbigniew Gałązka. 2022. "Volumetric Flow Assessment in Extracranial Arteries in Patients with 70–99% Internal Carotid Artery Stenosis" Diagnostics 12, no. 9: 2216. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12092216