
Evaluation of Hepcidin Level in COVID-19 Patients Admitted to the Intensive Care Unit
 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Group
2.2. Measurement of Hepcidin Level
2.3. Measurement of Other Laboratory Parameters
2.4. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhou, P.; Yang, X.L.; Wang, X.G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.R.; Zhu, Y.; Li, B.; Huang, C.L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. National Institutes of Health. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 19 October 2021).
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA 2020, 323, 1061. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Nai, A.; Lorè, N.I.; Pagani, A.; De Lorenzo, R.; Di Modica, S.; Saliu, F.; Cirillo, D.M.; Rovere-Querini, P.; Manfredi, A.A.; Silvestri, L. Hepcidin levels predict Covid-19 severity and mortality in a cohort of hospitalized Italian patients. Am. J. Hematol. 2021, 96, E32–E35. [Google Scholar] [CrossRef] [PubMed]
- DePalma, R.G.; Hayes, V.W.; O’Leary, T.J. Optimal serum ferritin level range: Iron status measure and inflammatory biomarker. Metallomics 2021, 13, mfab030. [Google Scholar] [CrossRef]
- Nemeth, E.; Ganz, T. The role of hepcidin in iron metabolism. Acta Haematol. 2009, 122, 78–86. [Google Scholar] [CrossRef] [Green Version]
- Nemeth, E.; Ganz, T. Hepcidin-Ferroportin interaction controls systemic iron homeostasis. Int. J. Mol. Sci. 2021, 22, 6493. [Google Scholar] [CrossRef]
- Jiao, Y.; Yong, C.; Zhang, R.; Wang, D. Hepcidin alleviates LPS-induced ARDS by regulating the ferritin-mediated suppression of ferroptosis. Shock 2022, 57, 274–281. [Google Scholar] [CrossRef]
- Ganz, T. Macrophages and systemic iron homeostasis. J. Innate. Immun. 2012, 4, 446–453. [Google Scholar] [CrossRef]
- Zhou, C.; Chen, Y.; Ji, Y.; He, X.; Xue, D. Increased serum levels of hepcidin and ferritin are associated with severity of COVID-19. Med. Sci. Monit. 2020, 26, e926178. [Google Scholar] [CrossRef]
- Zhao, K.; Huang, J.; Dai, D.; Feng, Y.; Liu, L.; Nie, S. Serum iron level as a potential predictor of Coronavirus Disease 2019 severity and mortality: A retrospective study. Open. Forum. Infect. Dis. 2020, 7, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.; Frost, J.N.; Aaron, L.; Donovan, K.; Drakesmith, H. Systemic hypoferremia and severity of hypoxemic respiratory failure in COVID-19. Crit. Care 2020, 24, 320. [Google Scholar] [CrossRef] [PubMed]
- Ciotti, M.; Ciccozzi, M.; Pieri, M.; Bernardini, S. The COVID-19 pandemic: Viral variants and vaccine efficacy. Crit. Rev. Clin. Lab. Sci. 2022, 59, 66–75. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Madhavan, M.V.; Sehgal, K.; Nair, N.; Mahajan, S.; Sehrawat, T.S.; Bikdeli, B.; Ahluwalia, N.; Ausiello, J.C.; Wan, E.Y. Extrapulmonary manifestations of COVID-19. Nat. Med. 2020, 26, 1017–1032. [Google Scholar] [CrossRef]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Rostami, M.; Mansouritorghabeh, H. D-dimer level in COVID-19 infection: A systematic review. Expert Rev. Hematol. 2020, 13, 1265–1275. [Google Scholar] [CrossRef]
- Nugroho, J.; Wardhana, A.; Maghfirah, I.; Mulia, E.P.B.; Rachmi, D.A.; Ayun, M.Q.; Septianda, I. Relationship of D-dimer with severity and mortality in SARS-CoV-2 patients: A meta-analysis. Int. J. Lab. Hematol. 2021, 43, 110–115. [Google Scholar] [CrossRef]
- Bansal, A.; Singh, A.D.; Jain, V.; Aggarwal, M.; Gupta, S.; Padappayil, R.P.; Nadeem, M.; Joshi, S.; Mian, A.; Greathouse, T.; et al. The association of D-dimers with mortality, intensive care unit admission or acute respiratory distress syndrome in patients hospitalized with coronavirus disease 2019 (COVID-19): A systematic review and metaanalysis. Heart Lung 2021, 50, 9–12. [Google Scholar] [CrossRef]
- Henry, B.M.; Aggarwal, G.; Wong, J.; Benoit, S.; Vikse, J.; Plebani, M.; Lippi, G. Lactate dehydrogenase levels predict coronavirus disease 2019 (COVID-19) severity and mortality: A pooled analysis. Am. J. Emerg. Med. 2020, 38, 1722–1726. [Google Scholar] [CrossRef]
- Szarpak, L.; Ruetzler, K.; Safiejko, K.; Hampel, M.; Pruc, M.; Kanczuga-Koda, L.; Filipiak, K.J.; Jaguszewski, M.J. Lactate dehydrogenase levels as a COVID-19 severity marker. Am. J. Emerg. Med. 2021, 45, 638–639. [Google Scholar] [CrossRef]
- Huang, Y.; Guo, L.; Chen, J.; Wu, M.; Zhang, C.; Liu, Z.; Li, J.; Li, K.; Xiong, Z.; Wu, Q.; et al. Serum lactate dehydrogenase level as a prognostic factor for COVID-19: A retrospective study based on a large sample size. Front. Med. 2022, 8, 671667. [Google Scholar] [CrossRef] [PubMed]
- Bao, J.; Li, C.; Zhang, K.; Kang, H.; Chen, W.; Gu, B. Comparative analysis of laboratory indexes of severe and non-severe patients infected with COVID-19. Clin. Chim. Acta 2020, 509, 180–194. [Google Scholar] [CrossRef] [PubMed]
- Gu, Y.; Wang, D.; Chen, C.; Lu, W.; Liu, H.; Lv, T.; Song, Y.; Zhang, F. PaO2/FiO2 and IL-6 are risk factors of mortality for intensive care COVID-19 patients. Sci. Rep. 2021, 11, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; Guo, P.; Zhang, L.; Wang, F. Serum Interleukin-6 concentrations and the severity of COVID-19 pneumonia: A retrospective study at a single center in Bengbu City, Anhui Province, China, in January and February 2020. Med. Sci. Monit. 2020, 26, e926941. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Wu, D.; Guo, W.; Cao, Y.; Huang, D.; Wang, H.; Wang, T.; Zhang, X.; Chen, H.; Yu, H.; et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J. Clin. Investig. 2020, 130, 2620–2629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halim, C.; Mirza, A.F.; Sari, M.I. The Association between TNF-α, IL-6, and Vitamin D Levels and COVID-19 Severity and Mortality: A Systematic Review and Meta-Analysis. Pathogens 2022, 11, 195. [Google Scholar] [CrossRef] [PubMed]
- Del Valle, D.M.; Kim-Schulze, S.; Huang, H.H.; Beckmann, N.D.; Nirenberg, S.; Wang, B.; Lavin, Y.; Swartz, T.H.; Madduri, D.; Stock, A.; et al. An inflammatory cytokine signature predicts COVID-19 severity and survival. Nat. Med. 2020, 26, 1636–1643. [Google Scholar] [CrossRef]
- Yang, A.P.; Liu, J.P.; Tao, W.Q.; Li, H.M. The diagnostic and predictive role of NLR, d-NLR and PLR in COVID-19 patients. Int. Immunopharmacol. 2020, 84, 106504. [Google Scholar] [CrossRef]
- Reusch, N.; De Domenico, E.; Bonaguro, L.; Schulte-Schrepping, J.; Baßler, K.; Schultze, J.L.; Aschenbrenner, A.C. Neutrophils in COVID-19. Front. Immunol. 2021, 12, 652470. [Google Scholar] [CrossRef]
- Huang, I.; Pranata, R.; Lim, M.A.; Oehadian, A.; Alisjahbana, B. C-reactive protein, procalcitonin, D-dimer, and ferritin in severe coronavirus disease-2019: A meta-analysis. Ther. Adv. Respir. Dis. 2020, 14, 1–14. [Google Scholar] [CrossRef]
- Ochoa, N.E.L.; Rodríguez, G.; Reyes, I.D.; Rivas, K.M.R.; Ramírez, C.; Duron, R.M. Differences in inflammatory markers between coronavirus disease 2019 and sepsis in hospitalised patients. Clin. Epidemiol. Glob. Health 2022, 15, 101059. [Google Scholar] [CrossRef] [PubMed]
- Claisea, C.; Salehb, J.; Rezeka, M.; Vaulont, S.; Peyssonnaux, C.; Edeas, M. Low transferrin levels predict heightened inflammation in patients with COVID-19: New insights. Int. J. Infect. Dis. 2022, 116, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Hegelund, M.H.; Glenthøj, A.; Ryrsø, C.K.; Ritz, C.; Dungu, A.M.; Sejdic, A.; Knudsen List, K.C.; Krogh-Madsen, R.; Lindegaard, B.; Anders, J.; et al. Biomarkers for iron metabolism among patients hospitalized with community-acquired pneumonia caused by infection with SARS-CoV-2, bacteria, and influenza. APMIS 2022, 130, 590–596. [Google Scholar] [CrossRef] [PubMed]
- Pieri, M.; Ciotti, M.; Nuccetelli, M.; Perrone, M.A.; Calio, M.T.; Lia, M.S.; Minieri, M.; Bernardini, S. Serum Amyloid A Protein as a useful biomarker to predict COVID-19 patients severity and prognosis. Int. Pharmacol. 2021, 95, 107512. [Google Scholar] [CrossRef]
- Minieri, M.; Di Lecce, V.N.; Lia, M.S.; Maurici, M.; Leonardis, F.; Longo, S.; Colangeli, L.; Paganelli, C.; Levantesi, S.; Terrinoni, A.; et al. Predictive value of MR-proADM in the risk stratification and in the adequate care setting of COVID-19 patients assessed at the triage of the Emergency Department. Diagnostics 2022, 12, 1971. [Google Scholar] [CrossRef]
- Ciotti, M.; Ciccozzi, M. Terrinoni, A.; Jiang, W.-C.; Wang, C.B.; Bernardini, S. The COVID-19 pandemic. Crit. Rev. Lab. Sci. 2020, 57, 365–388. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Survivors | Non-Survivors | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Min | Max | Median | 95% CI | Min | Max | Median | 95% CI | p-Value | |
| Aspartate Aminotransferase (U/L) | 15 | 59 | 29 | 21.06 to 40.08 | 12 | 1876 | 31 | 23.34 to 53.65 | 0.455 |
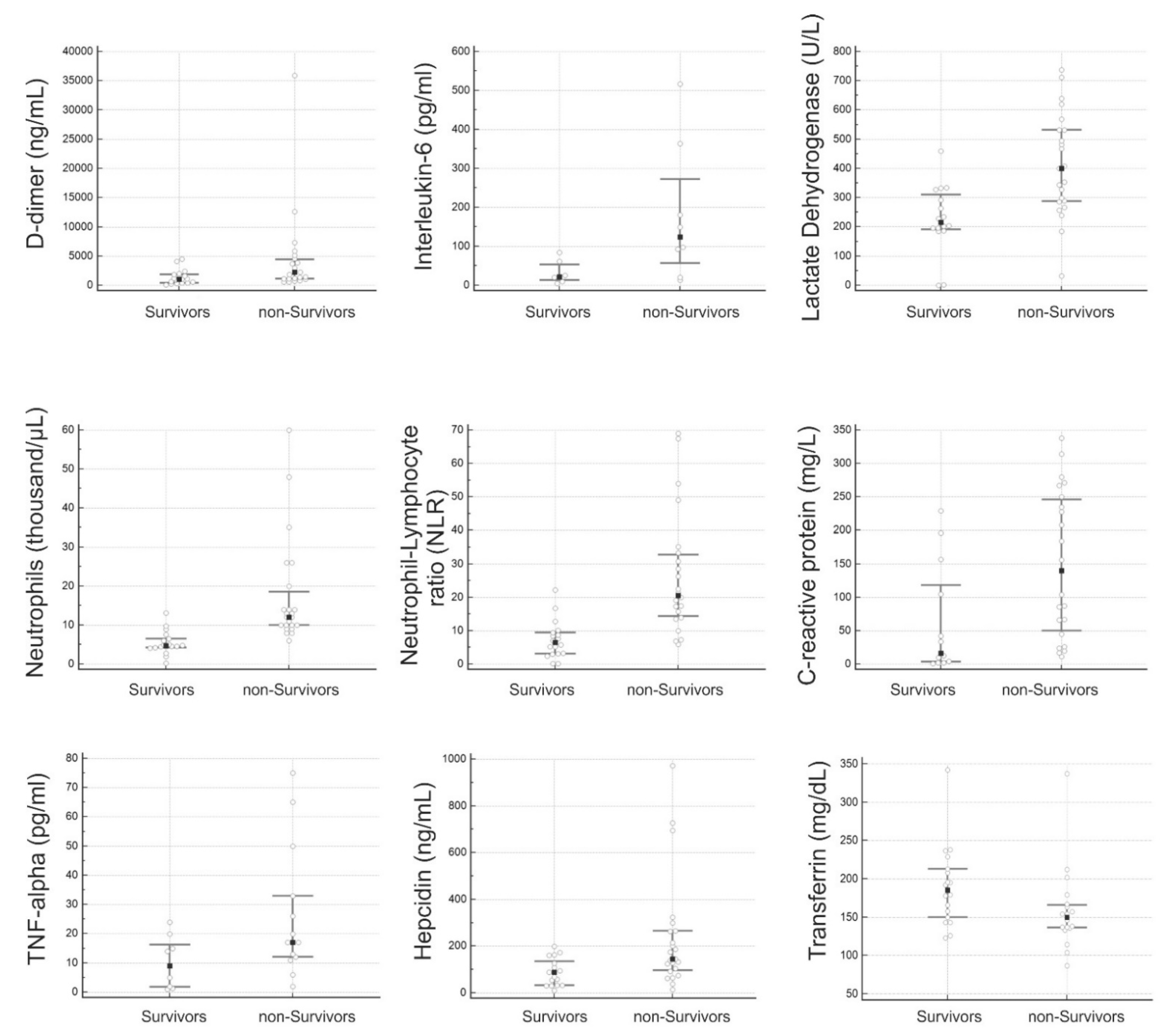
| D-dimer (ng/mL) | 80 | 4507 | 1062.5 | 485.9 to 1770.9 | 581 | 35,873 | 2223 | 1156.41 to 3802.27 | 0.014 |
| Eosinophils (thousand/μL) | 0 | 1.15 | 0.0450 | 0.020 to 0.10 | 0 | 0.81 | 0.01 | 0.0 to 0.11 | 0.86 |
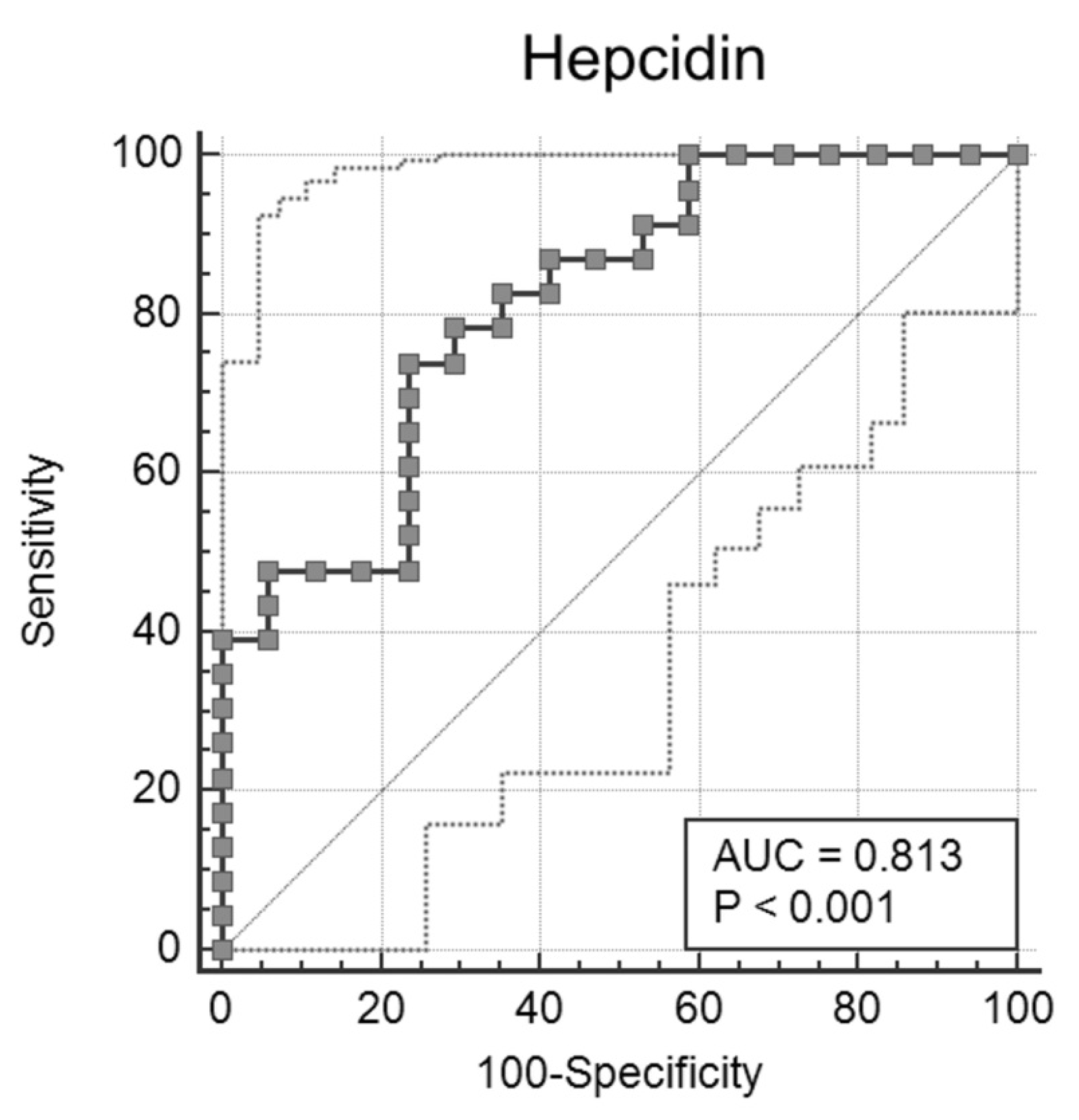
| Hepcidin (ng/mL) | 10.2 | 198.1 | 88 | 33.03 to 126.69 | 13.08 | 971.44 | 144.96 | 111.67 to 245.59 | 0.005 |
| Ferritin (ng/mL) | 198 | 1315 | 596.5 | 332.27 to 763.80 | 434.01 | 11,853 | 1335 | 487.57 to 4555.79 | 0.17 |
| Fibrinogen (mg/dL) | 95 | 919 | 450 | 367.38 to 556.62 | 36 | 1144 | 508 | 392.0 to 611.55 | 0.438 |
| Hemoglobin (ng/dL) | 8 | 13.9 | 10.95 | 9.61 to 12.02 | 7.6 | 15.3 | 9.7 | 8.7 to 11.03 | 0.52 |
| Interleukin-6 (pg/mL) | 5 | 84.3 | 22 | 7.48 to 73.10 | 13 | 517 | 124 | 19.48 to 392.95 | 0.032 |
| Lactate Dehydrogenase (U/L) | 184 | 974 | 231 | 200.47 to 329.44 | 185 | 737 | 400 | 292.48 to 518.44 | 0.003 |
| Leucocyte (thousand/μL) | 0.29 | 13 | 3.21 | 0.812 to 6.603 | 0.26 | 49 | 1.01 | 0.547 to 9.651 | 0.9895 |
| Lymphocytes (thousand/μL) | 0.27 | 21.7 | 0.915 | 0.60 to 1.39 | 0.26 | 2.59 | 0.58 | 0.56 to 1.047 | 0.168 |
| Lipase (U/L) | 9 | 137 | 30 | 24.26 to 44.42 | 7 | 328 | 28 | 23.0 to 59.49 | 0.849 |
| Neutrophils (thousand/μL) | 2.83 | 21.69 | 5.045 | 4.52 to 7.19 | 0.41 | 47.88 | 12.12 | 9.86 to 13.80 | 0.0001 |
| Neutrophil-Lymphocyte ratio (NLR) | 0.204 | 36.15 | 7.311 | 4.01 to 9.87 | 6.198 | 68.345 | 20.5 | 16.56 to 28.13 | 0.0001 |
| C-reactive protein (mg/L) | 2.3 | 228.8 | 33.9 | 7.34 to 157.62 | 11.2 | 337.6 | 148.35 | 66.93 to 236.06 | 0.015 |
| Platelets (thousand/μL) | 59 | 485 | 225.5 | 172.31 to 304.24 | 55 | 439 | 178 | 144.48 to 242.20 | 0.27 |
| Tumor Necrosis Factor-α (pg/mL) | 0.97 | 24 | 9 | 1.448 to 19.31 | 2 | 75 | 17 | 11.89 to 22.02 | 0.0438 |
| Transferrin (mg/dL) | 123 | 342 | 185.5 | 153.17 to 211.01 | 87 | 337 | 150 | 136.78 to 163.87 | 0.0245 |
| Sideremia (µg/dL) | 28 | 137 | 55.5 | 43.38 to 69.20 | 21 | 165 | 72 | 40.17 to 108.66 | 0.38 |
| n = 38; 18 Survived, 20 Died | D-Dimer (ng/mL) | Hepcidin (ng/mL) | IL-6 (pg/mL) | Lactate Dehydrogenase (U/L) | Neutrophils (Thousand/μL) | Neutrophil Lymphocyte Ratio (NLR) | C-Reactive Protein (mg/L) | Tumor Necrosis Factor-α (pg/mL) | Transferrin (mg/dL) | Sideremia (µg/dL) |
|---|---|---|---|---|---|---|---|---|---|---|
| Sensitivity (%) | 52 | 74 | 75 | 95 | 91 | 82 | 82 | 80 | 68 | 50 |
| Specificity (%) | 83 | 76 | 100 | 56 | 78 | 83 | 61 | 43 | 72 | 78 |
| Cut-off | >1981 | >127 | >84 | >234 | >7.62 | >12.75 | >41.5 | >17.35 | <157 | >70 |
| Area under the ROC curve (AUC); 95% Confidence interval | 0.726; 0.564 to 0.853 | 0.813; 0.659 to 0.919 | 0.830; 0.553 to 0.970 | 0.779; 0.617 to 0.895 | 0.853; 0.707 to 0.944 | 0.850; 0.704 to 0.942 | 0.748; 0.573 to 0.879 | 0.557; 0.302 to 0.792 | 0.716; 0.545 to 0.852 | 0.583; 0.412 to 0.741 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ciotti, M.; Nuccetelli, M.; Pieri, M.; Petrangeli, C.M.; Giovannelli, A.; Cosio, T.; Rosa, L.; Valenti, P.; Leonardis, F.; Legramante, J.M.; et al. Evaluation of Hepcidin Level in COVID-19 Patients Admitted to the Intensive Care Unit. Diagnostics 2022, 12, 2665. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12112665
Ciotti M, Nuccetelli M, Pieri M, Petrangeli CM, Giovannelli A, Cosio T, Rosa L, Valenti P, Leonardis F, Legramante JM, et al. Evaluation of Hepcidin Level in COVID-19 Patients Admitted to the Intensive Care Unit. Diagnostics. 2022; 12(11):2665. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12112665
Chicago/Turabian StyleCiotti, Marco, Marzia Nuccetelli, Massimo Pieri, Carlo Maria Petrangeli, Alfredo Giovannelli, Terenzio Cosio, Luigi Rosa, Piera Valenti, Francesca Leonardis, Jacopo Maria Legramante, and et al. 2022. "Evaluation of Hepcidin Level in COVID-19 Patients Admitted to the Intensive Care Unit" Diagnostics 12, no. 11: 2665. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12112665