
Automated Artificial Intelligence-Based Assessment of Lower Limb Alignment Validated on Weight-Bearing Pre- and Postoperative Full-Leg Radiographs

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection and Sample Description
2.2. Validation Images and Measured Parameters
- -
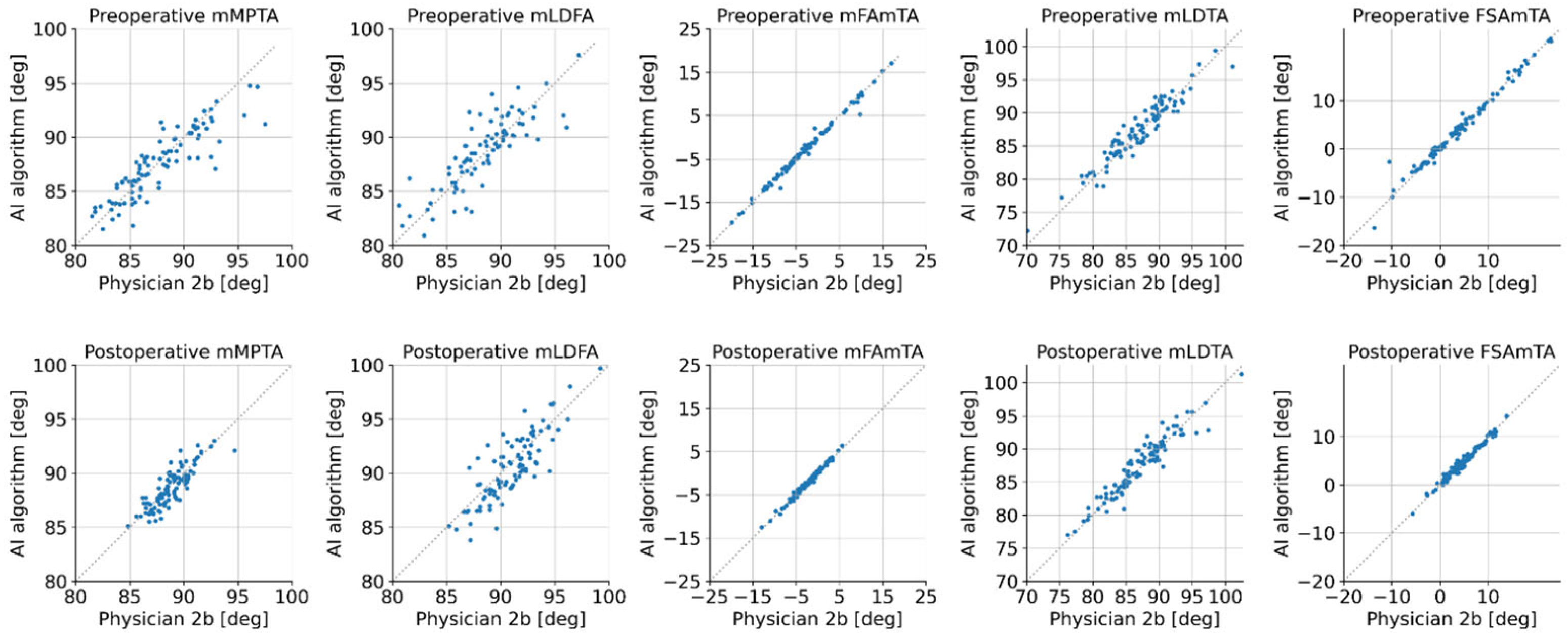
- mFAmTA: angle between the mechanical axis of the femur and the mechanical axis of the tibia, also known as the hip-knee-ankle angle.
- -
- FSAmTA: angle between the anatomical femur shaft axis and the mechanical axis of the tibia.
- -
- mMPTA: angle between the mechanical axis of the tibia and the tibial plateau knee joint line, measured on the medial side.
- -
- mLDFA: angle between the mechanical axis of the femur and the femoral condyles knee joint line, measured on the lateral side.
- -
- mLDTA: angle between the mechanical axis of the tibia and the tibial plafond, measured on the lateral side.
2.3. Manual Measurement Procedure
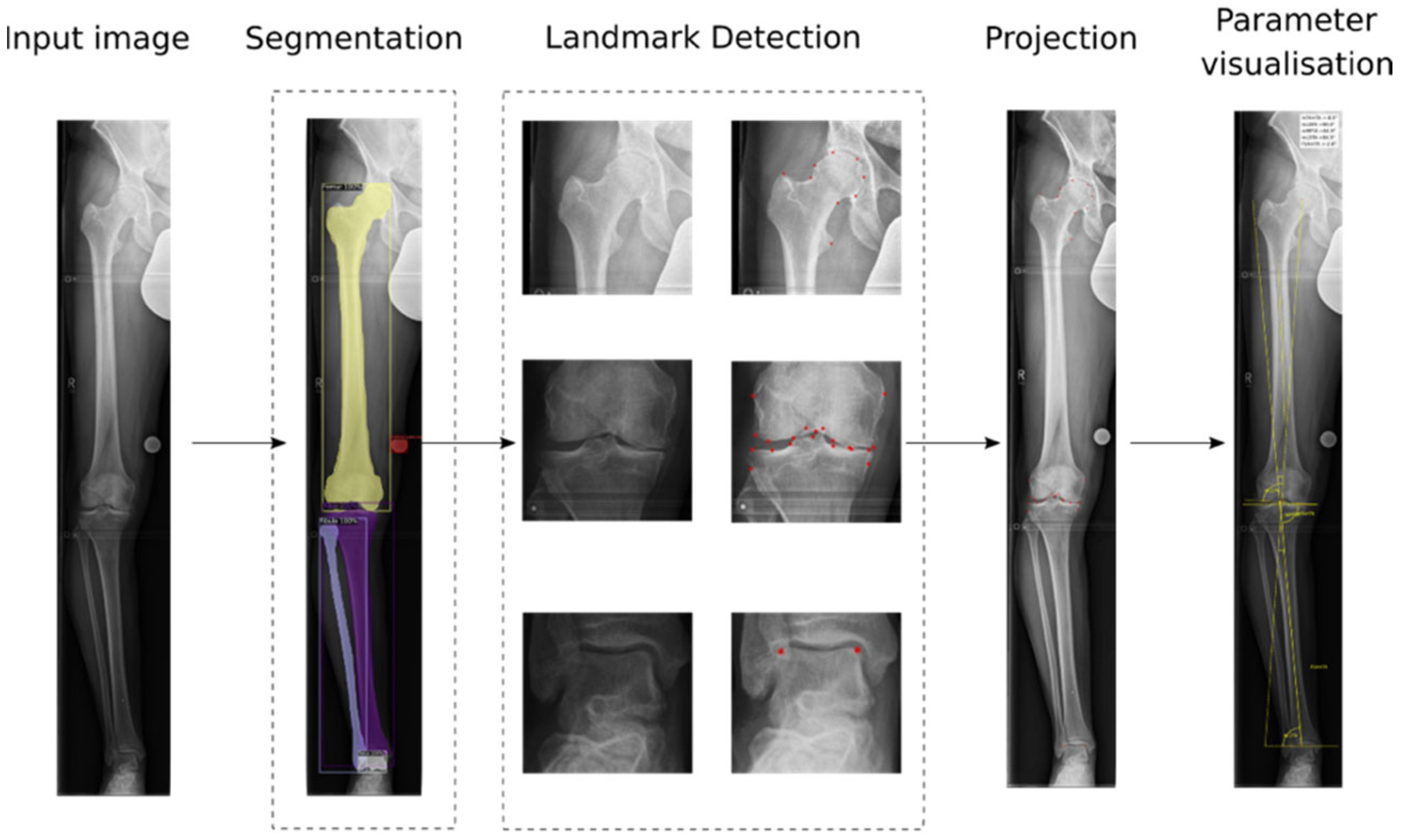
2.4. Automated AI-Workflow and Training Procedure
2.5. Preprocessing
2.6. Segmentation of Anatomical Structures and Implants
Training of the Segmentation Model
2.7. Landmark Placement
Training of the Landmark Placement Models
2.8. Projection and Parameter Computation
2.9. Statistical Analysis
3. Results
3.1. Patient Sample
3.2. Human vs. Human Intra-Rater Reliability Analysis
3.3. Human vs. Human Inter-Rater Reliability Analysis
3.4. AI Detection Rates
3.5. Human vs. AI Inter-Rater Reliability Analysis
4. Discussion
4.1. Critical Comparison with Literature
4.2. General Limitations of Method
4.3. Limitations of the Study
4.4. Outlook and Connecting Factors
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Colyn, W.; Agricola, R.; Arnout, N.; Verhaar, J.A.; Bellemans, J. How does lower leg alignment differ between soccer players, other athletes, and non-athletic controls? Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 3619–3626. [Google Scholar] [CrossRef] [PubMed]
- Thienpont, E.; Schwab, P.E.; Cornu, O.; Bellemans, J.; Victor, J. Bone morphotypes of the varus and valgus knee. Arch. Orthop. Trauma Surg. 2017, 137, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Zheng, Z.L.; Lv, J.; Hao, R.Z.; Yang, Y.P.; Zhang, Y.Z. Relationships between Morphological Changes of Lower Limbs and Gender during Medial Compartment Knee Osteoarthritis. Orthop. Surg. 2019, 11, 835–844. [Google Scholar] [CrossRef]
- Swärd, P.; Fridén, T.; Boegård, T.; Kostogiannis, I.; Neuman, P.; Roos, H. Association between varus alignment and post-traumatic osteoarthritis after anterior cruciate ligament injury. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 2040–2047. [Google Scholar] [CrossRef] [PubMed]
- Paternostre, F.; Schwab, P.E.; Thienpont, E. The difference between weight-bearing and non-weight-bearing alignment in patient-specific instrumentation planning. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 674–679. [Google Scholar] [CrossRef]
- Jud, L.; Trache, T.; Tondelli, T.; Fürnstahl, P.; Fucentese, S.F.; Vlachopoulos, L. Rotation or flexion alters mechanical leg axis measurements comparably in patients with different coronal alignment. Knee Surg. Sports Traumatol. Arthrosc. 2020, 28, 3128–3134. [Google Scholar] [CrossRef]
- Vaishya, R.; Vijay, V.; Birla, V.P.; Agarwal, A.K. Inter-observer variability and its correlation to experience in measurement of lower limb mechanical axis on long leg radiographs. J. Clin. Orthop. Trauma 2016, 7, 260–264. [Google Scholar] [CrossRef] [Green Version]
- Brar, A.S.; Howell, S.M.; Hull, M.L. What are the bias, imprecision, and limits of agreement for finding the flexion-extension plane of the knee with five tibial reference lines? Knee 2016, 23, 406–411. [Google Scholar] [CrossRef] [Green Version]
- Berenson, R.A.; Rice, T. Beyond Measurement and Reward: Methods of Motivating Quality Improvement and Accountability. Health Serv. Res. 2015, 50 (Suppl. S2), 2155–2186. [Google Scholar] [CrossRef] [Green Version]
- Goker, B.; Block, J.A. Improved precision in quantifying knee alignment angle. Clin. Orthop. Relat. Res. 2007, 458, 145–149. [Google Scholar] [CrossRef]
- Fakhrai, N.; Widhalm, P.; Chiari, C.; Weber, M.; Langs, G.; Donner, R.; Ringl, H.; Jantsch, M.; Peloschek, P. Automatic assessment of the knee alignment angle on full-limb radiographs. Eur. J. Radiol. 2010, 74, 236–240. [Google Scholar] [CrossRef]
- Federer, S.J.; Jones, G.G. Artificial intelligence in orthopaedics: A scoping review. PLoS ONE 2021, 16, e0260471. [Google Scholar] [CrossRef] [PubMed]
- Tack, A.; Preim, B.; Zachow, S. Fully automated Assessment of Knee Alignment from Full-Leg X-rays employing a “YOLOv4 And Resnet Landmark regression Algorithm” (YARLA): Data from the Osteoarthritis Initiative. Comput. Methods Programs Biomed. 2021, 205, 106080. [Google Scholar] [CrossRef] [PubMed]
- Simon, S.; Schwarz, G.M.; Aichmair, A.; Frank, B.J.H.; Hummer, A.; DiFranco, M.D.; Dominkus, M.; Hofstaetter, J.G. Fully automated deep learning for knee alignment assessment in lower extremity radiographs: A cross-sectional diagnostic study. Skelet. Radiol. 2022, 51, 1249–1259. [Google Scholar] [CrossRef] [PubMed]
- Sariyar, M.; Holm, J. Medical Informatics in a Tension between Black-Box AI and Trust. Stud. Health Technol. Inform. 2022, 289, 41–44. [Google Scholar]
- Kelly, B.S.; Judge, C.; Bollard, S.M.; Clifford, S.M.; Healy, G.M.; Aziz, A.; Mathur, P.; Islam, S.; Yeom, K.W.; Lawlor, A.; et al. Radiology artificial intelligence: A systematic review and evaluation of methods (RAISE). Eur. Radiol. 2022, 1–10. [Google Scholar]
- Rosery, H.; Schönfelder, T. Healthcare System Stakeholders. In White Paper on Joint Replacement: Status of Hip and Knee Arthroplasty Care in Germany; Bleß, H.H., Kip, M., Eds.; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Lützner, J.; Lange, T.; Schmitt, J.; Kopkow, C.; Aringer, M.; Böhle, E.; Bork, H.; Dreinhöfer, K.; Friederich, N.; Gravius, S. S2k-Leitlinie: Indikation Knieendoprothese. Der Orthopäde 2018, 47, 777–781. [Google Scholar] [CrossRef]
- Osmanski-Zenk, K.; Klinder, A.; Haas, H.; Mittelmeier, W. Influence of Revision Surgeries and Revision Rate on Quality Indicators in Certified Centres for Joint Replacement (EndoProthetikZentren). Z. Orthop. Unf. 2020, 158, 481–489. [Google Scholar] [CrossRef]
- Schröter, S.; Müller-Rath, R. Registerforschung rund ums Knie: DEKOR, DART und KnorpelRegister DGOU: Aktive Wissenschaft für jedermann. Knie J. 2021, 3, 154–160. [Google Scholar] [CrossRef]
- He, K.; Gkioxari, G.; Dollár, P.; Girshick, R. Mask r-cnn. In Proceedings of the IEEE International Conference on Computer Vision, Venice, Italy, 22–29 October 2017. [Google Scholar]
- Paszke, A.; Gross, S.; Massa, F.; Lerer, A.; Bradbury, J.; Chanan, G. Pytorch: An imperative style, high-performance deep learning library. Adv. Neural Inf. Process. Syst. 2019, 32, 1–12. [Google Scholar]
- Ronneberger, O.; Fischer, P.; Brox, T. U-net: Convolutional networks for biomedical image segmentation. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Munich, Germany, 5–9 October 2015; Springer: Berlin/Heidelberg, Germany, 2015. [Google Scholar]
- Abadi, M.; Agarwal, A.; Barham, P.; Brevdo, E.; Chen, Z.; Citro, C. Tensorflow: Large-scale machine learning on heterogeneous distributed systems. arXiv Prepr. 2016, arXiv:1603.04467. [Google Scholar]
- Brouwer, R.W.; Jakma, T.S.; Brouwer, K.H.; Verhaar, J.A. Pitfalls in determining knee alignment: A radiographic cadaver study. J. Knee Surg. 2007, 20, 210–215. [Google Scholar] [CrossRef] [PubMed]
- Zahn, R.K.; Renner, L.; Perka, C.; Hommel, H. Weight-bearing radiography depends on limb loading. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 1470–1476. [Google Scholar] [CrossRef]
- Nishida, R.; Hiranaka, T.; Kamenaga, T.; Hida, Y.; Fujishiro, T.; Okamoto, K.; Kuroda, R.; Matsumoto, T. Impact of joint line orientation on clinical outcomes in bilateral Oxford mobile-bearing unicompartmental knee arthroplasty. Knee 2021, 28, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Labott, J.R.; Warne, C.N.; Wyles, C.C.; Trousdale, R.T. Incidence of Leg-Length Discrepancy After Index Hinge Total Knee Arthroplasty. J. Arthroplast. 2021, 36, 1607–1610. [Google Scholar] [CrossRef] [PubMed]
- Hwang, D.; Ahn, S.; Park, Y.B.; Kim, S.H.; Han, H.S.; Lee, M.C.; Ro, D.H. Deep Learning-Based Muscle Segmentation and Quantification of Full-Leg Plain Radiograph for Sarcopenia Screening in Patients Undergoing Total Knee Arthroplasty. J. Clin. Med. 2022, 11, 3612. [Google Scholar] [CrossRef]
- Ren, M.; Yi, P.H. Artificial intelligence in orthopedic implant model classification: A systematic review. Skelet. Radiol. 2022, 51, 407–416. [Google Scholar] [CrossRef] [PubMed]
- Bonakdari, H.; Jamshidi, A.; Pelletier, J.P.; Abram, F.; Tardif, G.; Martel-Pelletier, J. A warning machine learning algorithm for early knee osteoarthritis structural progressor patient screening. Ther. Adv. Musculoskelet. Dis. 2021, 13, 1759720X21993254. [Google Scholar] [CrossRef]
- Bellemans, J.; Colyn, W.; Vandenneucker, H.; Victor, J. The Chitranjan Ranawat award: Is neutral mechanical alignment normal for all patients? The concept of constitutional varus. Clin. Orthop. Relat. Res. 2012, 470, 45–53. [Google Scholar] [CrossRef] [Green Version]
- Rivière, C.; Villet, L.; Jeremic, D.; Vendittoli, P.A. What you need to know about kinematic alignment for total knee arthroplasty. Orthop. Traumatol. Surg. Res. 2021, 107, 102773. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Intra-Rater Reliability (Rater 2a vs. Rater 2b) | ||||||
|---|---|---|---|---|---|---|
| Statistical Method | mMPTA [°] | mLDFA [°] | mFAmTA [°] | mLDTA [°] | FSAmTA [°] | |
| Preoperative | ICC (95% CI) | 0.97 (0.95–0.98) | 0.95 (0.93–0.97) | 1.0 (1.0–1.0) | 0.97 (0.96–0.98) | 1.0 (1.0–1.0) |
| Mean error (95% CI) | −0.07 (−0.27–0.13) | −0.02 (−0.22–0.19) | −0.01 (−0.06–0.05) | −0.13 (−0.37–0.12) | −0.05 (−0.14–0.03) | |
| SD | 0.97 | 1.0 | 0.26 | 1.19 | 0.4 | |
| RMSE | 0.97 | 1.0 | 0.26 | 1.2 | 0.41 | |
| Pearson correlation r (p-value) | 0.97 (<0.001) | 0.95 (<0.001) | 1.0 (<0.001) | 0.97 (<0.001) | 1.0 (<0.001) | |
| Postoperative | ICC (95% CI) | 0.96 (0.94–0.97) | 0.97 (0.95–0.98) | 1.0 (0.99–1.0) | 0.96 (0.94–0.97) | 0.99 (0.99–1.0) |
| Mean error (95% CI) | 0.0 (−0.1–0.09) | −0.05 (−0.2–0.1) | −0.01 (−0.07–0.04) | 0.15 (−0.1–0.4) | 0.01 (−0.06–0.08) | |
| SD | 0.48 | 0.77 | 0.28 | 1.29 | 0.37 | |
| RMSE | 0.48 | 0.77 | 0.28 | 1.3 | 0.37 | |
| Pearson correlation r (p-value) | 0.96 (<0.001) | 0.97 (<0.001) | 1.0 (<0.001) | 0.96 (<0.001) | 1.0 (<0.001) | |
| Inter-Rater Reliability (Rater 1 vs. Rater 2a) | ||||||
|---|---|---|---|---|---|---|
| Statistical Method | mMPTA [°] | mLDFA [°] | mFAmTA [°] | mLDTA [°] | FSAmTA [°] | |
| Preoperative | ICC (95% CI) | 0.91 (0.87–0.94) | 0.91 (0.87–0.94) | 0.99 (0.99–0.99) | 0.88 (0.82–0.92) | 0.99 (0.99–0.99) |
| Mean error (95% CI) | 0.18 (−0.14–0.49) | 0.07 (−0.19–0.33) | 0.09 (−0.14–0.32) | −0.46 (−0.91–−0.01) | 0.1 (−0.11–0.31) | |
| SD | 1.53 | 1.29 | 1.11 | 2.0 | 1.03 | |
| RMSE | 1.55 | 1.29 | 1.11 | 2.0 | 1.03 | |
| Pearson correlation r (p-value) | 0.92 (<0.001) | 0.91 (<0.001) | 0.99 (<0.001) | 0.89 (<0.001) | 0.99 (<0.001) | |
| Inter-rater Reliability (Rater 1 vs. Rater 2b) | ||||||
| Preoperative | ICC (95% CI) | 0.89 (0.84–0.93) | 0.92 (0.88–0.95) | 0.99 (0.99–0.99) | 0.85 (0.78–0.90) | 0.99 (0.99–0.99) |
| Mean error (95% CI) | 0.11 (−0.24–0.45) | 0.05 (−0.2–0.31) | 0.08 (−0.14–0.31) | −0.59 (−1.09–−0.09) | 0.05 (−0.16–0.26) | |
| SD | 1.69 | 1.26 | 1.09 | 2.43 | 1.05 | |
| RMSE | 1.7 | 1.26 | 1.1 | 2.5 | 1.05 | |
| Pearson correlation r (p-value) | 0.89 (<0.001) | 0.92 (<0.001) | 0.99 (<0.001) | 0.87 (<0.001) | 0.99 (<0.001) | |
| Inter-Rater Reliability (AI method vs. Rater 1) | ||||||
|---|---|---|---|---|---|---|
| Statistical Method | mMPTA [°] | mLDFA [°] | mFAmTA [°] | mLDTA [°] | FSAmTA [°] | |
| Preoperative | ICC (95% CI) | 0.86 (0.80–0.91) | 0.84 (0.76–0.89) | 1.0 (0.99–1.0) | 0.88 (0.77–0.93) | 0.99 (0.98–0.99) |
| Mean error (95% CI) | −0.29 (−0.66–0.08) | 0.15 (−0.26–0.56) | −0.03 (−0.17–0.11) | 0.97 (0.56–1.38) | 0.24 (0.0–0.48) | |
| SD | 1.8 | 1.92 | 0.67 | 1.98 | 1.15 | |
| RMSE | 1.83 | 1.93 | 0.67 | 2.2 | 1.18 | |
| Pearson correlation r (p-value) | 0.87 (<0.001) | 0.84 (<0.001) | 1.0 (<0.001) | 0.90 (<0.001) | 0.99 (<0.001) | |
| Inter-rater Reliability (AI method vs. Rater 2a) | ||||||
| Preoperative | ICC (95% CI) | 0.90 (0.85–0.93) | 0.80 (0.71–0.87) | 0.99 (0.99–1.0) | 0.95 (0.92–0.97) | 0.99 (0.98–0.99) |
| Mean error (95% CI) | −0.19 (−0.53–0.14) | 0.19 (−0.27–0.65) | 0.0 (−0.19–0.19) | 0.49 (0.21–0.78) | 0.26 (0.02–0.49) | |
| SD | 1.61 | 2.16 | 0.89 | 1.38 | 1.14 | |
| RMSE | 1.62 | 2.17 | 0.89 | 1.46 | 1.16 | |
| Pearson correlation r (p-value) | 0.91 (<0.001) | 0.81 (<0.001) | 0.99 (<0.001) | 0.96 (<0.001) | 0.99 (<0.001) | |
| Postoperative | ICC (95% CI) | 0.83 (0.76–0.88) | 0.87 (0.81–0.91) | 0.99 (0.98–0.99) | 0.94 (0.91–0.96) | 0.99 (0.98–0.99) |
| Mean error (95% CI) | −0.13 (−0.32–0.07) | −0.31 (−0.63–0.01) | 0.15 (0.05–0.24) | 0.23 (−0.06–0.52) | −0.07 (−0.17–0.04) | |
| SD | 1.0 | 1.61 | 0.48 | 1.47 | 0.53 | |
| RMSE | 1.0 | 1.64 | 0.51 | 1.49 | 0.53 | |
| Pearson correlation r (p-value) | 0.83 (<0.001) | 0.88 (<0.001) | 0.99 (<0.001) | 0.94 (<0.001) | 0.99 (<0.001) | |
| Inter-rater Reliability (AI method vs. Rater 2b) | ||||||
| Preoperative | ICC (95% CI) | 0.88 (0.83–0.92) | 0.83 (0.75–0.88) | 0.99 (0.99–1.0) | 0.95 (0.92–0.97) | 0.99 (0.98–0.99) |
| Mean error (95% CI) | −0.26 (−0.61–0.08) | 0.19 (−0.24–0.62) | −0.01 (−0.18–0.17) | 0.35 (0.04–0.65) | 0.2 (−0.02–0.43) | |
| SD | 1.68 | 2.02 | 0.82 | 1.49 | 1.11 | |
| RMSE | 1.7 | 2.03 | 0.82 | 1.53 | 1.13 | |
| Pearson correlation r (p-value) | 0.89 (<0.001) | 0.83 (<0.001) | 0.99 (<0.001) | 0.95 (<0.001) | 0.99 (<0.001) | |
| Postoperative | ICC (95% CI) | 0.85 (0.78–0.89) | 0.85 (0.79–0.90) | 0.99 (0.98–0.99) | 0.95 (0.92–0.96) | 0.99 (0.98–0.99) |
| Mean error (95% CI) | −0.14 (−0.33–0.04) | −0.39 (−0.73–−0.06) | 0.16 (0.07–0.25) | 0.37 (0.09–0.65) | −0.08 (−0.2–0.03) | |
| SD | 0.94 | 1.65 | 0.43 | 1.42 | 0.57 | |
| RMSE | 0.95 | 1.7 | 0.46 | 1.46 | 0.58 | |
| Pearson correlation r (p-value) | 0.85 (<0.001) | 0.87 (<0.001) | 0.99 (<0.001) | 0.95 (<0.001) | 0.99 (<0.001) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Erne, F.; Grover, P.; Dreischarf, M.; Reumann, M.K.; Saul, D.; Histing, T.; Nüssler, A.K.; Springer, F.; Scholl, C. Automated Artificial Intelligence-Based Assessment of Lower Limb Alignment Validated on Weight-Bearing Pre- and Postoperative Full-Leg Radiographs. Diagnostics 2022, 12, 2679. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12112679
Erne F, Grover P, Dreischarf M, Reumann MK, Saul D, Histing T, Nüssler AK, Springer F, Scholl C. Automated Artificial Intelligence-Based Assessment of Lower Limb Alignment Validated on Weight-Bearing Pre- and Postoperative Full-Leg Radiographs. Diagnostics. 2022; 12(11):2679. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12112679
Chicago/Turabian StyleErne, Felix, Priyanka Grover, Marcel Dreischarf, Marie K. Reumann, Dominik Saul, Tina Histing, Andreas K. Nüssler, Fabian Springer, and Carolin Scholl. 2022. "Automated Artificial Intelligence-Based Assessment of Lower Limb Alignment Validated on Weight-Bearing Pre- and Postoperative Full-Leg Radiographs" Diagnostics 12, no. 11: 2679. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12112679