
Predicting IDH Mutation Status in Low-Grade Gliomas Based on Optimal Radiomic Features Combined with Multi-Sequence Magnetic Resonance Imaging


Abstract
:1. Introduction
2. Materials and Methods
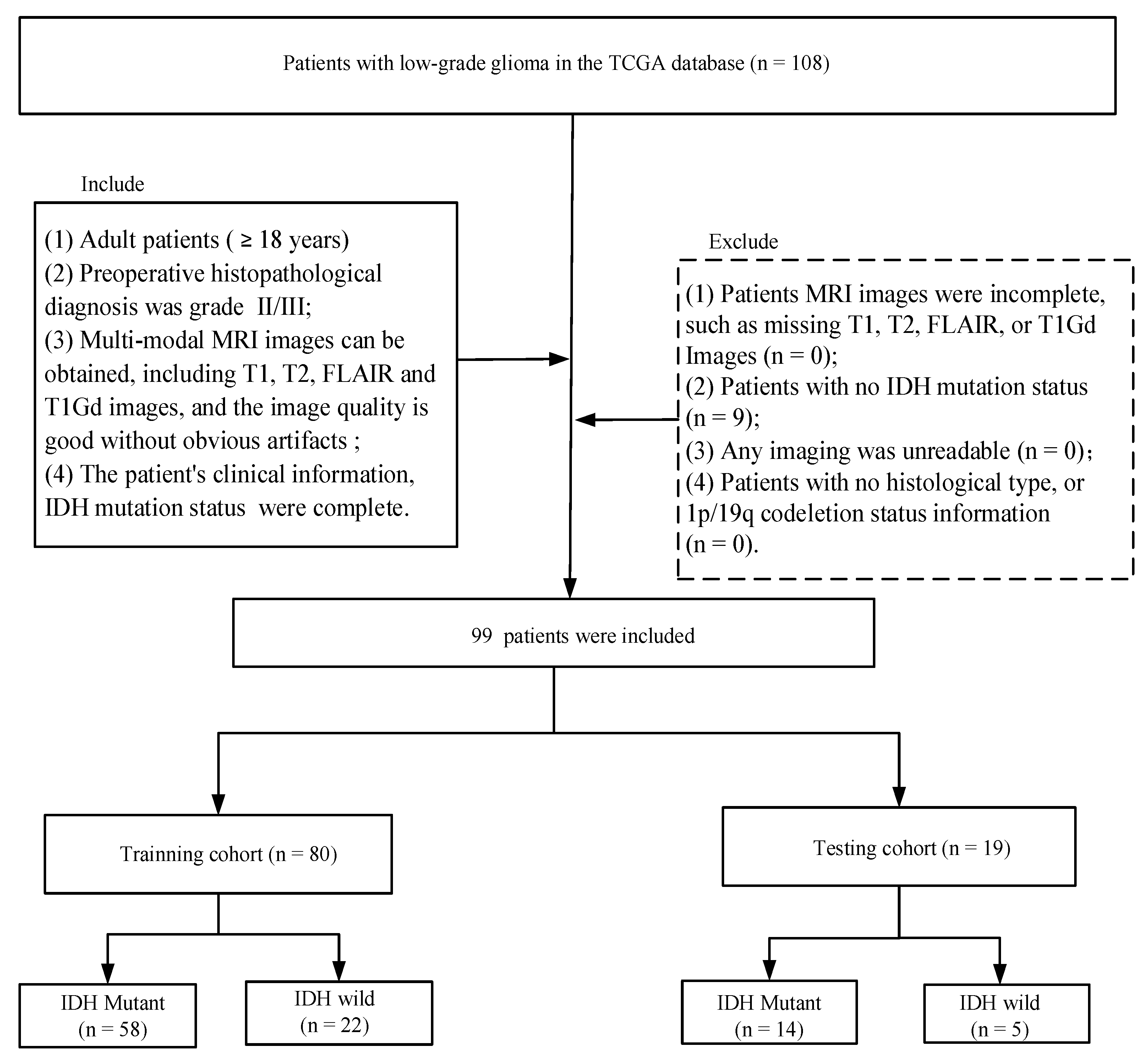
2.1. Data Cohort
2.2. Imaging Data Acquisition
2.3. Radiomics Feature Extraction
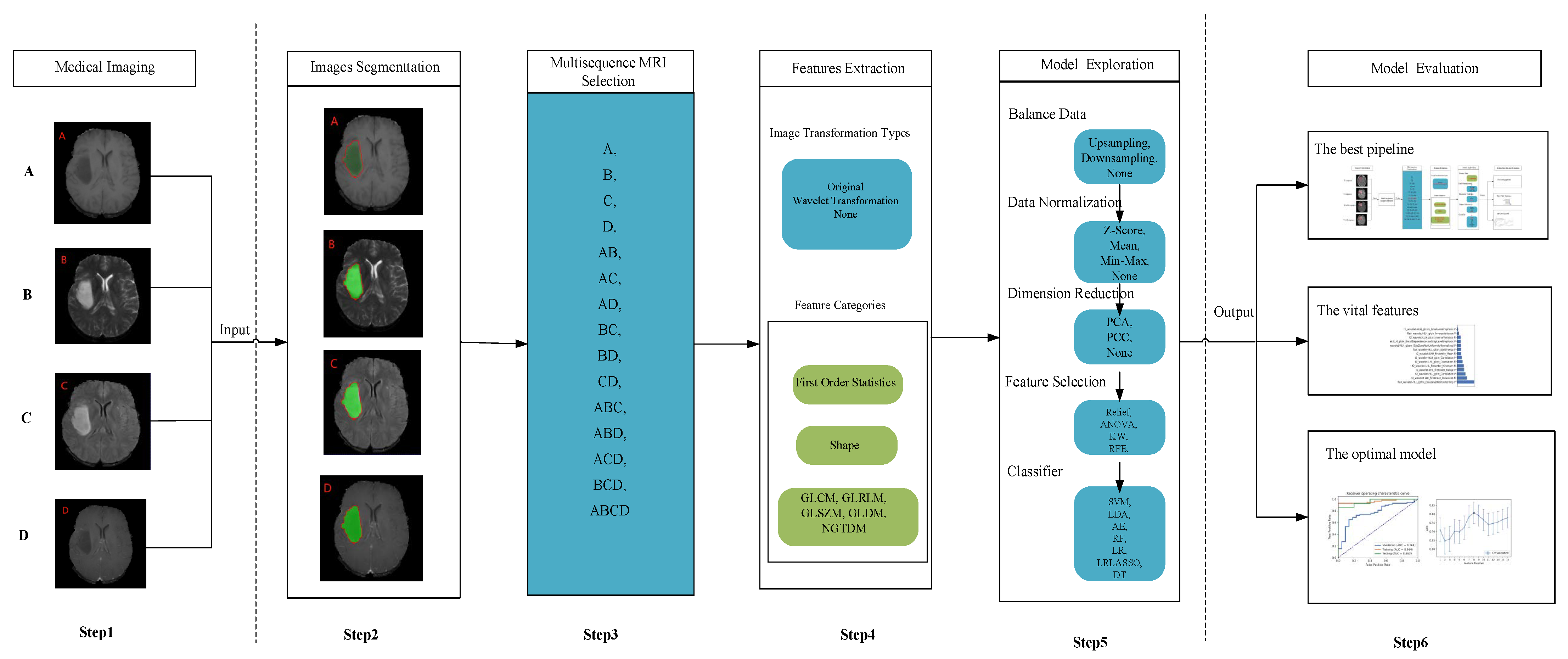
2.4. “6-Step” General Radiomics Model Exploration
2.5. Model Evaluation
2.6. Statistical Analysis
3. Results
3.1. Clinical Characteristics
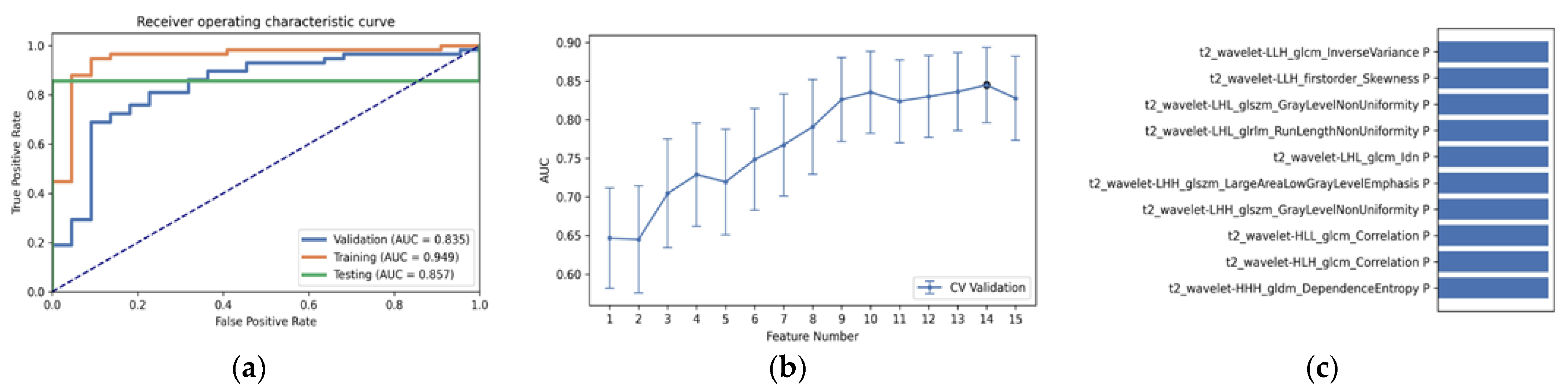
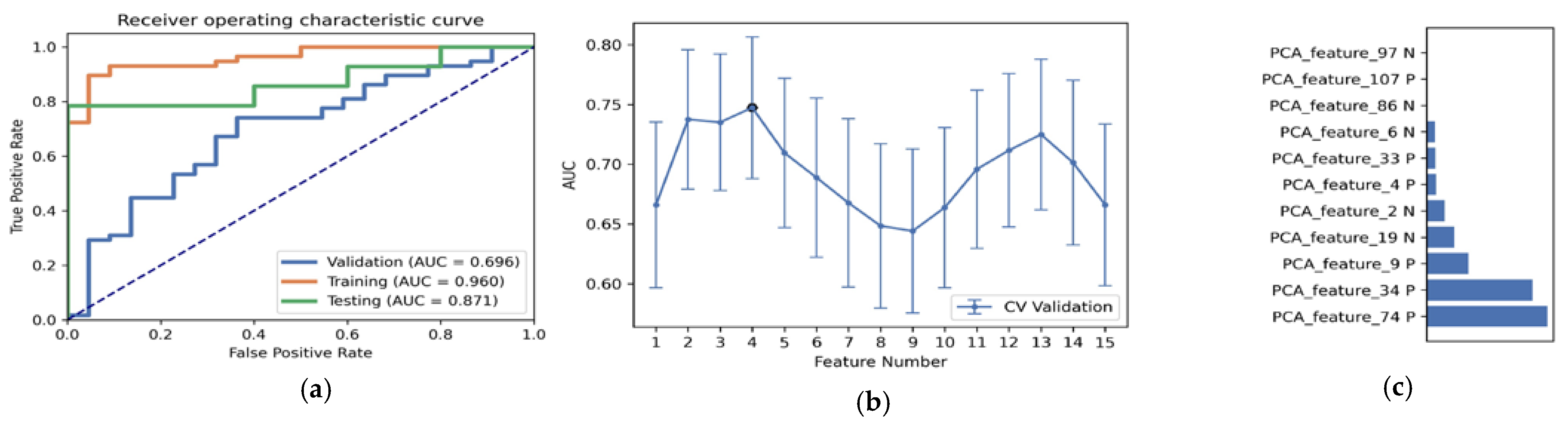
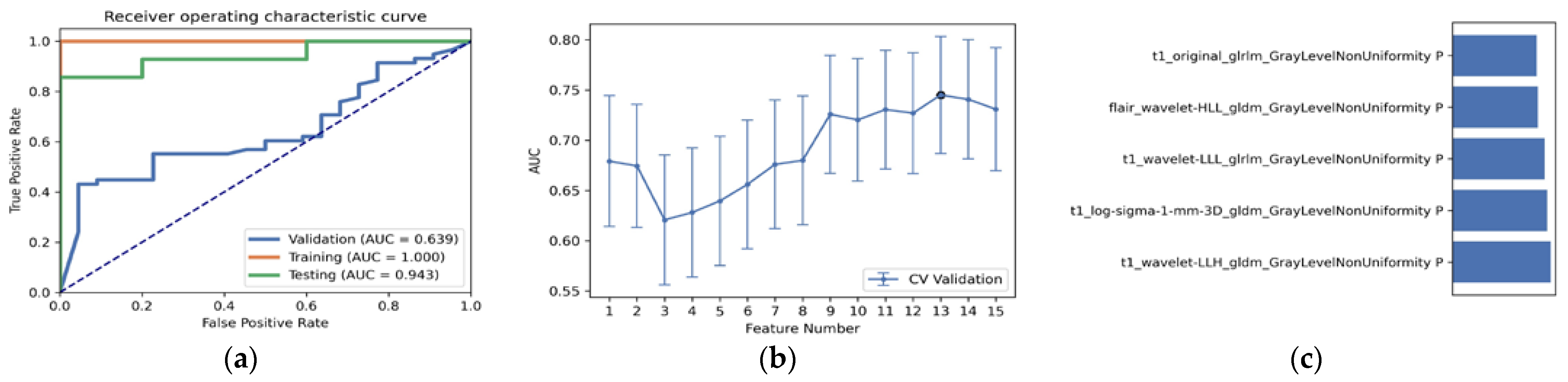
3.2. Comparison of the Performance of Different Combined Multi-Sequence MRIs Generated by the “6-Step” General Radiomics Model
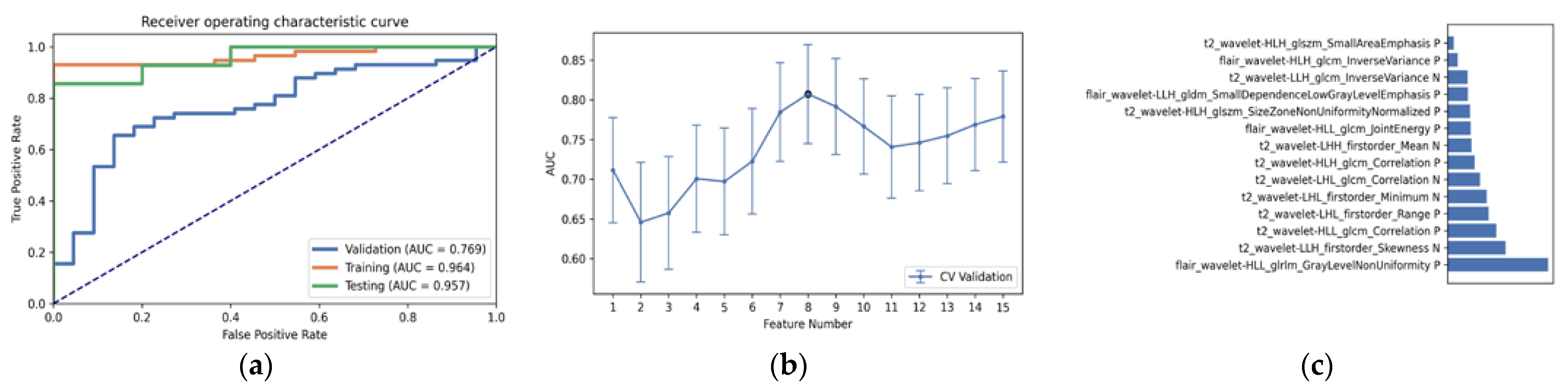
3.3. Statistical Result and Feature Analysis
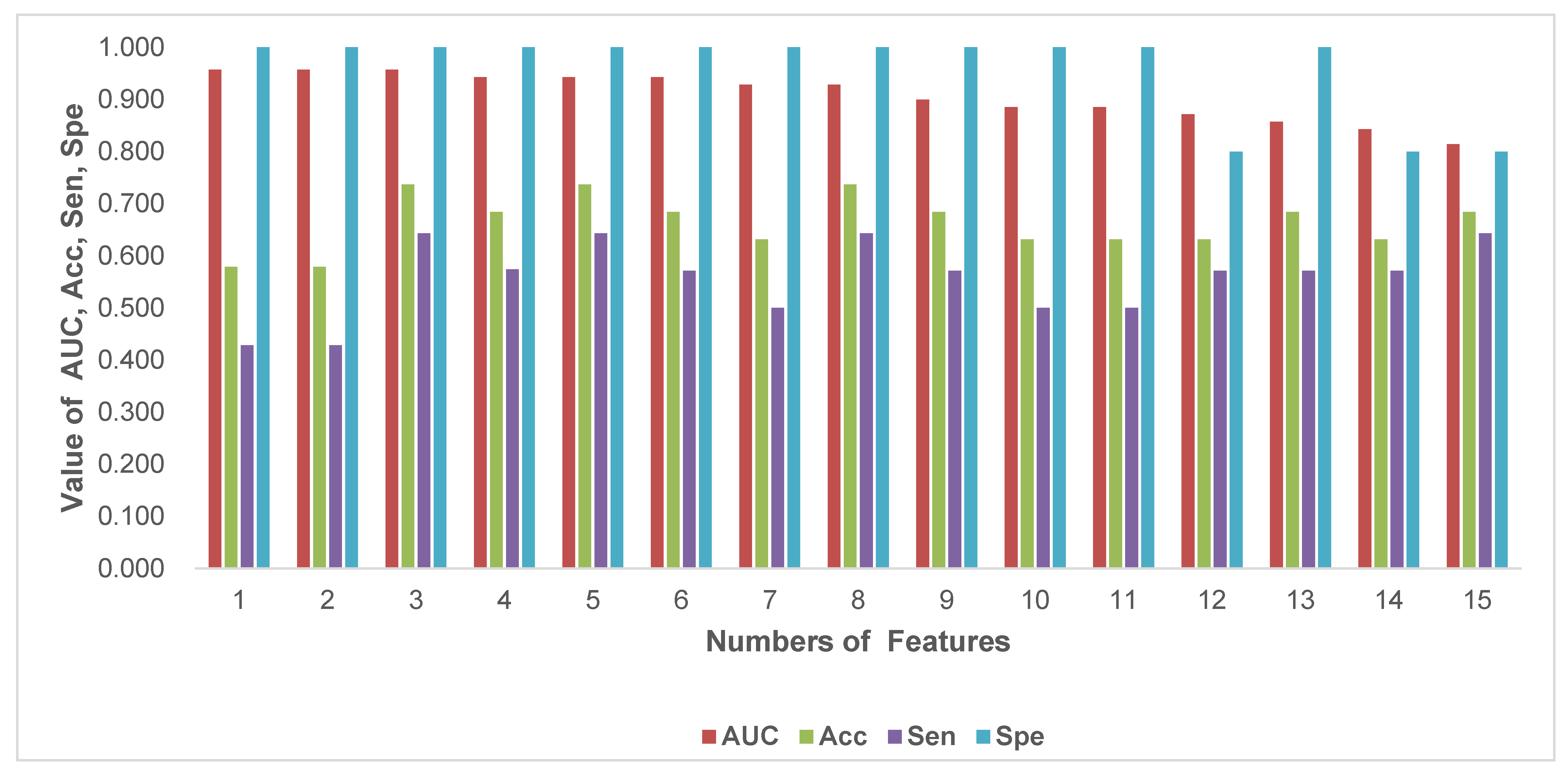
3.4. The Accuracy, Stability and Efficiency of the “6-Step” General Radiomics Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yang, K.; Wu, Z.; Zhang, H.; Zhang, N.; Wu, W.; Wang, Z.; Dai, Z.; Zhang, X.; Zhang, L.; Peng, Y.; et al. Glioma targeted therapy: Insight into future of molecular approaches. Mol. Cancer. 2022, 21, 39. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.S.; Ahn, S.S.; Chang, J.H.; Kang, S.-G.; Kim, E.H.; Kim, S.H.; Jain, R.; Lee, S.-K. Machine learning and radiomic phenotyping of lower grade gliomas: Improving survival prediction. Eur. Radiol. 2020, 307, 3834–3842. [Google Scholar] [CrossRef] [PubMed]
- Galbraith, K.; Snuderl, M. Molecular Pathology of Gliomas. Surg. Pathol. Clin. 2021, 14, 379–386. [Google Scholar] [CrossRef] [PubMed]
- Weller, M.; van den Bent, M.; Tonn, J.C. European Association for Neuro-Oncology (EANO) guideline on the diagnosis and treatment of adult astrocytic and oligodendroglial gliomas. Lancet Oncol. 2017, 18, e315–e329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.-B.; Karpova, A.; Gritsenko, M.A.; Kyle, J.E.; Cao, S.; Li, Y.; Rykunov, D.; Colaprico, A.; Rothstein, J.H.; Hong, R.; et al. Clinical Proteomic Tumor Analysis Consortium. Proteogenomic and metabolomic characterization of human glioblastoma. Cancer Cell. 2021, 39, 509–528. [Google Scholar] [CrossRef]
- Louis, D.N.; Perry, A.; Reifenberger, G.; Von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [Green Version]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary. Neuro Oncol. 2021, 23, 1231–1251. [Google Scholar] [CrossRef]
- Lambin, P.; Leijenaar, R.T.H.; Deist, T.M.; Peerlings, J.; de Jong, E.E.C.; van Timmeren, J.; Sanduleanu, S.; Larue, R.T.H.M.; Even, A.J.G.; Jochems, A.; et al. Radiomics: The bridge between medical imaging and personalized medicine. Nat. Rev. Clin. Oncol. 2017, 14, 749–762. [Google Scholar] [CrossRef] [Green Version]
- Lambin, P.; Velazquez, E.; Leijenaar, R.; Carvalho, S.; van Stiphout, R.G.P.M.; Granton, P.; Zegers, C.M.L.; Gillies, R.; Boellard, R.; Dekker, A.; et al. Radiomics: Extracting more information from medical images using advanced feature analysis. Eur. J. Cancer 2012, 48, 441–446. [Google Scholar] [CrossRef] [Green Version]
- Aerts, H.J.W.L.; Velazquez, E.R.; Leijenaar, R.T.H.; Parmar, C.; Grossmann, P.; Carvalho, S.; Bussink, J.; Monshouwer, R.; Haibe-Kains, B.; Rietveld, D.; et al. Decoding tumour phenotype by noninvasive imaging using a quantitative radiomics approach. Nat. Commun. 2014, 5, 4644. [Google Scholar] [CrossRef]
- Luo, H.; Zhuang, Q.; Wang, Y.; Abudumijiti, A.; Shi, K.; Rominger, A.; Chen, H.; Yang, Z.; Tran, V.; Wu, G.; et al. A novel image signature-based radiomics method to achieve precise diagnosis and prognostic stratification of gliomas. Lab. Investig. 2021, 101, 450–462. [Google Scholar] [CrossRef] [PubMed]
- Pyka, T.; Krzyzanowska, I.; Rominger, A.; Delbridge, C.; Meyer, B.; Boeckh-Behrens, T.; Zimmer, C.; Gempt, J. Multiparametric Characterization of Intracranial Gliomas Using Dynamic [18F]FET-PET and Magnetic Resonance Spectroscopy. Diagnostics 2022, 12, 2331. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Tian, Q.; Wang, L.; Liu, Y.; Li, B.; Liang, Z.; Gao, P.; Zheng, K.; Zhao, B.; Lu, H. Radiomics strategy for molecular subtype stratification of lower-grade glioma: Detecting IDH and TP53 mutations based on multimodal MRI. J. Magn. Reson. Imaging 2018, 48, 916–926. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Jung, S.Y.; Park, J.E.; Jo, Y.; Park, S.Y.; Nam, S.J.; Kim, J.H.; Kim, H.S. Diffusion-and perfusion-weighted MRI radiomics model may predict isocitrate dehydrogenase (IDH) mutation and tumor aggressiveness in diffuse lower grade glioma. Eur. Radiol. 2020, 30, 2142–2151. [Google Scholar] [CrossRef]
- Liu, X.; Li, Y.; Li, S.; Fan, X.; Sun, Z.; Yang, Z.; Wang, K.; Zhang, Z.; Jiang, T.; Liu, Y.; et al. IDH mutation-specific radiomic signature in lower-grade gliomas. Aging 2019, 11, 673. [Google Scholar] [CrossRef]
- Wu, S.; Meng, J.; Yu, Q.; Li, P.; Fu, S. Radiomics-based machine learning methods for isocitrate dehydrogenase genotype prediction of diffuse gliomas. J. Cancer Res. Clin. Oncol. 2019, 145, 543–550. [Google Scholar] [CrossRef] [Green Version]
- Tan, Y.; Zhang, S.T.; Wei, J.W.; Dong, D.; Wang, X.C.; Yang, G.Q.; Tian, J.; Zhang, H. A radiomics nomogram may improve the prediction of IDH genotype for astrocytoma before surgery. Eur. Radiol. 2019, 29, 3325–3337. [Google Scholar] [CrossRef]
- Santinha, J.; Matos, C.; Figueiredo, M.; Papanikolaou, N. Improving performance and generalizability in radiogenomics: A pilot study for prediction of IDH1/2 mutation status in gliomas with multicentric data. J. Med. Imaging 2021, 8, 031905. [Google Scholar] [CrossRef]
- Li, Y.; Ammari, S.; Lawrance, L.; Quillent, A.; Assi, T.; Lassau, N.; Chouzenoux, E. Radiomics-Based Method for Predicting the Glioma Subtype as Defined by Tumor Grade, IDH Mutation, and 1p/19q Codeletion. Cancers 2022, 14, 1778. [Google Scholar] [CrossRef]
- Li, Y.; Qin, Q.; Zhang, Y.; Cao, Y. Noninvasive Determination of the IDH Status of Gliomas Using MRI and MRI-Based Radiomics: Impact on Diagnosis and Prognosis. Curr. Oncol. 2022, 29, 6893–6907. [Google Scholar] [CrossRef]
- Choi, Y.S.; Bae, S.; Chang, J.H.; Kang, S.G.; Kim, S.H.; Kim, J.; Rim, T.H.; Choi, S.H.; Jain, R.; Lee, S.K. Fully automated hybrid approach to predict the IDH mutation status of gliomas via deep learning and radiomics. Neuro Oncol. 2021, 23, 304–313. [Google Scholar] [CrossRef] [PubMed]
- Bi, W.L.; Hosny, A.; Schabath, M.B.; Giger, M.L.; Birkbak, N.; Mehrtash, A.; Allison, T.; Arnaout, O.; Abbosh, C.; Dunn, I.F.; et al. Artificial Intelligence in Cancer Imaging: Clinical Challenges and Applications. CA Cancer J. Clin. 2019, 69, 127–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, X.L.; Ren, J.L.; Yao, T.Y.; Zhao, D.; Niu, J. Radiomics based on multi-sequence magnetic resonance imaging for the preoperative prediction of peritoneal metastasis in ovarian cancer. Eur. Radiol. 2021, 31, 8438–8446. [Google Scholar] [CrossRef] [PubMed]
- Rohlfing, T.; Zahr, N.M.; Sullivan, E.V.; Pfefferbaum, A. The SRI24 multichannel atlas of normal adult human brain structure. Hum. Brain Mapp. 2010, 31, 798–819. [Google Scholar] [CrossRef] [Green Version]
- Bakas, S.; Zeng, K.; Sotiras, A.; Rathore, S.; Akbari, H.; Gaonkar, B.; Rozycki, M.; Pati, S.; Davatzikos, C. GLISTRboost: Combining multimodal MRI segmentation, registration, and biophysical tumor growth modeling with gradient boosting machines for glioma segmentation. Brainlesion 2015, 9556, 144–155. [Google Scholar] [CrossRef] [Green Version]
- Bakas, S.; Akbari, H.; Sotiras, A.; Bilello, M.; Rozycki, M.; Kirby, J.S.; Freymann, J.B.; Farahani, K.; Davatzikos, C. Advancing the cancer genome atlas glioma MRI collections with expert segmentation labels and radiomic features. Sci. Data 2017, 4, 170117. [Google Scholar] [CrossRef] [Green Version]
- Song, Y.; Zhang, J.; Zhang, Y.-D.; Hou, Y.; Yan, X.; Wang, Y.; Zhou, M.; Yao, Y.-F.; Yang, G. FeAture Explorer (FAE): A tool for developing and comparing radiomics models. PLoS ONE 2020, 15, e0237587. [Google Scholar] [CrossRef]
- Yogananda, C.G.B.; Shah, B.R.; Vejdani-Jahromi, M.; Nalawade, S.; Murugesan, G.K.; Yu, F.F.; Pinho, M.C.; Wagner, B.C.; Mickey, B.; Patel, T.R.; et al. A novel fully automated MRI-based deep-learning method for classification of IDH mutation status in brain gliomas. Neuro Oncol. 2020, 22, 402–411. [Google Scholar] [CrossRef]
- Chang, K.; Bai, H.X.; Zhou, H.; Su, C.; Bi, W.L.; Agbodza, E.; Kavouridis, V.K.; Senders, J.T.; Boaro, A.; Beers, A.; et al. Residual Convolutional Neural Network for the Determination of IDH Status in Low- and High-Grade Gliomas from MR Imaging. Clin. Cancer Res. 2018, 24, 1073–1081. [Google Scholar] [CrossRef] [Green Version]
- Broen, M.P.G.; Smits, M.; Wijnenga, M.M.J.; Dubbink, H.J.; Anten, M.H.M.E.; Schijns, O.E.M.G.; Beckervordersandforth, J.; Postma, A.A.; Bent, M.V.D. The T2-FLAIR mismatch sign as an imaging marker for nonenhancing IDH-mutant, 1p/19q-intact low-grade glioma: A validation study. Neuro Oncol. 2018, 20, 1393–1399. [Google Scholar] [CrossRef]
- Patel, S.H.; Poisson, L.M.; Brat, D.J.; Zhou, Y.; Cooper, L.; Snuderl, M.; Thomas, C.; Franceschi, A.M.; Griffith, B.; Flanders, A.E.; et al. T2-FLAIR Mismatch, an Imaging Biomarker for IDH and 1p/19q Status in Low-grade Gliomas: A TCGA/TCIA Project. Clin. Cancer Res. 2017, 23, 6078–6085. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.I.; Suh, C.H.; Guenette, J.P.; Huang, R.Y.; Kim, H.S. The T2-FLAIR mismatch sign as a predictor of IDH-mutant,1p/19q-noncodeleted lower-grade gliomas: A systematic review and diagnostic meta-analysis. Eur. Radiol. 2021, 31, 5289–5299. [Google Scholar] [CrossRef] [PubMed]
- Shofty, B.; Artzi, M.; Ben Bashat, D.; Liberman, G.; Haim, O.; Kashanian, A.; Bokstein, F.; Blumenthal, D.T.; Ram, Z.; Shahar, T. MRI radiomic analysis of molecular alterations in low-grade gliomas. Int. J. Comput. Assist. Radiol. Surg. 2018, 13, 563–571. [Google Scholar] [CrossRef]
- D’Alessio, A.; Proietti, G.; Sica, G.; Scicchitano, B.M. Pathological and Molecular Features of Glioblastoma and Its Peritumoral Tissue. Cancers 2019, 11, 469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, M.; Scott, J.; Chaudhury, B.; Hall, L.; Goldgof, D.; Yeom, K.; Iv, M.; Ou, Y.; Kalpathy-Cramer, J.; Napel, S.; et al. Radiomics in Brain Tumor: Image Assessment, Quantitative Feature Descriptors, and Machine-Learning Approaches. Am. J. Neuroradiol. 2018, 39, 208–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jakola, A.S.; Zhang, Y.-H.; Skjulsvik, A.J.; Solheim, O.; Bø, H.K.; Berntsen, E.M.; Reinertsen, I.; Gulati, S.; Förander, P.; Brismar, T.B. Quantitative texture analysis in the prediction of IDH status in low-grade gliomas. Clin. Neurol. Neurosurg. 2018, 164, 114–120. [Google Scholar] [CrossRef]
- Ma, M.; Gan, L.; Liu, Y.; Jiang, Y.; Xin, L.; Liu, Y.; Qin, N.; Cheng, Y.; Liu, Q.; Xu, L.; et al. radiomic features based on automatic segmented MRI images: Prognostic biomarkers for triple-negative breast cancer treated with neoadjuvant chemotherapy. Eur. J. Radiol. 2022, 146, 110095. [Google Scholar] [CrossRef]
- Ma, M.; Gan, L.; Jiang, Y.; Qin, N.; Li, C.; Zhang, Y.; Wang, X. Radiomics Analysis Based on Automatic Image Segmentation of DCE-MRI for Predicting Triple-Negative and Nontriple-Negative Breast Cancer. Comput. Math. Methods Med. 2021, 2021, 1–7. [Google Scholar] [CrossRef]
- Chen, C.; Qin, Y.; Cheng, J.; Gao, F.; Zhou, X. Texture Analysis of Fat-Suppressed T2-Weighted Magnetic Resonance Imaging and Use of Machine Learning to Discriminate Nasal and Paranasal Sinus Small Round Malignant Cell Tumors. Front. Oncol. 2021, 11, 701289. [Google Scholar] [CrossRef]
- Chen, C.; Qin, Y.; Chen, H.; Cheng, J.; He, B.; Wan, Y.; Zhu, D.; Gao, F.; Zhou, X. Machine learning to differentiate small round cell malignant tumors and non-small round cell malignant tumors of the nasal and paranasal sinuses using apparent diffusion coefficient values. Eur. Radiol. 2022, 2, 3819–3829. [Google Scholar] [CrossRef]
- Jin, Z.; Chen, L.; Zhong, B.; Zhou, H.; Zhu, H.; Zhou, H.; Song, J.; Guo, J.; Zhu, X.; Ji, J.; et al. Machine-learning analysis of contrast-enhanced computed tomography radiomic predicts patients with hepatocellular carcinoma who are unsuitable for initial transarterial chemoembolization monotherapy: A multicenter study. Transl. Oncol. 2021, 14, 101034. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| The Main Radiomics Pipeline | Options |
|---|---|
| Medical images | T1, T2, FLAIR, T1Gd |
| Combined Multi-sequence MRI | T1, T2, FLAIR, T1Gd, T1+T2, T1+FLAIR, T1+T1Gd, T2+FLAIR, T2+T1Gd, T1Gd+FLAIR, T1+T2+FLAIR, T1+T1Gd+FLAIR, T1+T2+T1Gd, T2+FLAIR+T1Gd, T1+T2+T1Gd+FLAIR. |
| Images filters | Original/wavelet Transformation/None |
| Data Balance | Upsampling/Downsampling/None |
| Normalization | Z- Score/Mean/MinMax/None |
| Dimension Reduction | PCA/PCC/None |
| Feature Selection | ANOVA/KW/RFE/Relief |
| Classifier | SVM/AE/LD/RF/LR/LR-Lasso/DT |
| Characteristic | Total | Train Cohort | Test Cohort | p-Value |
|---|---|---|---|---|
| Number (%) | 99 (100) | 80 (80.8) | 19 (19.2) | |
| Age | 45.41 ± 13.69 | 44.88 ± 13.88 | 47.68 ± 12.98 | 0.62 |
| Gender Female Male | 53 46 | 39 41 | 14 5 | 0.13 |
| IDH status Wildtype Mutation | 27 72 | 22 58 | 5 14 | 0.92 |
| Histological type Astrocytomas Oligodendrogliomas NEC | 57 14 28 | 46 11 23 | 11 3 5 | 0.962 |
| 1p/19q codeletion status No Yes | 84 15 | 68 12 | 16 3 | 0.089 |
| Combined Multi-Sequence MRI | Test | Acc | Sen | Spe | Optimal Pipeline |
|---|---|---|---|---|---|
| T1 | 0.778 ± 0.09 | 0.699 ± 0.15 | 0.729 ± 0.15 | 0.720 ± 0.19 | Wavelet_MinMax_PCC_RFE_15_RF |
| T2 | 0.842 ± 0.05 | 0.779 ± 0.08 | 0.780 ± 0.13 | 0.780 ± 0.19 | Wavelet_Mean_PCC_RFE_10_LDA |
| FLAIR | 0.800 ± 0.08 | 0.742 ± 0.09 | 0.736 ± 0.11 | 0.730 ± 0.25 | Wavelet_MinMax_Pcc_RFE_15_RF |
| T1Gd | 0.764 ± 0.04 | 0.679 ± 0.09 | 0.686 ± 0.16 | 0.66 ± 0.16 | Wavelet_Mean_PCA_RFE_15_LRLasso |
| T1+T2 | 0.696 ± 0.12 | 0.663 ± 0.09 | 0.714 ± 0.16 | 0.520 ± 0.22 | Wavelet_Mean_PCC_RFE_14_LDA |
| T1Gd+FLAIR | 0.647 ± 0.12 | 0.658 ± 0.09 | 0.722 ± 0.11 | 0.480 ± 0.20 | Wavelet_Mean_PCC_RFE_10_LR |
| T1+FLAIR | 0.858 ± 0.08 | 0.737 ± 0.08 | 0.686 ± 0.12 | 0.88 ± 0.16 | Wavelet_Mean_PCC_KW_13_AE |
| T1+T1Gd | 0.713 ± 0.09 | 0.637 ± 0.08 | 0.636 ± 0.07 | 0.640 ± 0.17 | Wavelet_MinMax_PCC_Relief_15_LDA |
| T1Gd+T2 | 0.825 ± 0.09 | 0.737 ± 0.07 | 0.786 ± 0.12 | 0.600 ± 0.24 | Wavelet_Zscore_PCC_RFE_14_SVM |
| T2+FLAIR | 0.873 ± 0.05 | 0.876 ± 0.09 | 0.875 ± 0.11 | 0.877 ± 0.15 | Wavelet_Mean_PCC_RFE_14_SVM |
| T1+FLAIR+T1Gd | 0.807 ± 0.07 | 0.763 ± 0.08 | 0.786 ± 0.12 | 0.700 ± 0.18 | Wavelet_Mean_PCA_RFE_12_AE |
| T1+T2+FLAIR | 0.738 ± 0.14 | 0.711 ± 0.11 | 0.714 ± 0.12 | 0.700 ± 0.18 | Wavelet_MinMax_PCC_Relief_3_RF |
| T2+FLAIR+T1Gd | 0.624 ± 0.16 | 0.663 ± 0.13 | 0.729 ± 0.17 | 0.480 ± 0.27 | Wavelet_Mean_PCC_RFE_10_LR |
| T1+T2+T1Gd | 0.816 ± 0.11 | 0.747 ± 0.08 | 0.743 ± 0.10 | 0.760 ± 0.20 | Wavelet_Zscore_PCA_RFE_10_SVM |
| T1+T2+T1Gd+FLAIR | 0.811 ± 0.07 | 0.763 ± 0.09 | 0.771 ± 0.10 | 0.740 ± 0.16 | Wavelet_Mean_PCC_ANOVA_10_RF |
| Statistics | Value |
|---|---|
| Accuracy | 0.9357 |
| AUC | 0.957 |
| AUC 95% CIs | [0.926–1.000] |
| NPV | 0.8148 |
| PPV | 1.0000 |
| Sensitivity | 0.9138 |
| Specificity | 1.0000 |
| Features | Rank | Description |
|---|---|---|
| FLAIR_wavelet-HLL_glrlm_GrayLevelNonUniformity | 1 | Flair wavelet texture gray region size matrix characteristic gray nonuniformity |
| T2_wavelet-LLH_firstorder_Skewness | 2 | T2 wavelet first order characteristic skewness |
| T2_wavelet-HLL_glcm_Correlation | 3 | T2 wavelet characteristic correlation of texture gray level co-occurrence matrix |
| T2_wavelet-LHL_firstorder_Range | 4 | T2 wavelet texture first-order feature deviation |
| T2_wavelet-LHL_firstorder_Minimum | 5 | T2 wavelet texture first-order feature minimum |
| T2_wavelet-LHL_glcm_Correlation | 6 | Feature correlation of T2 wavelet texture gray level co-occurrence matrix |
| T2_wavelet-HLH_glcm_Correlation | 7 | Feature correlation of T2 wavelet texture gray level co-occurrence matrix |
| T2_wavelet-LHH_firstorder _Mean | 8 | T2 wavelet texture first-order feature mean |
| FLAIR_wavelet-HLL_glcm_JointEnergy | 9 | Joint energy of flair wavelet texture gray level co-occurrence matrix features |
| T2_wavelet-HLH_glszm_SizeZoneNonUniformityNormalized | 10 | T2 wavelet texture gray region size matrix feature normalized region size nonuniformity |
| FLAIR_wavelet-LLH_gldm_SmallDependence-LowGrayLevelEmphasis | 11 | Flair wavelet texture gray correlation matrix small dependence low gray emphasis |
| T2_wavelet-LLH_glcm_ InverseVariance | 12 | T2 wavelet texture gray level co-occurrence matrix characteristic deficit square |
| FLAIR_wavelet-HLH_glcm_InverseVariance | 13 | Characteristic deficit square of gray level co-occurrence matrix of flair wavelet texture |
| T2_wavelet-HLH_glszm_SmallAreaEmphasis | 14 | T2 wavelet texture gray area size matrix feature small area emphasis |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
He, A.; Wang, P.; Zhu, A.; Liu, Y.; Chen, J.; Liu, L. Predicting IDH Mutation Status in Low-Grade Gliomas Based on Optimal Radiomic Features Combined with Multi-Sequence Magnetic Resonance Imaging. Diagnostics 2022, 12, 2995. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12122995
He A, Wang P, Zhu A, Liu Y, Chen J, Liu L. Predicting IDH Mutation Status in Low-Grade Gliomas Based on Optimal Radiomic Features Combined with Multi-Sequence Magnetic Resonance Imaging. Diagnostics. 2022; 12(12):2995. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12122995
Chicago/Turabian StyleHe, Ailing, Peng Wang, Aihua Zhu, Yankui Liu, Jianhuan Chen, and Li Liu. 2022. "Predicting IDH Mutation Status in Low-Grade Gliomas Based on Optimal Radiomic Features Combined with Multi-Sequence Magnetic Resonance Imaging" Diagnostics 12, no. 12: 2995. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12122995