
Potential Value of Visfatin, Omentin-1, Nesfatin-1 and Apelin in Renal Cell Carcinoma (RCC): A Systematic Review and Meta-Analysis
 , and
, and
Abstract
:1. Background
2. Method
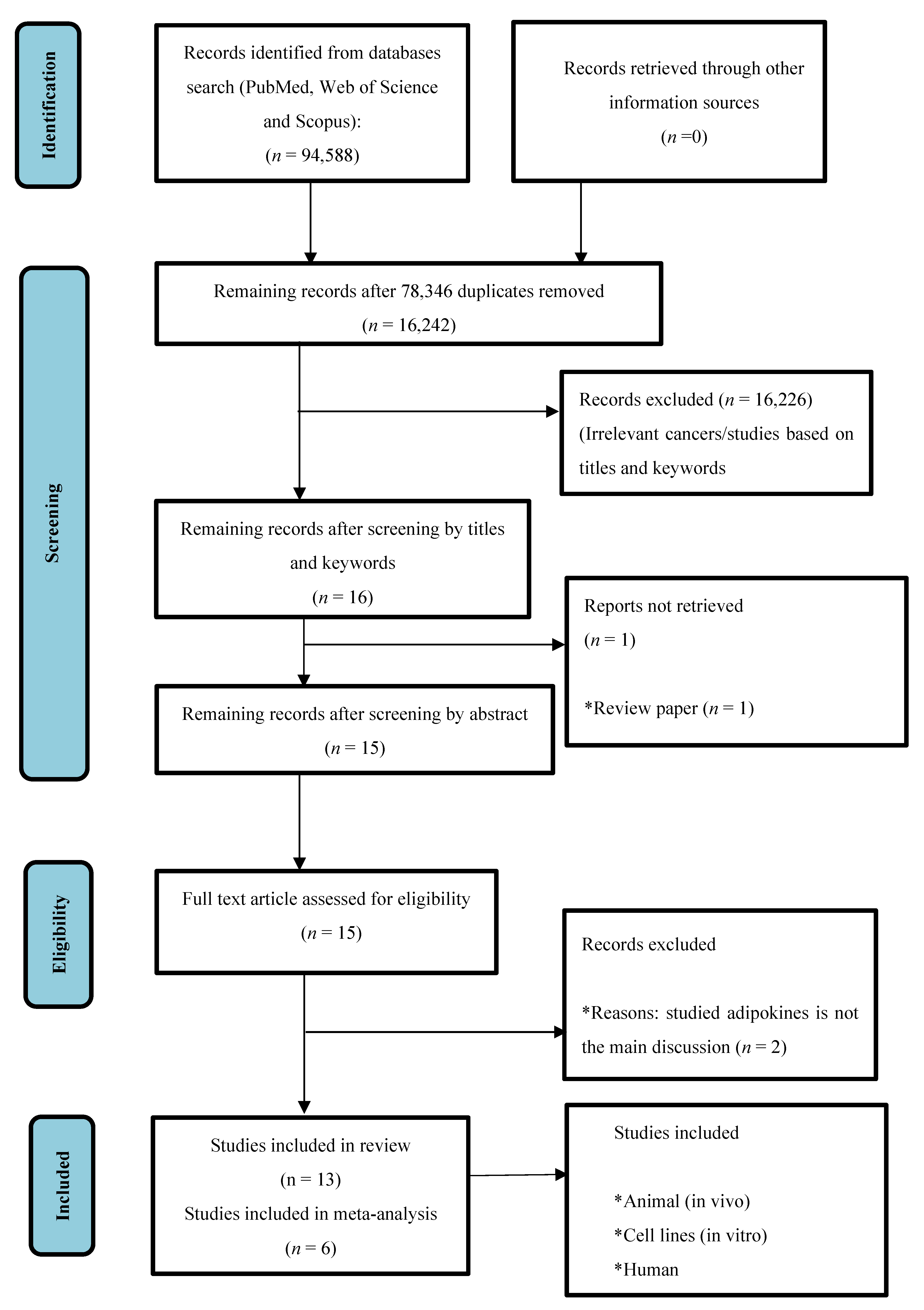
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Extraction of Data for Hypothesis Evaluation
2.4. Assessment of Study Quality
2.5. Data Analysis
3. Results
3.1. Study Selection and Study Characteristics
3.2. Quality of Studies
3.3. Summary of Systematic Review Findings
3.3.1. Visfatin
3.3.2. Omentin-1
3.3.3. Nesfatin-1
3.3.4. Apelin
3.4. Meta-Analysis Outcomes
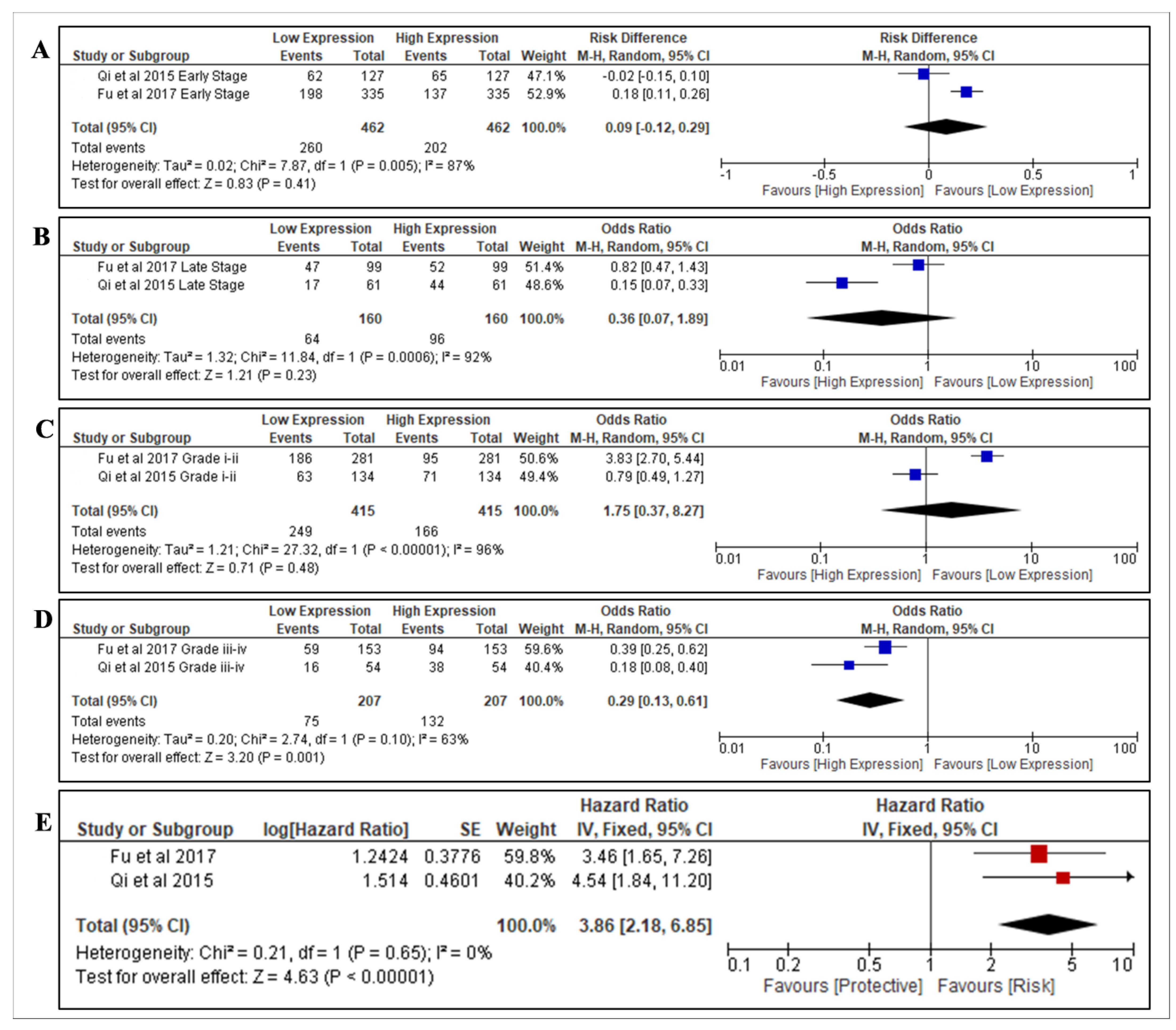
3.4.1. Nesfatin-1
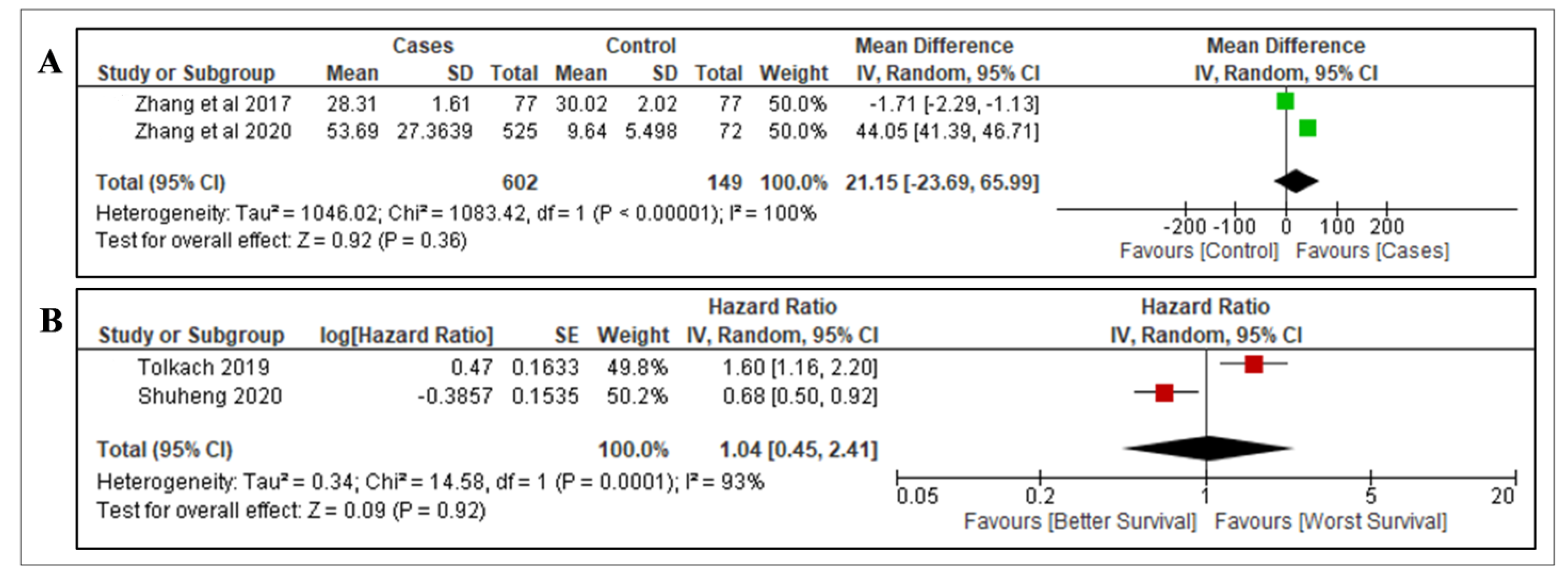
3.4.2. Apelin
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hsieh, J.J.; Purdue, M.P.; Signoretti, S.; Swanton, C.; Albiges, L.; Schmidinger, M.; Heng, D.Y.; Larkin, J.; Ficarra, V. Renal cell carcinoma. Nat. Rev. Dis. Prim. 2017, 3, 17009. [Google Scholar]
- Muglia, V.F.; Prando, A. Renal cell carcinoma: Histological classification and correlation with imaging findings. Radiol. Bras. 2015, 48, 166–174. [Google Scholar] [CrossRef]
- Susman, E. Smoking and Renal Cancer a Fatal Combination. Oncol. Times 2016, 38, 24. [Google Scholar] [CrossRef]
- Antwi, S.O.; Eckel-Passow, J.E.; Diehl, N.D.; Serie, D.J.; Custer, K.M.; Wu, K.J.; Cheville, J.C.; Thiel, D.D.; Leibovich, B.C.; Parker, A.S. Alcohol consumption, variability in alcohol dehydrogenase genes and risk of renal cell carcinoma. Int. J. Cancer 2018, 142, 747–756. [Google Scholar] [CrossRef]
- Gati, A.; Kouidhi, S.; Marrakchi, R.; El Gaaied, A.; Kourda, N.; Derouiche, A.; Chebil, M.; Caignard, A.; Perier, A. Obesity and renal cancer: Role of adipokines in the tumor-immune system conflict. Oncoimmunology 2014, 3, e27810. [Google Scholar] [CrossRef]
- Kim, C.S.; Han, K.-D.; Choi, H.S.; Bae, E.H.; Ma, S.K.; Kim, S.W. Association of Hypertension and Blood Pressure with Kidney Cancer Risk. Hypertension 2020, 75, 1439–1446. [Google Scholar] [CrossRef]
- Schouten, L.J.; van de Pol, J.; Kviatkovsky, M.J.; van den Brandt, P.A. Reproductive and external hormonal factors and the risk of renal cell cancer in the Netherlands Cohort Study. Cancer Epidemiol. 2022, 79, 102171. [Google Scholar] [CrossRef]
- Liss, M.; Natarajan, L.; Hasan, A.; Noguchi, J.L.; White, M.; Parsons, J.K. Physical Activity Decreases Kidney Cancer Mortality. Curr. Urol. 2017, 10, 193–198. [Google Scholar] [CrossRef]
- Graff, R.E.; Cho, E.; Preston, M.A.; Sanchez, A.; Mucci, L.A.; Wilson, K.M. Dietary Acrylamide Intake and Risk of Renal Cell Carcinoma in Two Large Prospective Cohorts. Cancer Epidemiol. Biomark Prev. 2018, 27, 979–982. [Google Scholar] [CrossRef]
- Mariusdottir, E.; Ingimarsson, J.P.; Jonsson, E.; Einarsson, G.V.; Aspelund, T.; Gudnason, V.; Gudbjartsson, T. Occupation as a risk factor for renal cell cancer: A nationwide, prospective epidemiological study. Scand. J. Urol. 2016, 50, 181–185. [Google Scholar] [CrossRef]
- Navai, N.; Wood, C.G. Environmental and modifiable risk factors in renal cell carcinoma. Urol. Oncol. 2012, 30, 220–224. [Google Scholar] [CrossRef]
- Maher, E.R. Hereditary renal cell carcinoma syndromes: Diagnosis, surveillance and management. World J. Urol. 2018, 36, 1891–1898. [Google Scholar] [CrossRef]
- Liao, L.M.; Weinstein, S.J.; Pollak, M.; Li, Z.; Virtamo, J.; Albanes, D.; Chow, W.H.; Purdue, M.P. Prediagnostic circulating adipokine concentrations and risk of renal cell carcinoma in male smokers. Carcinogenesis 2013, 34, 109–112. [Google Scholar] [CrossRef]
- Dalamaga, M.; Diakopoulos, K.N.; Mantzoros, C.S. The role of adiponectin in cancer: A review of current evidence. Endocr. Rev. 2012, 33, 547–594. [Google Scholar] [CrossRef]
- Rajandram, R.; Perumal, K.; Yap, N.Y. Prognostic biomarkers in renal cell carcinoma: Is there a relationship with obesity? Transl. Androl. Urol. 2018, 8 (Suppl. S2), S138–S146. [Google Scholar] [CrossRef]
- Boot, A.; Magnuson, A.; Fouts, J.; Foster, M. Adipose tissue, obesity and adipokines: Role in cancer promotion. Horm. Mol. Biol. Clin. Investig. 2015, 21, 57–74. [Google Scholar] [CrossRef]
- Zhu, H.; Li, W.; Mao, S.; Wang, L. Association between leptin level and renal cell carcinoma susceptibility and progression: A meta-analysis. J. Cancer Res. Ther. 2018, 14, 873–880. [Google Scholar]
- Fang, J.; Xu, X.; Mao, Q.; Ying, Y.; Zhang, X.; Xie, L. Lower circulating adiponectin is associated with higher risk of renal cell carcinoma: A meta-analysis. Int. J. Biol. Markers. 2020, 35, 57–64. [Google Scholar] [CrossRef]
- Ito, R.; Narita, S.; Huang, M.; Nara, T.; Numakura, K.; Takayama, K.; Tsuruta, H.; Maeno, A.; Saito, M.; Inoue, T.; et al. The impact of obesity and adiponectin signaling in patients with renal cell carcinoma: A potential mechanism for the “obesity paradox”. PLoS ONE 2017, 12, e0171615. [Google Scholar] [CrossRef]
- Fan, W.L.; Yeh, Y.M.; Liu, T.T.; Lin, W.M.; Yang, T.Y.; Lee, C.W.; Lin, T.C. Leptin Is Associated with Poor Clinical Outcomes and Promotes Clear Cell Renal Cell Carcinoma Progression. Biomolecules 2021, 11, 431. [Google Scholar] [CrossRef]
- Perumal, K.; Mun, K.S.; Yap, N.Y.; Razack, A.H.A.; Gobe, G.C.; Ong, T.A.; Kuppusamy, S.; Rajandram, R. A Study on the Immunohistochemical Expressions of Leptin and Leptin Receptor in Clear Cell Renal Cell Carcinoma. BioMed Res. Int. 2020, 2020, 3682086. [Google Scholar] [CrossRef]
- Pu, X.; Chen, D. Targeting Adipokines in Obesity-Related Tumors. Front. Oncol. 2021, 11, 3099. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef]
- Altman, D.G.; McShane, L.M.; Sauerbrei, W.; Taube, S.E. Reporting Recommendations for Tumor Marker Prognostic Studies (REMARK): Explanation and elaboration. BMC Med. 2012, 10, 1–39. [Google Scholar] [CrossRef]
- Percie du Sert, N.; Hurst, V.; Ahluwalia, A.; Alam, S.; Avey, M.T.; Baker, M.; Browne, W.J.; Clark, A.; Cuthill, I.C.; Dirnagl, U.; et al. The ARRIVE guidelines 2.0: Updated guidelines for reporting animal research. J. Cereb. Blood Flow Metab. 2020, 40, 1769–1777. [Google Scholar] [CrossRef]
- Zhang, H.P.; Zou, J.; Xu, Z.Q.; Ruan, J.; Yang, S.D.; Yin, Y.; Mu, H.J. Association of leptin, visfatin, apelin, resistin and adiponectin with clear cell renal cell carcinoma. Oncol. Lett. 2017, 13, 463–468. [Google Scholar] [CrossRef]
- Yamada, Y.; Arai, T.; Sugawara, S.; Okato, A.; Kato, M.; Kojima, S.; Yamazaki, K.; Naya, Y.; Ichikawa, T.; Seki, N. Impact of novel oncogenic pathways regulated by antitumor miR-451a in renal cell carcinoma. Cancer Sci. 2018, 109, 1239–1253. [Google Scholar] [CrossRef]
- Choi, S.H.; Chun, S.Y.; Kim, T.H.; Kwon, T.G. Identifying the emerging role of adipokine as a diagnostic and prognostic biomarker of renal cell carcinoma. Urol. Oncol. 2016, 34, e15–e259. [Google Scholar] [CrossRef]
- Shackelford, R.E.; Abdulsattar, J.; Wei, E.X.; Cotelingam, J.; Coppola, D.; Herrera, G.A. Increased Nicotinamide Phosphoribosyltransferase and Cystathionine-β-Synthase in Renal Oncocytomas, Renal Urothelial Carcinoma, and Renal Clear Cell Carcinoma. Anticancer Res. 2017, 37, 3423–3427. [Google Scholar]
- Shen, X.; Zhang, L. Circulating levels of adipocytokine omentin-1 in patients with renal cell cancer. Transl. Androl. Urol. 2016, 5 (Suppl. S1), AB154. [Google Scholar] [CrossRef]
- Fu, H.; Zhu, Y.; Wang, Y.; Liu, Z.; Zhang, J.; Wang, Z.; Xie, H.; Dai, B.; Xu, J.; Ye, D. High NUCB2 expression level represents an independent negative prognostic factor in Chinese cohorts of non-metastatic clear cell renal cell carcinoma patients. Oncotarget 2017, 8, 35244–35254. [Google Scholar] [CrossRef] [PubMed]
- Qi, C.; Ma, H.; Zhang, H.T.; Gao, J.D.; Xu, Y. Nucleobindin 2 expression is an independent prognostic factor for clear cell renal cell carcinoma. Histopathology 2015, 66, 650–657. [Google Scholar] [CrossRef] [PubMed]
- Xin, R.; Qu, D.; Xu, H.; Chen, D. Correction: Circ_001504 promotes the development of renal cell carcinoma by sponging microRNA-149 to increase NUCB2. Cancer Gene Ther. 2022, 29, 1074. [Google Scholar] [CrossRef] [PubMed]
- Tao, R.; Niu, W.B.; Dou, P.H.; Ni, S.B.; Yu, Y.P.; Cai, L.C.; Wang, X.Y.; Li, S.Y.; Zhang, C.; Luo, Z.G. Nucleobindin-2 enhances the epithelial-mesenchymal transition in renal cell carcinoma. Oncol. Lett. 2020, 19, 3653–3664. [Google Scholar] [CrossRef]
- Xu, H.; Li, W.; Qi, K.; Zhou, J.; Gu, M.; Wang, Z. A novel function of NUCB2 in promoting the development and invasion of renal cell carcinoma. Oncol. Lett. 2018, 15, 2425–2430. [Google Scholar] [CrossRef] [PubMed]
- Tolkach, Y.; Ellinger, J.; Kremer, A.; Esser, L.; Müller, S.C.; Stephan, C.; Jung, K.; Toma, M.; Kristiansen, G.; Hauser, S. Apelin and apelin receptor expression in renal cell carcinoma. Br. J. Cancer 2019, 120, 633–639. [Google Scholar] [CrossRef]
- Bai, S.; Wu, Y.; Yan, Y.; Shao, S.; Zhang, J.; Liu, J.; Hui, B.; Liu, R.; Ma, H.; Zhang, X.; et al. Construct a circRNA/miRNA/mRNA regulatory network to explore potential pathogenesis and therapy options of clear cell renal cell carcinoma. Sci. Rep. 2020, 10, 13659. [Google Scholar] [CrossRef]
- Zhang, N.; Chen, W.; Gan, Z.; Abudurexiti, A.; Hu, X.; Sang, W. Identification of biomarkers of clear cell renal cell carcinoma by bioinformatics analysis. Medicine 2020, 99, e20470. [Google Scholar] [CrossRef]
- Taylor, E.B. The complex role of adipokines in obesity, inflammation, and autoimmunity. Clin. Sci. 2021, 135, 731–752. [Google Scholar] [CrossRef]
- Gluba-Brzózka, A.; Rysz, J.; Ławiński, J.; Franczyk, B. Renal Cell Cancer and Obesity. Int. J. Mol. Sci. 2022, 23, 3404. [Google Scholar] [CrossRef] [PubMed]
- Lin, T.C. The role of visfatin in cancer proliferation, angiogenesis, metastasis, drug resistance and clinical prognosis. Cancer Manag. Res. 2019, 11, 3481–3491. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.Y.; Chen, H.D.; Lo, S.; Chen, Y.K.; Huang, Y.C.; Hu, S.C.; Hsieh, Y.C.; Hung, A.C.; Hou, M.F.; Yuan, S.S.F. Visfatin Enhances Breast Cancer Progression through CXCL1 Induction in Tumor-Associated Macrophages. Cancers 2020, 12, 3526. [Google Scholar] [CrossRef] [PubMed]
- Christodoulatos, G.S.; Antonakos, G.; Karampela, I.; Psallida, S.; Stratigou, T.; Vallianou, N.; Lekka, A.; Marinou, I.; Vogiatzakis, E.; Kokoris, S.; et al. Circulating Omentin-1 as a Biomarker at the Intersection of Postmenopausal Breast Cancer Occurrence and Cardiometabolic Risk: An Observational Cross-Sectional Study. Biomolecules 2021, 11, 1609. [Google Scholar] [CrossRef]
- Panagiotou, G.; Triantafyllidou, S.; Tarlatzis, B.C.; Papakonstantinou, E. Serum Levels of Irisin and Omentin-1 in Breast Neoplasms and Their Association with Tumor Histology. Int. J. Endocrinol. 2021, 2021, 6656671. [Google Scholar] [CrossRef]
- Zhang, Y.Y.; Zhou, L.M. Omentin-1, a new adipokine, promotes apoptosis through regulating Sirt1-dependent p53 deacetylation in hepatocellular carcinoma cells. Eur. J. Pharmacol. 2013, 698, 137–144. [Google Scholar] [CrossRef]
- Fryczkowski, M.; Bułdak, R.J.; Hejmo, T.; Kukla, M.; Żwirska-Korczala, K. Circulating Levels of Omentin, Leptin, VEGF, and HGF and Their Clinical Relevance with PSA Marker in Prostate Cancer. Dis. Markers 2018, 2018, 3852401. [Google Scholar] [CrossRef]
- Aleksandrova, K.; di Giuseppe, R.; Isermann, B.; Biemann, R.; Schulze, M.; Wittenbecher, C.; Fritsche, A.; Lehmann, R.; Menzel, J.; Weikert, C.; et al. Circulating Omentin as a Novel Biomarker for Colorectal Cancer Risk: Data from the EPIC-Potsdam Cohort Study. Cancer Res. 2016, 76, 3862–3871. [Google Scholar] [CrossRef]
- Stengel, A.; Mori, M.; Taché, Y. The role of nesfatin-1 in the regulation of food intake and body weight: Recent developments and future endeavors. Obes. Rev. 2013, 14, 859–870. [Google Scholar] [CrossRef]
- Liu, G.M.; Xu, Z.Q.; Ma, H.S. Nesfatin-1/Nucleobindin-2 Is a Potent Prognostic Marker and Enhances Cell Proliferation, Migration, and Invasion in Bladder Cancer. Dis. Markers 2018, 2018, 4272064. [Google Scholar] [CrossRef]
- Kim, J.; Yang, H. Nesfatin-1 as a new potent regulator in reproductive system. Dev. Reprod. 2012, 16, 253–264. [Google Scholar] [CrossRef] [PubMed]
- Wysocka, M.B.; Pietraszek-Gremplewicz, K.; Nowak, D. The Role of Apelin in Cardiovascular Diseases, Obesity and Cancer. Front. Physiol. 2018, 9, 557. [Google Scholar] [CrossRef] [PubMed]
- Lacquaniti, A.; Chirico, V.; Lupica, R.; Buemi, A.; Loddo, S.; Caccamo, C.; Salis, P.; Bertani, T.; Buemi, M. Apelin and copeptin: Two opposite biomarkers associated with kidney function decline and cyst growth in autosomal dominant polycystic kidney disease. Peptides 2013, 49, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Podgórska, M.; Pietraszek-Gremplewicz, K.; Nowak, D. Apelin Effects Migration and Invasion Abilities of Colon Cancer Cells. Cells 2018, 7, 113. [Google Scholar] [CrossRef] [PubMed]
- Lacquaniti, A.; Altavilla, G.; Picone, A.; Donato, V.; Chirico, V.; Mondello, P.; Aloisi, C.; Marabello, G.; Loddo, S.; Buemi, A.; et al. Apelin beyond kidney failure and hyponatremia: A useful biomarker for cancer disease progression evaluation. Clin. Exp. Med. 2015, 15, 97–105. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Reference | Author | Title | Country | Study Subject | Adipokine | Study Sample | Diagnostic Value/Prognostic Value (Stage/Grade)/Overall Survival (OS)/p Value | Studies Included in Meta-Analysis | Fixation Type | Antibody Used for Fixation | Scoring Procedure | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Serum/Plasma/Tissue/Cell Lines/Animal Model | Sample Size | |||||||||||
| [27] | Zhang et al. (2017) | Association of leptin, visfatin, apelin, resistin and adiponectin with clear cell renal cell carcinoma | China | Human | Visfatin | Tissue | 77 Controls 77 ccRCC | Control 25.24 ± 1.07 (77) Case 22.73 ± 0.88 (77) p < 0.01 | No | N/A | N/A | N/A |
| [28] | Yamada Y et al. (2018) | Impact of novel oncogenic pathways regulated by antitumor miR-451a in renal cell carcinoma | Japan | Human | Visfatin | Tissue | 261 RCC | p = 0.0138 | No | N/A | N/A | N/A |
| [29] | Choi SH et al. (2016) | Identifying the emerging role of adipokine as a diagnostic and prognostic biomarker of renal cell carcinoma | Korea | Human | Visfatin | Plasma | 25 Controls 54 ccRCC | Control 2.06 (1.52–2.68) (25) Case 2.26 (2.06–2.73) (54) p = 0.035 | No | N/A | N/A | N/A |
| [30] | Shackelford RE et al. (2017) | Increased Nicotinamide Phosphoribosyltransferase and Cystathionine-β-Synthase in Renal Oncocytomas, Renal Urothelial Carcinoma, and Renal Clear Cell Carcinoma | USA | Human | Visfatin | Tissue microarrays (ccRCC Fuhrman grades: grade I–IV) | 107 ccRCC | Not reported | No | Immunohistochemistry (IHC) | Mouse monoclonal antibody to human visfatin | The IHC score was the product of the percentage of cells stained multiplied by the intensity score, allowing for a maximal score of 9 and a minimal score of 0. |
| [31] | Shen X et al. (2016) | Circulating levels of adipocytokine omentin-1 in patients with renal cell cancer | China | Human | Omentin-1 | Serum | 42 Controls 41 RCC | Not reported | No | N/A | N/A | N/A |
| [32] | Fu H et al. (2017) | High NUCB2 expression level represents an independent negative prognostic factor in Chinese cohorts of non-metastatic clear cell renal cell carcinoma patients | China | Human | Nesfatin-1 | non-metastasis (pT1–3N0M0) clear cell renal cell carcinoma (ccRCC) | 434 ccRCC | Early stage (low expression = 198/335) 60.0% (high expression = 137/335) 40.0% Late stage (low expression = 47/99) 47.0% (high expression = 52/99) 53.0% p = 0.107 Early grade (low expression = 186/281) 66.0% (high expression = 95/281) 34.0% Late grade (low expression = 59/153) 39.0% (high expression = 94/153) 61.0% p ≤ 0.001 HR 3.464, 95% CI (1.859–6.454) p < 0.001 | Yes | Immunohistochemistry (IHC) | Rabbit anti-NUCB2 polyclonal antibody | A semi-quantitative H-score was computed for each sample by multiplying the staining intensities (0: negative, 1: weak staining, 2: moderate staining, 3: strong staining) and distribution areas (0–100%), which ranged from 0 to 300. |
| [33] | Qi C et al. (2015) | Nucleobindin 2 expression is an independent prognostic factor for clear cell renal cell carcinoma | China | Human | Nesfatin-1 | ccRCC tumours from patients | 188 ccRCC | Early stage (low expression = 62/127) 48.8% (high expression = 65/127) 51.2% Late stage (low expression = 17/61) 27.9% (high expression = 44/61) 72.1% p = 0.006 Early grade (low expression = 63/134) 47.0% (high expression = 71/134) 53.0% Late grade (low expression = 16/54) 29.6% (high expression = 38/54) 70.4% p = 0.029 HR 4.545, 95% CI (2.122–9.733) p < 0.001 | Yes | Immunohistochemistry (IHC) | Rabbit anti-NUCB2 polyclonal antibody | The score was the sum of the intensity and area scores, and on this basis staining was considered negative if the final score was 0–2 and positive if it was 3–4. |
| [34] | Xin R et al. (2022) | circ_001504 promotes the development of renal cell carcinoma by sponging microRNA-149 to increase NUCB2 | China | Human | Nesfatin-1 | Tissue | 72 ccRCC | Not reported | No | N/A | N/A | N/A |
| [35] | Tao R et al. (2020) | Nucleobindin-2 enhances the epithelial-mesenchymal transition in renal cell carcinoma | China | In vitro, in vivo | Nesfatin-1 | SK-RC-52 Renca cell BALB/c mice | n/a | Not reported | No | N/A | N/A | N/A |
| [36] | Xu H et al. (2018) | A novel function of NUCB2 in promoting the development and invasion of renal cell carcinoma | China | In vitro | Nesfatin-1 | 786-O ACHN HEK-293 | n/a | Not reported | No | N/A | N/A | N/A |
| [37] | Tolkach Y et al. (2019) | Apelin and apelin receptor expression in renal cell carcinoma | Germany | Human | Apelin | Tissue | 481 ccRCC | HR 1.6, 95% CI 1.2–2.2, p = 0.004 | Yes | N/A | N/A | N/A |
| [38] | Bai S et al. (2020) | Construct a circRNA/miRNA/mRNA regulatory network to explore potential pathogenesis and therapy options of clear cell renal cell carcinoma | China | Human | Apelin | Tissue | 258 ccRCC | HR 0.68, p = 0.012 | Yes | N/A | N/A | N/A |
| [39] | Zhang N et al. (2020) | Identification of biomarkers of clear cell renal cell carcinoma by bioinformatics analysis | China | Human | Apelin | Tissue | 72 Controls 525 ccRCC | Controls 9.64 ± 5.498 (72) transcript per million Cases 53.69 ± 27.36 (525) transcript per million | Yes | N/A | N/A | N/A |
| [27] | Zhang HP et al. (2017) | Association of leptin, visfatin, apelin, resistin and adiponectin with clear cell renal cell carcinoma | China | Human | Apelin | Tissue | 77 Controls 77 ccRCC | Control 30.02 ± 2.02 (77) Case 28.31 ± 1.61 (77) | Yes | N/A | N/A | N/A |
| Reference | Author | Country | Title | Sample Type | No of Participant | Outcome |
|---|---|---|---|---|---|---|
| Visfatin | ||||||
| [28] | Yamada Y et al. (2018) | Japan | Impact of novel oncogenic pathways regulated by antitumor miR-451a in renal cell carcinoma | Tissue | 261 RCC | High expression of visfatin was significantly associated with poor prognosis. |
| [29] | Choi SH et al. (2016) | Korea | Identifying the emerging role of adipokine as a diagnostic and prognostic biomarker of renal cell carcinoma | Plasma | 54 ccRCC 25 Controls | Visfatin levels were higher in RCC patients (2.26 (2.06–2.73) than in normal healthy controls (2.06 (1.52–2.68), p = 0.035, and significantly associated with RCC severity (T stage). Expressed as the median (interquartile range). |
| [30] | Shackelford RE et al. (2017) | USA | Increased Nicotinamide Phosphoribosyltransferase and Cystathionine-β-Synthase in Renal Oncocytomas, Renal Urothelial Carcinoma, and Renal Clear Cell Carcinoma | Tissue | 94 ccRCC | Visfatin protein levels increase in RCC at higher Fuhrman grades. RCC Fuhrman I (n = 44) 3.27 ± 0.13 RCC Fuhrman II (n = 28) 5.18 ± 0.32 RCC Fuhrman III (n = 13) 6.54 ± 0.54 RCC Fuhrman IV (n = 9) 8.67 ± 0.71 Expressed as mean ± standard error of measurement. |
| [27] | Zhang et al. (2017) | China | Association of leptin, visfatin, apelin, resistin and adiponectin with clear cell renal cell carcinoma | Tissue | 77 Controls 77 ccRCC | Visfatin gene expression was upregulated in the ccRCC (22.73 ± 0.88) compared to adjacent normal tissue (25.24 ± 1.07), p < 0.01. |
| Omentin-1 | ||||||
| [31] | Shen X et al. (2016) | China | Circulating levels of adipocytokine omentin-1 in patients with renal cell cancer | Serum | 41 RCC 42 Controls | The omentin-1 levels in healthy controls (9.86 ± 1.44) were higher compared to RCC patients (3.62 ± 0.76). Expressed in terms of ± standard error of measurement. |
| Reference | Author | Country | Title | No of Studies | Study Test | Outcome |
|---|---|---|---|---|---|---|
| In vivo | ||||||
| [35] | Tao R et al. (2020) | China | Nucleobindin-2 enhances the epithelial-mesenchymal transition in renal cell carcinoma | 10 control mice 10 knockdown mice | Transfection RT-PCR | Transfection with shRNA significantly decreased nesfatin-1 mRNA and protein levels and the growth of tumours in the nesfatin-1 KD group was significantly slower compared with the control group, indicating nesfatin-1 has a role in the growth of RCC. |
| In vitro | ||||||
| [35] | Tao R et al. (2020) | China | Nucleobindin-2 enhances the epithelial-mesenchymal transition in renal cell carcinoma | - | Knockout RT-PCR Western blotting | Nesfatin-1 knockout in the RCC cell line inhibited cell migration, proliferation and invasion. Snail and Slug expression was significantly decreased in the nesfatin-1 knockout cells, suggesting that it may be involved in EMT through ZEB1 signalling. |
| [36] | Xu H et al. (2018) | China | A novel function of NUCB2 in promoting the development and invasion of renal cell carcinoma | - | Knockdown (KD) RT-PCR | Upon transfection, mRNA and protein levels of nesfatin-1 decreased significantly. The KD of nesfatin-1 induced an increased apoptotic rate in RCC. Nesfatin-1 KD cells also showed significantly reduced invasion. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chinapayan, S.M.; Kuppusamy, S.; Yap, N.Y.; Perumal, K.; Gobe, G.; Rajandram, R. Potential Value of Visfatin, Omentin-1, Nesfatin-1 and Apelin in Renal Cell Carcinoma (RCC): A Systematic Review and Meta-Analysis. Diagnostics 2022, 12, 3069. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12123069
Chinapayan SM, Kuppusamy S, Yap NY, Perumal K, Gobe G, Rajandram R. Potential Value of Visfatin, Omentin-1, Nesfatin-1 and Apelin in Renal Cell Carcinoma (RCC): A Systematic Review and Meta-Analysis. Diagnostics. 2022; 12(12):3069. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12123069
Chicago/Turabian StyleChinapayan, Sugania Malar, Shanggar Kuppusamy, Ning Yi Yap, Komathi Perumal, Glenda Gobe, and Retnagowri Rajandram. 2022. "Potential Value of Visfatin, Omentin-1, Nesfatin-1 and Apelin in Renal Cell Carcinoma (RCC): A Systematic Review and Meta-Analysis" Diagnostics 12, no. 12: 3069. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12123069