

Stability and Reproducibility of Radiomic Features Based on Various Segmentation Techniques on Cervical Cancer DWI-MRI

 ,
,  , ,
, ,
Abstract
:1. Introduction
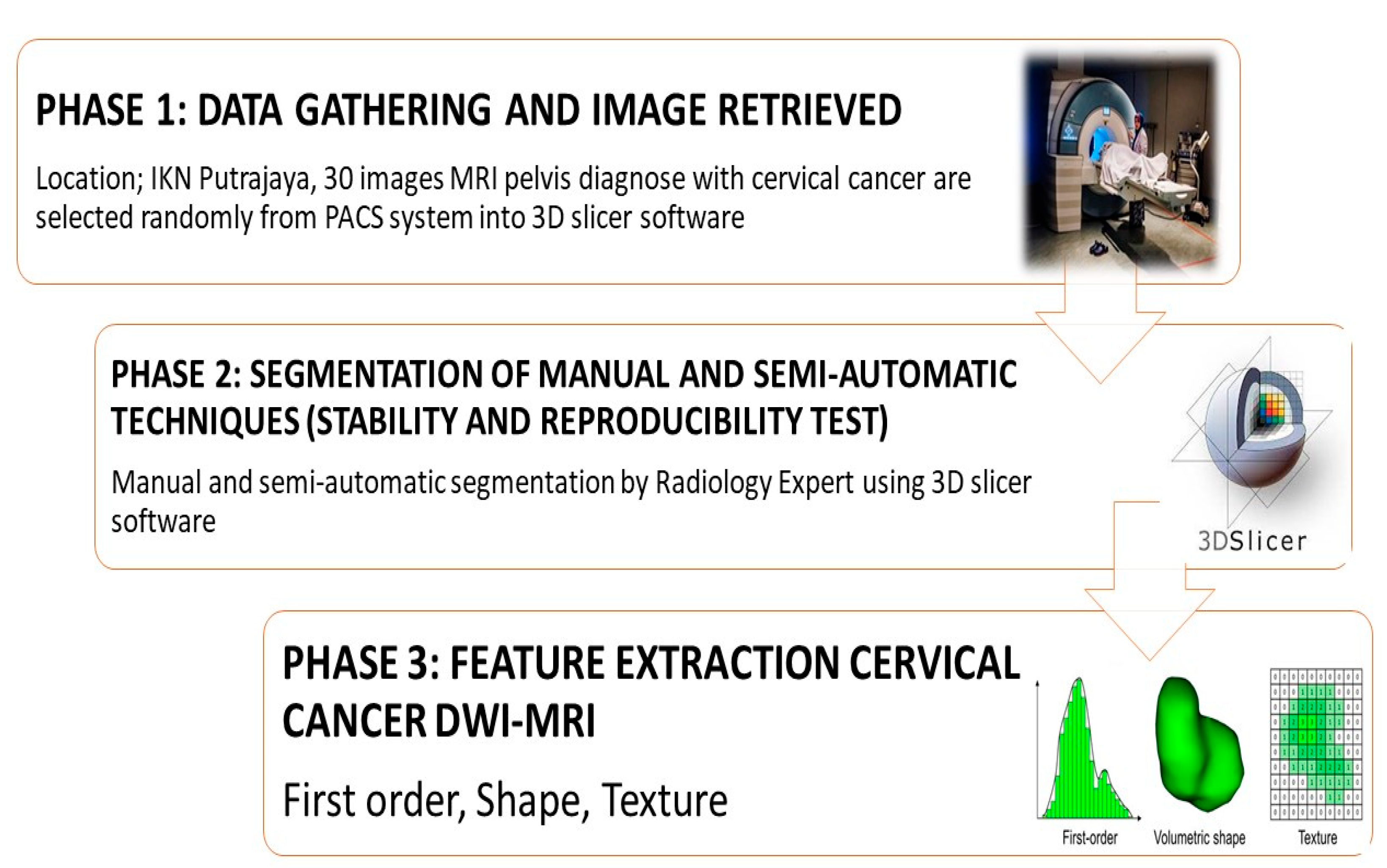
2. Materials and Methods
2.1. MRI DWI-Weighted Cervical Cancer Images
2.2. Semi-Automatic Segmentation
2.3. Feature Extraction
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- National Cancer Registry. Malaysian Study on Cancer Survival (MySCan); National Cancer Registry: Putrajaya, Malaysia, 2018; Volume 4, ISBN 9789671614204. [Google Scholar]
- Mustafa, W.A.; Halim, A.; Nasrudin, M.W.; Rahman, K.S.A. Cervical Cancer Situation in Malaysia: A Systematic Literature Review. Biocell 2022, 46, 367–381. [Google Scholar] [CrossRef]
- Schick, U.; Lucia, F.; Dissaux, G.; Visvikis, D.; Badic, B.; Masson, I.; Pradier, O.; Bourbonne, V.; Hatt, M. MRI-Derived Radiomics: Methodology and Clinical Applications in the Field of Pelvic Oncology. Br. J. Radiol. 2019, 92, 20190105. [Google Scholar] [CrossRef]
- Fiset, S.; Welch, M.L.; Weiss, J.; Pintilie, M.; Conway, J.L.; Milosevic, M.; Fyles, A.; Traverso, A.; Jaffray, D.; Metser, U.; et al. Repeatability and Reproducibility of MRI-Based Radiomic Features in Cervical Cancer. Radiother. Oncol. 2019, 135, 107–114. [Google Scholar] [CrossRef]
- Padhani, A.R.; Liu, G.; Mu-koh, D.; Chenevert, T.L.; Thoeny, H.C.; Ross, B.D.; Van Cauteren, M.; Collins, D.; Hammoud, D.A.; Rustin, G.J.S.; et al. Diffusion-Weighted Magnetic Resonance Imaging as a Cancer Biomarker: Consensus and Recommendations. Neoplasia 2009, 11, 102–125. [Google Scholar] [CrossRef] [Green Version]
- Radzi, S.F.M.; Karim, M.K.A.; Saripan, M.I.; Rahman, M.A.A.; Isa, I.N.C.; Ibahim, M.J. Hyperparameter Tuning and Pipeline Optimization via Grid Search Method and Tree-Based AutoML in Breast Cancer Prediction. J. Pers. Med. 2021, 11, 978. [Google Scholar] [CrossRef]
- Scrivener, M.; de Jong, E.E.C.; van Timmeren, J.E.; Pieters, T.; Ghaye, B.; Geets, X. Radiomics Applied to Lung Cancer: A Review. Transl. Cancer Res. 2016, 5, 398–409. [Google Scholar] [CrossRef]
- Yunus, M.M.; Sabarudin, A.; Karim, M.K.A.; Nohuddin, P.N.E.; Zainal, I.A.; Shamsul, M.S.M.; Yusof, A.K.M. Reproducibility and Repeatability of Coronary Computed Tomography Angiography (CCTA) Image Segmentation in Detecting Atherosclerosis: A Radiomics Study. Diagnostics 2022, 12, 2007. [Google Scholar] [CrossRef]
- Izdihar, K.; Karim, M.K.A.A.; Aresli, N.N.; Radzi, S.F.M.M.; Sabarudin, A.; Yunus, M.M.; Rahman, M.A.A.A.A.; Shamsul, S. Detection of Novel Coronavirus from Chest X-Ray Radiograph Images via Automated Machine Learning and CAD4COVID. In Proceedings of the 2021 International Congress of Advanced Technology and Engineering, ICOTEN, Taiz, Yemen, 4–5 July 2021; pp. 1–4. [Google Scholar] [CrossRef]
- Çinarer, G.; Emiroğlu, B.G.; Yurttakal, A.H. Prediction of Glioma Grades Using Deep Learning with Wavelet Radiomic Features. Appl. Sci. 2020, 10, 6296. [Google Scholar] [CrossRef]
- Boldrini, L.; Cusumano, D.; Chiloiro, G.; Casà, C.; Masciocchi, C.; Lenkowicz, J.; Cellini, F.; Dinapoli, N.; Azario, L.; Teodoli, S.; et al. Delta Radiomics for Rectal Cancer Response Prediction with Hybrid 0.35 T Magnetic Resonance-Guided Radiotherapy (MRgRT): A Hypothesis-Generating Study for an Innovative Personalized Medicine Approach. Radiol. Med. 2019, 124, 145–153. [Google Scholar] [CrossRef]
- Peerlings, J.; Woodruff, H.C.; Winfield, J.M.; Ibrahim, A.; Van Beers, B.E.; Heerschap, A.; Jackson, A.; Wildberger, J.E.; Mottaghy, F.M.; Desouza, N.M.; et al. Stability of Radiomics Features in Apparent Diffusion Coefficient Maps from a Multi-Centre Test-Retest Trial. Sci. Rep. 2019, 9, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Oikonomou, A.; Wong, A.; Haider, M.A.; Khalvati, F. Radiomics-Based Prognosis Analysis for Non-Small Cell Lung Cancer. Sci Rep. 2017, 7, srep46349. [Google Scholar] [CrossRef] [Green Version]
- Radzi, S.F.M.; Karim, M.K.A.; Saripan, M.I.; Abd Rahman, M.A.; Osman, N.H.; Dalah, E.Z.; Noor, N.M. Impact of Image Contrast Enhancement on Stability of Radiomics Feature Quantification on a 2D Mammogram Radiograph. IEEE Access 2020, 8, 127720–127731. [Google Scholar] [CrossRef]
- Yunus, M.M.; Mohamed Yusof, A.K.; Ab Rahman, M.Z.; Koh, X.J.; Sabarudin, A.; Nohuddin, P.N.E.; Ng, K.H.; Kechik, M.M.A.; Karim, M.K.A. Automated Classification of Atherosclerotic Radiomics Features in Coronary Computed Tomography Angiography (CCTA). Diagnostics 2022, 12, 1660. [Google Scholar] [CrossRef]
- Mohd Yunus, M.; Hui Sin, N.; Sabarudin, A.; Abdul Karim, M.K.; Ar, R.; Mohd Shamsul, M.S. Comparative Study of the Manual and Semi- Automated Segmentation Technique in Computed Tomography (CT) Lung Cancer: A Radiomics Study. J. Med. Health 2021, 16, 1–62. [Google Scholar]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Zhou, J.; Lu, J.; Gao, C.; Zeng, J.; Zhou, C.; Lai, X.; Cai, W.; Xu, M. Predicting the Response to Neoadjuvant Chemotherapy for Breast Cancer: Wavelet Transforming Radiomics in MRI. BMC Cancer 2020, 20, 100. [Google Scholar] [CrossRef] [Green Version]
- Lambin, P.; Rios-Velazquez, E.; Leijenaar, R.; Carvalho, S.; van Stiphout, R.G.P.M.; Granton, P.; Zegers, C.M.L.; Gillies, R.; Boellard, R.; Dekker, A.; et al. Radiomics: Extracting More Information from Medical Images Using Advanced Feature Analysis. Eur. J. Cancer 2012, 48, 441–446. [Google Scholar] [CrossRef] [Green Version]
- Afaq, A.; Andreou, A.; Koh, D.M. Diffusion-Weighted Magnetic Resonance Imaging for Tumour Response Assessment: Why, When and How? Cancer Imaging 2010, 10, 179–188. [Google Scholar] [CrossRef]
- Coenegrachts, K. Magnetic Resonance Imaging of the Liver: New Imaging Strategies for Evaluating Focal Liver Lesions. World J. Radiol. 2009, 1, 72–85. [Google Scholar] [CrossRef]
- Salles, H.; Magas, V.; Ganacim, F.; Gamba, H.R.; Ulbricht, L. Evaluation of Dynamic Thermograms Using Semiautomatic Segmentation Software: Applied to the Diagnosis of Thyroid Cancer. In IFMBE Proceedings; Springer Science and Business Media Deutschland GmbH: Berlin/Heidelberg, Germany, 2022; Volume 83, pp. 2417–2424. [Google Scholar]
- Clark, K.; Vendt, B.; Smith, K.; Freymann, J.; Kirby, J.; Koppel, P.; Moore, S.; Phillips, S.; Maffitt, D.; Pringle, M.; et al. The Cancer Imaging Archive (TCIA): Maintaining and Operating a Public Information Repository. J. Digit. Imaging 2013, 26, 1045–1057. [Google Scholar] [CrossRef]
- Yang, C.; Qin, L.; Xie, Y.; Liao, J. Deep Learning in CT Image Segmentation of Cervical Cancer: A Systematic Review and Meta-Analysis. Radiat. Oncol. 2022, 17, 175. [Google Scholar] [CrossRef]
- Zabihollahy, F.; Viswanathan, A.N.; Schmidt, E.J.; Lee, J. Fully Automated Segmentation of Clinical Target Volume in Cervical Cancer from Magnetic Resonance Imaging with Convolutional Neural Network. J. Appl. Clin. Med. Phys. 2022, 23, e13725. [Google Scholar] [CrossRef]
- Haniff, N.S.M.; Karim, M.K.B.A.; Ali, N.S.; Rahman, M.A.A.; Osman, N.H.; Saripan, M.I. Magnetic Resonance Imaging Radiomics Analysis for Predicting Hepatocellular Carcinoma. In Proceedings of the 2021 International Congress of Advanced Technology and Engineering, ICOTEN, Taiz, Yemen, 4–5 July 2021; pp. 1–5. [Google Scholar] [CrossRef]
- Sunil, R.A.; Bhavsar, D.; Shruthi, M.N.; Kunikullaya, U.S.; Vyas, R.K.; Parikh, A.; Mehta, M.J.; Patel, P.N. Combined External Beam Radiotherapy and Vaginal Brachytherapy versus Vaginal Brachytherapy in Stage I, Intermediate- and High-Risk Cases of Endometrium Carcinoma. J. Contemp. Brachytherapy 2018, 10, 105–114. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Zhang, K.; Jia, H.; Xia, B.; Zang, C.; Liu, Y.; Qian, L.; Dong, J. IVIM-DWI and MRI-Based Radiomics in Cervical Cancer: Prediction of Concurrent Chemoradiotherapy Sensitivity in Combination with Clinical Prognostic Factors. Magn. Reson. Imaging 2022, 91, 37–44. [Google Scholar] [CrossRef]
- Zheng, X.; Guo, W.; Dong, J.; Qian, L. Prediction of Early Response to Concurrent Chemoradiotherapy in Cervical Cancer: Value of Multi-Parameter MRI Combined with Clinical Prognostic Factors. Magn. Reson. Imaging 2020, 72, 159–166. [Google Scholar] [CrossRef]
- Boldrini, L.; Bibault, J.-E.; Masciocchi, C.; Shen, Y.; Bittner, M.-I. Deep Learning: A Review for the Radiation Oncologist. Front. Oncol. 2019, 9, 977. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Wu, C.J.; Bao, M.L.; Zhang, J.; Wang, X.N.; Zhang, Y.D. Machine Learning-Based Analysis of MR Radiomics Can Help to Improve the Diagnostic Performance of PI-RADS v2 in Clinically Relevant Prostate Cancer. Eur. Radiol. 2017, 27, 4082–4090. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Shape Features (n = 14) | GLDM, GLCM & GLRLM Texture Features (n = 14) | First Order Statistics (n = 18) |
|---|---|---|
| Voxel_Volume | Gray_Level_Variance | Interquartile_Range |
| Maximum_3D_Diameter | High_Gray_Level_Emphasis | Skewness |
| Mesh_Volume | Dependence_Entropy | Uniformity |
| Major_Axis_Length | Dependence_Non_Uniformity | Median |
| Sphericity | Gray_Level_Non_Uniformity | Energy |
| Least_Axis_Length | Small_Dependence_Emphasis | Robust_Mean_Absolute_Deviation |
| Elongation | Small_Dependence_High_Gray_Level_Emphasis | Mean_Absolute_Deviation |
| Surface_Volume_Ratio | Dependence_Non_Uniformity_Normalized | Total_Energy |
| Maximum_2D_Diameter_Slice | Large_Dependence_Emphasis | Maximum |
| Flatness | Large_Dependence_Low_Gray_Level_Emphasis | Root_Mean_Squared |
| Surface_Area | Dependence_Variance | 90 Percentile |
| Minor_Axis_Length | Large_Dependence_High_Gray_Level_Emphasis | Minimum |
| Maximum_2D_Diameter_Column | Small_Dependence_Low_Gray_Level_Emphasis | Entropy |
| Maximum_2D_Diameter_Row | Low_Gray_Level_Emphasis | Range |
| Joint_Average | Variance | |
| Sum_Average | 10 Percentile | |
| Joint_Entropy | Kurtosis | |
| Cluster_Shade | Mean | |
| Maximum_Probability | ||
| Idmn | ||
| Joint_Energy | ||
| Contrast | ||
| Difference_Entropy | ||
| Inverse_Variance | ||
| Difference_Variance | ||
| Idn | ||
| Idm | ||
| Correlation | ||
| Auto_correlation | ||
| Sum_Entropy | ||
| MCC | ||
| Sum_Squares | ||
| Cluster_Prominence | ||
| Imc2 | ||
| Imc1 | ||
| Difference_Average | ||
| Id | ||
| Cluster_Tendency | ||
| Short_Run_Low_Gray_Level_Emphasis | ||
| Gray_Level_Variance | ||
| Low_Gray_Level_Run_Emphasis | ||
| Gray_Level_Non_Uniformity_Normalized | ||
| Run_Variance | ||
| Gray_Level_Non_Uniformity | ||
| Long_Run_Emphasis | ||
| Short_Run_High_Gray_Level_Emphasis | ||
| Run_Length_Non_Uniformity | ||
| Short_Run_Emphasis | ||
| Long_Run_High_Gray_Level_Emphasis | ||
| Run_Percentage | ||
| Long_Run_Low_Gray_Level_Emphasis | ||
| Run_Entropy | ||
| High_Gray_Level_Run_Emphasis | ||
| Run_Length_Non_Uniformity_Normalized |
| Reproducibility Groups | Semi-Automatic | Manual |
|---|---|---|
| High (ICC ≥ 0.8) | 86 (100%) | 84 (97.67%) |
| Medium (0.8 ≥ ICC ≥ 0.5) | 0 (0%) | 1 (1.16%) |
| Low (ICC < 0.5) | 0 (0%) | 1 (1.16%) |
| Features | Original | SEMI_1 | SEMI_2 | MANUAL |
|---|---|---|---|---|
| Shape | Voxel_Volume | 0.999 | 0.998 | 0.955 |
| Maximum_3D_Diameter | 0.986 | 0.982 | 0.965 | |
| Mesh_Volume | 0.999 | 0.998 | 0.979 | |
| Major_Axis_Length | 0.998 | 0.988 | 0.976 | |
| Sphericity | 0.996 | 0.926 | 0.974 | |
| Least_Axis_Length * | 0.997 | 0.982 | 0.896 | |
| Elongation * | 0.869 | 0.937 | 0.897 | |
| Surface_Volume_Ratio | 0.979 | 0.989 | 0.89 | |
| Maximum_2D_Diameter_Slice | 0.993 | 0.994 | 0.89 | |
| Flatness | 0.985 | 0.989 | 0.891 | |
| Surface_Area * | 0.996 | 0.998 | 0.88 | |
| Minor_Axis_Length * | 0.982 | 0.988 | 0.871 | |
| Maximum_2D_Diameter_ Column * | 0.983 | 0.977 | 0.878 | |
| Maximum_2D_Diameter_Row * | 0.996 | 0.972 | 0.856 | |
| GLDM | Gray_Level_Variance | 0.996 | 0.995 | 0.907 |
| High_Gray_Level_Emphasis | 0.997 | 0.983 | 0.901 | |
| Dependence_Entropy | 0.872 | 0.975 | 0.901 | |
| Dependence_Non_Uniformity | 0.997 | 0.997 | 0.903 | |
| Gray_Level_Non_Uniformity | 0.998 | 0.997 | 0.903 | |
| Small_Dependence_Emphasis | 0.936 | 0.973 | 0.903 | |
| Small_Dependence_High_ Gray_Level_Emphasis | 0.968 | 0.971 | 0.903 | |
| Dependence_Non_ Uniformity_Normalized | 0.981 | 0.986 | 0.903 | |
| Large_Dependence_Emphasis | 0.988 | 0.981 | 0.903 | |
| Large_Dependence_Low_ Gray_Level_Emphasis | 0.989 | 0.994 | 0.903 | |
| Dependence_Variance | 0.979 | 0.984 | 0.903 | |
| Large_Dependence_High_ Gray_Level_Emphasis | 0.994 | 0.989 | 0.903 | |
| Small_Dependence_Low_ Gray_Level_Emphasis | 0.967 | 0.973 | 0.903 | |
| Low_Gray_Level_Emphasis | 0.998 | 0.999 | 0.904 | |
| GLCM | Joint_Average | 0.981 | 0.971 | 0.904 |
| Sum_Average | 0.981 | 0.971 | 0.915 | |
| Joint_Entropy | 0.973 | 0.973 | 0.920 | |
| Cluster_Shade | 0.991 | 0.981 | 0.954 | |
| Maximum_Probability | 1 | 1 | 0.907 | |
| Idmn | 1 | 0.997 | 0.938 | |
| Joint_Energy | 0.995 | 0.997 | 0.908 | |
| Contrast | 0.966 | 0.976 | 0.948 | |
| Difference_Entropy | 0.988 | 0.961 | 0.912 | |
| Inverse_Variance | 0.936 | 0.971 | 0.951 | |
| Difference_Variance | 0.995 | 0.989 | 0.905 | |
| Idn | 0.683 | 0.986 | 0.965 | |
| Idm | 0.962 | 0.972 | 0.904 | |
| Correlation | 0.905 | 0.972 | 0.908 | |
| Autocorrelation | 0.988 | 0.989 | 0.975 | |
| Sum_Entropy | 0.945 | 0.993 | 0.903 | |
| MCC | 0.993 | 0.995 | 0.927 | |
| Sum_Squares | 0.995 | 0.993 | 0.908 | |
| Cluster_Prominence | 0.939 | 0.999 | 0.909 | |
| Imc2 | 0.965 | 0.954 | 0.907 | |
| Imc1 | 0.978 | 0.971 | 0.906 | |
| Difference_Average | 0.991 | 0.959 | 0.906 | |
| Id | 0.958 | 0.973 | 0.902 | |
| Cluster_Tendency | 0.974 | 0.972 | 0.908 | |
| GLRLM | Short_Run_Low_Gray_Level Emphasis | 0.983 | 0.976 | 0.919 |
| Gray_Level_Variance | 0.972 | 0.963 | 0.975 | |
| Low_Gray_Level_ Run_Emphasis | 0.998 | 0.999 | 0.901 | |
| Gray_Level_Non_Uniformity Normalized | 0.998 | 0.997 | 0.904 | |
| Run_Variance | 0.981 | 0.963 | 0.903 | |
| Gray_Level_Non_Uniformity | 0.997 | 0.996 | 0.908 | |
| Long_Run_Emphasis | 0.982 | 0.966 | 0.903 | |
| Short_Run_High_Gray_Level Emphasis | 0.982 | 0.966 | 0.907 | |
| Run_Length_Non_Uniformity | 0.994 | 0.998 | 0.909 | |
| Short_Run_Emphasis | 0.996 | 0.994 | 0.902 | |
| Long_Run_High_Gray_Level Emphasis | 0.986 | 0.978 | 0.905 | |
| Run_Percentage | 1 | 0.969 | 0.901 | |
| Long_Run_Low_Gray_Level Emphasis | 0.999 | 0.998 | 0.909 | |
| Run_Entropy | 0.997 | 0.997 | 0.904 | |
| High_Gray_Level_ Run_Emphasis | 0.983 | 0.976 | 0.907 | |
| Run_Length_Non_Uniformity Normalized | 0.967 | 0.971 | 0.901 | |
| First Order Statistics | Interquartile_Range | 0.979 | 0.979 | 0.968 |
| Skewness | 0.974 | 0.936 | 0.943 | |
| Uniformity | 0.991 | 0.989 | 0.904 | |
| Median | 0.961 | 0.978 | 0.906 | |
| Energy | 0.999 | 0.999 | 0.549 | |
| Robust_Mean_Absolute Deviation | 0.966 | 0.998 | 0.904 | |
| Mean_Absolute_Deviation | 0.969 | 0.997 | 0.906 | |
| Total_Energy * | 0.999 | 0.998 | 0.053 | |
| Maximum | 0.978 | 0.944 | 0.904 | |
| Root_Mean_Squared | 0.989 | 0.978 | 0.919 | |
| 90_Percentile | 0.999 | 0.998 | 0.859 | |
| Minimum | 0.994 | 0.997 | 0.908 | |
| Entropy | 0.998 | 0.967 | 0.908 | |
| Range * | 0.997 | 0.991 | 0.853 | |
| Variance | 0.972 | 0.963 | 0.907 | |
| 10_Percentile | 0.947 | 0.986 | 0.918 | |
| Kurtosis | 0.988 | 0.948 | 0.904 | |
| Mean * | 0.999 | 0.982 | 0.861 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramli, Z.; Karim, M.K.A.; Effendy, N.; Abd Rahman, M.A.; Kechik, M.M.A.; Ibahim, M.J.; Haniff, N.S.M. Stability and Reproducibility of Radiomic Features Based on Various Segmentation Techniques on Cervical Cancer DWI-MRI. Diagnostics 2022, 12, 3125. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12123125
Ramli Z, Karim MKA, Effendy N, Abd Rahman MA, Kechik MMA, Ibahim MJ, Haniff NSM. Stability and Reproducibility of Radiomic Features Based on Various Segmentation Techniques on Cervical Cancer DWI-MRI. Diagnostics. 2022; 12(12):3125. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12123125
Chicago/Turabian StyleRamli, Zarina, Muhammad Khalis Abdul Karim, Nuraidayani Effendy, Mohd Amiruddin Abd Rahman, Mohd Mustafa Awang Kechik, Mohamad Johari Ibahim, and Nurin Syazwina Mohd Haniff. 2022. "Stability and Reproducibility of Radiomic Features Based on Various Segmentation Techniques on Cervical Cancer DWI-MRI" Diagnostics 12, no. 12: 3125. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics12123125