
Related Factors for Unfavorable Disease Course in Patients with Crohn’s Disease: An Observational Retrospective Study


Abstract
:1. Introduction
2. Materials and Methods
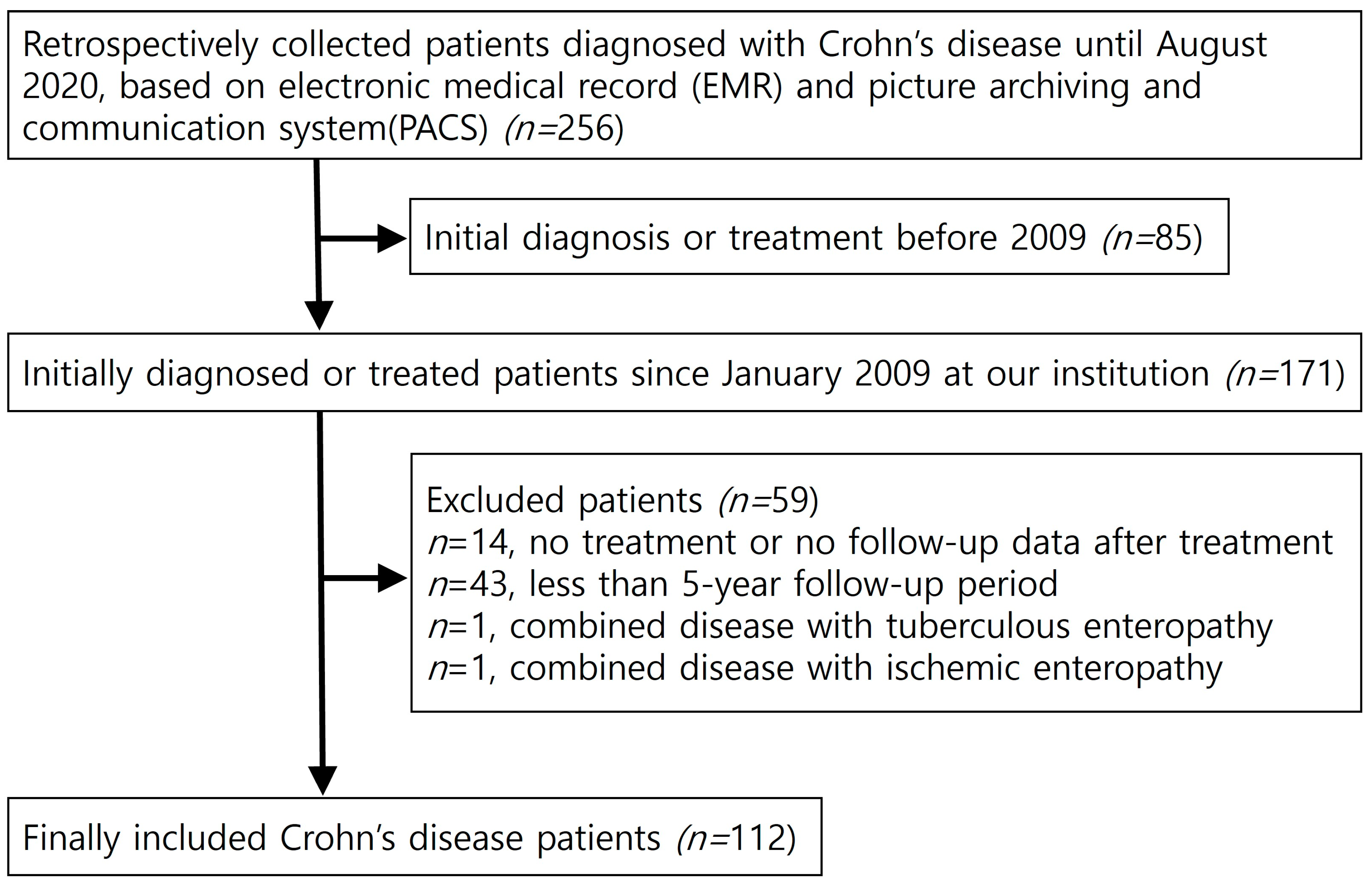
2.1. Patients
2.2. Clinical Data Analyses
2.3. Radiologic and Endoscopic Analyses of Disease Pattern
2.4. Classification of Disease course during the Entire Follow-Up Period
2.5. CT Techniques
2.6. Statistical Analyses
3. Results
3.1. Analyses of Disease Course during the Long-Term Follow-Up Period
3.1.1. Disease Course and Outcomes
3.1.2. Changes in Disease Patterns
3.2. Analyses of Disease Characteristics for Unfavorable Disease Course
3.3. Significant Factors for Unfavorable Disease Course
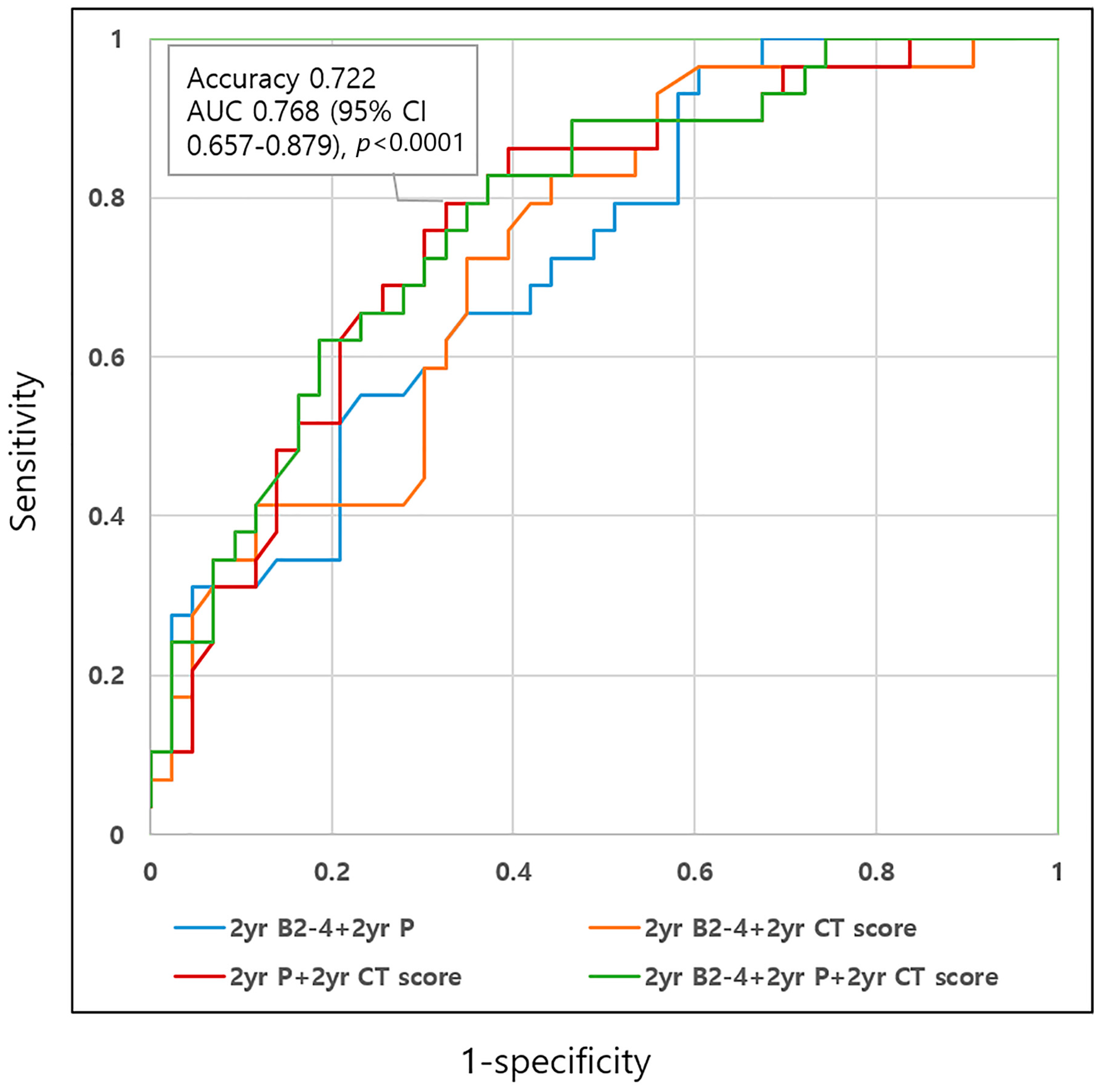
3.4. ROC Analyses for Unfavorable Disease Course Using Selected Disease Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pariente, B.; Cosnes, J.; Danese, S.; Sandborn, W.J.; Lewin, M.; Fletcher, J.G.; Chowers, Y.; D’Haens, G.; Feagan, B.G.; Hibi, T.; et al. Development of the Crohn’s disease digestive damage score, the Lemann score. Inflamm. Bowel Dis. 2011, 17, 1415–1422. [Google Scholar] [CrossRef] [Green Version]
- Lichtenstein, G.R.; Loftus, E.V.; Isaacs, K.L.; Regueiro, M.D.; Gerson, L.B.; Sands, B.E. ACG Clinical Guideline: Management of Crohn’s Disease in Adults. Am. J. Gastroenterol. 2018, 113, 481–517. [Google Scholar] [CrossRef] [PubMed]
- Silverberg, M.S.; Satsangi, J.; Ahmad, T.; Arnott, I.D.; Bernstein, C.N.; Brant, S.R.; Caprilli, R.; Colombel, J.F.; Gasche, C.; Geboes, K.; et al. Toward an integrated clinical, molecular and serological classification of inflammatory bowel disease: Report of a Working Party of the 2005 Montreal World Congress of Gastroenterology. Can. J. Gastroenterol. 2005, 19 (Suppl. A), 5A–36A. [Google Scholar] [CrossRef] [PubMed]
- Gajendran, M.; Loganathan, P.; Catinella, A.P.; Hashash, J.G. A comprehensive review and update on Crohn’s disease. Dis. Mon. 2018, 64, 20–57. [Google Scholar] [CrossRef] [PubMed]
- Van Assche, G.; Dignass, A.; Panes, J.; Beaugerie, L.; Karagiannis, J.; Allez, M.; Ochsenkuhn, T.; Orchard, T.; Rogler, G.; Louis, E.; et al. The second European evidence-based Consensus on the diagnosis and management of Crohn’s disease: Definitions and diagnosis. J. Crohns. Colitis 2010, 4, 7–27. [Google Scholar] [CrossRef] [Green Version]
- Loftus, E.V., Jr.; Silverstein, M.D.; Sandborn, W.J.; Tremaine, W.J.; Harmsen, W.S.; Zinsmeister, A.R. Crohn’s disease in Olmsted County, Minnesota, 1940–1993: Incidence, prevalence, and survival. Gastroenterology 1998, 114, 1161–1168. [Google Scholar] [CrossRef]
- Kolkman, J.J.; Falke, T.H.M.; Roos, J.C.; Van Dijk, D.H.; Bannink, I.M.J.; Den Hollander, W.; Cuesta, M.A.; Peña, A.S.; Meuwissen, S.G.M. Computed tomography and granulocyte scintigraphy in active inflammatory bowel disease. Dig. Dis. Sci. 1996, 41, 641–650. [Google Scholar] [CrossRef]
- Mao, R.; Gao, X.; Zhu, Z.-H.; Feng, S.-T.; Chen, B.-L.; He, Y.; Cui, Y.; Li, Z.-P.; Hu, P.-J.; Chen, M.-H. CT Enterography in Evaluating Postoperative Recurrence of Crohn’s Disease after Ileocolic Resection: Complementary Role to Endoscopy. Inflamm. Bowel Dis. 2013, 19, 977–982. [Google Scholar] [CrossRef]
- Mohamed, A.M.; Amin, S.K.; El-Shinnawy, M.A.; Elfouly, A.; Baki, A.H. Role of CT enterography in assessment of Crohn’s disease activity: Correlation with histopathologic diagnosis. Egypt. J. Radiol. Nucl. Med. 2012, 43, 353–359. [Google Scholar] [CrossRef] [Green Version]
- Tielbeek, J.A.W.; Bipat, S.; Boellaard, T.N.; Nio, C.Y.; Stoker, J. Training readers to improve their accuracy in grading Crohn’s disease activity on MRI. Eur. Radiol. 2014, 24, 1059–1067. [Google Scholar] [CrossRef]
- Puylaert, C.A.J.; Tielbeek, J.A.W.; Bipat, S.; Stoker, J. Grading of Crohn’s disease activity using CT, MRI, US and scintigraphy: A meta-analysis. Eur. Radiol. 2015, 25, 3295–3313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruining, D.H.; Zimmermann, E.M.; Loftus, E.V., Jr.; Sandborn, W.J.; Sauer, C.G.; Strong, S.A.; Society of Abdominal Radiology Crohn’s Disease-Focused Panel. Consensus Recommendations for Evaluation, Interpretation, and Utilization of Computed Tomography and Magnetic Resonance Enterography in Patients With Small Bowel Crohn’s Disease. Gastroenterology 2018, 154, 1172–1194. [Google Scholar] [CrossRef] [PubMed]
- Levine, A.; Griffiths, A.; Markowitz, J.; Wilson, D.C.; Turner, D.; Russell, R.K.; Fell, J.; Ruemmele, F.M.; Walters, T.; Sherlock, M.; et al. Pediatric modification of the Montreal classification for inflammatory bowel disease: The Paris classification. Inflamm. Bowel Dis. 2011, 17, 1314–1321. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.; Fedorak, R.N.; Kaplan, G.G.; Dieleman, L.A.; Devlin, S.M.; Stern, N.; Kroeker, K.I.; Seow, C.H.; Leung, Y.; Novak, K.L.; et al. Long-term Maintenance of Clinical, Endoscopic, and Radiographic Response to Ustekinumab in Moderate-to-Severe Crohn’s Disease: Real-world Experience from a Multicenter Cohort Study. Inflamm. Bowel Dis. 2017, 23, 833–839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solberg, I.C.; Vatn, M.H.; Hoie, O.; Stray, N.; Sauar, J.; Jahnsen, J.; Moum, B.; Lygren, I.; Group, I.S. Clinical course in Crohn’s disease: Results of a Norwegian population-based ten-year follow-up study. Clin. Gastroenterol. Hepatol. 2007, 5, 1430–1438. [Google Scholar] [CrossRef] [PubMed]
- Thia, K.T.; Sandborn, W.J.; Harmsen, W.S.; Zinsmeister, A.R.; Loftus, E.V., Jr. Risk factors associated with progression to intestinal complications of Crohn’s disease in a population-based cohort. Gastroenterology 2010, 139, 1147–1155. [Google Scholar] [CrossRef] [Green Version]
- Ye, B.D.; Yang, S.K.; Cho, Y.K.; Park, S.H.; Yang, D.H.; Yoon, S.M.; Kim, K.J.; Byeon, J.S.; Myung, S.J.; Yu, C.S.; et al. Clinical features and long-term prognosis of Crohn’s disease in Korea. Scand. J. Gastroenterol. 2010, 45, 1178–1185. [Google Scholar] [CrossRef]
- Rackovsky, O.; Hirten, R.; Ungaro, R.; Colombel, J.F. Clinical updates on perianal fistulas in Crohn’s disease. Expert. Rev. Gastroenterol. Hepatol. 2018, 12, 597–605. [Google Scholar] [CrossRef]
- Beaugerie, L.; Le Quintrec, Y.; Paris, J.C.; Godchaux, J.M.; Saint-Raymond, A.; Schmitz, J.; Ricour, C.; Haddak, M.; Diday, E. Testing for course patterns in Crohn’s disease using clustering analysis. Gastroenterol. Clin. Biol. 1989, 13, 1036–1041. [Google Scholar]
- Munkholm, P.; Langholz, E.; Davidsen, M.; Binder, V. Disease activity courses in a regional cohort of Crohn’s disease patients. Scand. J. Gastroenterol. 1995, 30, 699–706. [Google Scholar] [CrossRef]
- Oriuchi, T.; Hiwatashi, N.; Kinouchi, Y.; Takahashi, S.; Takagi, S.; Negoro, K.; Shimosegawa, T. Clinical course and longterm prognosis of Japanese patients with Crohn’s disease: Predictive factors, rates of operation, and mortality. J. Gastroenterol. 2003, 38, 942–953. [Google Scholar] [CrossRef] [PubMed]
- Ouaz, A.; Fekih, M.; Labidi, A.; Ben Mustapha, N.; Serghini, M.; Zouiten, L.; Boubaker, J.; Filali, A. Changes of Crohn’s disease phenotype over time. Tunis Med. 2016, 94, 167–170. [Google Scholar] [PubMed]
- Song, E.M.; Lee, H.S.; Kim, Y.J.; Oh, E.H.; Ham, N.S.; Kim, J.; Hwang, S.W.; Park, S.H.; Yang, D.H.; Ye, B.D.; et al. Clinical outcomes and long-term prognosis of perianal Crohn’s disease in an Asian population. J. Gastroenterol. Hepatol. 2021, 36, 1571–1579. [Google Scholar] [CrossRef]
- Niriella, M.A.; Liyanage, I.K.; Kodisinghe, S.K.; De Silva, A.P.; Jayatissa, A.; Navarathne, N.M.M.; Peiris, R.K.; Kalubovila, U.P.; Kumarasena, S.R.; Jayasekara, R.W.; et al. Changing phenotype, early clinical course and clinical predictors of inflammatory bowel disease in Sri Lanka: A retrospective, tertiary care-based, multi-centre study. BMC Gastroenterol. 2021, 21, 71. [Google Scholar] [CrossRef]
- Yan, W.; Meihao, W.; Zihan, S.; Lingjie, H.; Haotian, C.; Qian, C.; Lianli, S. Correlation Between Crohn’s Disease Activity and Serum Selenium Concentration. Clin. Ther. 2022, 44, 736–743.e733. [Google Scholar] [CrossRef] [PubMed]
- van Rheenen, P.F.; Aloi, M.; Assa, A.; Bronsky, J.; Escher, J.C.; Fagerberg, U.L.; Gasparetto, M.; Gerasimidis, K.; Griffiths, A.; Henderson, P.; et al. The Medical Management of Paediatric Crohn’s Disease: An ECCO-ESPGHAN Guideline Update. J. Crohns. Colitis 2020, 15, 171–194. [Google Scholar] [CrossRef]
- Makanyanga, J.C.; Pendse, D.; Dikaios, N.; Bloom, S.; McCartney, S.; Helbren, E.; Atkins, E.; Cuthbertson, T.; Punwani, S.; Forbes, A.; et al. Evaluation of Crohn’s disease activity: Initial validation of a magnetic resonance enterography global score (MEGS) against faecal calprotectin. Eur. Radiol. 2014, 24, 277–287. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| None: 0 | Mild: 1 | Moderate: 2 | Severe: 3 | |
|---|---|---|---|---|
| Wall thickness | ≤3 mm | 4–5 mm | 6–7 mm | ≥8 mm |
| Wall enhancement (compared to adjacent vessels) | Normal | Mild: minor increase, but less than vessels | Moderate: moderate increase, but less than vessels | Severe: marked increase, similar to vessels |
| Enhancement pattern | Normal | Homogenous | Mucosal ₤ | Layered € |
| Disease length | None | 5 cm | 5–15 cm | >15 cm |
| Comb sign | No | Yes | ||
| None: no signs of active disease. Mild: total scores ≤6, no features with score 3. Moderate: total scores 7–10 or presence of any one feature ≥3. Severe: total scores ≥11 or presence of at least one complication including abscess, fistula, or stenosis. | ||||
| Variables | Overall | Well-Controlled Disease Course (n = 72) (Remission+ Stable) | Unfavorable Disease Course (n = 40) (Refractory+ Relapse) | p-Value (<0.05) |
|---|---|---|---|---|
| Age at diagnosis, mean (±sd) | 24.73 (±9.4) | 25.15 ± 9.84 | 23.98 ± 8.63 | 0.709 |
| Male (%) | 92 (82.1) | 60 (83.33) | 32 (80) | 0.797 |
| Smoking (%) | 0.382 | |||
| Nonsmoker | 26 (23.2) | 17 (70.83) | 9 (60) | |
| Former | 2 (1.8) | 2 (8.33) | 0 | |
| Current | 11 (9.8) | 5 (20.83) | 6 (40) | |
| Unknown | 73 (65.2) | |||
| Family history (%) | 1.000 | |||
| No | 23 (20.5) | 15 (93.75) | 8 (100) | |
| Yes | 1 (0.9) | 1 (6.25) | 0 | |
| Unknown | 88 (78.6) | |||
| Prior operation history (%) | 6 (5.4) | 3 (4.2) | 3 (7.5) | 0.664 |
| Prior perianal operation history (%) | 24 (21.4) | 14 (19.44) | 10 (25) | 0.631 |
| Systemic steroid at initial visit (%) | 6 (5.4) | 3 (4.92) | 3 (8.11) | 0.669 |
| Induction of remission (%) | 0.14 | |||
| Steroid (per oral) ± sulfasalazine/antibiotics | 90 (80.4) | 61 (84.7) | 29 (72.5) | |
| Biologics (IFX or ADA) | 22 (19.6) | 11 (15.2) | 11 (27.5) | |
| Immunosuppressants (IS) (%) | 108 (96.4) | 69 (95.8) | 39 (97.5) | 1.000 |
| Time points of first usage of Biologics (%) | 0.012 | |||
| Initial | 26 (29.2) | 13 (25.4) | 13 (34.2) | |
| Within 2-year f/u | 24 (26.9) | 14 (27.4) | 10 (26.3) | |
| Within 5-year f/u | 23 (25.8) | 16 (31.4) | 7 (18.4) | |
| After 5-year f/u | 16 (17.9) | 8 (15.7) | 8 (21) | |
| Combination therapy (%) | 72 (64.3) | 39 (55.71) | 33 (82.5) | 0.006 |
| Switch of IS to biologics (%) | 62 (55.4) | 37 (51.39) | 25 (62.5) | 0.322 |
| Switch of one to another biologic (%) | 35 (31.3) | 9 (12.5) | 26 (65) | <0.0001 |
| Dose intensification (%) | 21 (18.8) | 5 (6.94) | 16 (40) | <0.0001 |
| Variables | Overall | Well-Controlled Disease Course (n = 72) (Remission+ Stable) | Unfavorable Disease Course (n = 40) (Refractory+ Relapse) | p-Value (<0.05) |
|---|---|---|---|---|
| Initial visit | ||||
| Location at initial visit(n, %) | 0.839 | |||
| L1 | 26 (23.2) | 18 (25) | 8 (20) | |
| L2 | 3 (2.7) | 2 (2.78) | 1 (2.5) | |
| L3 | 83 (74.1) | 52 (72.22) | 31 (77.5) | |
| L4 lesion at initial visit (n, %) | 48 (42.9) | 28 (38.89) | 20 (50) | 0.319 |
| α L4a | 9/31 (29) | 6/18 (33.3) | 3/13 (23) | |
| β L4b | 8/31 (25.8) | 4/18 (22.2) | 4/13 (30.7) | 0.897 |
| Behavior at initial visit (n, %) | 1.000 | |||
| B1 | 89 (79.5) | 57 (79.17) | 32 (80) | |
| B2 | 7 (6.3) | 5 (6.94) | 2 (5) | |
| B3 | 16 (14.2) | 10 (13.8) | 6 (15) | |
| γ B2B3 | 1/31 (3.2) | 0/18 | 1/13 (3.2) | |
| Perianal disease at initial visit (n, %) | 80 (71.4) | 49 (68.06) | 31 (77.5) | 0.383 |
| CT activity score at initial visit (n, %) | 0.137 | |||
| None | 3 (2.7) | 2 (2.82) | 1 (2.5) | |
| Mild | 6 (5.4) | 6 (8.45) | 0 (0) | |
| Moderate | 34 (30.4) | 24 (33.8) | 10 (25) | |
| Severe | 68 (60.7) | 39 (54.93) | 29 (72.5) | |
| SES-CD score at initial visit (mean± SD) | 9.97 ± 5.57 | 9.88 ± 5.52 | 10.15 ± 5.72 | 0.804 |
| SES-CD score at initial visit (n, %) | 0.95 | |||
| Remission (<4) | 9 (8) | 6 (8) | 3 (7.5) | |
| Mild (4–6) | 24 (21.4) | 15 (21.1) | 9 (22.5) | |
| Moderate (7–15) | 56 (50) | 37 (52.1) | 19 (47.5) | |
| Severe (>15) | 22 (19.6) | 13 (18.3) | 9 (22.5) | |
| Second-year follow up | ||||
| Location at 2nd-year f/u | 0.345 | |||
| No lesion (n, %) | 6 (7.9) | 5 (10.42) | 1 (3.23) | |
| L1 | 28 (35.4) | 19 (39.58) | 9 (29.03) | |
| L2 | 6 (7.6) | 4 (8.33) | 2 (6.45) | |
| L3 | 39 (49.4) | 20 (41.67) | 19 (61.29) | |
| L4 lesion at 2nd-year f/u (n, %) | 22 (28.2) | 10 (21.28) | 12 (38.71) | 0.124 |
| α L4a | 3/20 (15) | 2/12 (16.6) | 1/8 (12.5) | |
| β L4b | 3/20 (15) | 1/12 (8.3) | 2/8 (25) | 0.785 |
| Behavior at 2nd-year f/u (n, %) | 0.045 | |||
| No lesion | 5 (6.3) | |||
| B1 | 58 (73.4) | B1: 42 (87.5) | B1: 21 (67.74) | |
| B2 | 7 (8.9) | B2-3: 6 (12.5) | B2-3: 10 (32.26) | |
| B3 | 9 (11.4) | |||
| Perianal disease at 2nd-year f/u (n, %) | 41 (51.3) | 19 (39.58) | 22 [68.75] | 0.013 |
| CT activity score at 2nd-year f/u (n, %) | <0.001 | |||
| None | 13 (18.1) | 10 (23.26) | 3 (10.34) | |
| Mild | 14 (19.4) | 12 (27.91) | 2 (6.9) | |
| Moderate | 24 (33.3) | 16 (37.21) | 8 (27.59) | |
| Severe | 21 (29.2) | 5 (11.63) | 16 (55.17) | |
| SES-CD score at 2nd-year f/u (mean± SD) | 4.36 ± 4.86 | 4.67± 5.27 | 3.82 ± 4.06 | 0.422 |
| SES-CD score at 2nd-year f/u (n, %) | 0.923 | |||
| Remission (<4) | 56 (50) | 34 (56.6) | 22 (64.7) | |
| Mild (4–6) | 18 (16.1) | 12 (20) | 6 (17.6) | |
| Moderate (7–15) | 14 (12.5) | 10 (16.6) | 4 (11.7) | |
| Severe (>15) | 6 (5.4) | 4 (6.7) | 2 (5.8) | |
| Exp(B) | 95% Confidence Interval (CI) | p-Value | |
|---|---|---|---|
| Initial L4 lesion | 1.6 | 0.71–3.60 | 0.255 |
| Initial disease behavior: B2-3 | 0.99 | 0.35–2.80 | 0.990 |
| Initial perianal lesion | 1.49 | 0.58–3.84 | 0.412 |
| Initial moderate-to-severe CT activity score | 3.65 | 0.56–23.83 | 0.176 |
| Initial SES-CD score | 1.01 | 0.94–1.08 | 0.82 |
| 2-year L4 lesion | 2.33 | 0.83–6.56 | 0.109 |
| 2-year disease behavior: B2-3 | 3.87 | 1.14–13.16 | 0.030 |
| 2-year perianal disease | 3.43 | 1.24–9.51 | 0.017 |
| 2-year moderate-to-severe CT activity score | 4.95 | 1.55–15.83 | 0.007 |
| 2-year SES-CD score | 0.96 | 0.87–1.05 | 0.41 |
| Use of immunosuppressants (IS) | 1.18 | 0.13–10.58 | 0.885 |
| First biologics use within 2 years | 0.48 | 0.21–1.07 | 0.072 |
| Biologics change | 12.38 | 4.54–33.75 | <0.0001 |
| Dose intensification | 7.81 | 2.59–23.51 | <0.0001 |
| Combination therapy | 3.31 | 1.30–8.43 | 0.012 |
| Sensitivity | Specificity | Accuracy | AUC € (CI) | p-Value | |
|---|---|---|---|---|---|
| 2yr disease behavior: B2-3 | 0.621 (18/29) | 0.628 (27/43) | 0.625 (45/72) | 0.625 | 0.07 |
| 2yr perianal disease | 0.793 (23/29) | 0.558 (24/43) | 0.653 (47/72) | 0.673 | 0.007 |
| 2yr moderate-to-severe CT activity score | 0.759 (22/29) | 0.628 (27/43) | 0.681 (49/72) | 0.686 | 0.004 |
| 2yr B2-4+ 2yr P | 0.655 (19/29) | 0.651 (28/43) | 0.653 (47/72) | 0.724 | 0.0002 |
| 2yr B2-3+ 2yr CT score | 0.724 (21/29) | 0.651 (28/43) | 0.681 (49/72) | 0.731 | 0.0001 |
| 2yr P+ 2yr CT score | 0.793 (23/29) | 0.674 (29/43) | 0.722 (52/72) | 0.768 | <0.0001 |
| 2yr B2-3 + 2yr P + 2yr CT score | 0.759 (22/29) | 0.674 (29/43) | 0.708 (51/72) | 0.779 | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, D.Y.; You, M.-W.; Oh, C.H.; Park, S.J. Related Factors for Unfavorable Disease Course in Patients with Crohn’s Disease: An Observational Retrospective Study. Diagnostics 2023, 13, 273. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics13020273
Han DY, You M-W, Oh CH, Park SJ. Related Factors for Unfavorable Disease Course in Patients with Crohn’s Disease: An Observational Retrospective Study. Diagnostics. 2023; 13(2):273. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics13020273
Chicago/Turabian StyleHan, Dong Yoon, Myung-Won You, Chi Hyuk Oh, and Seong Jin Park. 2023. "Related Factors for Unfavorable Disease Course in Patients with Crohn’s Disease: An Observational Retrospective Study" Diagnostics 13, no. 2: 273. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics13020273