
Exploring the Intersection of Artificial Intelligence and Clinical Healthcare: A Multidisciplinary Review

 ,
,  ,
,  , and
, and
Abstract
:1. Introduction
1.1. What Is AI?
1.2. How Does It Work?
1.3. Methodology
2. Artificial Intelligence Branches Explained
2.1. Machine Learning
2.2. Computer Vision
2.3. Fuzzy Logic
- ▪
- Rule base: Has all the rules and if–then conditions.
- ▪
- Fuzzification: Helps to convert inputs.
- ▪
- Inference engine: Determines the degree of match between rules and fuzzy inputs.
- ▪
- Defuzzification: Converts fuzzy sets into crips values.
2.4. Expert Systems
2.5. Robotics
2.6. Neural Networks/Deep Learning
2.7. Natural Language Processing
3. Artificial Intelligence in Medicine
3.1. A Brief History of AI
3.2. Artificial Intelligence Algorithms in Medicine
- (1)
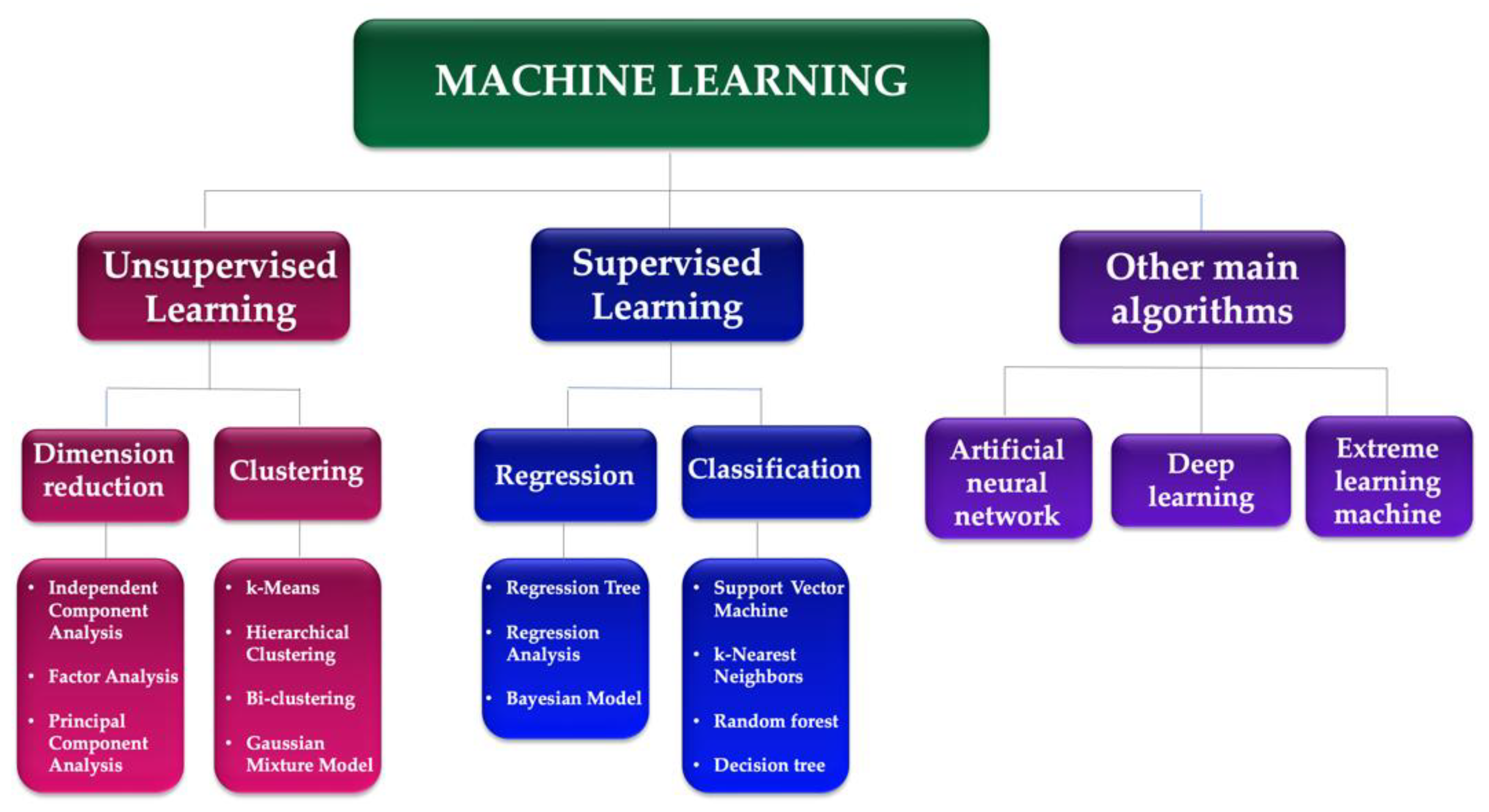
- Supervised learning: These models are trained on labeled data to learn patterns and make predictions. They are widely used in medical image analyses, such as identifying cancer cells in pathology images or detecting lung nodules in CT scans [7]. Some examples of supervised learning models used in medicine include convolutional neural networks (CNNs), deep neural networks (DNNs), and random forests.
- (2)
- Unsupervised learning models: These models are used to identify patterns and relationships in unlabeled data. They are used in medical data clustering, anomaly detection, and feature extraction. Some examples of unsupervised learning models used in medicine include k-means clustering, a principal component analysis (PCA), and autoencoders [31].
- (3)
- Reinforcement learning models: These models are used to learn from trial-and-error interactions with an environment. They can be used in medical decision making, such as personalized treatment planning and drug dosage optimization [32]. Examples of such models include Q-learning, policy gradient methods, and actor–critic models.
- (4)
- Hybrid models: These models combine multiple types of AI models to leverage their strengths and overcome their weaknesses. For example, a hybrid model could use a CNN to identify features in medical images followed by an unsupervised learning algorithm to cluster the features and identify subtypes of cancer [33].
4. AI in Cardiology

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Target | Type of Algorithm | Data Sample | Results | Study |
|---|---|---|---|---|
| Signal processing | ||||
| Detection of VF and VT (shockable rhythms) to improve shock advice algorithms in automated external defibrillators | Convolutional neural network as a feature extractor and boosting classifier | 1135 shockable segments and 5185 non-shockable segments from 57 records in public databases | Accuracy 99.3%, sensitivity 97.1%, specificity 99.4% | Nguyen et al., (2018) [57] |
| Automated detection of AF based on PPG and accelerometer recordings of smartwatches | Deep neural network with heuristic pre-training | Heart rate and step count data obtained using the Cardiogram mobile application on Apple Watches from 9759 Health eHeart Study participants | Sensitivity 98.0%, specificity 90.2%, C-statistic 0.97 | Tison et al., (2018) [58] |
| Binary classification ofcardiovascular abnormality using time–frequency features of cardio-mechanical signals, namely, SCG and GCG signals | Decision tree and SVM methods with features generated by a continuous wavelet transform | Experimental measurements from 12 patients with cardiovascular diseases and 12 healthy subjects | Accuracy > 94%, with the best performance of SVM applied to GCG features (99.5%) | Yang et al., (2018) [59] |
| Automated detection of AF based on Apple Watch Series 2 or 3 with KardioBand (AliveCor) | SmartRhythm 2.0, a convolutional neural network | Data of the heart rate, activity level, and ECGs from 7500 AliveCor users (training), and data from 24 patients with an insertable cardiac monitor and history of paroxysmal AF (validation) | Episode sensitivity 97.5%, duration sensitivity 97.7%, patient sensitivity 83.3% overall and 100% during time worn | Wasserlauf et al., (2019) [60] |
| Identify LV territory of regional wall motion abnormality on parasternal short-axis views | Convolutional neural networks (supervised) | In total, 400 patients (1200 short-axis echo videos) who had undergone a coronary angiography and echo | Area under the receiver operating characteristic curve for detection of regional wall motion abnormalities: 0.90–0.97 | Kusunose et al., (2019) [61] |
| Identification of asymptomatic LV dysfunction based on an ECG | Convolutional neural network using the Keras framework with a Tensorflow (Google) backend and Python | ECG–TTE pairs: 35,970 (training), 8989 (internal validation), 52,870 (testing) | Accuracy 85.7%, sensitivity 86.3%, specificity 85.7%, C-statistic 0.93 | Attia et al., (2019) [50] |
| Image processing | ||||
| Rapid and reproducible measurement of LV volumes, EF, and average biplane LS on ECG | Convolutional neural networks | Four- and two-chamber ECG views from 255 patients in sinus rhythm | Feasibility 98%, good agreements with the reference for automated EF and LS, with no variability | Knackstedt et al., (2015) [62] |
| Decreasing the computational demand of the FFR calculation by developing a ML-based model as an alternative to computational fluid dynamics approaches | Deep neural network | In total, 125 lesions in 87 patient-specific anatomic models generated from CT data using image segmentation | Excellent correlation (0.9994; p < 0.001) and no systematic bias in the Bland–Altman analysis: FFR 0.80 was predicted with sensitivity 81.6%, specificity 83.9%, accuracy 83.2% | Itu et al., (2016) [63] |
| Automated ECG interpretation, including view identification, segmentation of cardiac chambers across five commonviews, quantification of structures and function, and disease detection | Convolutional neural networks | In total, 14,035 echocardiograms spanning a 10-year period | Identification of views in >95%, median absolute deviation of 15–17% for structure and <10% for function, detection of hypertrophic cardiomyopathy, cardiac amyloidosis, and pulmonary disease with C-statistics of 0.93, 0.87, and 0.85, respectively | Zhang et al., (2018) [64] |
| Measurement of RV and LV volume and function in MRI images for a range of clinical indications and pathologies | Deep neural network | In total, 200 non-congenital clinical cardiac MRI examinations | Strong correlations for LV (>0.94) and RV (>0.92) volumes | Retson et al., (2020) [65] |
| Detection of subclinical AF | Convolutional neural networks | Training set of 454,789 images and testing on 130,801 images | AUC 0.90, sensitivity 82.3%, specificity 83.4%, accuracy 83.3% | Alzubaidi et al., (2021) [66] |
| Clinical risk stratification | ||||
| Identification of HF cases from both structured and unstructured EMRs | Random forest models | In total, 2,139,299 notes in the Maine Health Information Exchange EMR database from 1 July 2012 to 30 June 2014 | Positive predictive value of 91.4% | Wang et al., (2015) [67] |
| Development of CHIEF to automatically extract LV function mentions and values, congestive HF medications, and documented reasons for a patient not receiving these medications | Combination of rules, dictionaries, and ML methods | Various clinical notes from 1083 Veterans Health Administration patients | High recall and precision for HF medications and EF (>0.960), while only reaching fair recall and precision for reasons for not prescribing HF medications (<0.400) | Meystre et al., (2017) [68] |
| Risk prediction model of incident essential hypertension within the following year | Feature selection and generation of an ensemble of classification trees with the use of XGBoost | Data from individual patient electronic health records as part of the Health Information Exchange data set of Maine | C-statistics of 0.917 in the retrospective cohort and 0.870 in the prospective cohort | Ye et al., (2018) [69] |
| Predict survival following a routine echo using clinical and structured echo report data | Nonlinear random forest classifier (supervised) | In total, 171,519 patients (331,317 echo studies) using 90 clinical variables, LVEF, and 57 echo measurements. Labels were from clinical data and reported echo measurements | Area under the receiver operating characteristic curve: 1-year mortality, 0.85 5-year mortality, 0.89 | Samad et al., (2019) [70] |
| Predict in-hospital mortality following an echo in patients admitted with heart disease using echo report data | Deep neural network (supervised) | In total, 25,776 in-patients admitted with heart disease based on ICD-10 codes. Labels were from clinical data and reported echo measurements | Area under the receiver operating characteristic curve: Overall, 0.90 Coronary heart disease subgroup, 0.96 Heart failure subgroup, 0.91 Area under the precision–recall curve, 0.28 | Kwon et al., (2019) [71] |
| Prediction of CAD on CTA | Boosted ensemble algorithm | Clinical, CTA (CACS) in 13,054 subjects | AUC 0.881 | Lu et al., (2022) [72] |
5. AI Implications in Immunology, Allergology, and COVID-19
6. AI in Endocrinology
7. AI in Dentistry
| Target | AI Model | Sample | Results | Study |
|---|---|---|---|---|
| Detection of simulated dental caries | Learning vector quantization | Teeth | AI is beneficial in diagnosing dental cavities. | Kositbowornchai et al., (2006) [150] |
| Dental caries detection | Adaptive dragonfly algorithm and neural network | 120 dental images | Using the image processing method, a unique and upgraded model exhibits a much higher performance in detecting dental caries. | Patil et al., (2019) [151] |
| Dental caries detection | CNN | 185 transillumination images | ROC of 83.6% for occlusal caries and ROC of 84.6% for proximal caries. | Casalegno et al., (2019) [152] |
| Root caries identification | ANN | 357 variables in 5135 cases | 97.1%, 95.1% precision, 99.6% sensitivity, 94.3% specificity. | Hung et al., (2019) [153] |
| To predict post-Streptococcus mutants | ANN | 45 primary molars | Efficiency of 0.99033 | Javed et al., (2020) [154] |
| Dental caries diagnosis | Backpropagation neural network | 105 periapical X-rays | This model yielded an accuracy of 97.1%, a false positive (FP) rate of 2.8%, a receiver operating characteristic (ROC) area of 0.987, and a precision–recall curve (PRC) area of 0.987. | Geetha et al., (2020) [155] |
| Diagnosis of interproximal caries lesions | CNN | 1000 digital bitewing radiographs | Total accuracy of 94.59% AUC of 7.19% | Bayraktar and Ayan (2022) [156] |
| Caries detection | CNN | 2417 photographs | Accuracy of 92.5% (SE, 89.6; SP, 94.3; AUC, 0.964). | Kühnisch et al., (2022) [146] |
| Caries detection | CNN | 226 extracted teeth 1319 teeth from 56 patients in vivo | Models trained and tested on in vivo data outperformed those trained and tested on in vitro data by a large margin. When evaluated in vitro, the models trained in vivo performed considerably lower (0.70 ± 0.01; p < 0.01). Similarly, when assessed in vivo, in vitro-taught models had considerably reduced accuracy (0.61 ± 0.04; p < 0.05). | Holtkamp et al., (2021) [157] |
| Detection and classification of dental restorations in panoramic radiography | Cubic support vector machine algorithm with error-correcting output codes | 83 panoramic X-rays | Accuracy of 93.6% | Abdalla-Aslan et al., (2020) [158] |
8. AI Advantages in Medicine
9. AI Disadvantages and Limitations in Medicine
10. Discussion
10.1. Implications for Practice
10.2. Future Directions
10.3. Contribution to Literature and Limitations
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| 3CLpro | 3C-like protease |
| AD | Atopic dermatitis |
| AF | Atrial fibrillation |
| AI | Artificial intelligence |
| ANN | Artificial neural network |
| AUC | Area under the curve |
| CASNET | Causal associational network |
| CBCT | Cone-beam computed tomography |
| ChatGBT | Chat generative pre-trained transformer |
| CHIEF | Congestive heart failure treatment performance measure information extraction framework |
| CI | Confidence interval |
| CNN | Convolutional neural network |
| COVID-19 | Coronavirus disease 2019 |
| CRSwNP | Chronic rhinosinusitis with nasal polyps |
| CT | Computed tomography |
| CVD | Cardiovascular disease |
| DL | Deep learning |
| DNN | Deep neural network |
| ECG | Electrocardiogram |
| eCRSwNP | Eosinophilic chronic rhinosinusitis with nasal polyps |
| EF | Ejection fraction |
| EMR | Electronic medical record |
| FFR | Fractional flow reserve |
| GCG | Gyrocardiography |
| HF | Heart failure |
| HGAT | Heterogeneous graph attention |
| IVF | In vitro fertilization |
| LightGBM | Light gradient boosting machine |
| LS | Longitudinal strain |
| LV | Left ventricular |
| ML | Machine learning |
| MLP | Multilayer perceptron |
| MMTOP | Multiple models for missing values at time of prediction |
| MRI | Magnetic resonance imaging |
| NLP | Natural language processing |
| OCNet | Optimal channel networks |
| PCA | Principal component analysis |
| PCOS | Polycystic ovary syndrome |
| PNN | Probabilistic neural network |
| PPG | Photoplethysmography |
| PPT | Postprandial targeting |
| RBD | Receptor-binding domain |
| R-CNN | Region-based convolutional neural network |
| RNA | Ribonucleic acid |
| ROC | Receiver operating characteristic |
| RV | Right ventricular |
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
| SCG | Seismocardiography |
| SLE | Systemic lupus erythematosus |
| SNN | Simulated neural network |
| SVM | Support vector machine |
| TTE | Transthoracic echocardiography |
| VF | Ventricular fibrillation |
| VT | Ventricular tachycardia |
| XGBoost | Extreme gradient boosting |
References
- Zhang, C.; Lu, Y. Study on Artificial Intelligence: The State of the Art and Future Prospects. J. Ind. Inf. Integr. 2021, 23, 100224. [Google Scholar] [CrossRef]
- Muftić, F.; Kadunić, M.; Mušinbegović, A.; Almisreb, A.A. Exploring Medical Breakthroughs: A Systematic Review of ChatGPT Applications in Healthcare. Southeast Eur. J. Soft Comput. 2023, 12, 13–41. [Google Scholar] [CrossRef]
- Esteva, A.; Chou, K.; Yeung, S.; Naik, N.; Madani, A.; Mottaghi, A.; Liu, Y.; Topol, E.; Dean, J.; Socher, R. Deep Learning-Enabled Medical Computer Vision. npj Digit. Med. 2021, 4, 5. [Google Scholar] [CrossRef] [PubMed]
- Zeng, X.; Wang, F.; Luo, Y.; Kang, S.; Tang, J.; Lightstone, F.C.; Fang, E.F.; Cornell, W.; Nussinov, R.; Cheng, F. Deep Generative Molecular Design Reshapes Drug Discovery. Cell Rep. Med. 2022, 3, 100794. [Google Scholar] [CrossRef]
- Manickam, P.; Mariappan, S.A.; Murugesan, S.M.; Hansda, S.; Kaushik, A.; Shinde, R.; Thipperudraswamy, S.P. Artificial Intelligence (AI) and Internet of Medical Things (IoMT) Assisted Biomedical Systems for Intelligent Healthcare. Biosensors 2022, 12, 562. [Google Scholar] [CrossRef]
- Kulkarni, S.; Seneviratne, N.; Baig, M.S.; Khan, A.H.A. Artificial Intelligence in Medicine: Where Are We Now? Acad. Radiol. 2020, 27, 62–70. [Google Scholar] [CrossRef]
- Barragán-Montero, A.; Javaid, U.; Valdés, G.; Nguyen, D.; Desbordes, P.; Macq, B.; Willems, S.; Vandewinckele, L.; Holmström, M.; Löfman, F.; et al. Artificial Intelligence and Machine Learning for Medical Imaging: A Technology Review. Phys. Med. 2021, 83, 242–256. [Google Scholar] [CrossRef]
- Ali, N.M.; Shaheen, M.; Mabrouk, M.S.; Aborizka, M. Machine Learning-Based Models for Detection of Biomarkers of Autoimmune Diseases by Fragmentation and Analysis of MiRNA Sequences. Appl. Sci. 2022, 12, 5583. [Google Scholar] [CrossRef]
- Kang, J.; Hanif, M.; Mirza, E.; Khan, M.A.; Malik, M. Machine Learning in Primary Care: Potential to Improve Public Health. J. Med. Eng. Technol. 2021, 45, 75–80. [Google Scholar] [CrossRef]
- Khan, A.A.; Laghari, A.A.; Awan, S.A. Machine Learning in Computer Vision: A Review. EAI Endorsed Trans. Scalable Inf. Syst. 2021, 8, e4. [Google Scholar] [CrossRef]
- Murugesan, G.; Ahmed, T.I.; Bhola, J.; Shabaz, M.; Singla, J.; Rakhra, M.; More, S.; Samori, I.A. Fuzzy Logic-Based Systems for the Diagnosis of Chronic Kidney Disease. BioMed. Res. Int. 2022, 2022, e2653665. [Google Scholar] [CrossRef]
- Vlamou, E.; Papadopoulos, B. Fuzzy Logic Systems and Medical Applications. AIMS Neurosci. 2019, 6, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Saibene, A.; Assale, M.; Giltri, M. Expert Systems: Definitions, Advantages and Issues in Medical Field Applications. Expert Syst. Appl. 2021, 177, 114900. [Google Scholar] [CrossRef]
- Vrontis, D.; Christofi, M.; Pereira, V.; Tarba, S.; Makrides, A.; Trichina, E. Artificial Intelligence, Robotics, Advanced Technologies and Human Resource Management: A Systematic Review. Int. J. Hum. Resour. Manag. 2022, 33, 1237–1266. [Google Scholar] [CrossRef]
- Polling, M.; Li, C.; Cao, L.; Verbeek, F.; de Weger, L.A.; Belmonte, J.; De Linares, C.; Willemse, J.; de Boer, H.; Gravendeel, B. Neural Networks for Increased Accuracy of Allergenic Pollen Monitoring. Sci. Rep. 2021, 11, 11357. [Google Scholar] [CrossRef]
- Ghorbani, A.; Ouyang, D.; Abid, A.; He, B.; Chen, J.H.; Harrington, R.A.; Liang, D.H.; Ashley, E.A.; Zou, J.Y. Deep Learning Interpretation of Echocardiograms. npj Digit. Med. 2020, 3, 10. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.; Cai, Z.; Tan, C.-W.; Huang, Q.; Liu, H. Natural Language Processing (NLP) in Management Research: A Literature Review. J. Manag. Anal. 2020, 7, 139–172. [Google Scholar] [CrossRef]
- Khurana, D.; Koli, A.; Khatter, K.; Singh, S. Natural Language Processing: State of the Art, Current Trends and Challenges. Multimed. Tools Appl. 2023, 82, 3713–3744. [Google Scholar] [CrossRef]
- Moran, M.E. Evolution of Robotic Arms. J. Robot. Surg. 2007, 1, 103–111. [Google Scholar] [CrossRef]
- Kaul, V.; Enslin, S.; Gross, S.A. History of Artificial Intelligence in Medicine. Gastrointest. Endosc. 2020, 92, 807–812. [Google Scholar] [CrossRef]
- Kuipers, B.; Feigenbaum, E.A.; Hart, P.E.; Nilsson, N.J. Shakey: From Conception to History. AIMag 2017, 38, 88–103. [Google Scholar] [CrossRef]
- Kulikowski, C.A. Beginnings of Artificial Intelligence in Medicine (AIM): Computational Artifice Assisting Scientific Inquiry and Clinical Art—With Reflections on Present AIM Challenges. Yearb. Med. Inf. 2019, 28, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.J.; Bang, C.S. Application of Artificial Intelligence in Gastroenterology. World J. Gastroenterol. 2019, 25, 1666–1683. [Google Scholar] [CrossRef] [PubMed]
- Ferrucci, D.; Levas, A.; Bagchi, S.; Gondek, D.; Mueller, E.T. Watson: Beyond Jeopardy! Artif. Intell. 2013, 199–200, 93–105. [Google Scholar] [CrossRef]
- Bakkar, N.; Kovalik, T.; Lorenzini, I.; Spangler, S.; Lacoste, A.; Sponaugle, K.; Ferrante, P.; Argentinis, E.; Sattler, R.; Bowser, R. Artificial Intelligence in Neurodegenerative Disease Research: Use of IBM Watson to Identify Additional RNA-Binding Proteins Altered in Amyotrophic Lateral Sclerosis. Acta Neuropathol. 2018, 135, 227–247. [Google Scholar] [CrossRef]
- Comendador, B.E.V.; Francisco, B.M.B.; Medenilla, J.S.; Nacion, S.M.T.; Serac, T.B.E. Pharmabot: A Pediatric Generic Medicine Consultant Chatbot. J. Autom. Control. Eng. 2015, 3, 137–140. [Google Scholar] [CrossRef]
- Ni, L.; Lu, C.; Liu, N.; Liu, J. MANDY: Towards a Smart Primary Care Chatbot Application. In Knowledge and Systems Sciences, Proceedings of the Knowledge and Systems Sciences, Beijing, China, 11–12 June 2022; Chen, J., Theeramunkong, T., Supnithi, T., Tang, X., Eds.; Springer: Singapore, 2017; pp. 38–52. [Google Scholar]
- Rider, N.L.; Srinivasan, R.; Khoury, P. Artificial Intelligence and the Hunt for Immunological Disorders. Curr. Opin. Allergy Clin. Immunol. 2020, 20, 565–573. [Google Scholar] [CrossRef]
- Drummond, D. Between Competence and Warmth: The Remaining Place of the Physician in the Era of Artificial Intelligence. npj Digit. Med. 2021, 4, 85. [Google Scholar] [CrossRef]
- Gomes de Melo e Castro e Melo, J.A.; Faria Araújo, N.M. Impact of the Fourth Industrial Revolution on the Health Sector: A Qualitative Study. Healthc. Inf. Res. 2020, 26, 328–334. [Google Scholar] [CrossRef]
- Gonem, S.; Janssens, W.; Das, N.; Topalovic, M. Applications of Artificial Intelligence and Machine Learning in Respiratory Medicine. Thorax 2020, 75, 695–701. [Google Scholar] [CrossRef]
- Nayarisseri, A.; Khandelwal, R.; Tanwar, P.; Madhavi, M.; Sharma, D.; Thakur, G.; Speck-Planche, A.; Singh, S.K. Artificial Intelligence, Big Data and Machine Learning Approaches in Precision Medicine & Drug Discovery. Curr. Drug Targets 2021, 22, 631–655. [Google Scholar] [CrossRef] [PubMed]
- Saravi, B.; Hassel, F.; Ülkümen, S.; Zink, A.; Shavlokhova, V.; Couillard-Despres, S.; Boeker, M.; Obid, P.; Lang, G.M. Artificial Intelligence-Driven Prediction Modeling and Decision Making in Spine Surgery Using Hybrid Machine Learning Models. J. Pers. Med. 2022, 12, 509. [Google Scholar] [CrossRef] [PubMed]
- Si, T.; Bagchi, J.; Miranda, P.B.C. Artificial Neural Network Training Using Metaheuristics for Medical Data Classification: An Experimental Study. Expert Syst. Appl. 2022, 193, 116423. [Google Scholar] [CrossRef]
- Ramya, S.P.; Sumitha, B.; Ranjani, R.; Ahamed, M.A. A Comparative Study on Aspects Level Drug Reviews Using Back Propagation Neural Networks. In Proceedings of the 2022 3rd International Conference on Electronics and Sustainable Communication Systems (ICESC), Coimbatore, India, 17–19 August 2022; pp. 1341–1344. [Google Scholar]
- Van de Schoot, R.; Depaoli, S.; King, R.; Kramer, B.; Märtens, K.; Tadesse, M.G.; Vannucci, M.; Gelman, A.; Veen, D.; Willemsen, J.; et al. Bayesian Statistics and Modelling. Nat. Rev. Methods Prim. 2021, 1, 1. [Google Scholar] [CrossRef]
- Raita, Y.; Camargo, C.A.; Liang, L.; Hasegawa, K. Big Data, Data Science, and Causal Inference: A Primer for Clinicians. Front. Med. 2021, 8, 678047. [Google Scholar] [CrossRef]
- Sarvamangala, D.R.; Kulkarni, R.V. Convolutional Neural Networks in Medical Image Understanding: A Survey. Evol. Intell. 2022, 15, 1–22. [Google Scholar] [CrossRef]
- Malhotra, P.; Gupta, S.; Koundal, D.; Zaguia, A.; Enbeyle, W. Deep Neural Networks for Medical Image Segmentation. J. Healthc. Engin. 2022, 2022, 9580991. [Google Scholar] [CrossRef]
- Prediction Model of Hypertension Complications Based on GBDT and LightGBM—IOPscience. Available online: https://0-iopscience-iop-org.brum.beds.ac.uk/article/10.1088/1742-6596/1813/1/012008/meta (accessed on 16 February 2023).
- Li, X.-D.; Wang, J.-S.; Hao, W.-K.; Wang, M.; Zhang, M. Multi-Layer Perceptron Classification Method of Medical Data Based on Biogeography-Based Optimization Algorithm with Probability Distributions. Appl. Soft. Comput. 2022, 121, 108766. [Google Scholar] [CrossRef]
- Yuan, Y.; Huang, L.; Guo, J.; Zhang, C.; Chen, X.; Wang, J. OCNet: Object Context Network for Scene Parsing 2021. arXiv 2018, arXiv:1809.00916. [Google Scholar]
- Masegosa, A.R.; Cabañas, R.; Langseth, H.; Nielsen, T.D.; Salmerón, A. Probabilistic Models with Deep Neural Networks. Entropy 2021, 23, 117. [Google Scholar] [CrossRef]
- MacEachern, S.J.; Forkert, N.D. Machine Learning for Precision Medicine. Genome 2021, 64, 416–425. [Google Scholar] [CrossRef] [PubMed]
- Weerakody, P.B.; Wong, K.W.; Wang, G.; Ela, W. A Review of Irregular Time Series Data Handling with Gated Recurrent Neural Networks. Neurocomputing 2021, 441, 161–178. [Google Scholar] [CrossRef]
- Choi, B.W.; Kang, S.; Kim, H.W.; Kwon, O.D.; Vu, H.D.; Youn, S.W. Faster Region-Based Convolutional Neural Network in the Classification of Different Parkinsonism Patterns of the Striatum on Maximum Intensity Projection Images of [18F]FP-CIT Positron Emission Tomography. Diagnostics 2021, 11, 1557. [Google Scholar] [CrossRef]
- Cha, J.-Y.; Yoon, H.-I.; Yeo, I.-S.; Huh, K.-H.; Han, J.-S. Peri-Implant Bone Loss Measurement Using a Region-Based Convolutional Neural Network on Dental Periapical Radiographs. J. Clin. Med. 2021, 10, 1009. [Google Scholar] [CrossRef] [PubMed]
- K Faieq, A.; Mijwil, M. Prediction of of Heart Diseases Utilising Support Vector Machine and Artificial Neural Network. Indones. J. Electr. Eng. Comput. Sci. 2022, 26, 374–380. [Google Scholar] [CrossRef]
- Moore, A.; Bell, M. XGBoost, A Novel Explainable AI Technique, in the Prediction of Myocardial Infarction: A UK Biobank Cohort Study. Clin. Med. Insights Cardiol. 2022, 16, 11795468221133612. [Google Scholar] [CrossRef] [PubMed]
- Attia, Z.I.; Kapa, S.; Lopez-Jimenez, F.; McKie, P.M.; Ladewig, D.J.; Satam, G.; Pellikka, P.A.; Enriquez-Sarano, M.; Noseworthy, P.A.; Munger, T.M.; et al. Screening for Cardiac Contractile Dysfunction Using an Artificial Intelligence-Enabled Electrocardiogram. Nat. Med. 2019, 25, 70–74. [Google Scholar] [CrossRef]
- Lippi, G.; Sanchis-Gomar, F.; Cervellin, G. Global Epidemiology of Atrial Fibrillation: An Increasing Epidemic and Public Health Challenge. Int. J. Stroke 2021, 16, 217–221. [Google Scholar] [CrossRef]
- Wegner, F.K.; Plagwitz, L.; Doldi, F.; Ellermann, C.; Willy, K.; Wolfes, J.; Sandmann, S.; Varghese, J.; Eckardt, L. Machine Learning in the Detection and Management of Atrial Fibrillation. Clin. Res. Cardiol. 2022, 111, 1010–1017. [Google Scholar] [CrossRef]
- Zhang, X.; Gu, K.; Miao, S.; Zhang, X.; Yin, Y.; Wan, C.; Yu, Y.; Hu, J.; Wang, Z.; Shan, T.; et al. Automated Detection of Cardiovascular Disease by Electrocardiogram Signal Analysis: A Deep Learning System. Cardiovasc. Diagn. 2020, 10, 227–235. [Google Scholar] [CrossRef]
- AI Predicts Heart Disease Risk Using Single X-ray. Available online: https://press.rsna.org/timssnet/media/pressreleases/14_pr_target.cfm?id=2388 (accessed on 17 February 2023).
- Hamatani, Y.; Nishi, H.; Iguchi, M.; Esato, M.; Tsuji, H.; Wada, H.; Hasegawa, K.; Ogawa, H.; Abe, M.; Fukuda, S.; et al. Machine Learning Risk Prediction for Incident Heart Failure in Patients With Atrial Fibrillation. JACC Asia 2022, 2, 706–716. [Google Scholar] [CrossRef] [PubMed]
- Kee, O.T.; Harun, H.; Mustafa, N.; Abdul Murad, N.A.; Chin, S.F.; Jaafar, R.; Abdullah, N. Cardiovascular Complications in a Diabetes Prediction Model Using Machine Learning: A Systematic Review. Cardiovasc. Diabetol. 2023, 22, 13. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, M.T.; Nguyen, B.V.; Kim, K. Deep Feature Learning for Sudden Cardiac Arrest Detection in Automated External Defibrillators. Sci. Rep. 2018, 8, 17196. [Google Scholar] [CrossRef] [PubMed]
- Tison, G.H.; Sanchez, J.M.; Ballinger, B.; Singh, A.; Olgin, J.E.; Pletcher, M.J.; Vittinghoff, E.; Lee, E.S.; Fan, S.M.; Gladstone, R.A.; et al. Passive Detection of Atrial Fibrillation Using a Commercially Available Smartwatch. JAMA Cardiol. 2018, 3, 409–416. [Google Scholar] [CrossRef]
- Yang, C.; Aranoff, N.D.; Green, P.; Tavassolian, N. A Binary Classification of Cardiovascular Abnormality Using Time-Frequency Features of Cardio-Mechanical Signals. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 18–21 July 2018; pp. 5438–5441. [Google Scholar] [CrossRef]
- Wasserlauf, J.; You, C.; Patel, R.; Valys, A.; Albert, D.; Passman, R. Smartwatch Performance for the Detection and Quantification of Atrial Fibrillation. Circ. Arrhythm. Electrophysiol. 2019, 12, e006834. [Google Scholar] [CrossRef]
- Kusunose, K.; Abe, T.; Haga, A.; Fukuda, D.; Yamada, H.; Harada, M.; Sata, M. A Deep Learning Approach for Assessment of Regional Wall Motion Abnormality from Echocardiographic Images. JACC Cardiovasc. Imaging 2020, 13, 374–381. [Google Scholar] [CrossRef]
- Knackstedt, C.; Bekkers, S.C.A.M.; Schummers, G.; Schreckenberg, M.; Muraru, D.; Badano, L.P.; Franke, A.; Bavishi, C.; Omar, A.M.S.; Sengupta, P.P. Fully Automated Versus Standard Tracking of Left Ventricular Ejection Fraction and Longitudinal Strain: The FAST-EFs Multicenter Study. J. Am. Coll. Cardiol. 2015, 66, 1456–1466. [Google Scholar] [CrossRef]
- Itu, L.; Rapaka, S.; Passerini, T.; Georgescu, B.; Schwemmer, C.; Schoebinger, M.; Flohr, T.; Sharma, P.; Comaniciu, D. A Machine-Learning Approach for Computation of Fractional Flow Reserve from Coronary Computed Tomography. J. Appl. Physiol. 2016, 121, 42–52. [Google Scholar] [CrossRef]
- Zhang, J.; Gajjala, S.; Agrawal, P.; Tison, G.H.; Hallock, L.A.; Beussink-Nelson, L.; Lassen, M.H.; Fan, E.; Aras, M.A.; Jordan, C.; et al. Fully Automated Echocardiogram Interpretation in Clinical Practice. Circulation 2018, 138, 1623–1635. [Google Scholar] [CrossRef]
- Retson, T.A.; Masutani, E.M.; Golden, D.; Hsiao, A. Clinical Performance and Role of Expert Supervision of Deep Learning for Cardiac Ventricular Volumetry: A Validation Study. Radiol. Artif. Intell. 2020, 2, e190064. [Google Scholar] [CrossRef]
- Alzubaidi, L.; Zhang, J.; Humaidi, A.J.; Al-Dujaili, A.; Duan, Y.; Al-Shamma, O.; Santamaría, J.; Fadhel, M.A.; Al-Amidie, M.; Farhan, L. Review of Deep Learning: Concepts, CNN Architectures, Challenges, Applications, Future Directions. J. Big Data 2021, 8, 53. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Luo, J.; Hao, S.; Xu, H.; Shin, A.Y.; Jin, B.; Liu, R.; Deng, X.; Wang, L.; Zheng, L.; et al. NLP Based Congestive Heart Failure Case Finding: A Prospective Analysis on Statewide Electronic Medical Records. Int. J. Med. Inf. 2015, 84, 1039–1047. [Google Scholar] [CrossRef] [PubMed]
- Meystre, S.M.; Kim, Y.; Gobbel, G.T.; Matheny, M.E.; Redd, A.; Bray, B.E.; Garvin, J.H. Congestive Heart Failure Information Extraction Framework for Automated Treatment Performance Measures Assessment. J. Am. Med. Inf. Assoc. 2017, 24, e40–e46. [Google Scholar] [CrossRef]
- Ye, C.; Fu, T.; Hao, S.; Zhang, Y.; Wang, O.; Jin, B.; Xia, M.; Liu, M.; Zhou, X.; Wu, Q.; et al. Prediction of Incident Hypertension Within the Next Year: Prospective Study Using Statewide Electronic Health Records and Machine Learning. J. Med. Internet Res. 2018, 20, e22. [Google Scholar] [CrossRef]
- Samad, M.D.; Ulloa, A.; Wehner, G.J.; Jing, L.; Hartzel, D.; Good, C.W.; Williams, B.A.; Haggerty, C.M.; Fornwalt, B.K. Predicting Survival From Large Echocardiography and Electronic Health Record Datasets: Optimization With Machine Learning. JACC Cardiovasc. Imaging 2019, 12, 681–689. [Google Scholar] [CrossRef]
- Kwon, J.-M.; Kim, K.-H.; Jeon, K.-H.; Park, J. Deep Learning for Predicting In-Hospital Mortality among Heart Disease Patients Based on Echocardiography. Echocardiography 2019, 36, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Hutchens, R.; Hung, J.; Bennamoun, M.; McQuillan, B.; Briffa, T.; Sohel, F.; Murray, K.; Stewart, J.; Chow, B.; et al. Performance of Multilabel Machine Learning Models and Risk Stratification Schemas for Predicting Stroke and Bleeding Risk in Patients with Non-Valvular Atrial Fibrillation. Comput. Biol. Med. 2022, 150, 106126. [Google Scholar] [CrossRef] [PubMed]
- Steele, A.J.; Denaxas, S.C.; Shah, A.D.; Hemingway, H.; Luscombe, N.M. Machine Learning Models in Electronic Health Records Can Outperform Conventional Survival Models for Predicting Patient Mortality in Coronary Artery Disease. PLoS ONE 2018, 13, e0202344. [Google Scholar] [CrossRef]
- Chi, C.-L.; Wang, J.; Ying Yew, P.; Lenskaia, T.; Loth, M.; Mani Pradhan, P.; Liang, Y.; Kurella, P.; Mehta, R.; Robinson, J.G.; et al. Producing Personalized Statin Treatment Plans to Optimize Clinical Outcomes Using Big Data and Machine Learning. J. Biomed. Inf. 2022, 128, 104029. [Google Scholar] [CrossRef]
- Malizia, V.; Cilluffo, G.; Fasola, S.; Ferrante, G.; Landi, M.; Montalbano, L.; Licari, A.; La Grutta, S. Endotyping Allergic Rhinitis in Children: A Machine Learning Approach. Pediatr. Allergy Immunol. 2022, 33 (Suppl. S27), 18–21. [Google Scholar] [CrossRef]
- Yang, J.; Zhang, M.; Liu, P.; Yu, S. Multi-Label Rhinitis Prediction Using Ensemble Neural Network Chain with Pre-Training. Appl. Soft Comput. 2022, 122, 108839. [Google Scholar] [CrossRef]
- Bhardwaj, P.; Tyagi, A.; Tyagi, S.; Antão, J.; Deng, Q. Machine Learning Model for Classification of Predominantly Allergic and Non-Allergic Asthma among Preschool Children with Asthma Hospitalization. J. Asthma 2023, 60, 487–495. [Google Scholar] [CrossRef] [PubMed]
- Van Breugel, M.; Qi, C.; Xu, Z.; Pedersen, C.-E.T.; Petoukhov, I.; Vonk, J.M.; Gehring, U.; Berg, M.; Bügel, M.; Carpaij, O.A.; et al. Nasal DNA Methylation at Three CpG Sites Predicts Childhood Allergic Disease. Nat. Commun. 2022, 13, 7415. [Google Scholar] [CrossRef]
- Proper, S.P.; Azouz, N.P.; Mersha, T.B. Achieving Precision Medicine in Allergic Disease: Progress and Challenges. Front. Immunol. 2021, 12, 720746. [Google Scholar] [CrossRef]
- Wu, C.; Lu, P.; Xu, F.; Duan, J.; Hua, X.; Shabaz, M. The Prediction Models of Anaphylactic Disease. Inf. Med. Unlocked 2021, 24, 100535. [Google Scholar] [CrossRef]
- Khoury, P.; Srinivasan, R.; Kakumanu, S.; Ochoa, S.; Keswani, A.; Sparks, R.; Rider, N.L. A Framework for Augmented Intelligence in Allergy and Immunology Practice and Research-A Work Group Report of the AAAAI Health Informatics, Technology, and Education Committee. J. Allergy Clin. Immunol. Pract. 2022, 10, 1178–1188. [Google Scholar] [CrossRef] [PubMed]
- Ridolo, E.; Incorvaia, C.; Heffler, E.; Cavaliere, C.; Paoletti, G.; Canonica, G.W. The Present and Future of Allergen Immunotherapy in Personalized Medicine. J. Pers. Med. 2022, 12, 774. [Google Scholar] [CrossRef]
- Wild, C.P. Complementing the Genome with an “Exposome”: The Outstanding Challenge of Environmental Exposure Measurement in Molecular Epidemiology. Cancer Epidemiol. Biomark. Prev. 2005, 14, 1847–1850. [Google Scholar] [CrossRef]
- Tunyasuvunakool, K.; Adler, J.; Wu, Z.; Green, T.; Zielinski, M.; Žídek, A.; Bridgland, A.; Cowie, A.; Meyer, C.; Laydon, A.; et al. Highly Accurate Protein Structure Prediction for the Human Proteome. Nature 2021, 596, 590–596. [Google Scholar] [CrossRef]
- Olsson, O.; Karlsson, M.; Persson, A.S.; Smith, H.G.; Varadarajan, V.; Yourstone, J.; Stjernman, M. Efficient, Automated and Robust Pollen Analysis Using Deep Learning. Methods Ecol. Evol. 2021, 12, 850–862. [Google Scholar] [CrossRef]
- Samonte, M.J.; Sunga, C.F.; Samonte, D. AlleRT: Food Recommender Web Application with Allergy Filtration. In Proceedings of the 5th European International Conference on Industrial Engineering and Operations Management, Rome, Italy, 26–28 July 2022. [Google Scholar]
- Joumaa, H.; Sigogne, R.; Maravic, M.; Perray, L.; Bourdin, A.; Roche, N. Artificial Intelligence to Differentiate Asthma from COPD in Medico-Administrative Databases. BMC Pulm. Med. 2022, 22, 357. [Google Scholar] [CrossRef] [PubMed]
- Hurst, J.H.; Zhao, C.; Hostetler, H.P.; Ghiasi Gorveh, M.; Lang, J.E.; Goldstein, B.A. Environmental and Clinical Data Utility in Pediatric Asthma Exacerbation Risk Prediction Models. BMC Med. Inf. Decis. Mak. 2022, 22, 108. [Google Scholar] [CrossRef] [PubMed]
- Guimarães, P.; Batista, A.; Zieger, M.; Kaatz, M.; Koenig, K. Artificial Intelligence in Multiphoton Tomography: Atopic Dermatitis Diagnosis. Sci. Rep. 2020, 10, 7968. [Google Scholar] [CrossRef] [PubMed]
- Hurault, G.; Domínguez-Hüttinger, E.; Langan, S.M.; Williams, H.C.; Tanaka, R.J. Personalized Prediction of Daily Eczema Severity Scores Using a Mechanistic Machine Learning Model. Clin. Exp. Allergy 2020, 50, 1258–1266. [Google Scholar] [CrossRef] [PubMed]
- Maintz, L.; Welchowski, T.; Herrmann, N.; Brauer, J.; Kläschen, A.S.; Fimmers, R.; Schmid, M.; Bieber, T.; CK-CARE Study Group; Schmid-Grendelmeier, P.; et al. Machine Learning-Based Deep Phenotyping of Atopic Dermatitis: Severity-Associated Factors in Adolescent and Adult Patients. JAMA Derm. 2021, 157, 1414–1424. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Fan, W.; Qin, D.; Liu, P.; Gao, Z.; Lv, H.; Zhang, W.; Xiang, R.; Xu, Y. Development, Validation and Comparison of Artificial Neural Network and Logistic Regression Models Predicting Eosinophilic Chronic Rhinosinusitis with Nasal Polyps. Allergy Asthma Immunol. Res. 2023, 15, 67–82. [Google Scholar] [CrossRef] [PubMed]
- Moreno, E.M.; Moreno, V.; Laffond, E.; Gracia-Bara, M.T.; Muñoz-Bellido, F.J.; Macías, E.M.; Curto, B.; Campanon, M.V.; de Arriba, S.; Martin, C.; et al. Usefulness of an Artificial Neural Network in the Prediction of β-Lactam Allergy. J. Allergy Clin. Immunol. Pract. 2020, 8, 2974–2982.e1. [Google Scholar] [CrossRef]
- Ramisetty, K.; Christopher, J.; Panda, S.; Lazarus, Y. Machine Learning and XAI Approaches for Allergy Diagnosis. Biomed. Signal Process Control 2021, 69, 102681. [Google Scholar] [CrossRef]
- Jorge, A.; Castro, V.M.; Barnado, A.; Gainer, V.; Hong, C.; Cai, T.; Cai, T.; Carroll, R.; Denny, J.C.; Crofford, L.; et al. Identifying Lupus Patients in Electronic Health Records: Development and Validation of Machine Learning Algorithms and Application of Rule-Based Algorithms. Semin. Arthritis Rheum. 2019, 49, 84–90. [Google Scholar] [CrossRef]
- Zhou, Y.; Wang, M.; Zhao, S.; Yan, Y. Machine Learning for Diagnosis of Systemic Lupus Erythematosus: A Systematic Review and Meta-Analysis. Comput. Intell. Neurosci. 2022, 2022, 7167066. [Google Scholar] [CrossRef]
- Ma, Y.; Chen, J.; Wang, T.; Zhang, L.; Xu, X.; Qiu, Y.; Xiang, A.P.; Huang, W. Accurate Machine Learning Model to Diagnose Chronic Autoimmune Diseases Utilizing Information From B Cells and Monocytes. Front. Immunol. 2022, 13, 870531. [Google Scholar] [CrossRef]
- Li, Y.; Ma, C.; Liao, S.; Qi, S.; Meng, S.; Cai, W.; Dai, W.; Cao, R.; Dong, X.; Krämer, B.K.; et al. Combined Proteomics and Single Cell RNA-Sequencing Analysis to Identify Biomarkers of Disease Diagnosis and Disease Exacerbation for Systemic Lupus Erythematosus. Front. Immunol. 2022, 13, 969509. [Google Scholar] [CrossRef] [PubMed]
- Martin-Gutierrez, L.; Peng, J.; Thompson, N.L.; Robinson, G.A.; Naja, M.; Peckham, H.; Wu, W.; J’bari, H.; Ahwireng, N.; Waddington, K.E.; et al. Stratification of Patients With Sjögren’s Syndrome and Patients With Systemic Lupus Erythematosus According to Two Shared Immune Cell Signatures, With Potential Therapeutic Implications. Arthritis Rheumatol. 2021, 73, 1626–1637. [Google Scholar] [CrossRef] [PubMed]
- Mo, X.; Chen, X.; Ieong, C.; Zhang, S.; Li, H.; Li, J.; Lin, G.; Sun, G.; He, F.; He, Y.; et al. Early Prediction of Clinical Response to Etanercept Treatment in Juvenile Idiopathic Arthritis Using Machine Learning. Front. Pharm. 2020, 11, 1164. [Google Scholar] [CrossRef] [PubMed]
- Zeng, X.; Zhu, S.; Lu, W.; Liu, Z.; Huang, J.; Zhou, Y.; Fang, J.; Huang, Y.; Guo, H.; Li, L.; et al. Target Identification among Known Drugs by Deep Learning from Heterogeneous Networks. Chem. Sci. 2020, 11, 1775–1797. [Google Scholar] [CrossRef]
- Madhukar, N.S.; Khade, P.K.; Huang, L.; Gayvert, K.; Galletti, G.; Stogniew, M.; Allen, J.E.; Giannakakou, P.; Elemento, O. A Bayesian Machine Learning Approach for Drug Target Identification Using Diverse Data Types. Nat. Commun. 2019, 10, 5221. [Google Scholar] [CrossRef] [PubMed]
- Bukhari, S.N.H.; Webber, J.; Mehbodniya, A. Decision Tree Based Ensemble Machine Learning Model for the Prediction of Zika Virus T-Cell Epitopes as Potential Vaccine Candidates. Sci. Rep. 2022, 12, 7810. [Google Scholar] [CrossRef]
- Anantpadma, M.; Lane, T.; Zorn, K.M.; Lingerfelt, M.A.; Clark, A.M.; Freundlich, J.S.; Davey, R.A.; Madrid, P.B.; Ekins, S. Ebola Virus Bayesian Machine Learning Models Enable New in Vitro Leads. ACS Omega 2019, 4, 2353–2361. [Google Scholar] [CrossRef]
- Crooke, S.N.; Ovsyannikova, I.G.; Kennedy, R.B.; Poland, G.A. Immunoinformatic Identification of B Cell and T Cell Epitopes in the SARS-CoV-2 Proteome. Sci. Rep. 2020, 10, 14179. [Google Scholar] [CrossRef]
- Abbasi, B.A.; Saraf, D.; Sharma, T.; Sinha, R.; Singh, S.; Sood, S.; Gupta, P.; Gupta, A.; Mishra, K.; Kumari, P.; et al. Identification of Vaccine Targets & Design of Vaccine against SARS-CoV-2 Coronavirus Using Computational and Deep Learning-Based Approaches. PeerJ 2022, 10, e13380. [Google Scholar] [CrossRef]
- Nambiar, A.; Liu, S.; Heflin, M.; Forsyth, J.M.; Maslov, S.; Hopkins, M.; Ritz, A. Transformer Neural Networks for Protein Family and Interaction Prediction Tasks. J. Comput. Biol. 2023, 30, 95–111. [Google Scholar] [CrossRef] [PubMed]
- Pesciullesi, G.; Schwaller, P.; Laino, T.; Reymond, J.-L. Transfer Learning Enables the Molecular Transformer to Predict Regio- and Stereoselective Reactions on Carbohydrates. Nat. Commun. 2020, 11, 4874. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.-T.; Zhang, J.-S.; Zhang, H.-H.; Nan, Y.-D.; Zhao, Y.; Fu, E.-Q.; Xie, Y.-H.; Liu, W.; Li, W.-P.; Zhang, H.-J.; et al. Automated Detection and Quantification of COVID-19 Pneumonia: CT Imaging Analysis by a Deep Learning-Based Software. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 2525–2532. [Google Scholar] [CrossRef] [PubMed]
- Mohanty, S.; Harun Ai Rashid, M.; Mridul, M.; Mohanty, C.; Swayamsiddha, S. Application of Artificial Intelligence in COVID-19 Drug Repurposing. Diabetes Metab. Syndr. 2020, 14, 1027–1031. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.-R.; Lu, L.; Zhang, J.-Y.; Huo, T.-T.; Liu, S.-X.; Ye, Z.-W. Application of Artificial Intelligence in Medicine: An Overview. Curr. Med. Sci. 2021, 41, 1105–1115. [Google Scholar] [CrossRef] [PubMed]
- Stebbing, J.; Krishnan, V.; de Bono, S.; Ottaviani, S.; Casalini, G.; Richardson, P.J.; Monteil, V.; Lauschke, V.M.; Mirazimi, A.; Youhanna, S.; et al. Mechanism of Baricitinib Supports Artificial Intelligence-Predicted Testing in COVID-19 Patients. EMBO Mol. Med. 2020, 12, e12697. [Google Scholar] [CrossRef]
- Chen, J.; Wang, R.; Gilby, N.B.; Wei, G.-W. Omicron Variant (B.1.1.529): Infectivity, Vaccine Breakthrough, and Antibody Resistance. J. Chem. Inf. Model 2022, 62, 412–422. [Google Scholar] [CrossRef]
- Lopez-Rincon, A.; Tonda, A.; Mendoza-Maldonado, L.; Mulders, D.G.J.C.; Molenkamp, R.; Perez-Romero, C.A.; Claassen, E.; Garssen, J.; Kraneveld, A.D. Classification and Specific Primer Design for Accurate Detection of SARS-CoV-2 Using Deep Learning. Sci. Rep. 2021, 11, 947. [Google Scholar] [CrossRef]
- Abdel-Basset, M.; Hawash, H.; Elhoseny, M.; Chakrabortty, R.K.; Ryan, M. DeepH-DTA: Deep Learning for Predicting Drug-Target Interactions: A Case Study of COVID-19 Drug Repurposing. IEEE Access 2020, 8, 170433–170451. [Google Scholar] [CrossRef]
- Beck, B.R.; Shin, B.; Choi, Y.; Park, S.; Kang, K. Predicting Commercially Available Antiviral Drugs That May Act on the Novel Coronavirus (SARS-CoV-2) through a Drug-Target Interaction Deep Learning Model. Comput. Struct. Biotechnol. J. 2020, 18, 784–790. [Google Scholar] [CrossRef]
- Gao, K.; Nguyen, D.D.; Wang, R.; Wei, G.-W. Machine Intelligence Design of 2019-NCoV Drugs. bioRxiv 2020. [Google Scholar] [CrossRef]
- Hofmarcher, M.; Mayr, A.; Rumetshofer, E.; Ruch, P.; Renz, P.; Schimunek, J.; Seidl, P.; Vall, A.; Widrich, M.; Hochreiter, S.; et al. Large-Scale Ligand-Based Virtual Screening for SARS-CoV-2 Inhibitors Using Deep Neural Networks. arXiv 2020, arXiv:2004.00979v3. [Google Scholar] [CrossRef]
- Tang, B.; He, F.; Liu, D.; Fang, M.; Wu, Z.; Xu, D. AI-Aided Design of Novel Targeted Covalent Inhibitors against SARS-CoV-2. Biomolecules 2022, 12, 746. [Google Scholar] [CrossRef] [PubMed]
- Zhavoronkov, A.; Aladinskiy, V.; Zhebrak, A.; Zagribelnyy, B.; Terentiev, V.; Bezrukov, D.S.; Polykovskiy, D.; Shayakhmetov, R.; Filimonov, A.; Orekhov, P.; et al. Potential COVID-2019 3C-like Protease Inhibitors Designed Using Generative Deep Learning Approaches. ChemRxiv 2020. [Google Scholar] [CrossRef]
- Abdelmageed, M.I.; Abdelmoneim, A.H.; Mustafa, M.I.; Elfadol, N.M.; Murshed, N.S.; Shantier, S.W.; Makhawi, A.M. Design of a Multiepitope-Based Peptide Vaccine against the E Protein of Human COVID-19: An Immunoinformatics Approach. Biomed. Res. Int. 2020, 2020, 2683286. [Google Scholar] [CrossRef]
- Fast, E.; Altman, R.B.; Chen, B. Potential T-Cell and B-Cell Epitopes of 2019-NCoV. bioRxiv 2020. [Google Scholar] [CrossRef]
- Ong, E.; Wong, M.U.; Huffman, A.; He, Y. COVID-19 Coronavirus Vaccine Design Using Reverse Vaccinology and Machine Learning. bioRxiv 2020. [Google Scholar] [CrossRef]
- Russo, G.; Di Salvatore, V.; Sgroi, G.; Parasiliti Palumbo, G.A.; Reche, P.A.; Pappalardo, F. A Multi-Step and Multi-Scale Bioinformatic Protocol to Investigate Potential SARS-CoV-2 Vaccine Targets. Brief Bioinform. 2022, 23, bbab403. [Google Scholar] [CrossRef]
- Sarkar, B.; Ullah, M.A.; Johora, F.T.; Taniya, M.A.; Araf, Y. The Essential Facts of Wuhan Novel Coronavirus Outbreak in China and Epitope-Based Vaccine Designing against COVID-19. bioRxiv 2020. [Google Scholar] [CrossRef]
- Susithra Priyadarshni, M.; Isaac Kirubakaran, S.; Harish, M.C. In Silico Approach to Design a Multi-Epitopic Vaccine Candidate Targeting the Non-Mutational Immunogenic Regions in Envelope Protein and Surface Glycoprotein of SARS-CoV-2. J. Biomol. Struct. Dyn. 2022, 40, 12948–12963. [Google Scholar] [CrossRef]
- Zhang, M.; Flores, K.B.; Tran, H.T. Deep Learning and Regression Approaches to Forecasting Blood Glucose Levels for Type 1 Diabetes. Biomed. Signal Process. Control 2021, 69, 102923. [Google Scholar] [CrossRef]
- Mujahid, O.; Contreras, I.; Vehi, J. Machine Learning Techniques for Hypoglycemia Prediction: Trends and Challenges. Sensors 2021, 21, 546. [Google Scholar] [CrossRef]
- Ma, S.; Schreiner, P.J.; Seaquist, E.R.; Ugurbil, M.; Zmora, R.; Chow, L.S. Multiple Predictively Equivalent Risk Models for Handling Missing Data at Time of Prediction: With an Application in Severe Hypoglycemia Risk Prediction for Type 2 Diabetes. J. Biomed. Inf. 2020, 103, 103379. [Google Scholar] [CrossRef] [PubMed]
- Faruqui, S.H.A.; Du, Y.; Meka, R.; Alaeddini, A.; Li, C.; Shirinkam, S.; Wang, J. Development of a Deep Learning Model for Dynamic Forecasting of Blood Glucose Level for Type 2 Diabetes Mellitus: Secondary Analysis of a Randomized Controlled Trial. JMIR Mhealth Uhealth 2019, 7, e14452. [Google Scholar] [CrossRef]
- Wu, Y.-T.; Zhang, C.-J.; Mol, B.W.; Kawai, A.; Li, C.; Chen, L.; Wang, Y.; Sheng, J.-Z.; Fan, J.-X.; Shi, Y.; et al. Early Prediction of Gestational Diabetes Mellitus in the Chinese Population via Advanced Machine Learning. J. Clin. Endocrinol. Metab. 2021, 106, e1191–e1205. [Google Scholar] [CrossRef] [PubMed]
- Lin, Z.; Feng, W.; Liu, Y.; Ma, C.; Arefan, D.; Zhou, D.; Cheng, X.; Yu, J.; Gao, L.; Du, L.; et al. Machine Learning to Identify Metabolic Subtypes of Obesity: A Multi-Center Study. Front. Endocrinol. 2021, 12, 713592. [Google Scholar] [CrossRef]
- Rein, M.; Ben-Yacov, O.; Godneva, A.; Shilo, S.; Zmora, N.; Kolobkov, D.; Cohen-Dolev, N.; Wolf, B.-C.; Kosower, N.; Lotan-Pompan, M.; et al. Effects of Personalized Diets by Prediction of Glycemic Responses on Glycemic Control and Metabolic Health in Newly Diagnosed T2DM: A Randomized Dietary Intervention Pilot Trial. BMC Med. 2022, 20, 56. [Google Scholar] [CrossRef]
- Yang, J.; Shi, X.; Wang, B.; Qiu, W.; Tian, G.; Wang, X.; Wang, P.; Yang, J. Ultrasound Image Classification of Thyroid Nodules Based on Deep Learning. Front. Oncol. 2022, 12, 905955. [Google Scholar] [CrossRef]
- Islam, S.S.; Haque, M.S.; Miah, M.S.U.; Sarwar, T.B.; Nugraha, R. Application of Machine Learning Algorithms to Predict the Thyroid Disease Risk: An Experimental Comparative Study. PeerJ Comput. Sci. 2022, 8, e898. [Google Scholar] [CrossRef]
- Ndefo, U.A.; Eaton, A.; Green, M.R. Polycystic Ovary Syndrome: A Review of Treatment Options with a Focus on Pharmacological Approaches. P T 2013, 38, 336–355. [Google Scholar]
- Azziz, R. Polycystic Ovary Syndrome. Obs. Gynecol. 2018, 132, 321–336. [Google Scholar] [CrossRef] [PubMed]
- Ni, C.-M.; Huang, W.-L.; Jiang, Y.-M.; Xu, J.; Duan, R.; Zhu, Y.-L.; Zhu, X.-P.; Fan, X.-M.; Luo, G.-A.; Wang, Y.-M.; et al. Improving the Accuracy and Efficacy of Diagnosing Polycystic Ovary Syndrome by Integrating Metabolomics with Clinical Characteristics: Study Protocol for a Randomized Controlled Trial. Trials 2020, 21, 169. [Google Scholar] [CrossRef]
- Suha, S.A.; Islam, M.N. An Extended Machine Learning Technique for Polycystic Ovary Syndrome Detection Using Ovary Ultrasound Image. Sci. Rep. 2022, 12, 17123. [Google Scholar] [CrossRef] [PubMed]
- Zigarelli, A.; Jia, Z.; Lee, H. Machine-Aided Self-Diagnostic Prediction Models for Polycystic Ovary Syndrome: Observational Study. JMIR Res. 2022, 6, e29967. [Google Scholar] [CrossRef] [PubMed]
- Ding, T.; Ren, W.; Wang, T.; Han, Y.; Ma, W.; Wang, M.; Fu, F.; Li, Y.; Wang, S. Assessment and Quantification of Ovarian Reserve on the Basis of Machine Learning Models. Front. Endocrinol. 2023, 14, 1087429. [Google Scholar] [CrossRef]
- Yu, J.-L.; Su, Y.-F.; Zhang, C.; Jin, L.; Lin, X.-H.; Chen, L.-T.; Huang, H.-F.; Wu, Y.-T. Tracking of Menstrual Cycles and Prediction of the Fertile Window via Measurements of Basal Body Temperature and Heart Rate as Well as Machine-Learning Algorithms. Reprod. Biol. Endocrinol. 2022, 20, 118. [Google Scholar] [CrossRef]
- Bormann, C.L.; Kanakasabapathy, M.K.; Thirumalaraju, P.; Gupta, R.; Pooniwala, R.; Kandula, H.; Hariton, E.; Souter, I.; Dimitriadis, I.; Ramirez, L.B.; et al. Performance of a Deep Learning Based Neural Network in the Selection of Human Blastocysts for Implantation. eLife 2020, 9, e55301. [Google Scholar] [CrossRef]
- Louis, C.M.; Handayani, N.; Aprilliana, T.; Polim, A.A.; Boediono, A.; Sini, I. Genetic Algorithm-Assisted Machine Learning for Clinical Pregnancy Prediction in in Vitro Fertilization. AJOG Glob. Rep. 2023, 3, 100133. [Google Scholar] [CrossRef]
- Ameli, N.; Gibson, M.P.; Khanna, A.; Howey, M.; Lai, H. An Application of Machine Learning Techniques to Analyze Patient Information to Improve Oral Health Outcomes. Front. Dent. Med. 2022, 3, 833191. [Google Scholar] [CrossRef]
- Kühnisch, J.; Meyer, O.; Hesenius, M.; Hickel, R.; Gruhn, V. Caries Detection on Intraoral Images Using Artificial Intelligence. J. Dent. Res. 2022, 101, 158–165. [Google Scholar] [CrossRef]
- Schwendicke, F.; Rossi, J.G.; Göstemeyer, G.; Elhennawy, K.; Cantu, A.G.; Gaudin, R.; Chaurasia, A.; Gehrung, S.; Krois, J. Cost-Effectiveness of Artificial Intelligence for Proximal Caries Detection. J. Dent. Res. 2021, 100, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, P.; Nikhade, P. Artificial Intelligence in Dentistry: Past, Present, and Future. Cureus 2022, 14, e27405. [Google Scholar] [CrossRef] [PubMed]
- Mohammad-Rahimi, H.; Motamedian, S.R.; Rohban, M.H.; Krois, J.; Uribe, S.E.; Mahmoudinia, E.; Rokhshad, R.; Nadimi, M.; Schwendicke, F. Deep Learning for Caries Detection: A Systematic Review. J. Dent. 2022, 122, 104115. [Google Scholar] [CrossRef] [PubMed]
- Kositbowornchai, S.; Siriteptawee, S.; Plermkamon, S.; Bureerat, S.; Chetchotsak, D. An Artificial Neural Network for Detection of Simulated Dental Caries. Int. J. Comput. Assist. Radiol. Surg. 2006, 2, 91–96. [Google Scholar] [CrossRef]
- Patil, S.; Kulkarni, V.; Bhise, A. Algorithmic Analysis for Dental Caries Detection Using an Adaptive Neural Network Architecture. Heliyon 2019, 5, e01579. [Google Scholar] [CrossRef]
- Casalegno, F.; Newton, T.; Daher, R.; Abdelaziz, M.; Lodi-Rizzini, A.; Schürmann, F.; Krejci, I.; Markram, H. Caries Detection with Near-Infrared Transillumination Using Deep Learning. J. Dent. Res. 2019, 98, 1227–1233. [Google Scholar] [CrossRef]
- Hung, M.; Voss, M.W.; Rosales, M.N.; Li, W.; Su, W.; Xu, J.; Bounsanga, J.; Ruiz-Negrón, B.; Lauren, E.; Licari, F.W. Application of Machine Learning for Diagnostic Prediction of Root Caries. Gerodontology 2019, 36, 395–404. [Google Scholar] [CrossRef]
- Javed, S.; Zakirulla, M.; Baig, R.U.; Asif, S.M.; Meer, A.B. Development of Artificial Neural Network Model for Prediction of Post-Streptococcus Mutans in Dental Caries. Comput. Methods Programs Biomed. 2020, 186, 105198. [Google Scholar] [CrossRef]
- Geetha, V.; Aprameya, K.S.; Hinduja, D.M. Dental Caries Diagnosis in Digital Radiographs Using Back-Propagation Neural Network. Health Inf. Sci. Syst. 2020, 8, 8. [Google Scholar] [CrossRef]
- Bayraktar, Y.; Ayan, E. Diagnosis of Interproximal Caries Lesions with Deep Convolutional Neural Network in Digital Bitewing Radiographs. Clin. Oral Investig. 2022, 26, 623–632. [Google Scholar] [CrossRef]
- Holtkamp, A.; Elhennawy, K.; Cejudo Grano de Oro, J.E.; Krois, J.; Paris, S.; Schwendicke, F. Generalizability of Deep Learning Models for Caries Detection in Near-Infrared Light Transillumination Images. J. Clin. Med. 2021, 10, 961. [Google Scholar] [CrossRef]
- Abdalla-Aslan, R.; Yeshua, T.; Kabla, D.; Leichter, I.; Nadler, C. An Artificial Intelligence System Using Machine-Learning for Automatic Detection and Classification of Dental Restorations in Panoramic Radiography. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2020, 130, 593–602. [Google Scholar] [CrossRef] [PubMed]
- Krois, J.; Ekert, T.; Meinhold, L.; Golla, T.; Kharbot, B.; Wittemeier, A.; Dörfer, C.; Schwendicke, F. Deep Learning for the Radiographic Detection of Periodontal Bone Loss. Sci. Rep. 2019, 9, 8495. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.-H.; Kim, S.; Kim, H.-J.; Jeong, H.-O.; Lee, J.; Jang, J.; Joo, J.-Y.; Shin, Y.; Kang, J.; Park, A.K.; et al. Prediction of Chronic Periodontitis Severity Using Machine Learning Models Based On Salivary Bacterial Copy Number. Front. Cell Infect. Microbiol. 2020, 10, 571515. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.; Wu, J.; Mao, Y.; Zhu, S.; Huang, G.F.; Petritis, B.; Huang, R.-P. Developing a Periodontal Disease Antibody Array for the Prediction of Severe Periodontal Disease Using Machine Learning Classifiers. J. Periodontol. 2020, 91, 232–243. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-H.; Kim, D.-H.; Jeong, S.-N.; Choi, S.-H. Diagnosis and Prediction of Periodontally Compromised Teeth Using a Deep Learning-Based Convolutional Neural Network Algorithm. J. Periodontal. Implant. Sci. 2018, 48, 114–123. [Google Scholar] [CrossRef]
- Yauney, G.; Rana, A.; Wong, L.; Javia, P.; Muftu, A. Automated Process Incorporating Machine Learning Segmentation and Correlation of Oral Diseases with Systemic Health. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; IEEE: Piscataway, NJ, USA, 2019; pp. 3387–3393. [Google Scholar]
- Troiano, G.; Nibali, L.; Petsos, H.; Eickholz, P.; Saleh, M.H.A.; Santamaria, P.; Jian, J.; Shi, S.; Meng, H.; Zhurakivska, K.; et al. Development and International Validation of Logistic Regression and Machine-Learning Models for the Prediction of 10-Year Molar Loss. J. Clin. Periodontol. 2023, 50, 348–357. [Google Scholar] [CrossRef]
- Papantonopoulos, G.; Takahashi, K.; Bountis, T.; Loos, B.G. Artificial Neural Networks for the Diagnosis of Aggressive Periodontitis Trained by Immunologic Parameters. PLoS ONE 2014, 9, e89757. [Google Scholar] [CrossRef]
- Ozden, F.O.; Özgönenel, O.; Özden, B.; Aydogdu, A. Diagnosis of Periodontal Diseases Using Different Classification Algorithms: A Preliminary Study. Niger. J. Clin. Pr. 2015, 18, 416–421. [Google Scholar] [CrossRef]
- Alalharith, D.M.; Alharthi, H.M.; Alghamdi, W.M.; Alsenbel, Y.M.; Aslam, N.; Khan, I.U.; Shahin, S.Y.; Dianišková, S.; Alhareky, M.S.; Barouch, K.K. A Deep Learning-Based Approach for the Detection of Early Signs of Gingivitis in Orthodontic Patients Using Faster Region-Based Convolutional Neural Networks. Int. J. Environ. Res. Public Health 2020, 17, 8447. [Google Scholar] [CrossRef]
- Danks, R.P.; Bano, S.; Orishko, A.; Tan, H.J.; Moreno Sancho, F.; D’Aiuto, F.; Stoyanov, D. Automating Periodontal Bone Loss Measurement via Dental Landmark Localisation. Int. J. Comput. Assist. Radiol. Surg. 2021, 16, 1189–1199. [Google Scholar] [CrossRef] [PubMed]
- Ning, W.; Acharya, A.; Sun, Z.; Ogbuehi, A.C.; Li, C.; Hua, S.; Ou, Q.; Zeng, M.; Liu, X.; Deng, Y.; et al. Deep Learning Reveals Key Immunosuppression Genes and Distinct Immunotypes in Periodontitis. Front. Genet. 2021, 12, 648329. [Google Scholar] [CrossRef]
- Wang, C.-W.; Hao, Y.; Di Gianfilippo, R.; Sugai, J.; Li, J.; Gong, W.; Kornman, K.S.; Wang, H.-L.; Kamada, N.; Xie, Y.; et al. Machine Learning-Assisted Immune Profiling Stratifies Peri-Implantitis Patients with Unique Microbial Colonization and Clinical Outcomes. Theranostics 2021, 11, 6703–6716. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Liang, Y.; Zhang, X.; Liu, C.; He, L.; Miao, L.; Sun, W. A Deep Learning Approach to Automatic Gingivitis Screening Based on Classification and Localization in RGB Photos. Sci. Rep. 2021, 11, 16831. [Google Scholar] [CrossRef] [PubMed]
- Revilla-León, M.; Gómez-Polo, M.; Vyas, S.; Barmak, B.A.; Galluci, G.O.; Att, W.; Krishnamurthy, V.R. Artificial Intelligence Applications in Implant Dentistry: A Systematic Review. J. Prosthet. Dent. 2023, 129, 293–300. [Google Scholar] [CrossRef]
- Lee, S.; Gantes, B.; Riggs, M.; Crigger, M. Bone Density Assessments of Dental Implant Sites: 3. Bone Quality Evaluation during Osteotomy and Implant Placement. Int. J. Oral Maxillofac. Implant. 2007, 22, 208–212. [Google Scholar]
- Kernen, F.; Kramer, J.; Wanner, L.; Wismeijer, D.; Nelson, K.; Flügge, T. A Review of Virtual Planning Software for Guided Implant Surgery—Data Import and Visualization, Drill Guide Design and Manufacturing. BMC Oral Health 2020, 20, 251. [Google Scholar] [CrossRef]
- Sadighpour, L.; Rezaei, S.; Paknejad, M.; Jafary, F.; Aslani, P. The Application of an Artificial Neural Network to Support Decision Making in Edentulous Maxillary Implant Prostheses. J. Res. Pract. Dent. 2014, 2014, 369025. [Google Scholar] [CrossRef]
- Lerner, H.; Mouhyi, J.; Admakin, O.; Mangano, F. Artificial Intelligence in Fixed Implant Prosthodontics: A Retrospective Study of 106 Implant-Supported Monolithic Zirconia Crowns Inserted in the Posterior Jaws of 90 Patients. BMC Oral Health 2020, 20, 80. [Google Scholar] [CrossRef]
- Kurt Bayrakdar, S.; Orhan, K.; Bayrakdar, I.S.; Bilgir, E.; Ezhov, M.; Gusarev, M.; Shumilov, E. A Deep Learning Approach for Dental Implant Planning in Cone-Beam Computed Tomography Images. BMC Med. Imaging 2021, 21, 86. [Google Scholar] [CrossRef]
- Lee, D.-W.; Kim, S.-Y.; Jeong, S.-N.; Lee, J.-H. Artificial Intelligence in Fractured Dental Implant Detection and Classification: Evaluation Using Dataset from Two Dental Hospitals. Diagnostics 2021, 11, 233. [Google Scholar] [CrossRef] [PubMed]
- Thurzo, A.; Urbanová, W.; Novák, B.; Czako, L.; Siebert, T.; Stano, P.; Mareková, S.; Fountoulaki, G.; Kosnáčová, H.; Varga, I. Where Is the Artificial Intelligence Applied in Dentistry? Systematic Review and Literature Analysis. Healthcare 2022, 10, 1269. [Google Scholar] [CrossRef] [PubMed]
- Ding, H.; Wu, J.; Zhao, W.; Matinlinna, J.P.; Burrow, M.F.; Tsoi, J.K.H. Artificial Intelligence in Dentistry—A Review. Front. Dent. Med. 2023, 4, 1085251. [Google Scholar] [CrossRef]
- Junaid, N.; Khan, N.; Ahmed, N.; Abbasi, M.S.; Das, G.; Maqsood, A.; Ahmed, A.R.; Marya, A.; Alam, M.K.; Heboyan, A. Development, Application, and Performance of Artificial Intelligence in Cephalometric Landmark Identification and Diagnosis: A Systematic Review. Healthcare 2022, 10, 2454. [Google Scholar] [CrossRef]
- Thanathornwong, B. Bayesian-Based Decision Support System for Assessing the Needs for Orthodontic Treatment. Healthc. Inf. Res. 2018, 24, 22–28. [Google Scholar] [CrossRef]
- Xie, X.; Wang, L.; Wang, A. Artificial Neural Network Modeling for Deciding If Extractions Are Necessary Prior to Orthodontic Treatment. Angle Orthod. 2010, 80, 262–266. [Google Scholar] [CrossRef]
- Jung, S.-K.; Kim, T.-W. New Approach for the Diagnosis of Extractions with Neural Network Machine Learning. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 127–133. [Google Scholar] [CrossRef]
- Choi, H.-I.; Jung, S.-K.; Baek, S.-H.; Lim, W.H.; Ahn, S.-J.; Yang, I.-H.; Kim, T.-W. Artificial Intelligent Model With Neural Network Machine Learning for the Diagnosis of Orthognathic Surgery. J. Craniofac. Surg. 2019, 30, 1986–1989. [Google Scholar] [CrossRef]
- Yu, H.J.; Cho, S.R.; Kim, M.J.; Kim, W.H.; Kim, J.W.; Choi, J. Automated Skeletal Classification with Lateral Cephalometry Based on Artificial Intelligence. J. Dent. Res. 2020, 99, 249–256. [Google Scholar] [CrossRef]
- Kök, H.; Acilar, A.M.; İzgi, M.S. Usage and Comparison of Artificial Intelligence Algorithms for Determination of Growth and Development by Cervical Vertebrae Stages in Orthodontics. Prog. Orthod. 2019, 20, 41. [Google Scholar] [CrossRef]
- Bianchi, J.; de Oliveira Ruellas, A.C.; Gonçalves, J.R.; Paniagua, B.; Prieto, J.C.; Styner, M.; Li, T.; Zhu, H.; Sugai, J.; Giannobile, W.; et al. Osteoarthritis of the Temporomandibular Joint Can Be Diagnosed Earlier Using Biomarkers and Machine Learning. Sci. Rep. 2020, 10, 8012. [Google Scholar] [CrossRef] [PubMed]
- Kök, H.; Izgi, M.S.; Acilar, A.M. Determination of Growth and Development Periods in Orthodontics with Artificial Neural Network. Orthod. Craniofac. Res. 2021, 24 (Suppl. S2), 76–83. [Google Scholar] [CrossRef] [PubMed]
- Aubreville, M.; Knipfer, C.; Oetter, N.; Jaremenko, C.; Rodner, E.; Denzler, J.; Bohr, C.; Neumann, H.; Stelzle, F.; Maier, A. Automatic Classification of Cancerous Tissue in Laserendomicroscopy Images of the Oral Cavity Using Deep Learning. Sci. Rep. 2017, 7, 11979. [Google Scholar] [CrossRef] [PubMed]
- Hung, M.; Park, J.; Hon, E.S.; Bounsanga, J.; Moazzami, S.; Ruiz-Negrón, B.; Wang, D. Artificial Intelligence in Dentistry: Harnessing Big Data to Predict Oral Cancer Survival. World J. Clin. Oncol. 2020, 11, 918–934. [Google Scholar] [CrossRef] [PubMed]
- Brickley, M.R.; Shepherd, J.P. Performance of a Neural Network Trained to Make Third-Molar Treatment-Planning Decisions. Med. Decis. Mak. 1996, 16, 153–160. [Google Scholar] [CrossRef]
- Zhang, W.; Li, J.; Li, Z.-B.; Li, Z. Predicting Postoperative Facial Swelling Following Impacted Mandibular Third Molars Extraction by Using Artificial Neural Networks Evaluation. Sci. Rep. 2018, 8, 12281. [Google Scholar] [CrossRef]
- Poedjiastoeti, W.; Suebnukarn, S. Application of Convolutional Neural Network in the Diagnosis of Jaw Tumors. Healthcare Inf. Res. 2018, 24, 236–241. [Google Scholar] [CrossRef]
- Murata, M.; Ariji, Y.; Ohashi, Y.; Kawai, T.; Fukuda, M.; Funakoshi, T.; Kise, Y.; Nozawa, M.; Katsumata, A.; Fujita, H.; et al. Deep-Learning Classification Using Convolutional Neural Network for Evaluation of Maxillary Sinusitis on Panoramic Radiography. Oral Radiol. 2019, 35, 301–307. [Google Scholar] [CrossRef]
- Endres, M.G.; Hillen, F.; Salloumis, M.; Sedaghat, A.R.; Niehues, S.M.; Quatela, O.; Hanken, H.; Smeets, R.; Beck-Broichsitter, B.; Rendenbach, C.; et al. Development of a Deep Learning Algorithm for Periapical Disease Detection in Dental Radiographs. Diagnostics 2020, 10, 430. [Google Scholar] [CrossRef]
- Yang, H.; Jo, E.; Kim, H.J.; Cha, I.-H.; Jung, Y.-S.; Nam, W.; Kim, J.-Y.; Kim, J.-K.; Kim, Y.H.; Oh, T.G.; et al. Deep Learning for Automated Detection of Cyst and Tumors of the Jaw in Panoramic Radiographs. J. Clin. Med. 2020, 9, 1839. [Google Scholar] [CrossRef]
- Johari, M.; Esmaeili, F.; Andalib, A.; Garjani, S.; Saberkari, H. Detection of Vertical Root Fractures in Intact and Endodontically Treated Premolar Teeth by Designing a Probabilistic Neural Network: An Ex Vivo Study. Dentomaxillofac. Radiol. 2017, 46, 20160107. [Google Scholar] [CrossRef] [PubMed]
- Saghiri, M.A.; Asgar, K.; Boukani, K.K.; Lotfi, M.; Aghili, H.; Delvarani, A.; Karamifar, K.; Saghiri, A.M.; Mehrvarzfar, P.; Garcia-Godoy, F. A New Approach for Locating the Minor Apical Foramen Using an Artificial Neural Network. Int. Endod. J. 2012, 45, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Kositbowornchai, S.; Plermkamon, S.; Tangkosol, T. Performance of an Artificial Neural Network for Vertical Root Fracture Detection: An Ex Vivo Study. Dent. Traumatol. 2013, 29, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, M.; Inamoto, K.; Shibata, N.; Ariji, Y.; Yanashita, Y.; Kutsuna, S.; Nakata, K.; Katsumata, A.; Fujita, H.; Ariji, E. Evaluation of an Artificial Intelligence System for Detecting Vertical Root Fracture on Panoramic Radiography. Oral Radiol. 2020, 36, 337–343. [Google Scholar] [CrossRef]
- Orhan, K.; Bayrakdar, I.S.; Ezhov, M.; Kravtsov, A.; Özyürek, T. Evaluation of Artificial Intelligence for Detecting Periapical Pathosis on Cone-Beam Computed Tomography Scans. Int. Endod. J. 2020, 53, 680–689. [Google Scholar] [CrossRef] [PubMed]
- Mirbabaie, M.; Stieglitz, S.; Frick, N.R.J. Artificial Intelligence in Disease Diagnostics: A Critical Review and Classification on the Current State of Research Guiding Future Direction. Health Technol. 2021, 11, 693–731. [Google Scholar] [CrossRef]
- Mori, Y.; Kudo, S.-E.; East, J.E.; Rastogi, A.; Bretthauer, M.; Misawa, M.; Sekiguchi, M.; Matsuda, T.; Saito, Y.; Ikematsu, H.; et al. Cost Savings in Colonoscopy with Artificial Intelligence-Aided Polyp Diagnosis: An Add-on Analysis of a Clinical Trial (with Video). Gastrointest. Endosc. 2020, 92, 905–911.e1. [Google Scholar] [CrossRef]
- Lee, D.; Yoon, S.N. Application of Artificial Intelligence-Based Technologies in the Healthcare Industry: Opportunities and Challenges. Int. J. Environ. Res. Public Health 2021, 18, 271. [Google Scholar] [CrossRef]
- Salcedo, J.; Rosales, M.; Kim, J.S.; Nuno, D.; Suen, S.-C.; Chang, A.H. Cost-Effectiveness of Artificial Intelligence Monitoring for Active Tuberculosis Treatment: A Modeling Study. PLoS ONE 2021, 16, e0254950. [Google Scholar] [CrossRef]
- Wani, S.U.D.; Khan, N.A.; Thakur, G.; Gautam, S.P.; Ali, M.; Alam, P.; Alshehri, S.; Ghoneim, M.M.; Shakeel, F. Utilization of Artificial Intelligence in Disease Prevention: Diagnosis, Treatment, and Implications for the Healthcare Workforce. Healthcare 2022, 10, 608. [Google Scholar] [CrossRef]
- Tang, H.; Huang, H.; Liu, J.; Zhu, J.; Gou, F.; Wu, J. AI-Assisted Diagnosis and Decision-Making Method in Developing Countries for Osteosarcoma. Healthcare 2022, 10, 2313. [Google Scholar] [CrossRef] [PubMed]
- Fatima, A.; Shafi, I.; Afzal, H.; Díez, I.D.L.T.; Lourdes, D.R.-S.M.; Breñosa, J.; Espinosa, J.C.M.; Ashraf, I. Advancements in Dentistry with Artificial Intelligence: Current Clinical Applications and Future Perspectives. Healthcare 2022, 10, 2188. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.S.; Zary, N. Applications and Challenges of Implementing Artificial Intelligence in Medical Education: Integrative Review. JMIR Med. Educ. 2019, 5, e13930. [Google Scholar] [CrossRef] [PubMed]
- Li, D. 5G and Intelligence Medicine-How the next Generation of Wireless Technology Will Reconstruct Healthcare? Precis. Clin. Med. 2019, 2, 205–208. [Google Scholar] [CrossRef] [PubMed]
- Joyce, D.W.; Kormilitzin, A.; Smith, K.A.; Cipriani, A. Explainable Artificial Intelligence for Mental Health through Transparency and Interpretability for Understandability. NPJ Digit. Med. 2023, 6, 6. [Google Scholar] [CrossRef] [PubMed]
- Goldhahn, J.; Rampton, V.; Spinas, G.A. Could Artificial Intelligence Make Doctors Obsolete? BMJ 2018, 363, k4563. [Google Scholar] [CrossRef]
- Kumar, P.; Chauhan, S.; Awasthi, L.K. Artificial Intelligence in Healthcare: Review, Ethics, Trust Challenges & Future Research Directions. Eng. Appl. Artif. Intell. 2023, 120, 105894. [Google Scholar] [CrossRef]
- Shaheen, M.Y. Applications of Artificial Intelligence (AI) in Healthcare: A Review. Sci. Open 2021, 2021, 1–8. [Google Scholar] [CrossRef]
- Celi, L.A.; Cellini, J.; Charpignon, M.-L.; Dee, E.C.; Dernoncourt, F.; Eber, R.; Mitchell, W.G.; Moukheiber, L.; Schirmer, J.; Situ, J.; et al. Sources of Bias in Artificial Intelligence That Perpetuate Healthcare Disparities-A Global Review. PLOS Digit. Health 2022, 1, e0000022. [Google Scholar] [CrossRef]
- Abdullah, Y.I.; Schuman, J.S.; Shabsigh, R.; Caplan, A.; Al-Aswad, L.A. Ethics of Artificial Intelligence in Medicine and Ophthalmology. Asia Pac. J. Ophthalmol. 2021, 10, 289–298. [Google Scholar] [CrossRef]
- Reddy, S.; Allan, S.; Coghlan, S.; Cooper, P. A Governance Model for the Application of AI in Health Care. J. Am. Med. Inf. Assoc. 2020, 27, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Rudin, C.; Radin, J. Why Are We Using Black Box Models in AI When We Don’t Need To? A Lesson From An Explainable AI Competition. Harv. Data Sci. Rev. 2019, 1, 1–10. [Google Scholar] [CrossRef]
- Ying, X. An Overview of Overfitting and Its Solutions. J. Phys. Conf. Ser. 2019, 1168, 022022. [Google Scholar] [CrossRef]
- Mashar, M.; Chawla, S.; Chen, F.; Lubwama, B.; Patel, K.; Kelshiker, M.A.; Bachtiger, P.; Peters, N.S. Artificial Intelligence Algorithms in Health Care: Is the Current Food and Drug Administration Regulation Sufficient? JMIR AI 2023, 2, e42940. [Google Scholar] [CrossRef]
- Kermany, D.S.; Goldbaum, M.; Cai, W.; Valentim, C.C.S.; Liang, H.; Baxter, S.L.; McKeown, A.; Yang, G.; Wu, X.; Yan, F.; et al. Identifying Medical Diagnoses and Treatable Diseases by Image-Based Deep Learning. Cell 2018, 172, 1122–1131.e9. [Google Scholar] [CrossRef] [PubMed]
- Rosen, J.M.; Kun, L.; Mosher, R.E.; Grigg, E.; Merrell, R.C.; Macedonia, C.; Klaudt-Moreau, J.; Price-Smith, A.; Geiling, J. Cybercare 2.0: Meeting the Challenge of the Global Burden of Disease in 2030. Health Technol. 2016, 6, 35–51. [Google Scholar] [CrossRef] [PubMed]
- Houssami, N.; Kirkpatrick-Jones, G.; Noguchi, N.; Lee, C.I. Artificial Intelligence (AI) for the Early Detection of Breast Cancer: A Scoping Review to Assess AI’s Potential in Breast Screening Practice. Expert Rev. Med. Devices 2019, 16, 351–362. [Google Scholar] [CrossRef]
- Labovitz, D.L.; Shafner, L.; Reyes Gil, M.; Virmani, D.; Hanina, A. Using Artificial Intelligence to Reduce the Risk of Nonadherence in Patients on Anticoagulation Therapy. Stroke 2017, 48, 1416–1419. [Google Scholar] [CrossRef]




| System | Abbreviation | Function |
|---|---|---|
| Artificial Neural Network | ANN | It is trained by processing examples, each of which contains a known “input” and “result,” forming probability-weighted associations between the two, which are stored within the data structure of the net itself [34]. |
| Backpropagation Neural Network | - | Backpropagation is a process involved in training a neural network. It involves taking the error rate of a forward propagation and feeding this loss backward through the neural network layers to fine-tune the weights. Backpropagation is the essence of neural net training [35]. |
| Bayesian Inference | - | It allows for an algorithm to make predictions based on prior beliefs. In Bayesian inference, the posterior distribution of predictors (derived from observed data) is updated based on new evidence [36]. |
| Causal Associational Network | CASNET | This model consists of three main components: observations of a patient, pathophysiological states, and disease classifications. As observations are recorded, they are associated with the appropriate states [37]. |
| Convolutional Neural Network | CNN | A network architecture for deep learning that learns directly from data. CNNs are particularly useful for finding patterns in images to recognize objects, classes, and categories. They can also be quite effective for classifying audio, time-series, and signal data [38]. |
| Deep Neural Network | DNN | An ANN with multiple layers between the input and output layers. There are different types of neural networks but they always consist of the same components: neurons, synapses, weights, biases, and functions [39]. |
| Light Gradient Boosting Machine | LightGBM | LightGBM is a gradient-boosting ensemble method that is based on decision trees. As with other decision tree-based methods, LightGBM can be used for both classification and regression. LightGBM is optimized for a high performance with distributed systems [40]. |
| Multilayer Perceptron | MLP | A feedforward artificial neural network that generates a set of outputs from a set of inputs. An MLP is characterized by several layers of input nodes connected as a directed graph between the input and output layers. MLP uses backpropagation for training the network [41]. |
| Natural Language Processing | NLP | It enables machines to understand the human language. Its goal is to build systems that can make sense of text and automatically perform tasks such as translation, a spell check, or topic classification [18]. |
| Optimal Channel Networks | OCNet | Oriented spanning trees that reproduce all scaling features characteristic of real, natural river networks. As such, they can be used in a variety of numerical and laboratory experiments in the fields of hydrology, ecology, and epidemiology [42]. |
| Probabilistic Neural Network | PNN | A feedforward neural network used to handle classification and pattern recognition problems [43]. |
| Random Forest Models | An ensemble learning method for classification, regression, and other tasks that operates by constructing a multitude of decision trees at the training time [44]. | |
| Recurrent Neural Network | RNN | An ANN where connections between nodes can create a cycle, allowing output from some nodes to affect subsequent input to the same nodes. This allows it to exhibit temporal dynamic behavior [45]. |
| Region-based Convolutional Neural Network | R-CNN | The key concept behind the R-CNN series is region proposals. Region proposals are used to localize objects within an image [46,47]. |
| Support Vector Machine | SVM | A type of deep learning algorithm that performs supervised learning for classification or regression of data groups. In AI and machine learning, supervised learning systems provide both input and desired output data, which are labeled for classification [48]. |
| Extreme Gradient Boosting | XGBoost | XGBoost, which stands for extreme gradient boosting, is a scalable, distributed gradient-boosted decision tree (GBDT) machine learning library. It provides parallel tree boosting and is the leading machine learning library for regression, classification, and ranking problems [49]. |
| Target | Algorithm | Sample | Results | Study |
|---|---|---|---|---|
| Discriminating asthma from chronic obstructive pulmonary disease | Multinomial regression, gradient boosting, and recurrent neural networks | In total, 178,962 patients treated by two “R03” treatment prescriptions | The best models were obtained with the boosting approach and RNN, with an overall accuracy of 68% | Joumaa et al., (2022) [87] |
| Predicting pediatric asthma exacerbations | XGBoost (gradient-boosting decision trees) | Electronic health records for 5982 pediatric subjects | Sensitivity 70%, predictive values of 13.8% for 180-day outcomes and 2.9% for 30-day outcomes | Hurst et al., (2022) [88] |
| Diagnosis of AD on multiphoton tomography | CNN | In total, 3663 multiphoton tomography images from AD and healthy subjects | A correct diagnosis in 97.0% of all images Sensitivity of 0.966 Specificity of 0.977 | Guimarães et al., (2020) [89] |
| Prediction of AD severity over time | Bayesian inference | Recordings of AD severity scores and treatments used by 59 and 334 pediatric subjects | Improvement of the chance-level forecast by 60% | Hurault et al., (2020) [90] |
| Phenotyping and identification of severity-associated factors in adolescent and adult patients with atopic dermatitis | ML-gradient boosting approach with cross-validation-based tuning multinomial logistic regression. | 367 patients | The predictive performance of machine learning–gradient boosting vs. multinomial logistic regression differed only slightly (mean multiclass area under the curve value: 0.71 [95% CI, 0.69–0.72] vs. 0.68 [0.66–0.70], respectively | Maintz et al., (2021) [91] |
| Distinguishing different endotypes of CRSwNP based on clinical biomarkers | ANN logistic regression | In total, 15 clinical features from 60 healthy controls, 60 eCRSwNP, and 49 non-eCRSwNP | ANN models showed a better performance, significantly higher than those from the LR models (0.976 vs. 0.902, p = 0.048; 0.970 vs. 0.845, p = 0.011) | Zhou et al., (2023) [92] |
| Prediction of hypersensitivity to β-lactam | ANN logistic regression | Data records for 1271 allergic and non-allergic subjects |
ANN: sensitivity of 89.5% and 81.1%, specificity of 86.1% and 97.9%, positive predictive values of 82.1% and 91.1%
LR: sensitivity of 31.9% and specificity of 98.8% | Moreno et al., (2020) [93] |
| AI Model | Results | Study |
|---|---|---|
| Diagnosis | ||
| TopNetmAb model: Comprehensive topology-based AI. | Predict the binding free energy changes of S and ACE2/antibody complexes induced by mutations on the S RBD, of the Omicron variant. | Chen et al., (2022) [113] |
| DL method (3D-DL framework) for DNA sequence classification using CNN. | SARS-CoV-2 viral genomic sequencing. Viral evaluation accuracy > 99%. | Lopez-Rincon et al., (2021) [114] |
| Drug discovery | ||
| DeepH-DTA: A squeezed-excited dense convolutional network for learning hidden representations within amino acid sequences. | Predict the affinity scores of drugs against SARS-CoV-2 amino acid sequences. | Abdel-Basset et al., (2020) [115] |
| Estimated drug–target interactions. A list of antiviral drugs was identified. | Molecule transformer–drug target interaction (MT-DTI). | Beck et al., (2020) [116] |
| AI-based generative network complex | Generate 15 potential drugs. | Gao et al., (2020) [117] |
| ChemAI; a deep neural network protocol on three drug discovery databases. | Generate 30,000 small compounds that are SARS-CoV-2 inhibitors. | Hofmarcher et al., (2020) [118] |
| ADQN-FBDD: An advanced deep Q-learning network with the fragment-based drug design (a model-free reinforcement learning algorithm). | Generate 47 lead compounds, targeting the SARS-CoV2 3C-like main protease. | Tang et al., (2020) [119] |
| Dense fully convolutional neural network (DFCNN). A list of chemical ligands and peptide drugs was provided. | Used four chemical compound and tripeptide databases to identify potential drugs for COVID-19. | Zhang et al., (2020) [109] |
| Generative DL. An AI-based drug discovery pipeline. | Generate inhibitors for the SARS-CoV-2 3CLpro. | Zhavoronkov et al., (2020) [120] |
| Vaccine development | ||
| Bioinformatic tools and databases | Epitope vaccines were designed by using protein E as an antigenic site. | Abdelmageed et al., (2020) [121] |
| Computational methodology | Identify several epitopes in SARS-CoV-2 for the development of potential vaccines. S protein was identified as an immunogenic and effective vaccine candidate. | Fast et al., (2020) [122] |
| ML and reverse vaccinology | A cocktail vaccine with structural and non-structural proteins in which would accelerate efficient complementary immune responses. | Ong et al., (2020) [123] |
| Integrated bioinformatics pipeline that merges the prediction power of different software (in silico pipeline). | Predict the cross-reactivity of pre-existing vaccination interventions against SARS-CoV-2. | Russo et al., (2021) [124] |
| Immune informatics, reverse vaccinology, and molecular docking analysis. | Three epitope-based subunit vaccines were designated. Only one was reported as the best vaccine. | Sarkar et al., (2020) [125] |
| In silico approach. A molecular docking analysis. | A multi-epitopic vaccine candidate targeting the non-mutational immunogenic regions in envelope protein and surface glycoprotein of SARS-CoV-2. | Susithra Priyadarshni et al., (2021) [126] |
| Target | AI Model | Sample | Results | Study |
|---|---|---|---|---|
| To classify periodontitis by immune response profile to aggressive periodontitis or chronic periodontitis class. | MLP ANN | Data from 29 subjects | 90–98% accuracy | Papantonopoulos et al., (2014) [165] |
| Diagnosis of periodontal diseases. | ANNs, decision trees, and support vector machine | Data from 150 patients | Performance was 98%. The poorest correlation between input and output variables was found in ANN, and its performance was assessed to be 46%. | Ozden et al., (2015) [166] |
| To identify and predict periodontally compromised teeth. | CNN encoder + three dense layers | 1740 periapical X-rays | AUC of 73.4–82.6 [95% CI, 60.9–91.1] in predicting hopeless teeth. | J. H. Lee et al., (2018) [162] |
| To detect periodontal bone loss (PBL) on panoramic dental radiographs. | CNN + three dense layers | 85 panoramic X-rays | Predictive accuracy was determined to be 81%, which is similar to the examiners. | Krois et al., (2019) [159] |
| Pre-emptive detection and diagnosis of periodontal disease and gingivitis by using intraoral images. | Faster R-CNN | 134 photographs | Tooth detection accuracy of 100% to determine region of interest and 77.12% accuracy to detect inflammation. | Alalharith et al., (2020) [167] |
| Predicting periodontitis stage. | CNN | 340 periapical X-rays | Accuracy of 68.3% | Danks et al., (2021) [168] |
| Predicting immunosuppression genes in periodontitis. | DisGeNet, HisgAtlas | Saliva | Accuracy of 92.78% | Ning et al., (2021) [169] |
| Clinical, immune, and microbial profiling of peri-implantitis patients against health. | CNN FARDEEP | Metabolites | Successfully used in logistic regression of plaque samples. | Wang et al., (2021) [170] |
| Research trialing different methods of segmentation to assess plaque on photographs of tooth surfaces (including ‘dye labelling’). | CNN OCNet, Anet | 2884 photographs | AUC prediction of 87.11% for gingivitis and 80.11% for calculus. | Li et al., (2021) [171] |
| Target | AI Model | Sample | Results | Study |
|---|---|---|---|---|
| Decision making in edentulous maxillary implant prostheses | ANN | Implant cases | Within a learning rate of 0.005, the network functioned admirably. The network’s accuracy for the new instances was 83.3%. | Sadighpour et al., (2014) [175] |
| To fabricate implant-supported monolithic zirconia crowns | ANN | Quality of the fabrication of the individual (zirconia abutment) and clinical parameters in subjects | AI appears to be a dependable solution for the restoration of single implants with zirconia crowns cemented on customized hybrid abutments using a fully digital process. | Lerner et al., (2020) [176] |
| Implant planning | CNN | 75 CBCT images | There were statistically significant differences in bone thickness measurements between AI and manual measurements in all locations of the maxilla and mandible (p < 0.001). In addition, the proportion of correct recognition for canals was 72.2%, 66.4% for sinuses/fossae, and 95.3% for missing tooth areas. | Bayrakdar et al., (2021) [177] |
| Fractured dental implant detection and classification | CNN | Radiographic images of 251 intact and 194 fractured dental implants | When compared to fine-tuned and pre-trained VGGNet-19 and Google Net Inception-v3 architectures, automated DCNN architecture using periapical images demonstrated the highest and most reliable detection with an AUC of 0.984 [CI, 0.9–1.0] and classification performance AUC of 0.869 [CI, 0.778–0.929]. | D. W. Lee et al., (2021) [178] |
| Target | AI Model | Sample | Results | Study |
|---|---|---|---|---|
| To decide if extractions are necessary prior to orthodontic treatment | Backpropagation ANN | Data from 180 patients | Accuracy of 80% in predicting whether extraction or non-extraction treatments seemed appropriate for malocclusion patients aged 11 to 15 years. | Xie et al., (2010) [183] |
| To decide if extractions are necessary prior to orthodontic treatment | ANN | In total, 12 cephalometric variables and 6 indexes from 156 patients | Accuracy of 92% | Jung and Kim (2016) [184] |
| Determination of growth and development by cervical vertebrae stages | ANN | Cephalometric radiographs from 300 subjects | Mean accuracy of 77.2% | Kök et al., (2019) [187] |
| Osteoarthritis of the temporomandibular joint diagnosis | Logistic regression, random forest, LightGBM, XGBoost | CBCT blood serum saliva clinical investigation | Accuracy of 82.3% | Bianchi et al., (2020) [188] |
| Determination of growth and development periods | ANN | Cephalometric and hand–wrist radiographs in 419 subjects | Accuracy of 4.27% | Kök et al., (2021) [189] |
| Target | AI Model | Sample | Results | Study |
|---|---|---|---|---|
| Lower-third-molar treatment-planning decisions | Neural networks | Data from 119 patients | Sensitivity of 0.78, which was slightly lower than the oral surgeon’s (0.88), but the difference was not significant, and a specificity of 0.98, which was lower than the oral surgeon’s (0.99) (p = NS). | Brickley and Shepherd (1996) [192] |
| To predict postoperative facial swelling following impacted mandibular third molar extraction | ANN | Data from 400 patients | This AI-based algorithm was 98% reliable in forecasting facial swelling after extraction of impacted third molar teeth. | Zhang et al., (2018) [193] |
| Ameloblastoma and keratocystic odontogenic tumor diagnosis | CNN | 400/100 panoramic X-rays | The CNN had 81.8% sensitivity, 83.3% specificity, 83.0% accuracy, and a diagnostic time of 38 s, respectively. | Poedjiastoeti and Suebnukarn (2018) [194] |
| Evaluation of maxillary sinusitis on panoramic radiography | CNN | Panoramic X-rays from 400 maxillary sinusitis patients/400 healthy subjects | Accuracy of 87.5%, sensitivity of 86.7%, specificity of 88.3%, and area under the curve of 0.875 were obtained by the model. | Murata et al., (2019) [195] |
| Periapical disease detection | ANN | 2902 panoramic X-rays | The deep learning method outperformed 14 of the 24 surgeons in the sample, with an average accuracy of 0.60 (0.04). | Endres et al., (2020) [196] |
| Automated detection of cyst and tumors of the jaw | CNN | 1602 lesions on panoramic X-rays | Comparable with expert dentists. | Yang et al., (2020) [197] |
| Target | AI Model | Sample | Results | Study |
|---|---|---|---|---|
| Locating the minor apical foramen | ANN | 50 teeth | To enhance the accuracy of working length measurement using radiography, artificial neural networks can serve as a second opinion to find the apical foramen on radiographs. | Saghiri et al., (2012) [199] |
| Vertical root fracture detection | ANN | Digital X-rays: 50 sound and 150 vertical root fractures | Adequate sensitivity, specificity, and accuracy to be used as a model for vertical root fracture detection. | Kositbowornchai et al., (2013) [200] |
| Detecting vertical root fracture on X-ray images of endodontically treated and intact teeth | PNN | 240 radiographs (120/120) | 96.6% accuracy, 93.3% sensitivity, 100% specificity. | Johari et al., (2017) [198] |
| Detecting vertical root fracture on panoramic radiography | CNN | 300 panoramic images | Precision of 0.93 | Fukuda et al., (2020) [201] |
| To detect periapical pathosis | CNN | 153 CBCT images | Accuracy of 92.8% | Orhan et al., (2020) [202] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stafie, C.S.; Sufaru, I.-G.; Ghiciuc, C.M.; Stafie, I.-I.; Sufaru, E.-C.; Solomon, S.M.; Hancianu, M. Exploring the Intersection of Artificial Intelligence and Clinical Healthcare: A Multidisciplinary Review. Diagnostics 2023, 13, 1995. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics13121995
Stafie CS, Sufaru I-G, Ghiciuc CM, Stafie I-I, Sufaru E-C, Solomon SM, Hancianu M. Exploring the Intersection of Artificial Intelligence and Clinical Healthcare: A Multidisciplinary Review. Diagnostics. 2023; 13(12):1995. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics13121995
Chicago/Turabian StyleStafie, Celina Silvia, Irina-Georgeta Sufaru, Cristina Mihaela Ghiciuc, Ingrid-Ioana Stafie, Eduard-Constantin Sufaru, Sorina Mihaela Solomon, and Monica Hancianu. 2023. "Exploring the Intersection of Artificial Intelligence and Clinical Healthcare: A Multidisciplinary Review" Diagnostics 13, no. 12: 1995. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics13121995