
Association between the Immunophenotype of Peripheral Blood from mCRPC Patients and the Outcomes of Radium-223 Treatment
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient’s Samples
2.2. Flow Cytometry
2.3. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics of mCRPC Patients at Baseline
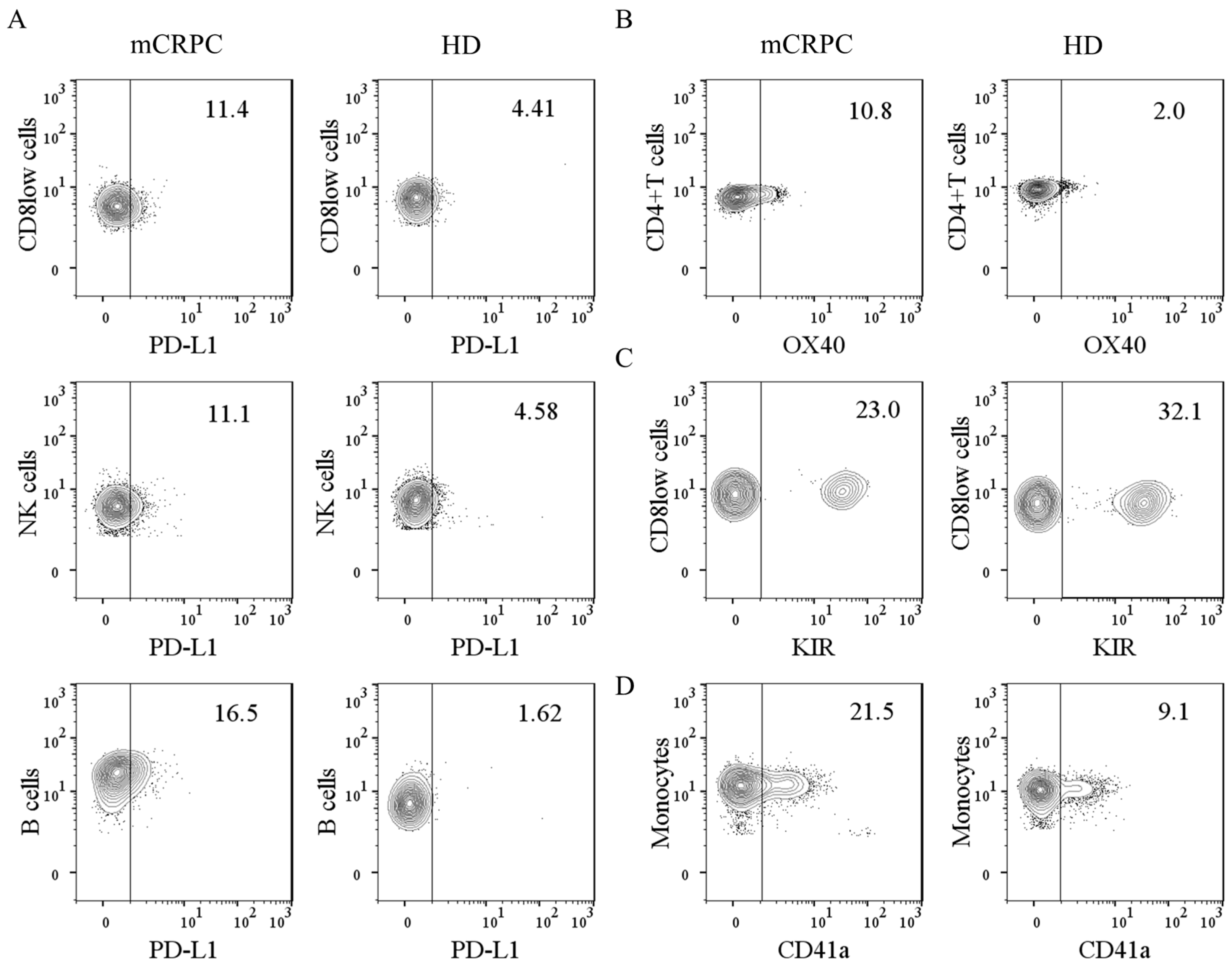
3.2. Baseline Expression of Immunomodulatory Molecules on Leukocytes and Leukocyte–Platelet Complexes
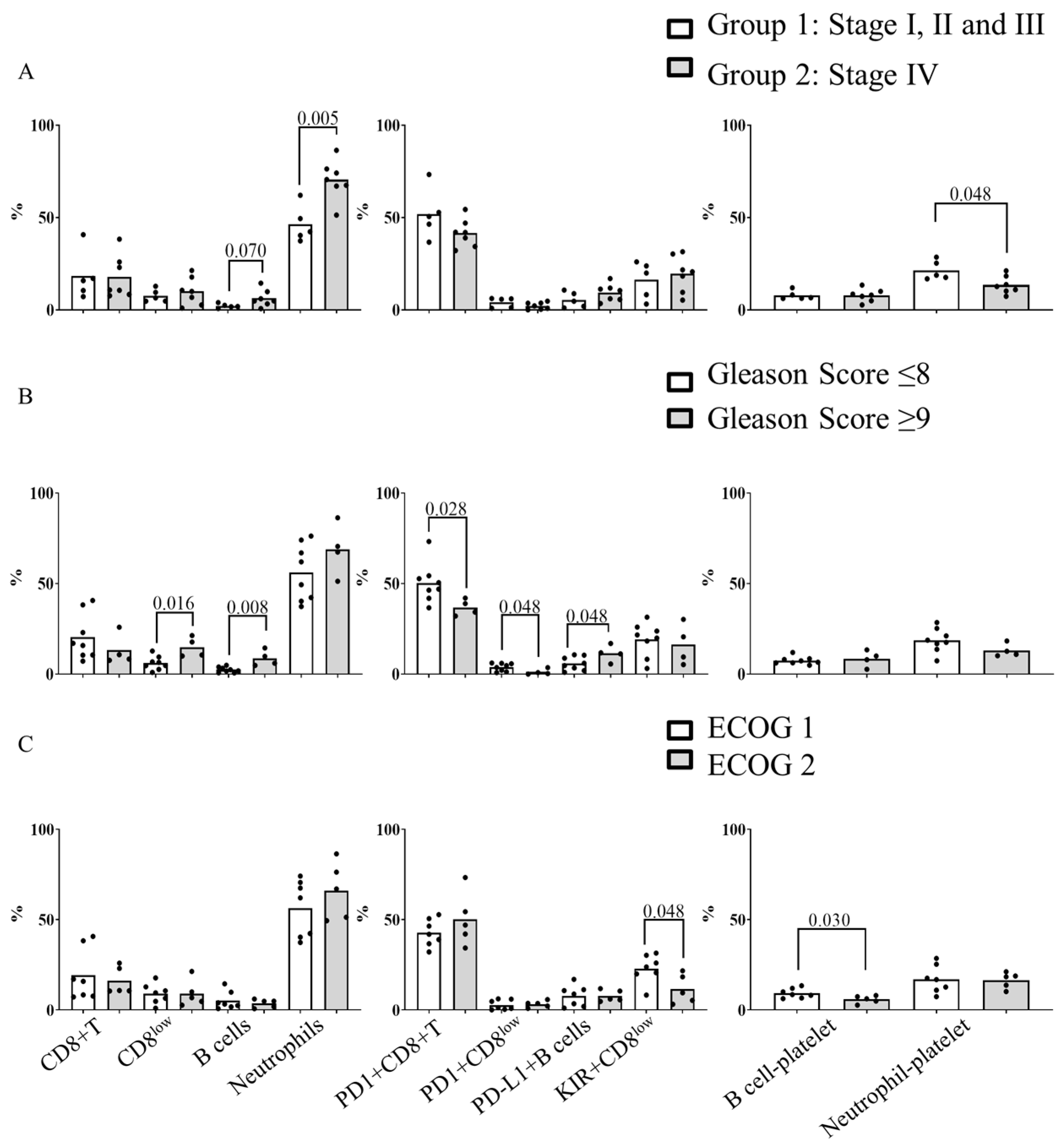
3.3. Relationship between Baseline Blood Immune Subpopulations, Leukocyte–Platelet Complexes and the Clinic Characteristics of mCRPC Patients
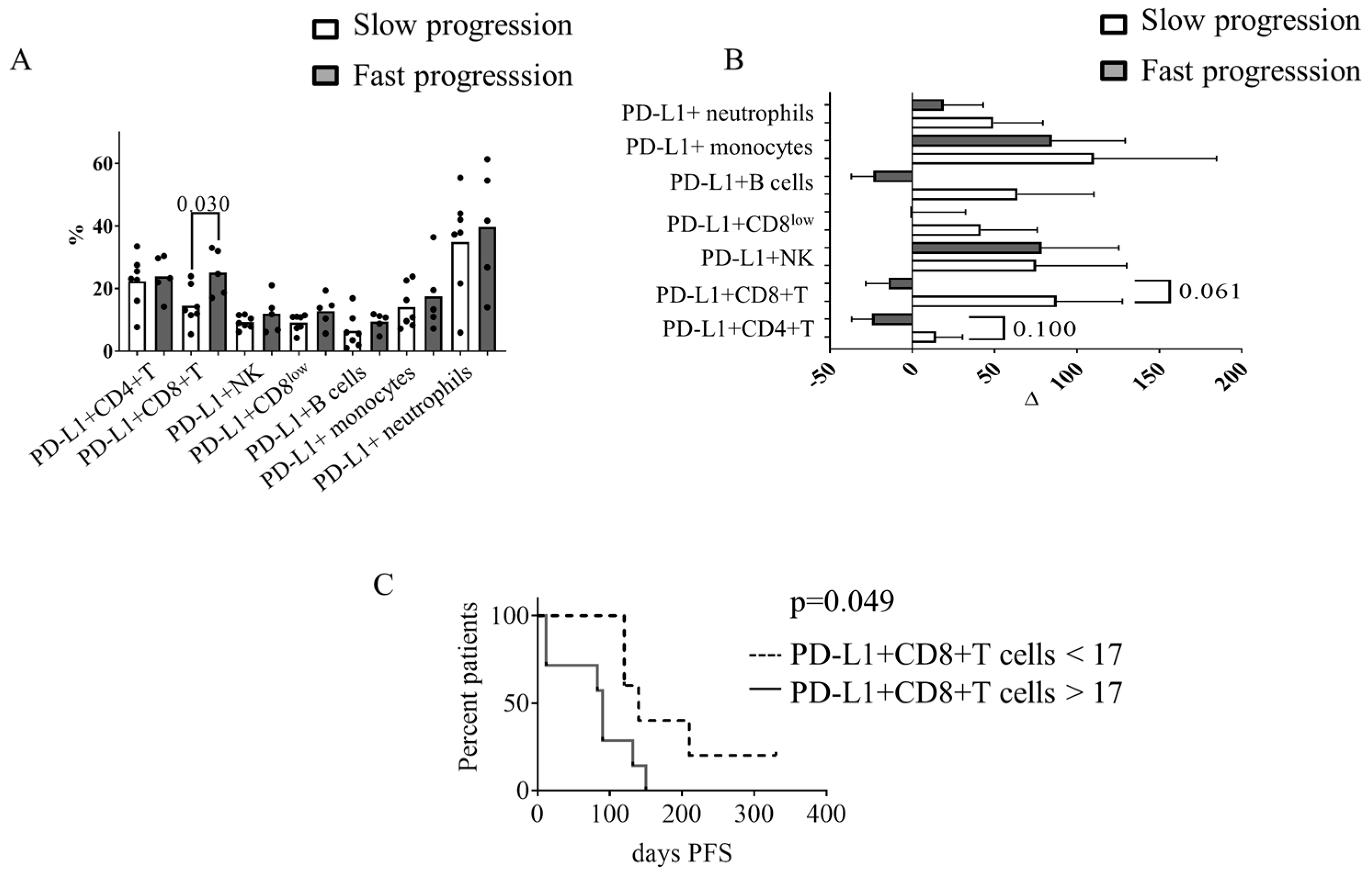
3.4. Circulating PD-L1+ CD8+ T Cells at Baseline Were Associated with Progression-Free Survival in mCRPC Patients
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Garje, R.; Chennamadhavuni, A.; Mott, S.L.; Chambers, I.M.; Gellhaus, P.; Zakharia, Y.; Brown, J. Utilization and Outcomes of Surgical Castration in Comparison to Medical Castration in Metastatic Prostate Cancer. Clin. Genitourin. Cancer 2019, 18, e157–e166. [Google Scholar] [CrossRef] [PubMed]
- Sharifi, N.; Gulley, J.L.; Dahut, W.L. An update on androgen deprivation therapy for prostate cancer. Endocr. Relat. Cancer 2010, 17, R305–R315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parker, C.; Nilsson, S.; Heinrich, D.; Helle, S.I.; O’Sullivan, J.M.; Fosså, S.D.; Chodacki, A.; Wiechno, P.; Logue, J.; Seke, M.; et al. Alpha Emitter Radium-223 and Survival in Metastatic Prostate Cancer. N. Engl. J. Med. 2013, 369, 213–223. [Google Scholar] [CrossRef] [Green Version]
- Deshayes, E.; Roumiguie, M.; Thibault, C.; Beuzeboc, P.; Cachin, F.; Hennequin, C.; Huglo, D.; Rozet, F.; Kassab-Chahmi, D.; Rebillard, X.; et al. Radium 223 dichloride for prostate cancer treatment. Drug Des. Dev. Ther. 2017, 11, 2643–2651. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.W.; Shin, M.S.; Kang, Y.; Kang, I.; Petrylak, D.P. Immune Analysis of Radium-223 in Patients With Metastatic Prostate Cancer. Clin. Genitourin. Cancer 2018, 16, e469–e476. [Google Scholar] [CrossRef] [Green Version]
- Creemers, J.H.A.; van der Doelen, M.J.; van Wilpe, S.; Hermsen, R.; Boer, T.D.-D.; Somford, D.M.; Janssen, M.J.R.; Sedelaar, J.P.M.; Mehra, N.; Textor, J.; et al. Immunophenotyping Reveals Longitudinal Changes in Circulating Immune Cells During Radium-223 Therapy in Patients With Metastatic Castration-Resistant Prostate Cancer. Front. Oncol. 2021, 11, 667658. [Google Scholar] [CrossRef] [PubMed]
- Vardaki, I.; Corn, P.; Gentile, E.; Song, J.H.; Madan, N.; Hoang, A.; Parikh, N.; Guerra, L.; Lee, Y.-C.; Lin, S.-C.; et al. Radium-223 Treatment Increases Immune Checkpoint Expression in Extracellular Vesicles from the Metastatic Prostate Cancer Bone Microenvironment. Clin. Cancer Res. 2021, 27, 3253–3264. [Google Scholar] [CrossRef]
- Catani, M.V.; Savini, I.; Tullio, V.; Gasperi, V. The “Janus Face” of Platelets in Cancer. Int. J. Mol. Sci. 2020, 21, 788. [Google Scholar] [CrossRef] [Green Version]
- Gay, L.J.; Felding-Habermann, B. Contribution of platelets to tumour metastasis. Nat. Rev. Cancer 2011, 11, 123–134. [Google Scholar] [CrossRef]
- Lepone, L.M.; Donahue, R.N.; Grenga, I.; Metenou, S.; Richards, J.; Heery, C.R.; Madan, R.A.; Gulley, J.L.; Schlom, J. Analyses of 123 Peripheral Human Immune Cell Subsets: Defining Differences with Age and between Healthy Donors and Cancer Patients Not Detected in Analysis of Standard Immune Cell Types. J. Circ. Biomarkers 2016, 5, 5. [Google Scholar] [CrossRef] [Green Version]
- Cihan, Y.B.; Arslan, A.; Ergul, M.A. Subtypes of White Blood Cells in Patients with Prostate Cancer or Benign Prostatic Hyperplasia and Healthy Individuals. Asian Pac. J. Cancer Prev. 2013, 14, 4779–4783. [Google Scholar] [CrossRef] [Green Version]
- Gallazzi, M.; Baci, D.; Mortara, L.; Bosi, A.; Buono, G.; Naselli, A.; Guarneri, A.; Dehò, F.; Capogrosso, P.; Albini, A.; et al. Prostate Cancer Peripheral Blood NK Cells Show Enhanced CD9, CD49a, CXCR4, CXCL8, MMP-9 Production and Secrete Monocyte-Recruiting and Polarizing Factors. Front. Immunol. 2021, 11, 586126. [Google Scholar] [CrossRef]
- Yi, J.S.; Cox, M.A.; Zajac, A.J. T-Cell Exhaustion: Characteristics, Causes and Conversion. Immunology 2010, 129, 474–481. [Google Scholar] [CrossRef] [PubMed]
- Veluswamy, P.; Bruder, D. PD-1/PD-L1 pathway inhibition to restore effector functions in exhausted CD8+ T cells: Chances, limitations and potential risks. Transl. Cancer Res. 2018, 7, S530–S537. [Google Scholar] [CrossRef]
- Jensen, S.M.; Maston, L.D.; Gough, M.J.; Ruby, C.E.; Redmond, W.L.; Crittenden, M.; Li, Y.; Puri, S.; Poehlein, C.H.; Morris, N.; et al. Signaling Through OX40 Enhances Antitumor Immunity. Semin. Oncol. 2010, 37, 524–532. [Google Scholar] [CrossRef] [Green Version]
- Massarelli, E.; Lam, V.K.; Parra, E.R.; Rodriguez-Canales, J.; Behrens, C.; Diao, L.; Wang, J.; Blando, J.; Byers, L.A.; Yanamandra, N.; et al. High OX-40 expression in the tumor immune infiltrate is a favorable prognostic factor of overall survival in non-small cell lung cancer. J. Immunother. Cancer 2019, 7, 351. [Google Scholar] [CrossRef] [PubMed]
- Duhen, R.; Ballesteros-Merino, C.; Frye, A.K.; Tran, E.; Rajamanickam, V.; Chang, S.-C.; Koguchi, Y.; Bifulco, C.B.; Bernard, B.; Leidner, R.S.; et al. Neoadjuvant anti-OX40 (MEDI6469) therapy in patients with head and neck squamous cell carcinoma activates and expands antigen-specific tumor-infiltrating T cells. Nat. Commun. 2021, 12, 1047. [Google Scholar] [CrossRef]
- Cantó, E.; Faba, R.; Zamora, C.; Mulet, M.; Garcia-Cuerva, M.S.; Palomino, A.; Anguera, G.; Breda, A.; Maroto, P.; Vidal, S. Immunological Status of Bladder Cancer Patients Based on Urine Leukocyte Composition at Radical Cystectomy. Biomedicines 2021, 9, 1125. [Google Scholar] [CrossRef] [PubMed]
- Larsson, A.-M.; Roxå, A.; Leandersson, K.; Bergenfelz, C. Impact of systemic therapy on circulating leukocyte populations in patients with metastatic breast cancer. Sci. Rep. 2019, 9, 13451. [Google Scholar] [CrossRef] [Green Version]
- Tavares-Murta, B.M.; Mendonça, M.A.O.; Duarte, N.L.; Da Silva, J.A.; Mutão, T.S.; Garcia, C.B.; Murta, E. Systemic Leukocyte Alterations Are Associated With Invasive Uterine Cervical Cancer. Int. J. Gynecol. Cancer 2010, 20, 1154–1159. [Google Scholar] [CrossRef]
- Hayashi, T.; Fujita, K.; Tanigawa, G.; Kawashima, A.; Nagahara, A.; Ujike, T.; Uemura, M.; Takao, T.; Yamaguchi, S.; Nonomura, N. Serum monocyte fraction of white blood cells is increased in patients with high Gleason score prostate cancer. Oncotarget 2016, 8, 35255–35261. [Google Scholar] [CrossRef] [Green Version]
- Bauckneht, M.; Rebuzzi, S.E.; Ponzano, M.; Borea, R.; Signori, A.; Frantellizzi, V.; Rizzini, E.L.; Mascia, M.; Lavelli, V.; Miceli, A.; et al. Prognostic Value of the BIO-Ra Score in Metastatic Castration-Resistant Prostate Cancer Patients Treated with Radium-223 after the European Medicines Agency Restricted Use: Secondary Investigations of the Multicentric BIO-Ra Study. Cancers 2022, 14, 1744. [Google Scholar] [CrossRef]
- Bauckneht, M.; Rebuzzi, S.E.; Signori, A.; Frantellizzi, V.; Murianni, V.; Rizzini, E.L.; Mascia, M.; Lavelli, V.; Donegani, M.I.; Ponzano, M.; et al. The prognostic power of inflammatory indices and clinical factors in metastatic castration-resistant prostate cancer patients treated with radium-223 (BIO-Ra study). Eur. J. Nucl. Med. 2021, 49, 1063–1074. [Google Scholar] [CrossRef]
- de Wit, R.; Wülfing, C.; Castellano, D.; Kramer, G.; Eymard, J.-C.; Sternberg, C.; Fizazi, K.; Tombal, B.; Bamias, A.; Carles, J.; et al. Baseline neutrophil-to-lymphocyte ratio as a predictive and prognostic biomarker in patients with metastatic castration-resistant prostate cancer treated with cabazitaxel versus abiraterone or enzalutamide in the CARD study. ESMO Open 2021, 6, 100241. [Google Scholar] [CrossRef] [PubMed]
- Parikh, S.; Murray, L.; Kenning, L.; Bottomley, D.; Din, O.; Dixit, S.; Ferguson, C.; Handforth, C.; Joseph, L.; Mokhtar, D.; et al. Real-world Outcomes and Factors Predicting Survival and Completion of Radium 223 in Metastatic Castrate-resistant Prostate Cancer. Clin. Oncol. 2018, 30, 548–555. [Google Scholar] [CrossRef]
- Zamora, C.; Riudavets, M.; Anguera, G.; Alserawan, L.; Sullivan, I.; Barba, A.; Serra, J.; Ortiz, M.A.; Gallardo, P.; Perea, L.; et al. Circulating leukocyte–platelet complexes as a predictive biomarker for the development of immune-related adverse events in advanced non-small cell lung cancer patients receiving anti-PD-(L)1 blocking agents. Cancer Immunol. Immunother. 2021, 70, 1691–1704. [Google Scholar] [CrossRef]
- Li, N. Platelets in cancer metastasis: To help the “villain” to do evil. Int. J. Cancer 2016, 138, 2078–2087. [Google Scholar] [CrossRef] [PubMed]
- Miyashita, T.; Tajima, H.; Makino, I.; Nakagawara, H.; Kitagawa, H.; Fushida, S.; Harmon, J.W.; Ohta, T. Metastasis-promoting role of extravasated platelet activation in tumor. J. Surg. Res. 2015, 193, 289–294. [Google Scholar] [CrossRef]
- Labelle, M.; Begum, S.; Hynes, R.O. Direct signaling between platelets and cancer cells induces an epithelial-mesenchymal-like transition and promotes metastasis. Cancer Cell 2011, 20, 576–590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chai, S.; Matsumoto, N.; Storgard, R.; Peng, C.-C.; Aparicio, A.; Ormseth, B.; Rappard, K.; Cunningham, K.; Kolatkar, A.; Nevarez, R.; et al. Platelet-Coated Circulating Tumor Cells Are a Predictive Biomarker in Patients with Metastatic Castrate-Resistant Prostate Cancer. Mol. Cancer Res. 2021, 19, 2036–2045. [Google Scholar] [CrossRef]
- Datar, I.; Sanmamed, M.F.; Wang, J.; Henick, B.S.; Choi, J.; Badri, T.; Dong, W.; Mani, N.; Toki, M.; Mejías, L.D.; et al. Expression Analysis and Significance of PD-1, LAG-3, and TIM-3 in Human Non–Small Cell Lung Cancer Using Spatially Resolved and Multiparametric Single-Cell Analysis. Clin. Cancer Res. 2019, 25, 4663–4673. [Google Scholar] [CrossRef] [PubMed]
- Qin, S.; Xu, L.; Yi, M.; Yu, S.; Wu, K.; Luo, S. Novel immune checkpoint targets: Moving beyond PD-1 and CTLA-4. Mol. Cancer 2019, 18, 155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polasky, C.; Wendt, F.; Pries, R.; Wollenberg, B. Platelet Induced Functional Alteration of CD4+ and CD8+ T Cells in HNSCC. Int. J. Mol. Sci. 2020, 21, 7507. [Google Scholar] [CrossRef] [PubMed]
- Zamora, C.; Cantó, E.; Nieto, J.C.; Bardina, J.; Diaz-Torné, C.; Moya, P.; Magallares, B.; Ortiz, M.A.; Julià, G.; Juarez, C.; et al. Binding of Platelets to Lymphocytes: A Potential Anti-Inflammatory Therapy in Rheumatoid Arthritis. J. Immunol. 2017, 198, 3099–3108. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Patients n = 12 | HDs n = 9 | |
|---|---|---|
| Age | 79.08 ± 7.62 | 62.48 ± 8.10 |
| Weight (kg) | 74.75 ± 10.10 | 68.13 ± 8.44 |
| Height (cm) | 168.18 ± 7.70 | 173.40 ± 3.92 |
| Months between diagnosis and sample collection | 94.10 ± 70.43 | |
| Months between resistance to castration and sample collection | 50.42 ± 37.78 | |
| Month between metastasis and sample collection | 47.82 ± 27.70 | |
| Stage disease at moment of diagnosis (%) Stage disease at moment of sample collection | I (16%); II (16%); III (8%); IV (60%) IV (100%) | |
| Gleason score (%): | ||
| ≤8 ≥9 ECOG performance-status score (0–2): 1 2 | 66% 33% 7 5 | |
| Median hematological and biochemical values: | ||
| Platelets (×109/L) | 217.89 ± 66.60 | |
| Lymphocytes (×109/L) Neutrophils (×109/L) Monocytes (×109/L) Hemoglobin (g/L) Albumin (g/L) Alkaline phosphatase (U/L) PSA (µg/L) Lactate dehydrogenase (U/L) | 1.32 ± 0.48 6.48 ± 3.58 0.50 ± 0.20 102.67 ± 14.47 38.85 ± 3.27 224.67 ± 197.39 305.77 ± 425.56 268.75 ± 69.22 | |
| Previous treatment: | ||
| Abiraterone (yes/no) Enzalutamide (yes/no) Chemotherapy (yes/no) | 11/1 10/2 9/3 |
| Count/µL | % | |||
|---|---|---|---|---|
| mCRPC | HD | mCRPC | HD | |
| a CD4+ T cells | 99.74 (53.27–160.8) | 332.1 (237.5–380.5) *** | 35.61 (26.3–39.36) | 40.14 (38.66–46.53) ** |
| a CD8+ T cells | 43.98 (32.41–116.3) | 164.4 (120.2–306.7) ** | 16.45 (10.49–35.17) | 22 (15.24–30.76) |
| a CD8low cells | 18.98 (9.41–69.86) | 31.8 (20.8–41.66) | 8.17 (3.26–12.24) | 3.77 (2.79–6.9) |
| a B cells | 13.28 (4.19–32.01) | 69 (43.76–104.5) ** | 3.60 (1.73–6.12) | 8.68 (6.12–15.66) ** |
| a NK cells | 40.61 (27.52–134.3) | 47.59 (21.7–97.58) | 14.58 (11.92–26.63) | 6.45 (3.49–12.28) ** |
| Monocytes | 109.5 (66.49–124.5) | 165.5 (140.8–171.7) | 94.23 (89.53–96.72) | 94.52 (92.49–96.01) |
| Neutrophils | 1734 (990.6–2382) | 1489 (1038–1610) | 64.72 (44.09–73.20) | 48.25 (45.52–53.07) * |
| PD-1 | PD-L1 | TIM3 | OX40 | KIR | ||
|---|---|---|---|---|---|---|
| a CD4+ T cells | mCRPC | 32.21 (27.92–44.28) | 23.2 (17.58–29.15) | 8.58 (3.80–11.76) ** | ||
| HDs | 24.65 (21.45–32.36) | 17.35 (10.62–23.98) | 1.56 (1.09–3.73) | |||
| a CD8+ T cells | mCRPC | 44.56 (37.23–52.20) | 17.85 (12.29–24.5) | 0.29 (0.11–1.62) | 0.86 (0.31–3.77) | |
| HDs | 43.24 (30.2–51.49) | 12 (8.21–20.88) | 0.04 (0.025–0.15) | 1.08 (0.47–2.74) | ||
| a CD8low cells | mCRPC | 2.89 (0.82–5.49) | 10.86 (7.47–13.21) * | 3.17 (0.64–4.78) | 20.27 (8.56–25.44) * | |
| HDs | 5.69 (1.02–6.20) | 5.49 (3.61–9.51) | 2.01 (1.06–4.58) | 28.44 (25.36–30.53) | ||
| a B cells | mCRPC | 1.32 (0.09–3.46) | 7.39 (3.75–11.08) ** | 0.11 (0.01–0.20) | ||
| HDs | 0.47 (0.21–0.67) | 1.74 (1.31–3.16) | 0.1 (0.03–0.18) | |||
| a NK cells | mCRPC | 2.60 (2.33–4.47) | 9.69 (7.03–11.78) * | 4.89 (1.84–7.60) | 17.71 (8.77–26.15) | |
| HDs | 3.36 (1.82–14.5) | 5.91 (4.02–8.92) | 2.25 (1.80–6.2) | 19.79 (15.89–27.09) | ||
| Monocytes | mCRPC | 10.85 (7.47–17.95) | 0.29 (0.13–0.78) | |||
| HDs | 8.31 (5.84–9.16) | 0.2 (0.08–0.3) | ||||
| Neutrophils | mCRPC | 39.8 (22.9–51.87) | ||||
| HDs | 40.65 (30.4–47.58) |
| mCRPC | HD | |
|---|---|---|
| CD4± platelet/CD4+ T cells | 9.08 (7.41–10.62) | 9.81 (8.35–11.67) |
| CD8± platelet/CD8+ T cells | 8.26 (6.89–11.39) | 9.42 (8.04–10.76) |
| CD8low−platelet/ CD8low cells | 7.88 (6.53–9.13) | 9.14 (8.25–10.37) |
| B cells-platelet/B cells | 7.69 (6.22–9.62) | 9.5 (7.61–11.27) |
| NK cells-platelet/NK cells | 8.00 (7.54–9.44) | 11.19 (8.48–11.88) |
| Monocyte-platelet /Monocytes | 25.79 (18.03–34.68) | 14.24 (10.75–19.55) ** |
| Neutrophil-platelet/Neutrophils | 17.21 (11.34–20.54) | 12.1 (9.23–14.8) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cantó, E.; Anguera, G.; Jiménez, N.; Mellado, B.; Ramírez, O.; Mariscal, A.; Maroto, P.; Vidal, S. Association between the Immunophenotype of Peripheral Blood from mCRPC Patients and the Outcomes of Radium-223 Treatment. Diagnostics 2023, 13, 2222. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics13132222
Cantó E, Anguera G, Jiménez N, Mellado B, Ramírez O, Mariscal A, Maroto P, Vidal S. Association between the Immunophenotype of Peripheral Blood from mCRPC Patients and the Outcomes of Radium-223 Treatment. Diagnostics. 2023; 13(13):2222. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics13132222
Chicago/Turabian StyleCantó, Elisabet, Georgia Anguera, Natalia Jiménez, Begoña Mellado, Ona Ramírez, Anais Mariscal, Pablo Maroto, and Silvia Vidal. 2023. "Association between the Immunophenotype of Peripheral Blood from mCRPC Patients and the Outcomes of Radium-223 Treatment" Diagnostics 13, no. 13: 2222. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics13132222