
Computer-Based Diagnosis of Celiac Disease by Quantitative Processing of Duodenal Endoscopy Images

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
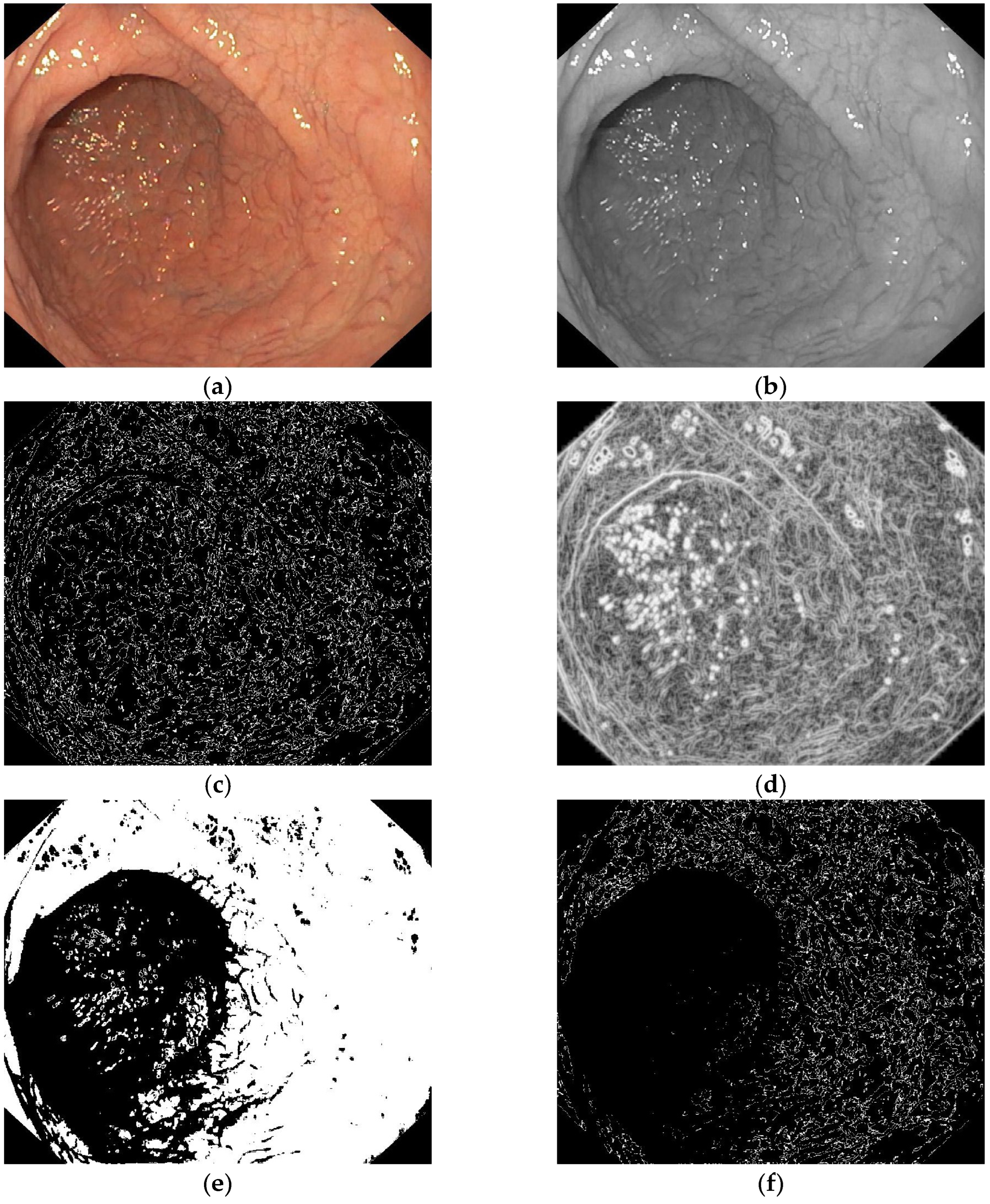
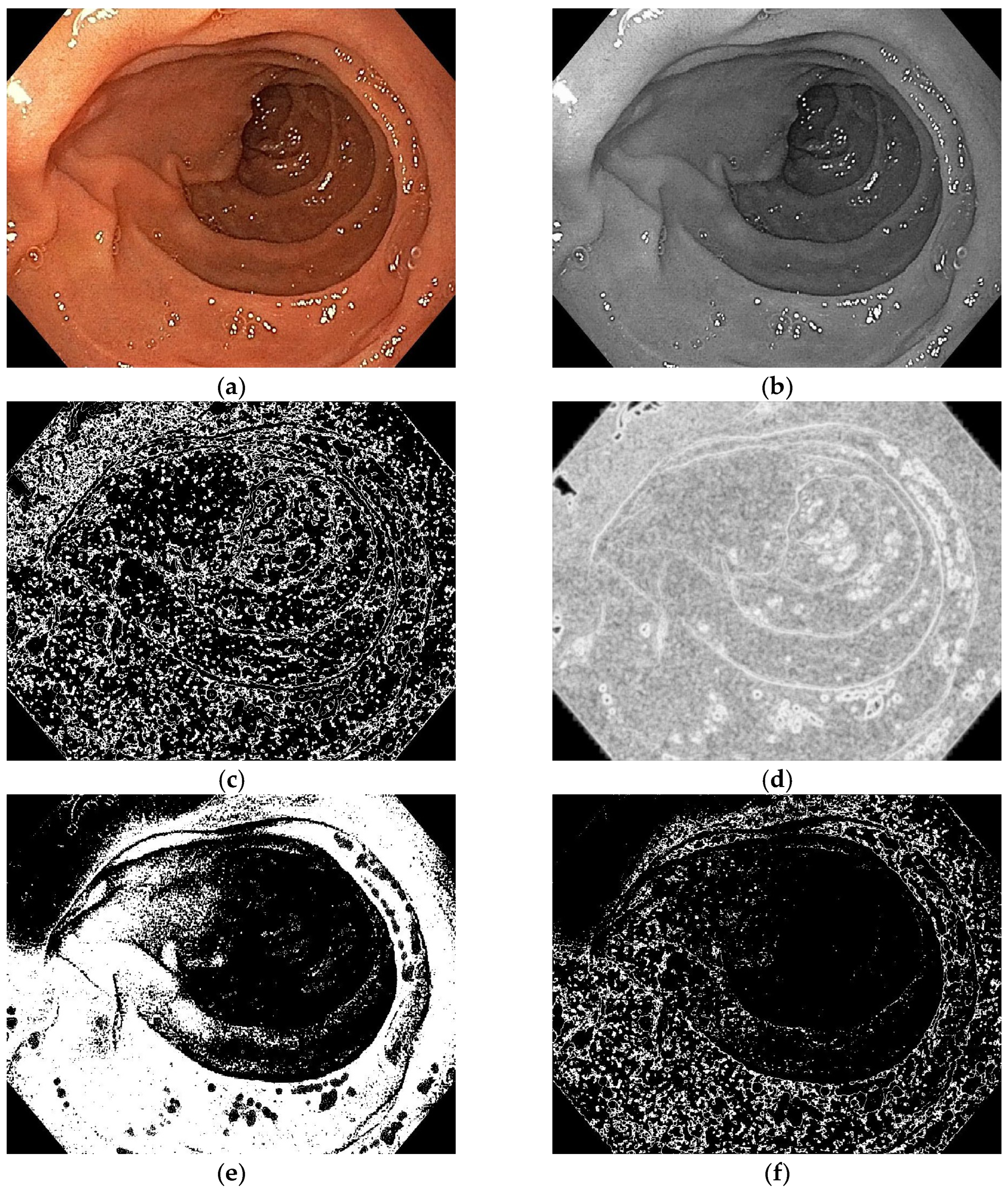
- Entropy filter applied on the gray level image;
- Binarization of the entropy-filtered image with high and low thresholds;
- Binarization of the gray level image using two high and low thresholds;
- Logic AND between binary images and dilatation;
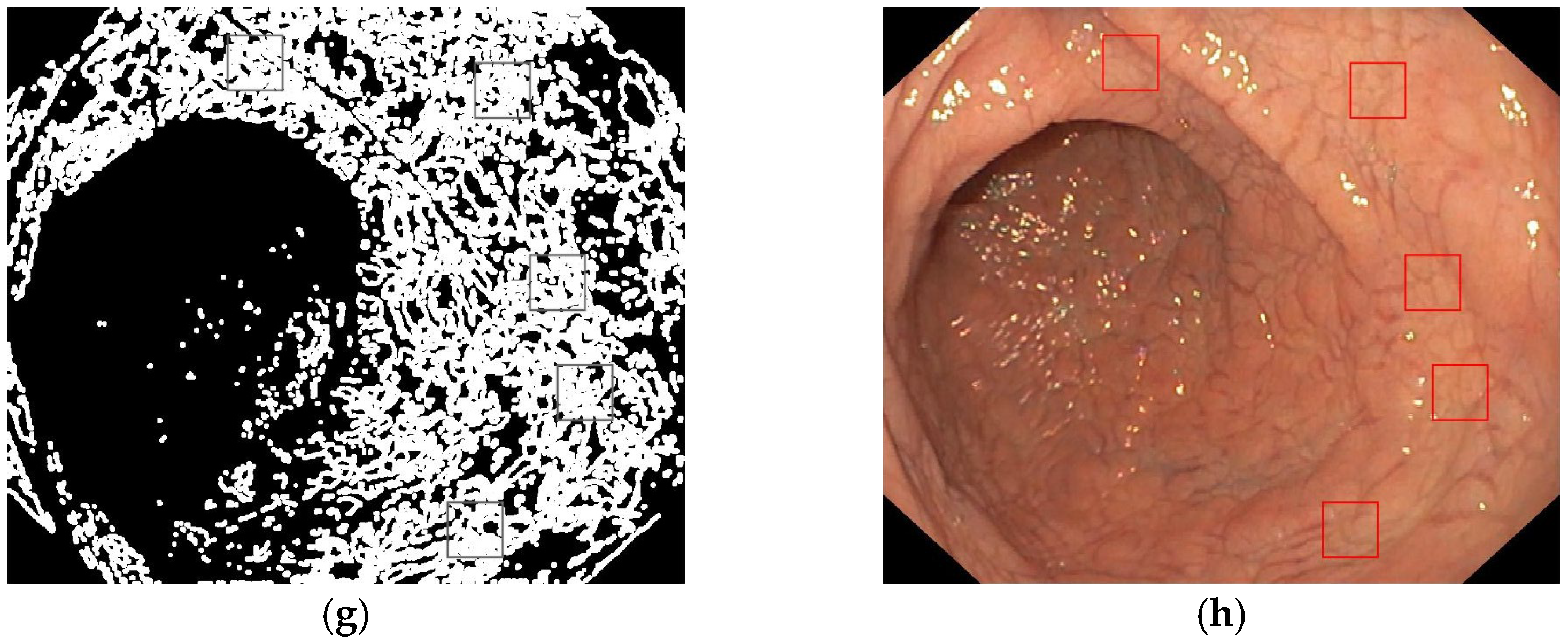
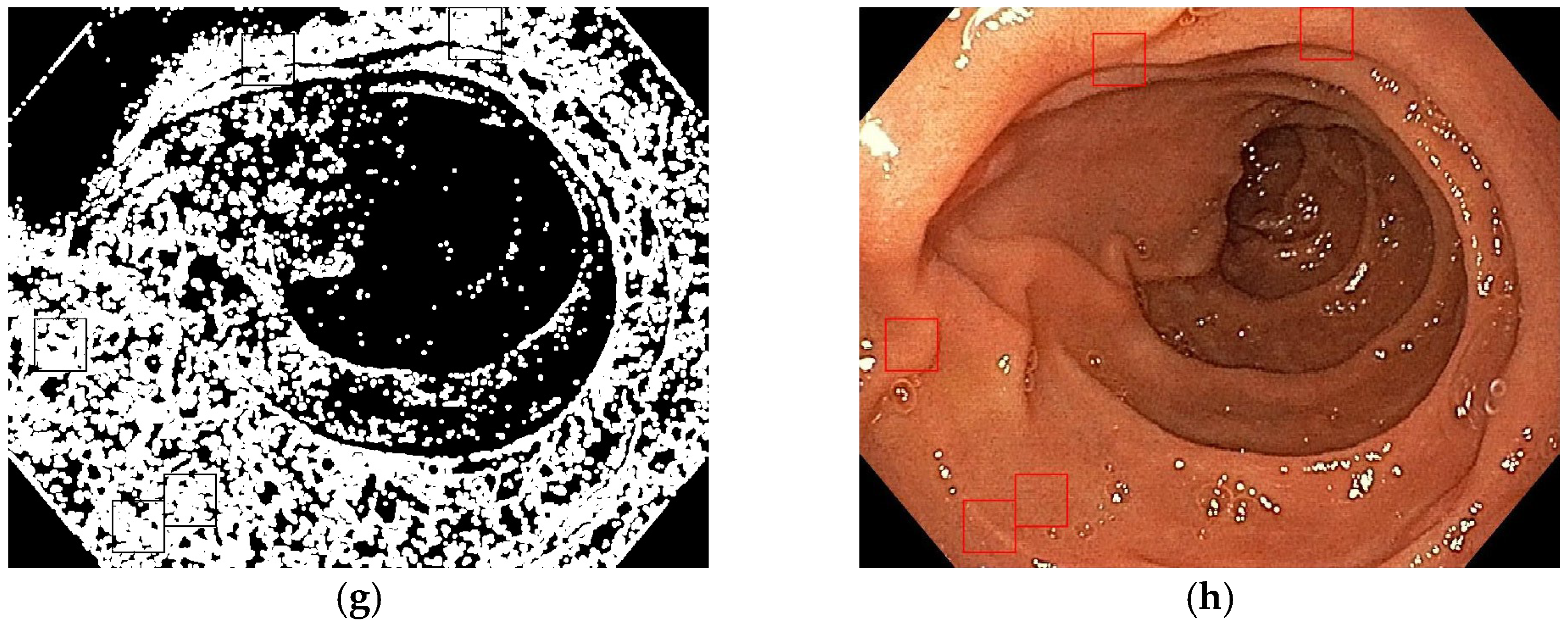
- Patches selection according to the final binary image and the gray level range.
- WKNN: K = 10, Euclidean distance, squared inverse distance weight;
- Boosted trees: AdaBoost ensemble method, 20 maximum splits, 30 learners, learning rate = 0.1;
- Bagged trees: bag ensemble method, 536 maximum splits, learning rate = 0.1.
- Sensitivity (True Positive Rate)—the probability of a positive test result, conditioned on the individual sample being a real positive in histological analysis;
- Accuracy (ACC)—the percentage of correct predictions (both true positives and true negatives according to histological analysis) of the total number of samples;
- Positive Predictive Value (PPV or Precision)—is the ratio between the true positives (TP) according to histological analysis and all positive instances (sum of true positives and false positives).
- Negative Predictive Value (NPV)—is the ratio between the true negatives (TN), using histology as reference, and all negative instances (sum of true negatives and false negatives).
3. Results
4. Discussion
Limits and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACC | Accuracy |
| Adam | Adaptive Moment Estimation |
| AI | Artificial Intelligence |
| CD | Celiac Disease |
| CNN | Convolutional Neural Network |
| DL | Deep Learning |
| FN | False Negative |
| FP | False Positive |
| ML | Machine Learning |
| NPV | Negative Predictive Value |
| PPV | Positive Predictive Value |
| SGD | Stochastic Gradient Descent |
| TN | True Negative |
| TP | True Positive |
| VA | Villous Atrophy |
| WKNN | Weighted K-Nearest Neighbors |
| WLE | White Light Endoscopy |
References
- Ludvigsson, J.F.; Card, T.R.; Kaukinen, K.; Bai, J.; Zingone, F.; Sanders, D.S.; A Murray, J. Screening for celiac disease in the general population and in high-risk groups. United Eur. Gastroenterol. J. 2015, 3, 106–120. [Google Scholar] [CrossRef]
- Singh, P.; Arora, A.; Strand, T.A.; Leffler, D.A.; Catassi, C.; Green, P.H.; Kelly, C.P.; Ahuja, V.; Makharia, G.K. Global Prevalence of Celiac Disease: Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2018, 16, 823–836.e2. [Google Scholar] [CrossRef] [PubMed]
- Al-Toma, A.; Volta, U.; Auricchio, R.; Castillejo, G.; Sanders, D.S.; Cellier, C.; Mulder, C.J.; Lundin, K.E.A. European Society for the Study of Coeliac Disease (ESsCD) guideline for coeliac disease and other gluten-related disorders. United Eur. Gastroenterol. J. 2019, 7, 583–613. [Google Scholar] [CrossRef] [PubMed]
- Husby, S.; Koletzko, S.; Korponay-Szabó, I.; Kurppa, K.; Mearin, M.L.; Ribes-Koninckx, C.; Shamir, R.; Troncone, R.; Auricchio, R.; Castillejo, G.; et al. European Society Paediatric Gastroenterology, Hepatology and Nutrition Guidelines for Diagnosing Coeliac Disease 2020. J. Pediatr. Gastroenterol. Nutr. 2020, 70, 141–156. [Google Scholar] [CrossRef] [PubMed]
- Penny, H.A.; Raju, S.A.; Lau, M.S.; Marks, L.J.; Baggus, E.M.; Bai, J.C.; Bassotti, G.; Bontkes, H.J.; Carroccio, A.; Danciu, M.; et al. Accuracy of a no-biopsy approach for the diagnosis of coeliac disease across different adult cohorts. Gut 2021, 70, 876–883. [Google Scholar] [CrossRef] [PubMed]
- Shiha, M.G.; Penny, H.A.; Sanders, D.S. Is There a Need to Undertake Conventional Gastroscopy and Biopsy When Making the Diagnosis of Coeliac Disease in Adults? J. Clin. Gastroenterol. 2023, 57, 139–142. [Google Scholar] [CrossRef] [PubMed]
- Schiepatti, A.; Savioli, J.; Vernero, M.; de Andreis, F.B.; Perfetti, L.; Meriggi, A.; Biagi, F. Pitfalls in the Diagnosis of Coeliac Disease and Gluten-Related Disorders. Nutrients 2020, 12, 1711. [Google Scholar] [CrossRef] [PubMed]
- Enache, I.; Balaban, D.V.; Vasilescu, F.; Jurcut, C.; Ionita-Radu, F.; Popp, A.; Matei, D.; Jinga, M. Upper Gastrointestinal Tract Associated Lesions in Patients with Newly Diagnosed Celiac Disease. Gastroenterol. Insights 2022, 13, 77–86. [Google Scholar] [CrossRef]
- Balaban, D.V.; Popp, A.; Vasilescu, F.; Haidautu, D.; Purcarea, R.M.; Jinga, M. Diagnostic yield of endoscopic markers for celiac disease. J. Med. Life 2015, 8, 452–457. [Google Scholar]
- Mauriño, E.; Bai, J.C. Endoscopic markers of celiac disease. Am. J. Gastroenterol. 2002, 97, 760–761. [Google Scholar] [CrossRef]
- Lebwohl, B.; Bhagat, G.; Markoff, S.; Lewis, S.K.; Smukalla, S.; Neugut, A.I.; Green, P.H. Prior endoscopy in patients with newly diagnosed celiac disease: A missed opportunity? Dig. Dis. Sci. 2013, 58, 1293–1298. [Google Scholar] [CrossRef] [PubMed]
- Nazarian, S.; Glover, B.; Ashrafian, H.; Darzi, A.; Teare, J. Diagnostic Accuracy of Artificial Intelligence and Computer-Aided Diagnosis for the Detection and Characterization of Colorectal Polyps: Systematic Review and Meta-analysis. J. Med. Internet Res. 2021, 23, e27370. [Google Scholar] [CrossRef] [PubMed]
- Molder, A.; Balaban, D.V.; Jinga, M.; Molder, C.C. Current Evidence on Computer-Aided Diagnosis of Celiac Disease: Systematic Review. Front. Pharmacol. 2020, 11, 341. [Google Scholar] [CrossRef] [PubMed]
- Gimeno-García, A.Z.; Hernández-Pérez, A.; Nicolás-Pérez, D.; Hernández-Guerra, M. Artificial Intelligence Applied to Colonoscopy: Is It Time to Take a Step Forward? Cancers 2023, 15, 2193. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.L.; Chinnaratha, M.A.; Woodman, R.; Martin, R.; Chen, H.-T.; Carneiro, G.; Singh, R. Diagnostic Accuracy of Artificial Intelligence (AI) to Detect Early Neoplasia in Barrett’s Esophagus: A Non-comparative Systematic Review and Meta-Analysis. Front. Med. 2022, 9, 890720. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Wei, N.; Wang, K.; Tao, T.; Yu, F.; Lv, B. Diagnostic value of artificial intelligence-assisted endoscopy for chronic atrophic gastritis: A systematic review and meta-analysis. Front. Med. 2023, 10, 1134980. [Google Scholar] [CrossRef]
- Koleth, G.; Emmanue, J.; Spadaccini, M.; Mascagni, P.; Khalaf, K.; Mori, Y.; Antonelli, G.; Maselli, R.; Carrara, S.; Galtieri, P.A.; et al. Artificial intelligence in gastroenterology: Where are we heading? Endosc. Int. Open 2022, 10, E1474–E1480. [Google Scholar] [CrossRef] [PubMed]
- Balaban, D.V.; Jinga, M. Digital histology in celiac disease: A practice changer. Artif. Intell. Gastroenterol. 2020, 1, 1–4. [Google Scholar] [CrossRef]
- Oberhuber, G.; Granditsch, G.; Vogelsang, H. The histopathology of coeliac disease: Time for a standardized report scheme for pathologists. Eur. J. Gastroenterol. Hepatol. 1999, 11, 1185–1194. [Google Scholar] [CrossRef]
- Rubio-Tapia, A.; Hill, I.D.; Kelly, C.P.; Calderwood, A.H.; Murray, J.A. American College of Gastroenterology. ACG clinical guidelines: Diagnosis and management of celiac disease. Am. J. Gastroenterol. 2013, 108, 656–676, quiz 677. [Google Scholar] [CrossRef]
- Liu, X.; Faes, L.; Kale, A.U.; Wagner, S.K.; Fu, D.J.; Bruynseels, A.; Mahendiran, T.; Moraes, G.; Shamdas, M.; Kern, C.; et al. A comparison of deep learning performance against health-care professionals in detecting diseases from medical imaging: A systematic review and meta-analysis. Lancet Digit Health 2019, 1, e271–e297. [Google Scholar] [CrossRef] [PubMed]
- Topol, E.J. High-performance medicine: The convergence of human and artificial intelligence. Nat. Med. 2019, 25, 44–56. [Google Scholar] [CrossRef] [PubMed]
- Sendak, M.P.; D’Arcy, J.; Kashyap, S.; Gao, M.; Nichols, M.; Corey, K.; Ratliff, W.; Balu, S. A Path for Translation of Machine Learning Products into Healthcare Delivery. EMJ. 27 January 2020. Available online: https://www.emjreviews.com/innovations/article/a-path-for-translation-of-machine-learning-products-into-healthcare-delivery/ (accessed on 28 December 2022).
- Hegenbart, S.; Uhl, A.; Vécsei, A. Impact of endoscopic image degradations on LBP based features using one-class SVM for classification of celiac disease. In Proceedings of the 2011 7th International Symposium on Image and Signal Processing and Analysis (ISPA), Dubrovnik, Croatia, 4–6 September 2011; pp. 715–720. [Google Scholar]
- Hegenbart, S.; Uhl, A.; Vécsei, A. Impact of Histogram Subset Selection on Classification using Multi-scale LBP-Operators. In Proceedings of the Bildverarbeitung für die Medizin, Lübeck, Germany, 20–22 March 2011. [Google Scholar]
- Wimmer, G.; Uhl, A.; Vécsei, A. Evaluation of domain specific data augmentation techniques for the classification of celiac disease using endoscopic imagery. In Proceedings of the 2017 IEEE 19th International Workshop on Multimedia Signal Processing (MMSP), Luton, UK, 16–18 October 2017; pp. 1–6. [Google Scholar]
- Burman, P. A comparative study of ordinary cross-validation, v-fold cross-validation and the repeated learning-testing methods. Biometrika 1989, 76, 503–514. [Google Scholar] [CrossRef]
- McNeish, A.S.; Harms, H.K.; Rey, J.; Shmerling, D.H.; Visakorpi, J.K.; Walker-Smith, J.A. The diagnosis of coeliac disease. A commentary on the current practices of members of the European Society for Paediatric Gastroenterology and Nutrition (ESPGAN). Arch. Dis. Child. 1979, 54, 783–786. [Google Scholar] [CrossRef] [PubMed]
- Rubio-Tapia, A.; Hill, I.D.; Semrad, C.; Kelly, C.P.; Lebwohl, B. American College of Gastroenterology Guidelines Update: Diagnosis and Management of Celiac Disease. Am. J. Gastroenterol. 2023, 118, 59–76. [Google Scholar] [CrossRef] [PubMed]
- Rostami, K.; Marsh, M.N.; Johnson, M.W.; Mohaghegh, H.; Heal, C.; Holmes, G.; Ensari, A.; Aldulaimi, D.; Bancel, B.; Bassotti, G.; et al. ROC-king onwards: Intraepithelial lymphocyte counts, distribution & role in coeliac disease mucosal interpretation. Gut 2017, 66, 2080–2086. [Google Scholar]
- Joelson, A.M.; Geller, M.G.; Zylberberg, H.M.; Green, P.H.R.; Lebwohl, B. Numbers and Features of Patients With a Diagnosis of Celiac Disease Without Duodenal Biopsy, Based on a National Survey. Clin. Gastroenterol. Hepatol. 2019, 17, 1089–1097.e2. [Google Scholar] [CrossRef]
- Bisschops, R.; Areia, M.; Coron, E.; Dobru, D.; Kaskas, B.; Kuvaev, R.; Pech, O.; Ragunath, K.; Weusten, B.; Familiari, P.; et al. Performance measures for upper gastrointestinal endoscopy: A European Society of Gastrointestinal Endoscopy (ESGE) Quality Improvement Initiative. Endoscopy 2016, 48, 843–864. [Google Scholar] [CrossRef]
- Beg, S.; Ragunath, K.; Wyman, A.; Banks, M.; Trudgill, N.; Pritchard, M.D.; Riley, S.; Anderson, J.; Griffiths, H.; Bhandari, P.; et al. Quality standards in upper gastrointestinal endoscopy: A position statement of the British Society of Gastroenterology (BSG) and Association of Upper Gastrointestinal Surgeons of Great Britain and Ireland (AUGIS). Gut 2017, 66, 1886–1899. [Google Scholar] [CrossRef]
- Banerjee, R.; Reddy, D.N. High-resolution narrow-band imaging can identify patchy atrophy in celiac disease: Targeted biopsy can increase diagnostic yield. Gastrointest. Endosc. 2009, 69, 984–985. [Google Scholar] [CrossRef]
- Doyev, R.; Cohen, S.; Ben-Tov, A.; Weintraub, Y.; Amir, A.; Galai, T.; Moran-Lev, H.; Yerushalmy-Feler, A. Ultra-short Celiac Disease Is a Distinct and Milder Phenotype of the Disease in Children. Dig. Dis. Sci. 2019, 64, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Mooney, P.D.; Kurien, M.; Evans, K.E.; Rosario, E.; Cross, S.S.; Vergani, P.; Hadjivassiliou, M.; Murray, J.A.; Sanders, D.S. Clinical and Immunologic Features of Ultra-Short Celiac Disease. Gastroenterology 2016, 150, 1125–1134. [Google Scholar] [CrossRef] [PubMed]
- Oberhuber, G.; Vogelsang, H. Clinical and Immunologic Features of Ultra-Short Celiac Disease. Gastroenterology 2016, 151, 773. [Google Scholar] [CrossRef]
- Neumann, H.; Kreft, A.; Sivanathan, V.; Rahman, F.; Galle, P.R. Evaluation of novel LCI CAD EYE system for real time detection of colon polyps. PLoS ONE 2021, 16, e0255955. [Google Scholar] [CrossRef] [PubMed]
- Kurien, M.; Mooney, P.D.; Cross, S.S.; Sanders, D.S. Bulb Biopsy in Adult Celiac Disease: Pros Outweigh the Cons? Am. J. Gastroenterol. 2016, 111, 1205–1206. [Google Scholar] [CrossRef] [PubMed]
- McCarty, T.R.; O’Brien, C.R.; Gremida, A.; Ling, C.; Rustagi, T. Efficacy of duodenal bulb biopsy for diagnosis of celiac disease: A systematic review and meta-analysis. Endosc. Int. Open 2018, 6, E1369–E1378. [Google Scholar] [CrossRef] [PubMed]
- Taavela, J.; Popp, A.; Korponay-Szabo, I.R.; Ene, A.; Vornanen, M.; Saavalainen, P.; Lähdeaho, M.-L.; Ruuska, T.; Laurila, K.; Parvan, A.; et al. A Prospective Study on the Usefulness of Duodenal Bulb Biopsies in Celiac Disease Diagnosis in Children: Urging Caution. Am. J. Gastroenterol. 2016, 111, 124–133. [Google Scholar] [CrossRef] [PubMed]
- Ianiro, G.; Gasbarrini, A.; Cammarota, G. Endoscopic tools for the diagnosis and evaluation of celiac disease. World J Gastroenterol. 2013, 19, 8562–8570. [Google Scholar] [CrossRef]
- Ianiro, G.; Bibbò, S.; Pecere, S.; Gasbarrini, A.; Cammarota, G. Current technologies for the endoscopic assessment of duodenal villous pattern in celiac disease. Comput. Biol. Med. 2015, 65, 308–314. [Google Scholar] [CrossRef]
- Schiepatti, A.; Sanders, D.S.; Baiardi, P.; Caio, G.; Ciacci, C.; Kaukinen, K.; Lebwohl, B.; Leffler, D.; Malamut, G.; Murray, J.A.; et al. Nomenclature and diagnosis of seronegative coeliac disease and chronic non-coeliac enteropathies in adults: The Paris consensus. Gut 2022, 71, 2218–2225. [Google Scholar] [CrossRef]
- Leonard, M.M.; Lebwohl, B.; Rubio-Tapia, A.; Biagi, F. AGA Clinical Practice Update on the Evaluation and Management of Seronegative Enteropathies: Expert Review. Gastroenterology 2021, 160, 437–444. [Google Scholar] [CrossRef]
- Manfredi, G.; Bertè, R.; Iiritano, E.; Alicante, S.; Londoni, C.; Brambilla, G.; Romeo, S.; Menozzi, F.; Griffanti, P.; Brandi, G.; et al. Premedication with simethicone and N-acetylcysteine for improving mucosal visibility during upper gastrointestinal endoscopy in a Western population. Endosc. Int. Open 2021, 9, E190–E194. [Google Scholar] [CrossRef]
- Krishnamurthy, V.; Joseph, A.; Venkataraman, S.; Kurian, G. Simethicone and N-acetyl cysteine combination as premedication before esophagogastroduodenoscopy: Double-blind randomized controlled trial. Endosc. Int. Open 2022, 10, E585–E592. [Google Scholar] [CrossRef]
- Varoquaux, G.; Cheplygina, V. Machine learning for medical imaging: Methodological failures and recommendations for the future. NPJ Digit. Med. 2022, 5, 48. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Atrophy of mucosa with prominent submucosal vascular pattern; Mucosal fissures or grooves, with mosaic or “cracked-mud” appearance; Nodularity of the mucosa; Scalloping of Kerckring folds; Reduction or loss of folds. |
| Class | Samples | Images | Patches | WKNN | Boosted Trees | Bagged Trees | CNN |
|---|---|---|---|---|---|---|---|
| CD | 18 | 66 | 477 | 139/143 | 135/143 | 141/143 | 142/143 |
| Control | 16 | 16 | 90 | 14/27 | 13/27 | 13/27 | 25/27 |
| Algorithm | Technique | Sensitivity | Accuracy | PPV | NPV |
|---|---|---|---|---|---|
| ML | WKNN | 97.20% | 90.00% | 91.45% | 77.78% |
| Boosted trees | 94.41% | 87.06% | 90.60% | 61.90% | |
| Bagged trees | 98.60% | 90.59% | 90.97% | 86.67% | |
| DL | CNN | 99.30% | 98.24% | 98.61% | 96.15% |
| Infectious (Giardia, Helicobacter pylori, Whipple’s disease, viruses); Common variable immune deficiency; Autoimmune enteropathy; Inflammatory bowel disease; Eosinophilic gastroenteritis; Peptic duodenitis; Small intestinal bacterial overgrowth; Drug-induced enteropathy (olmesartan, non-steroidal anti-inflammatory drugs). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Molder, A.; Balaban, D.V.; Molder, C.-C.; Jinga, M.; Robin, A. Computer-Based Diagnosis of Celiac Disease by Quantitative Processing of Duodenal Endoscopy Images. Diagnostics 2023, 13, 2780. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics13172780
Molder A, Balaban DV, Molder C-C, Jinga M, Robin A. Computer-Based Diagnosis of Celiac Disease by Quantitative Processing of Duodenal Endoscopy Images. Diagnostics. 2023; 13(17):2780. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics13172780
Chicago/Turabian StyleMolder, Adriana, Daniel Vasile Balaban, Cristian-Constantin Molder, Mariana Jinga, and Antonin Robin. 2023. "Computer-Based Diagnosis of Celiac Disease by Quantitative Processing of Duodenal Endoscopy Images" Diagnostics 13, no. 17: 2780. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics13172780