Smartphone Application with Virtual Reality Goggles for the Reliable and Valid Measurement of Active Craniocervical Range of Motion

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
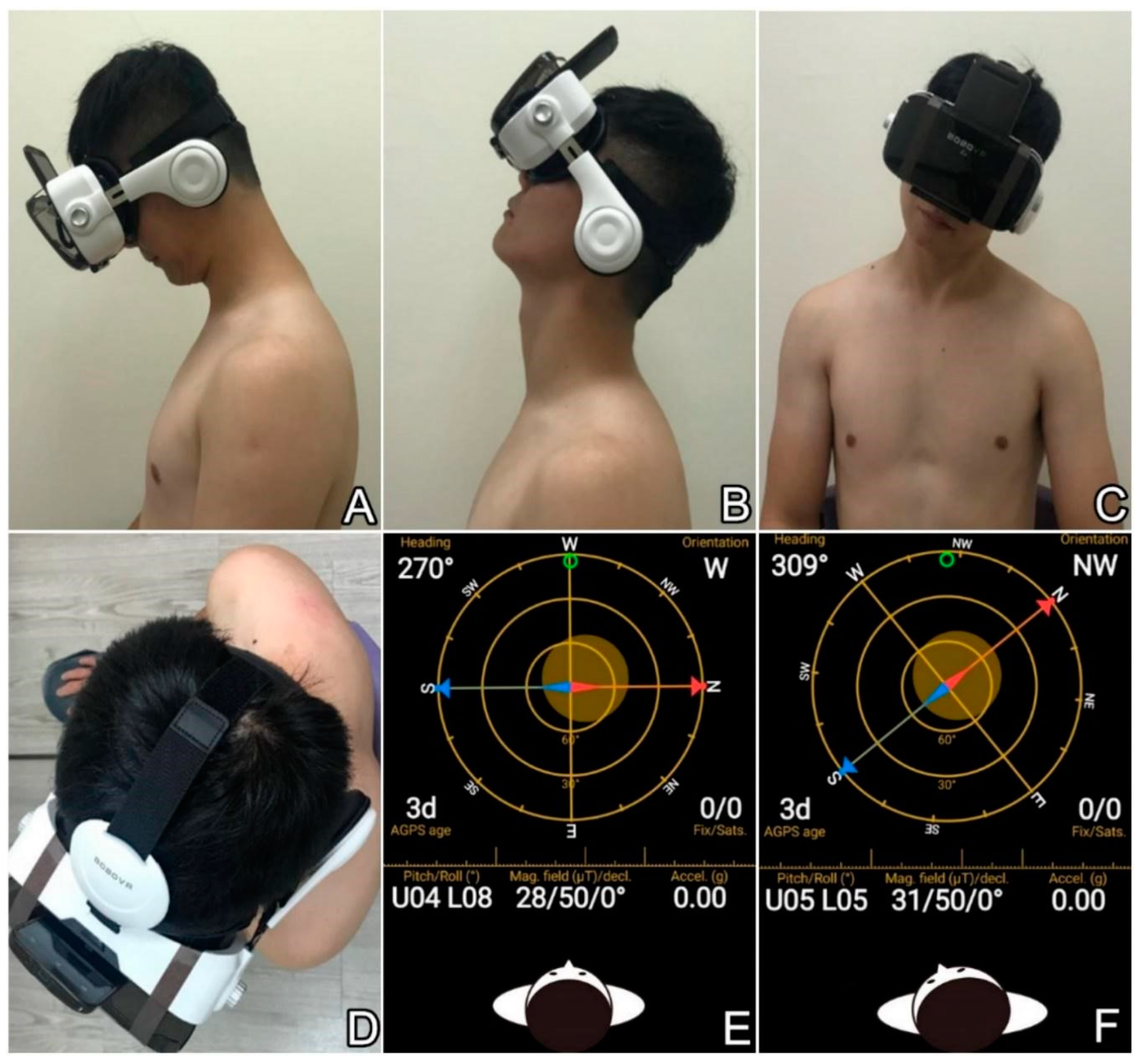
2.2. Hybrid Device for Evaluation of Cervical Range of Motion
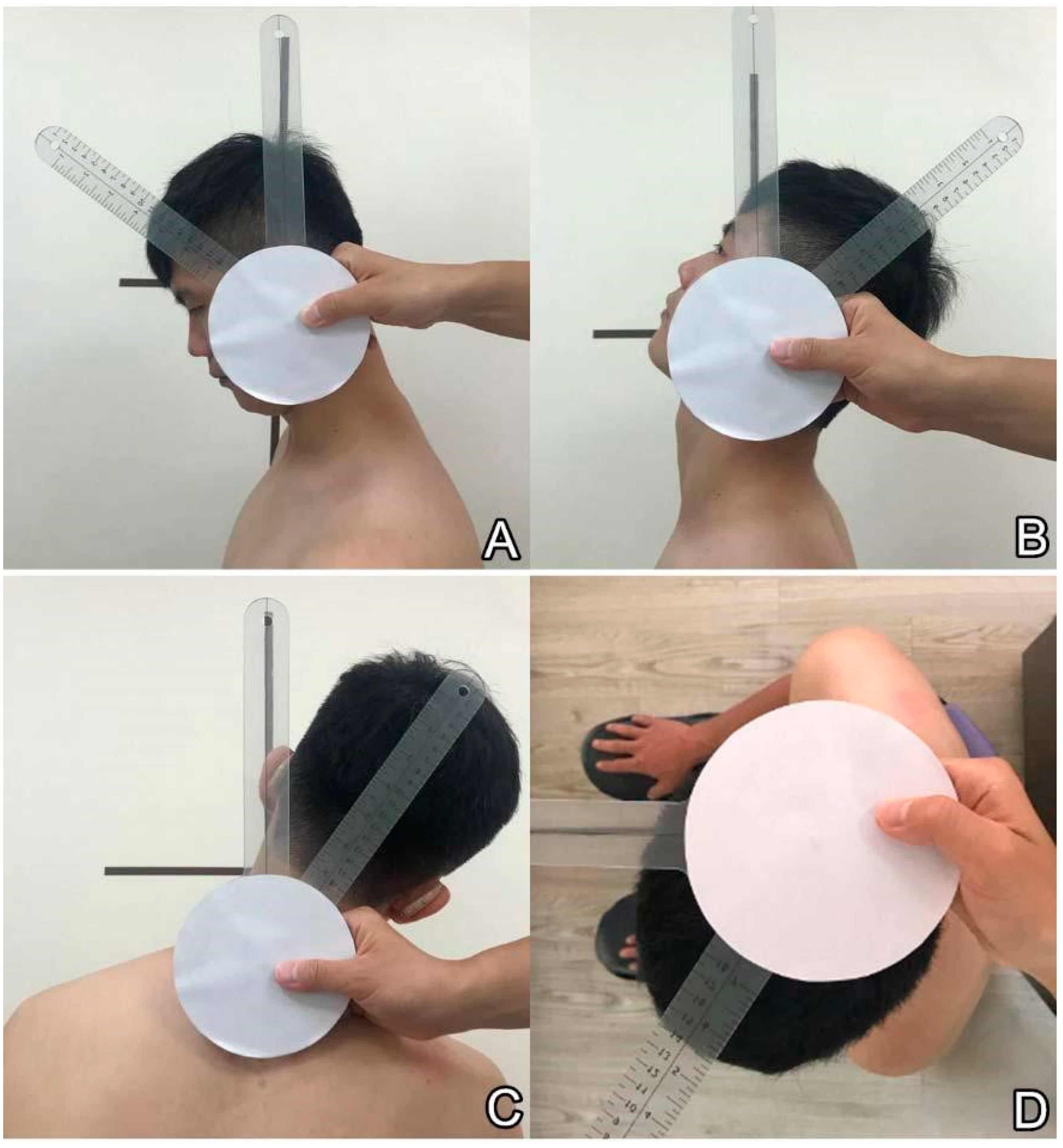
2.3. Universal Goniometer for Assessment of Cervical Range of Motion
2.4. Flow of Measurement of Craniocervical Range
2.5. Sample Size Estimation
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hoy, D.G.; Protani, M.; De, R.; Buchbinder, R. The epidemiology of neck pain. Best Pract. Res. Clin. Rheumatol. 2010, 24, 783–792. [Google Scholar] [CrossRef] [PubMed]
- Mejuto-Vazquez, M.J.; Salom-Moreno, J.; Ortega-Santiago, R.; Truyols-Dominguez, S.; Fernandez-de-Las-Penas, C. Short-term changes in neck pain, widespread pressure pain sensitivity, and cervical range of motion after the application of trigger point dry needling in patients with acute mechanical neck pain: A randomized clinical trial. J. Orthop. Sports Phys. Ther. 2014, 44, 252–260. [Google Scholar] [CrossRef] [PubMed]
- Ris, I.; Barbero, M.; Falla, D.; Larsen, M.H.; Kraft, M.N.; Søgaard, K.; Juul-Kristensen, B. Pain extent is more strongly associated with disability, psychological factors, and neck muscle function in people with non-traumatic versus traumatic chronic neck pain: A cross sectional study. Eur. J. Phys. Rehabil. Med. 2019, 55, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Hush, J.M.; Maher, C.G.; Refshauge, K.M. Risk factors for neck pain in office workers: A prospective study. BMC Musculoskelet. Disord. 2006, 7, 81. [Google Scholar] [CrossRef] [PubMed]
- Kauppi, M.J.; Barcelos, A.; da Silva, J.A. Cervical complications of rheumatoid arthritis. Ann. Rheum. Dis. 2005, 64, 355–358. [Google Scholar] [CrossRef] [PubMed]
- Farooq, M.N.; Mohseni Bandpei, M.A.; Ali, M.; Khan, G.A. Reliability of the universal goniometer for assessing active cervical range of motion in asymptomatic healthy persons. Pak. J. Med. Sci. 2016, 32, 457–461. [Google Scholar] [CrossRef] [PubMed]
- De Koning, C.H.; van den Heuvel, S.P.; Staal, J.B.; Smits-Engelsman, B.C.; Hendriks, E.J. Clinimetric evaluation of active range of motion measures in patients with non-specific neck pain: A systematic review. Eur. Spine J. 2008, 17, 905–921. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, S.; Allison, G.T.; Singer, K.P. Reliability of the spin-T cervical goniometer in measuring cervical range of motion in an asymptomatic Indian population. J. Manipulative. Physiol. Ther. 2005, 28, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Maksymowych, W.P.; Mallon, C.; Richardson, R.; Conner-Spady, B.; Jauregui, E.; Chung, C.; Zappala, L.; Pile, K.; Russell, A.S. Development and validation of a simple tape-based measurement tool for recording cervical rotation in patients with ankylosing spondylitis: Comparison with a goniometer-based approach. J. Rheumatol. 2006, 33, 2242–2249. [Google Scholar]
- Piva, S.R.; Erhard, R.E.; Childs, J.D.; Browder, D.A. Inter-tester reliability of passive intervertebral and active movements of the cervical spine. Man. Ther. 2006, 11, 321–330. [Google Scholar] [CrossRef]
- Prushansky, T.; Deryi, O.; Jabarreen, B. Reproducibility and validity of digital inclinometry for measuring cervical range of motion in normal subjects. Physiother. Res. Int. 2010, 15, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Rondoni, A.; Rossettini, G.; Ristori, D.; Gallo, F.; Strobe, M.; Giaretta, F.; Battistin, A.; Testa, M. Intrarater and Inter-rater Reliability of Active Cervical Range of Motion in Patients With Nonspecific Neck Pain Measured With Technological and Common Use Devices: A Systematic Review With Meta-regression. J. Manipulative. Physiol. Ther. 2017, 40, 597–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santos, C.; Pauchard, N.; Guilloteau, A. Reliability assessment of measuring active wrist pronation and supination range of motion with a smartphone. Hand. Surg. Rehabil. 2017, 36, 338–345. [Google Scholar] [CrossRef] [PubMed]
- Pourahmadi, M.R.; Ebrahimi Takamjani, I.; Sarrafzadeh, J.; Bahramian, M.; Mohseni-Bandpei, M.A.; Rajabzadeh, F.; Taghipour, M. Reliability and concurrent validity of a new iPhone((R)) goniometric application for measuring active wrist range of motion: A cross-sectional study in asymptomatic subjects. J. Anat. 2017, 230, 484–495. [Google Scholar] [CrossRef]
- Tousignant-Laflamme, Y.; Boutin, N.; Dion, A.M.; Vallee, C.A. Reliability and criterion validity of two applications of the iPhone to measure cervical range of motion in healthy participants. J. Neuroeng. Rehabil. 2013, 10, 69. [Google Scholar] [CrossRef]
- Quek, J.; Brauer, S.G.; Treleaven, J.; Pua, Y.H.; Mentiplay, B.; Clark, R.A. Validity and intra-rater reliability of an android phone application to measure cervical range-of-motion. J. Neuroeng. Rehabil. 2014, 11, 65. [Google Scholar] [CrossRef] [PubMed]
- Pourahmadi, M.R.; Bagheri, R.; Taghipour, M.; Takamjani, I.E.; Sarrafzadeh, J.; Mohseni-Bandpei, M.A. A new iPhone application for measuring active craniocervical range of motion in patients with non-specific neck pain: A reliability and validity study. Spine J. 2018, 18, 447–457. [Google Scholar] [CrossRef]
- Ullucci, P.A.; Jr Tudini, F.; Moran, M.F. Reliability of Smartphone Inclinometry to Measure Upper Cervical Range of Motion. J. Sport Rehabil. 2018, 1–12. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Kyrola, K.K.; Salme, J.; Tuija, J.; Tero, I.; Eero, K.; Arja, H. Intra- and Interrater Reliability of Sagittal Spinopelvic Parameters on Full-Spine Radiographs in Adults With Symptomatic Spinal Disorders. Neurospine. 2018, 15, 175–181. [Google Scholar] [CrossRef]
- Giavarina, D. Understanding Bland Altman analysis. Biochem. Med. 2015, 25, 141–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stenneberg, M.S.; Busstra, H.; Eskes, M.; van Trijffel, E.; Cattrysse, E.; Scholten-Peeters, G.G.M.; de Bie, R.A. Concurrent validity and interrater reliability of a new smartphone application to assess 3D active cervical range of motion in patients with neck pain. Musculoskelet. Sci. Pract. 2018, 34, 59–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, H.; Zhai, X.; Gao, Z.; Lu, T.; Tian, Q.; Li, H.; He, X. Reliability and validity of a Coda Motion 3-D Analysis system for measuring cervical range of motion in healthy subjects. J. Electromyogr. Kinesiol. 2018, 38, 56–66. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Rater First Evaluation in Degrees (95% CI) | First Rater Second Evaluation in Degrees (95% CI) | Second Rater First Evaluation in Degrees (95% CI) | Intra-Rater Mean Difference in Degrees (95% CI) | p Value | Inter-Rater Mean Difference in Degrees (95% CI) | p Value | |
|---|---|---|---|---|---|---|---|
| Flexion | 41.80 (37.70 to 45.90) | 41.63 (37.78 to 45.47) | 41.46 (37.58 to 45.34) | −0.17 (−1.23 to 0.89) | 0.748 | −0.34 (−1.14 to 0.46) | 0.397 |
| Extension | 51.48 (47.56 to 55.40) | 50.87 (47.39 to 54.36) | 52.09 (48.36 to 55.83) | −0.60 (−1.72 to 0.50) | 0.275 | 0.60 (−0.55 to 1.77) | 0.296 |
| Side-bending to right | 34.51 (32.78 to 36.23) | 33.75 (31.78 to 35.72) | 34.09 (32.12 to 36.06) | −0.75 (−1.47 to −0.04) | 0.038 * | −0.41 (−1.32 to 0.49) | 0.360 |
| Side-bending to left | 31.34 (29.48 to 33.19) | 31.53 (29.59 to 33.47) | 32.31 (30.34 to 34.29) | 0.19 (−0.46 to 0.85) | 0.555 | 0.97 (0.26 to 1.68) | 0.008 * |
| Rotating to right | 50.80 (48.16 to 53.44) | 50.56 (47.96 to 53.16) | 48.19 (45.62 to 50.76) | −0.24 (−0.98 to 0.49) | 0.510 | −2.60 (−5.95 to 0.73) | 0.122 |
| Rotating to left | 47.82 (45.51 to 50.14) | 48.90 (46.43 to 51.37) | 48.19 (45.62 to 50.76) | 1.07 (0.18 to 1.96) | 0.019 * | 0.36 (−0.36 to 1.09) | 0.314 |
| Intra-Rater ICC (95% CI) | Intra-Rater SEM (Degrees) | Intra-Rater MDC (Degrees) | Inter-Rater ICC (95% CI) | Inter-Rater SEM (Degrees) | Inter-Rater MDC (Degrees) | |
|---|---|---|---|---|---|---|
| Flexion | 0.963 (0.933 to 0.980) | 2.68 | 7.42 | 0.979 (0.962 to 0.989) | 1.81 | 5.01 |
| Extension | 0.954 (0.916 to 0.975) | 2.50 | 6.92 | 0.953 (0.914 to 0.975) | 2.61 | 7.24 |
| Side-bending to right | 0.925 (0.864 to 0.959) | 1.60 | 4.44 | 0.880 (0.786 to 0.934) | 2.03 | 5.63 |
| Side-bending to left | 0.939 (0.888 to 0.967) | 1.48 | 4.12 | 0.931 (0.875 to 0.963) | 1.59 | 4.39 |
| Rotating to right | 0.959 (0.925 to 0.978) | 1.66 | 4.61 | 0.942 (0.895 to 0.969) | 1.96 | 5.44 |
| Rotating to left | 0.931 (0.874 to 0.962) | 1.99 | 5.52 | 0.956 (0.919 to 0.976) | 1.63 | 4.51 |
| First Rater First Evaluation in Degrees by the Hybrid Device (95% CI) | First Rater First Evaluation in Degrees by the Universal Goniometer (95% CI) | Between-Device Mean Difference in Degrees (95% CI) | p Value | Correlation Coefficient r Value (95% CI) | p Value | Coefficient of Repeatability (Degrees) | |
|---|---|---|---|---|---|---|---|
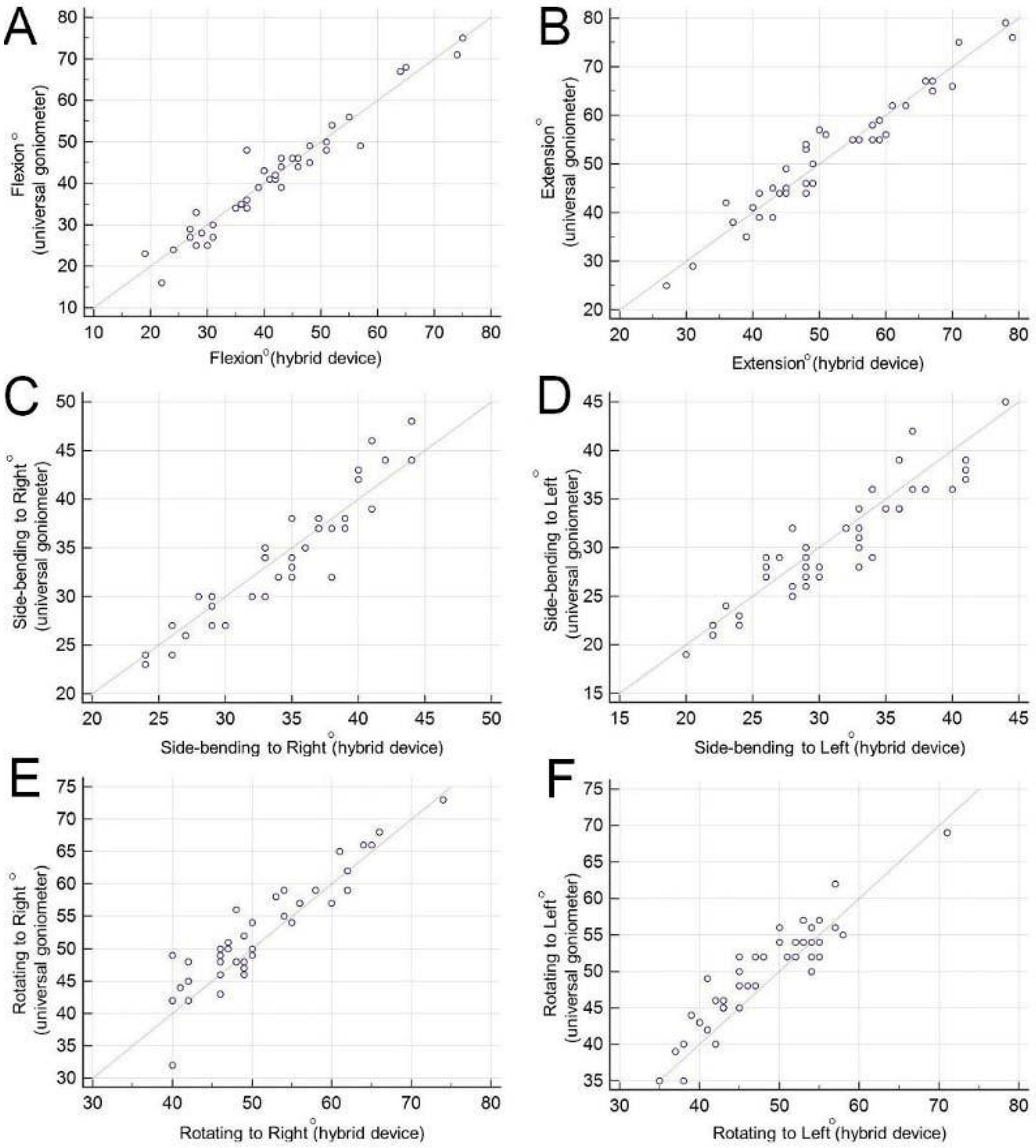
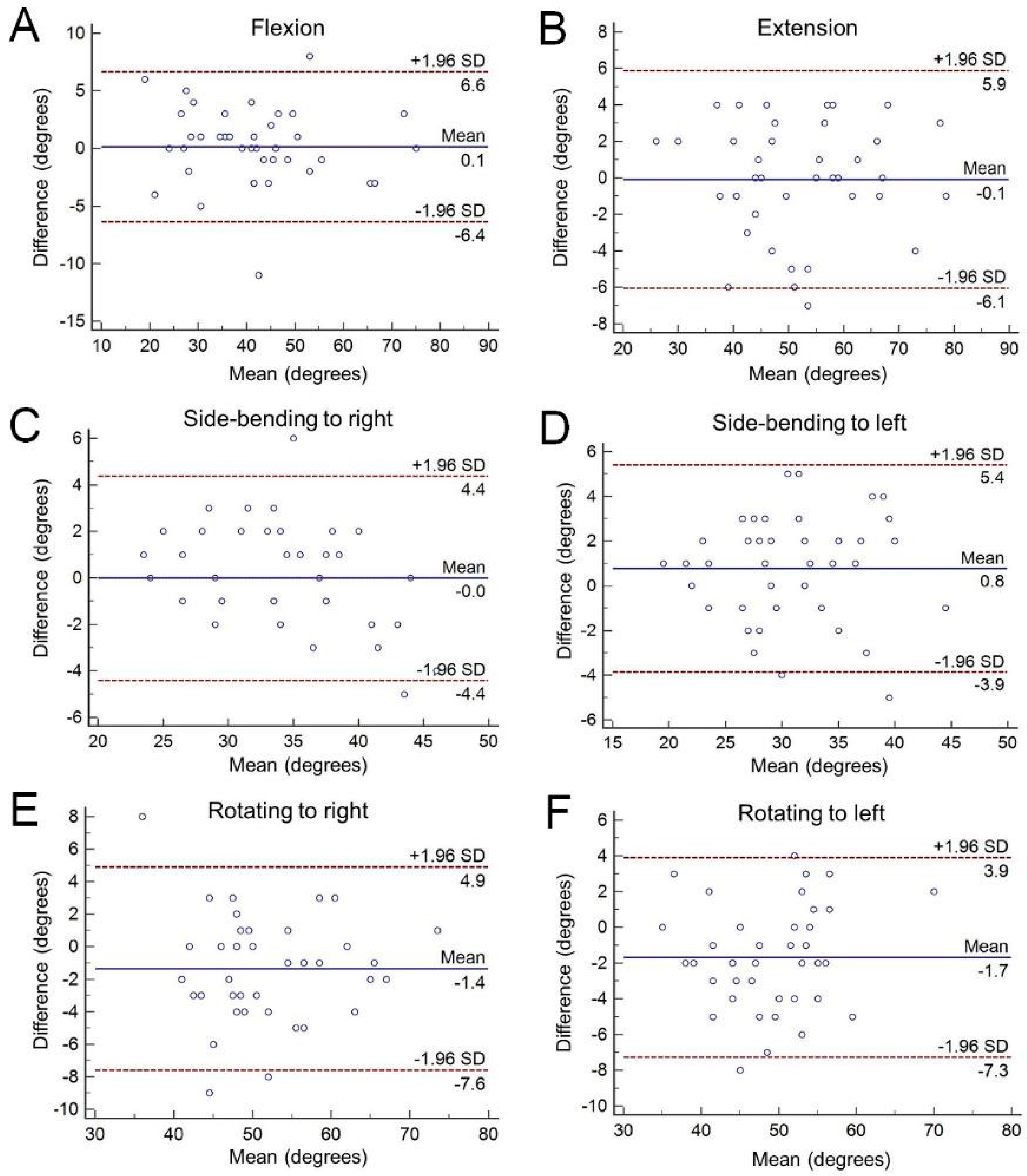
| Flexion | 41.80 (37.70 to 45.90) | 41.58 (37.47 to 45.88) | 0.12 (−0.92 to 1.16) | 0.815 | 0.968 (0.941 to 0.983) | <0.001 * | 6.428 |
| Extension | 51.48 (47.56 to 55.40) | 51.58 (47.67 to 55.49) | −0.09 (−1.05 to 0.86) | 0.838 | 0.969 (0.944 to 0.984) | <0.001 * | 5.888 |
| Side-bending to Right | 34.51 (32.78 to 36.23) | 34.53 (32.51 to 32.56) | −0.02 (−0.73 to 0.68) | 0.944 | 0.941 (0.892 to 0.968) | <0.001 * | 4.399 |
| Side-bending to Left | 31.34 (29.48 to 33.19) | 30.58 (28.73 to 32.43) | 0.75 (0.00 to 1.50) | 0.047 * | 0.918 (0.852 to 0.956) | <0.001 * | 4.810 |
| Rotating to Right | 50.80 (48.16 to 53.44) | 52.17 (49.52 to 54.81) | −1.36 (−2.37 to −0.36) | 0.009 * | 0.927 (0.867 to 0.961) | <0.001 * | 6.720 |
| Rotating to Left | 47.82 (45.51 to 50.14) | 49.51 (47.32 to 51.70) | −1.68 (−2.58 to −0.78) | 0.000 * | 0.921 (0.857 to 0.957) | <0.001 * | 6.428 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, K.-V.; Wu, W.-T.; Chen, M.-C.; Chiu, Y.-C.; Han, D.-S.; Chen, C.-C. Smartphone Application with Virtual Reality Goggles for the Reliable and Valid Measurement of Active Craniocervical Range of Motion. Diagnostics 2019, 9, 71. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics9030071
Chang K-V, Wu W-T, Chen M-C, Chiu Y-C, Han D-S, Chen C-C. Smartphone Application with Virtual Reality Goggles for the Reliable and Valid Measurement of Active Craniocervical Range of Motion. Diagnostics. 2019; 9(3):71. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics9030071
Chicago/Turabian StyleChang, Ke-Vin, Wei-Ting Wu, Mei-Chu Chen, Yi-Chi Chiu, Der-Sheng Han, and Chih-Cheng Chen. 2019. "Smartphone Application with Virtual Reality Goggles for the Reliable and Valid Measurement of Active Craniocervical Range of Motion" Diagnostics 9, no. 3: 71. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics9030071