
Conservative Non-Surgical Management of Horizontal Root-Fractured Maxillary Incisors in a Young Male with Angle Class II, Division 2, Malocclusion


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
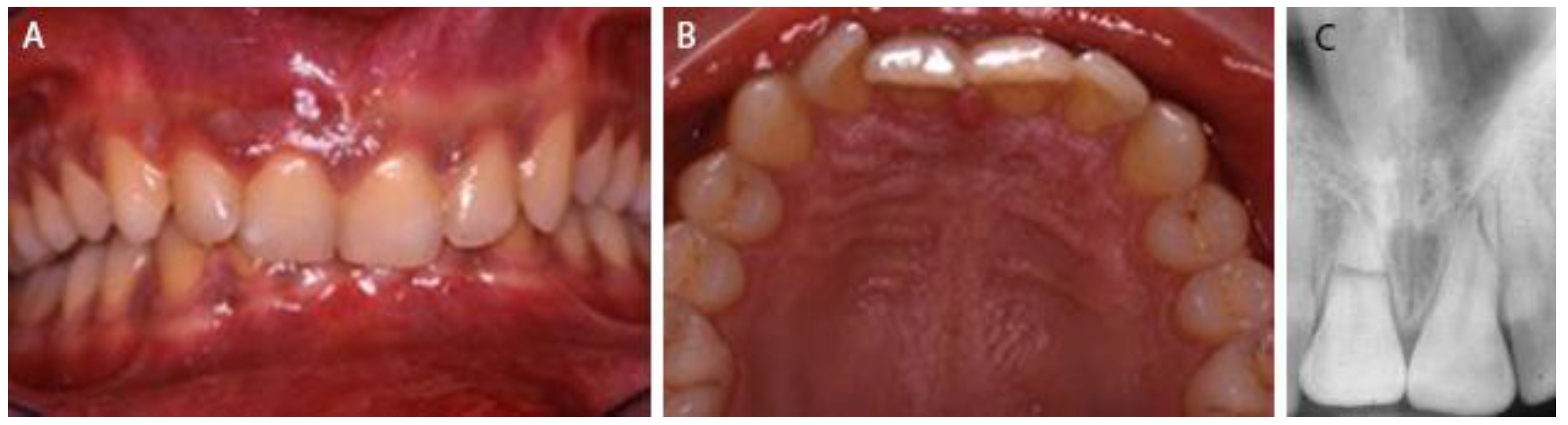
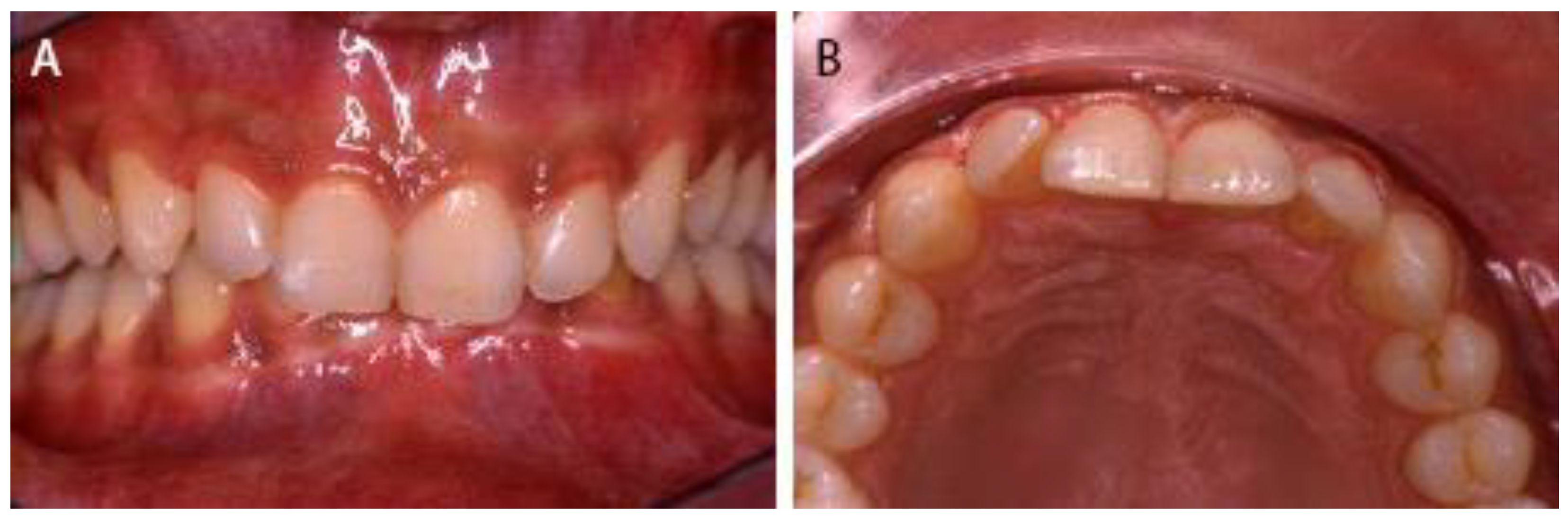
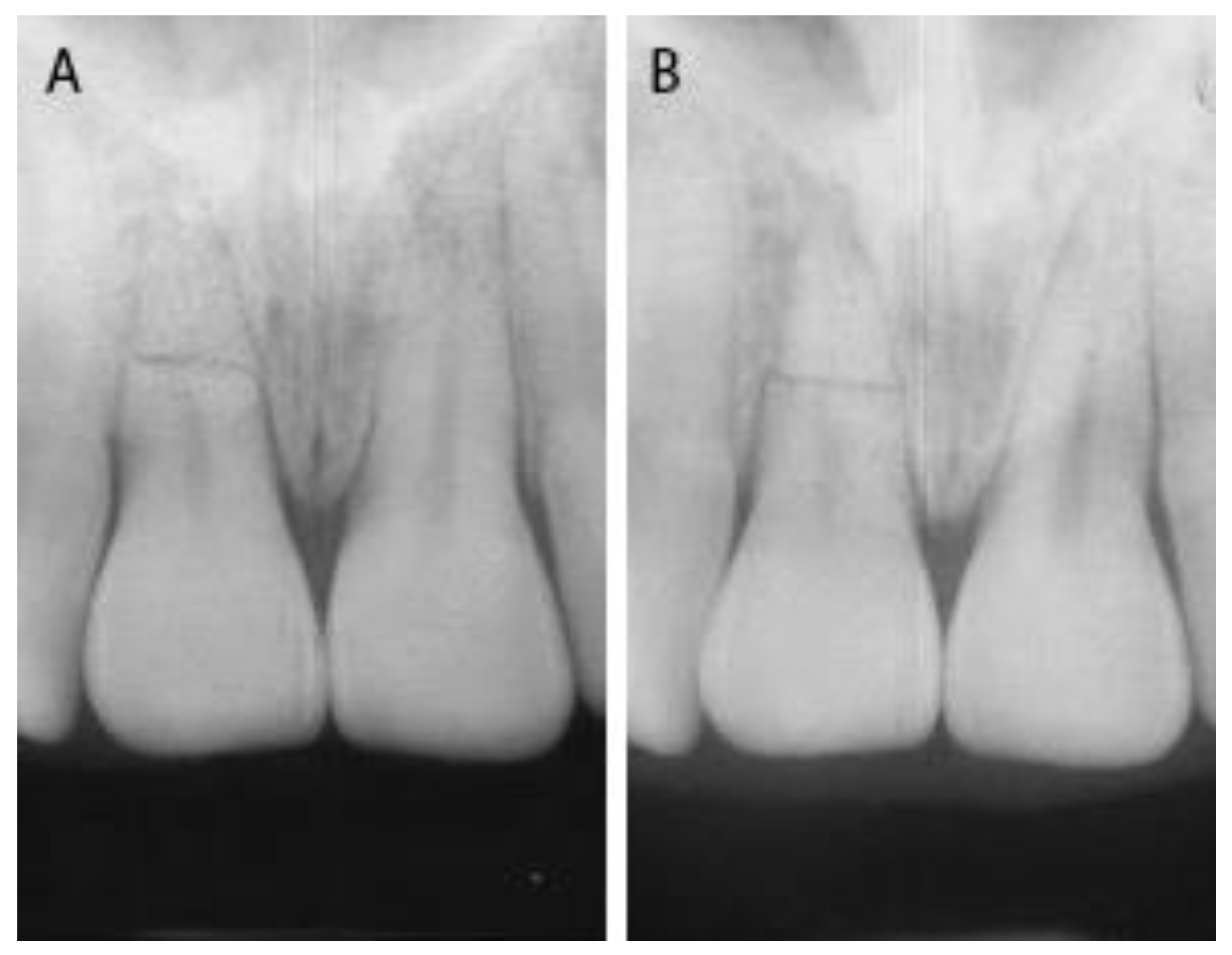
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Andreasen, F.M.; Andreasen, J.O.; Cveck, M. Root Fractures. In Textbook and Color Atlas of Traumatic Injuries to the Teeth, 4th ed.; Andreasen, J.O., Andreasen, F.M., Andersson, L., Eds.; Blackwell Publishing Ltd.: Oxford, UK, 2007; pp. 337–371. [Google Scholar]
- Caliscan, M.K.; Pehlivan, Y. Prognosis of root-fractured permanent incisors. Endod. Dent. Traumatol. 1996, 12, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Andreasen, J.O.; Hjorting-Hansen, E. Intra-alveolar root fractures: Radiographic and histologic study of 50 cases. J. Oral. Surg. 1967, 25, 414–426. [Google Scholar]
- Andreasen, J.O.; Ahrensburg, S.S.; Tsilingaridis, G. Tooth mobility changes subsequent to root fractures: A longitudinal clinical study of 44 permanent teeth. Dent. Traumatol. 2012, 28, 410–414. [Google Scholar] [CrossRef] [PubMed]
- Glendor, U. Aetiology and risk factors related to traumatic dental injuries—A review of the literature. Dent. Traumatol. 2009, 25, 19–31. [Google Scholar] [CrossRef] [PubMed]
- Zaleckiene, V.; Peciuliene, V.; Brukiene, V.; Drukteinis, S. Traumatic dental injuries: Etiology, prevalence and possible outcomes. Stomatologija 2014, 16, 7–14. [Google Scholar] [PubMed]
- Andreasen, J.O.; Andreasen, F.M.; Mejare, I.; Cvek, M. Healing of 400 intra-alveolar root fractures. 1. Effect pre-injury and injury factors such as sex, age, stage of root development, fracture type, location of fracture and severity of dislocation. Dent. Traumatol. 2004, 20, 192–202. [Google Scholar] [CrossRef]
- Andreasen, F.M. Pulpal healing after luxation injuries and root fracture in the permanent dentition. Endod. Dent. Traumatol. 1989, 5, 111–131. [Google Scholar] [CrossRef] [PubMed]
- Tsukiboshi, M. Root Fracture. Treatment Planning for Traumatized Teeth; Quintessence Publishing Co., Inc.: Carol Stream, IL, USA, 2000; pp. 47–57. [Google Scholar]
- Andreasen, J.O.; Andreasen, F.M.; Skeie, A.; Hiorting-Hansen, E. Effect of treatment delay upon pulp and periodontal healing of traumatic dental injuries—A review article. Dent. Traumatol. 2002, 18, 116–128. [Google Scholar] [CrossRef] [PubMed]
- Kahler, B.; Hu, J.Y.; Marriot-Smith, C.S.; Heithersay, G.S. Splinting of teeth following trauma: A review and a new splinting recommendation. Aust. Dent. J. 2016, 61, 59–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thaler, C.B.A.; Petschelt, A. Rigidity of commonly used dental trauma splints. Dent. Traumatol. 2009, 25, 248–255. [Google Scholar]
- Bourguignon, C.; Cohenca, N.; Lauridsen, E.; Flores, M.T.; O‘Connell, A.C.; Day, P.F.; Tsilingaridis, G.; Abbott, P.V.; Fouad, A.F.; Hicks, L.; et al. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries.1. Fractures and luxations. Dent. Traumatol. 2020, 36, 314–330. [Google Scholar] [CrossRef] [PubMed]
- Bardini, G.; Musu, D.; Mezzena, S.; Dettori, C.; Cotti, E. Combined management of apical root fracture and avulsion of two maxillary permanent central incisors: A case report. Dent. J. 2021, 9, 39. [Google Scholar] [CrossRef] [PubMed]
- Kahler, B.; Heithersay, G.S. An evidence_based appraisal of splinting luxated, avulsed and root-fracture teeth. Dent. Traumatol. 2008, 24, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Spinas, E.; Pipi, L.; Mezzena, S.; Giannetti, L. Use of orthodontic methods in the treatment of dental luxations: A scoping review. Dent. J. 2021, 9, 182. [Google Scholar] [CrossRef] [PubMed]
- Arikan, V.; Celikten, Z.K.; Sari, S. Treatment of horizontal root fractured central incisors and 30 months follow up: 2 case reports. Eur. J. Paediatr. Dent. 2014, 15, 199–202. [Google Scholar] [PubMed]
- Andreasen, J.O.; Andreasen, F.M.; Mejare, I.; Cveck, M. Healing of 400 intra-alveolar root fractures. 2. Effect of treatment factors such as treatment delay, repositioning, splinting type and period and antibiotics. Dent. Traumatol. 2004, 20, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Abbott, P.V. Diagnosis and management of transverse root fractures. Dent. Traumatol. 2019, 3, 333–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andreasen, F.M.; Andreasen, J.O. Prognosis of root-fractured permanent incisors prediction of healing modalities. Endod. Dent. Traumatol. 1989, 5, 11–22. [Google Scholar] [CrossRef] [PubMed]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Biagi, R.; Bardini, G.; Guidazzi, G.; Spinas, E. Conservative Non-Surgical Management of Horizontal Root-Fractured Maxillary Incisors in a Young Male with Angle Class II, Division 2, Malocclusion. Dent. J. 2021, 9, 55. https://0-doi-org.brum.beds.ac.uk/10.3390/dj9050055
Biagi R, Bardini G, Guidazzi G, Spinas E. Conservative Non-Surgical Management of Horizontal Root-Fractured Maxillary Incisors in a Young Male with Angle Class II, Division 2, Malocclusion. Dentistry Journal. 2021; 9(5):55. https://0-doi-org.brum.beds.ac.uk/10.3390/dj9050055
Chicago/Turabian StyleBiagi, Roberto, Giulia Bardini, Giuseppe Guidazzi, and Enrico Spinas. 2021. "Conservative Non-Surgical Management of Horizontal Root-Fractured Maxillary Incisors in a Young Male with Angle Class II, Division 2, Malocclusion" Dentistry Journal 9, no. 5: 55. https://0-doi-org.brum.beds.ac.uk/10.3390/dj9050055