
Entropy Measures in the Assessment of Heart Rate Variability in Patients with Cardiodepressive Vasovagal Syncope

Abstract
:1. Introduction
2. Methods
2.1. SampEn
2.2. PermEn
3. Procedures
3.1. Subjects
3.2. Physiological Measurements
3.3. Data Analysis
3.4. Statistical Methods
4. Results
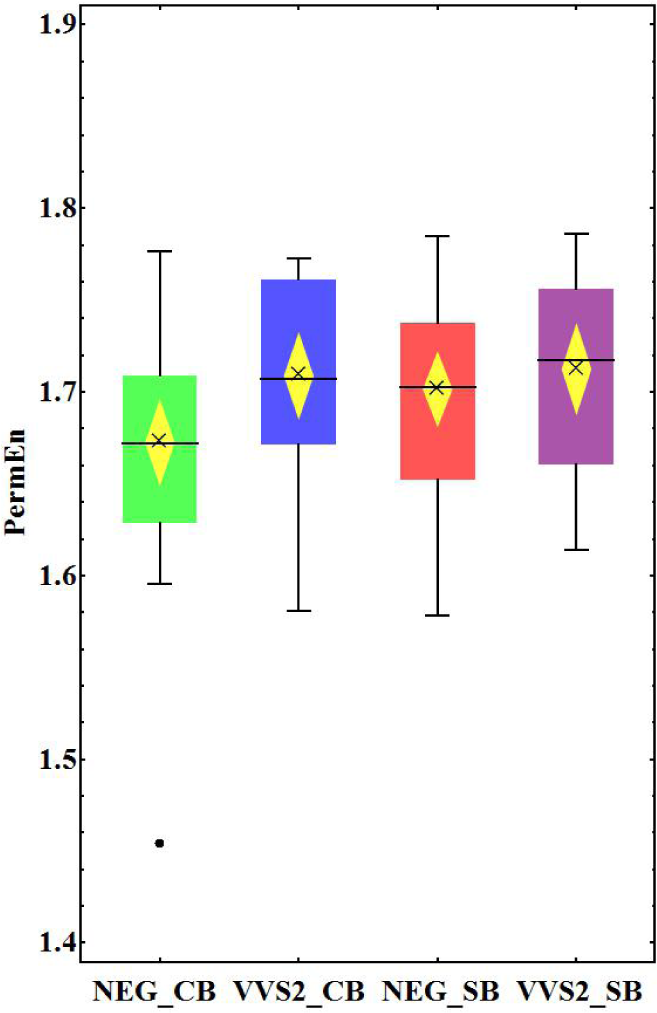
4.1. NEG vs. VVS_2 Groups
4.2. Spontaneous vs. Controlled Breathing
5. Discussion
5.1. NEG vs. VVS_2 Groups
5.2. Spontaneous vs. Controlled Breathing
5.3. Aspect of Gender
6. Conclusions
- In baseline recordings, SampEn and PermEn were able to show differences between groups with cardiodepressive or negative results for HUTT.
- Various entropy-based methods provide distinct information about heart rate complexity.
- In contrast to standard HRV parameters, SampEn and PermEn showed no significant differences when a comparison of the groups with the same reaction to HUTT, but different modes of respiration (NEG_SB vs. NEG_CB and VVS_2_SB vs. VVS_2_CB) was performed.
- Further studies in bigger groups of patients are needed to validate the above results.
Acknowledgments
- PACS classifications: 87.19.Hh; 89.70.Cf
List of Abbreviations
| ApEn | approximate entropy |
| HUTT | head-up tilt test |
| HUTT(−) | negative result of head-up tilt test (no syncope) |
| HUTT(+) | positive result of head-up tilt test (syncope) |
| NEG_CB | group with HUTT(−) and controlled breathing |
| NEG_SB | group with HUTT(−) and spontaneous breathing |
| PermEn | permutation entropy |
| SampEn | sample entropy |
| VVS_2_CB | group with HUTT(+) and controlled breathing |
| VVS_2_SB | group with HUTT(+) and spontaneous breathing |
Author Contributions
Conflicts of Interest
References
- Alboni, P.; Furlan, R. (Eds.) Vasovagal Syncope; Springer: Basel, Switzerland, 2015.
- Mosqueda-Garcia, R.; Fernandez-Violante, R.; Tank, J.; Snell, M.; Cunningha, G.; Furlan, R. Yohimbine in neurally mediated syncope. Pathophysiological implications. J. Clin. Invest. 1998, 102, 1824–1830. [Google Scholar]
- Folino, A.F.; Russo, G.; Porta, A.; Buja, G.; Cerutti, S.; Iliceto, S. Modulations of autonomic activity leading to tilt-mediated syncope. Int. J. Cardiol. 2007, 120, 102–107. [Google Scholar]
- Freitas, J.; Pereira, S.; Lago, P.; Costa, O.; Carvalho, M.J.; Falcão de Freitas, A. Impaired arterial baroreceptor sensitivity before tilt-induced syncope. Europace 1999, 1, 258–265. [Google Scholar]
- Grimm, W.; Wirths, A.; Hoffmann, J.; Menz, V.; Maisch, B. Heart rate variability during head-up tilt testing in patients with suspected neurally mediated syncope. Electrophysiology 1998, 21, 2411–2415. [Google Scholar]
- Lippman, N.; Stein, K.M.; Lerman, B.B. Failure to decrease parasympathetic tone during upright tilt predicts a positive tilt-table test. Am. J. Cardiol. 1995, 75, 591–595. [Google Scholar]
- Morillo, C.A.; Klein, G.J.; Jones, D.L.; Yee, R. Time and frequency domain analyses of heart rate variability during orthostatic stress in patients with neurally mediated syncope. Am. J. Cardiol. 1994, 74, 1258–1262. [Google Scholar]
- Tulppo, M.P.; Hughson, R.L.; Mäkikallio, T.H.; Airaksinen, K.E.J.; Seppänen, T.; Huikuri, H.V. Effects of exercise and passive head-up tilt on fractal and complexity properties of heart rate dynamics. Am. J. Physiol. Heart Circ. Physiol. 2001, 280, H1081–H1087. [Google Scholar]
- Kochiadakis, G.E.; Orfanakis, A.; Chryssostomakis, S.I.; Manios, E.G.; Kounali, D.K.; Vardas, P.E. Autonomic nervous system activity during tilt testing in syncopal patients, estimated by power spectral analysis of heart rate variability. Pacing. Clin. Electrophysiol. 1997, 20, 1332–1341. [Google Scholar]
- Kochiadakis, G.E.; Rombola, A.T.; Kanoupakis, E.M.; Simantirakis, E.N.; Chlouverakis, G.I.; Vardas, P.E. Assessment of autonomic function at rest and during tilt testing in patients with vasovagal syncope. Am. Heart J. 1997, 134, 459–466. [Google Scholar]
- Brignole, M.; Menozzi, C.; Rosso, A.D.; Costa, S.; Gaggioli, G.; Bottoni, N.; Bartoli, P.; Sutton, R. New classification of haemodynamics of vasovagal syncope: Beyond the VASIS classification. Analysis of the pre-syncopal phase of the tilt test without and with nitroglycerin challenge. Vasovagal Syncope International Study. Europace 2000, 2, 66–76. [Google Scholar]
- Guzmán, C.E.; Sánchez, G.M.; Márquez, M.F.; Hermosillo, A.G.; Cárdenas, M. Differences in heart rate variability between cardioinhibitory and vasodepressor responses to head-up tilt table testing. Arch. Med. Res. 1999, 30, 203–211. [Google Scholar]
- Kochiadakis, G.E.; Kanoupakis, E.M.; Igoumenidis, N.E.; Marketou, M.E.; Solomou, M.C.; Vardas, P.E. Spectral analysis of heart rate variability during tilt-table testing in patients with vasovagal syncope. Int. J. Cardiol. 1998, 64, 185–194. [Google Scholar]
- Kouakam, C.; Lacroix, D.; Zghal, N.; Logier, R.; Klug, D.; Franc, P.L.; Jarwe, M.; Kacet, S. Inadequate sympathovagal balance in response to orthostatism in patients with unexplained syncope and a positive head up tilt test. Heart 1999, 82, 312–318. [Google Scholar]
- Piccirillo, G.; Naso, C.; Moise, A.; Lionetti, M.; Carlo, M.N.S.D.; Laurentis, D.; Magri, D.; Cacciafesta, M.; Marigliano, V. Heart rate and blood pressure variability in subjects with vasovagal syncope. Clin. Sci. (Lond.) 2004, 107, 55–61. [Google Scholar]
- Lipsitz, L.A.; Wei, J.Y.; Rowe, J.W. Syncope in an elderly, institutionalised population: Prevalence, incidence, and associated risk. Q. J. Med. 1985, 55, 45–54. [Google Scholar]
- Vikman, S.; Mäkikallio, T.H.; Yli-Mäyry, S.; Pikkujämsä, S.; Koivisto, A.M.; Reinikainen, P.; Airaksinen, J.; Huikuri, H.V. Altered Complexity and Correlation Properties of R-R Interval Dynamics Before the Spontaneous Onset of Paroxysmal Atrial Fibrillation. Circulation 1999, 100, 2079–2084. [Google Scholar]
- Tuzcu, V.; Nas, S.; Borklu, T.; Ugur, A. Decrease in the heart rate complexity prior to the onset of atrial fibrillation. Europace 2006, 8, 398–402. [Google Scholar]
- Shin, D.G.; Yoo, C.S.; Yi, S.H.; Bae, J.H.; Kim, Y.J.; Park, J.S.; Hong, G.R. Prediction of Paroxysmal Atrial Fibrillation Using Nonlinear Analysis of the R-R Interval Dynamics Before the Spontaneous Onset of Atrial Fibrillation. Circ. J. 2006, 70, 94–99. [Google Scholar]
- Batchinsky, A.I.; Salinas, J.; Kuusela, T.; Necsoiu, C.; Jones, J.; Cancio, L. Rapid prediction of trauma patient survival by analysis of heart rate complexity: Impact of reducing data set size. Shock 2009, 32, 565–571. [Google Scholar]
- Hogue, C.W.J.; Domitrovich, P.P.; Stein, P.K.; Despotis, G.D.; Re, L.; Schuessler, R.B.; Kleiger, R.E.; Rottman, J.N. RR interval dynamics before atrial fibrillation in patients after coronary artery bypass graft surgery. Circulation 1998, 98, 429–434. [Google Scholar]
- Signorini, M.G.; Ferrario, M.; Marchetti, M.; Marseglia, A. Prediction of Paroxysmal Atrial Fibrillation Using Nonlinear Analysis of the R-R Interval Dynamics Before the Spontaneous Onset of Atrial Fibrillation. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2006, 1, 3431–3434. [Google Scholar]
- Ferrario, M.; Signorini, M.G.; Magenes, G.; Cerutti, S. Comparison of Entropy-Based Regularity Estimators: Application to the Fetal Heart Rate Signal for the Identification of Fetal Distress. IEEE Trans. Biomed. Eng. 2006, 53, 119–125. [Google Scholar]
- Amigó, J.M. Permutation Complexity in Dynamical Systems; Springer: Berlin/Heidelberg, Germany, 2010. [Google Scholar]
- Graff, B.; Graff, G.; Kaczkowska, A. Entropy Measures of Heart Rate Variability for Short ECG Datasets in Patients with Congestive Heart Failure. Acta Physica Polonica B Proc. Suppl. 2012, 5, 153–158. [Google Scholar]
- Parlitz, U.; Berg, S.; Luther, S.; Schirdewan, A.; Kurths, J.; Wessel, N. Classifying cardiac biosignals using ordinal pattern statistics and symbolic dynamics. Comput. Biol. Med. 2012, 42, 319–327. [Google Scholar]
- Richman, J.S.; Moorman, J.R. Physiological time-series analysis using approximate entropy and sample entropy. Am. J. Physiol. Heart Circ. Physiol. 2000, 278, H2039–H2049. [Google Scholar]
- Takens, F. Detecting strange attractors in turbulence. In Dynamical Systems and Turbulence; Springer: Berlin/Heidelberg, Germany, 1981; pp. 366–381. [Google Scholar]
- Alcaraz, R.; Abasolo, D.; Hornero, R.; Rieta, J.J. Optimal parameters study for sample entropy-based atrial fibrillation organization analysis. Comput. Methods Programs Biomed. 2010, 99, 124–132. [Google Scholar] [Green Version]
- Pincus, S.M. Approximate entropy as a measure of system complexity. Proc. Natl. Acad. Sci. USA 1991, 88, 2297–2301. [Google Scholar]
- Lake, D.E.; Richman, J.S.; Griffin, M.P.; Moorman, J.R. Sample entropy analysis of neonatal heart rate variability. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2002, 283, R789–R797. [Google Scholar]
- Ramdani, S.; Bouchara, F.; Lagarde, J. Influence of noise on the sample entropy algorithm. Chaos 2009, 19, 013123. [Google Scholar]
- Bandt, C.; Pompe, B. Permutation Entropy: A Natural Complexity Measure for Time Series. Phys. Rev. Lett. 2002, 88. [Google Scholar] [CrossRef]
- Sagristá-Sauleda, J.; Romero, B.; Permanyer-Miralda, G.; Moya, A.; Soler-Soler, A. Reproducibility of sequential head-up tilt testing in patients with recent syncope, normal ECG and no structural heart disease. Eur. Heart J. 2002, 23, 1706–1713. [Google Scholar]
- Porta, A.; Gnecchi-Ruscone, T.; Tobaldini, E.; Guzzetti, S.; Furlan, R.; Montano, N. Progressive decrease of heart period variability entropy-based complexity during graded head-up tilt. J. Appl. Physiol. (1985) 2007, 103, 1143–1149. [Google Scholar]
- Turianikova, Z.; Javorka, K.; Baumert, M.; Calkovska, A.; Javorka, M. The effect of orthostatic stress on multiscale entropy of heart rate and blood pressure. Physiol. Meas. 2011, 32, 1425–1437. [Google Scholar]
- Porta, A.; Castiglioni, P.; Bari, V.; Bassani, T.; Marchi, A.; Cividjian, A.; Quintin, L.; Rienzo, M.D. K-nearest-neighbor conditional entropy approach for the assessment of short-term complexity of cardiovascular control. Physiol. Meas. 2013, 34, 17–33. [Google Scholar]
- Weippert, M.; Behrens, M.; Rieger, A.; Behrens, K. Sample Entropy and Traditional Measures of Heart Rate Dynamics Reveal Different Modes of Cardiovascular Control During Low Intensity Exercise. Entropy 2014, 16, 5698–5711. [Google Scholar]
- Zanin, M.; Zunino, L.; Rosso, O.A.; Papo, D. Permutation entropy and its main biomedical and econophysics applications: A review. Entropy 2012, 14, 1553–1577. [Google Scholar]
- Keller, K.; Unakafov, A.M.; Unakafova, V.A. Ordinal Patterns, Entropy, and EEG. Entropy 2014, 16, 6212–6239. [Google Scholar]
- Graff, G.; Graff, B.; Kaczkowska, A.; Makowiec, D.; Amigó, J.M.; Piskorski, J.; Narkiewicz, K.; Guzik, P. Ordinal pattern statistics for the assessment of heart rate variability. Eur. Phys. J. Spec. Top. 2013, 222, 525–534. [Google Scholar]
- Porta, A.; Guzzetti, S.; Montano, N.; Pagani, M.; Somers, V.; Malliani, A.; Baselli, G.; Cerutti, S. Information domain analysis of cardiovascular variability signals: Evaluation of regularity, synchronisation and co-ordination. Med. Biol. Eng. Comput. 2000, 38, 180–188. [Google Scholar]
- Colman, N.; Nahm, K.; Ganzeboom, K.S.; Shen, W.K.; Reitsma, J.B.; Linzer, M.; Wieling, W.; Kaufmann, H. Epidemiology of reflex syncope. Clin. Auton. Res. 2004, 14, I/9–I/17. [Google Scholar]
- Kenny, R.A.; Bhangu, J.; King-Kallimanis, B.L. Epidemiology of syncope/collapse in younger and older Western patient populations. Prog. Cardiovasc. Dis. 2013, 55, 357–363. [Google Scholar]
- Ryan, S.M.; Goldberger, A.L.; Pincus, S.M.; Mietus, J.; Lipsitz, L.A. Gender- and age-related differences in heart rate dynamics: Are women more complex than men? J. Am. Coll. Cardiol. 1994, 24, 1700–1707. [Google Scholar]
- Catai, A.M.; Takahashi, A.C.; Perseguini, N.M.; Milan, J.C.; Minatel, V.; Rehder-Santos, P.; Marchi, A.; Bari, V.; Porta, A. Effect of the Postural Challenge on the Dependence of the Cardiovascular Control Complexity on Age. Entropy 2014, 16, 6686–6704. [Google Scholar]
- Mueller, A.; Bonnemeier, H.; Malberg, H.; Kurths, J.; Wessel, N. Age-dependent changes in the manifestations of gender-related differences in the cardiovascular regulation. Proceedings of the 8th Conference of the European Study Group on Cardiovascular Oscillations (ESGCO 2014), Trento, Italy, 25–28 May 2014; pp. 147–148.



{kind=link}
{kind=link}
| NEG_SB | VVS_2_SB | p | |
|---|---|---|---|
| RR | 753.00 ± 24.200 | 834.00 ± 22.200 | 0.024 |
| SDNN | 45.90 ± 5.200 | 48.60 ± 3.680 | 0.140 |
| RMSSD | 28.70 ± 4.400 | 33.30 ± 3.190 | 0.049 |
| pNN50 | 7.23 ± 2.050 | 13.00 ± 2.750 | 0.018 |
| α1 | 1.18 ± 0.041 | 1.11 ± 0.033 | 0.197 |
| sd1 | 20.30 ± 3.110 | 23.60 ± 2.260 | 0.051 |
| sd2 | 61.10 ± 6.810 | 64.50 ± 4.810 | 0.163 |
| SampEn | 1.29 ± 0.057 | 1.47 ± 0.057 | 0.040 |
| PermEn | 1.70 ± 0.010 | 1.71 ± 0.012 | 0.490 |
| NEG_CB | VVS_2_CB | p | |
|---|---|---|---|
| RR | 858.00 ± 25.300 | 909.00 ± 27.700 | 0.069 |
| SDNN | 59.30 ± 7.090 | 63.40 ± 6.020 | 0.308 |
| RMSSD | 46.90 ± 8.660 | 47.70 ± 5.650 | 0.223 |
| α1 | 1.06 ± 0.051 | 0.97 ± 0.061 | 0.286 |
| sd1 | 33.20 ± 6.130 | 33.80 ± 4.000 | 0.223 |
| sd2 | 76.00 ± 8.250 | 82.20 ± 8.020 | 0.348 |
| SampEn | 1.37 ± 0.047 | 1.50 ± 0.069 | 0.112 |
| PermEn | 1.67 ± 0.012 | 1.71 ± 0.011 | 0.048 |
| Pattern | NEG_SB | VVS_2_SB | NEG_CB | VVS_2_CB |
|---|---|---|---|---|
| (1 2 3) | 26.59 ± 4.83 | 25.66 ± 4.50 | 27.35 ± 5.55 | 25.68 ± 5.08 |
| (3 2 1) | 23.92 ± 6.88 | 24.35 ± 5.15 | 27.57 ± 5.17 | 24.60 ± 5.71 |
| (1 3 2) | 11.61 ± 2.57 | 12.02 ± 2.57 | 11.02 ± 2.64 | 12.27 ± 2.86 |
| (3 1 2) | 13.13 ± 2.96 | 12.97 ± 2.55 | 11.53 ± 2.51 | 12.59 ± 2.59 |
| (2 3 1) | 13.64 ± 3.11 | 13.74 ± 2.13 | 11.45 ± 2.80 | 13.35 ± 2.33 |
| (2 1 3) | 11.11 ± 2.26 | 11.26 ± 2.73 | 11.08 ± 2.25 | 11.51 ± 2.59 |
| NEG_SB | NEG_CB | p | |
|---|---|---|---|
| RR | 753.00 ± 24.200 | 858.00 ± 25.300 | 0.004 |
| SDNN | 45.90 ± 5.200 | 59.30 ± 7.090 | 0.082 |
| RMSSD | 28.70 ± 4.400 | 46.90 ± 8.660 | 0.075 |
| pNN50 | 7.23 ± 2.050 | 19.00 ± 3.860 | 0.054 |
| α1 | 1.18 ± 0.041 | 1.06 ± 0.051 | 0.072 |
| sd1 | 20.30 ± 3.110 | 33.20 ± 6.130 | 0.075 |
| sd2 | 61.10 ± 6.810 | 76.00 ± 8.250 | 0.087 |
| SampEn | 1.29 ± 0.057 | 1.37 ± 0.047 | 0.316 |
| PermEn | 1.70 ± 0.010 | 1.67 ± 0.012 | 0.080 |
| VVS_2_SB | VVS_2_CB | p | |
|---|---|---|---|
| RR | 834.00 ± 22.200 | 909.00 ± 27.700 | 0.036 |
| SDNN | 48.60 ± 3.680 | 63.40 ± 6.020 | 0.032 |
| RMSSD | 33.30 ± 3.190 | 47.70 ± 5.650 | 0.042 |
| pNN50 | 13.00 ± 2.750 | 23.00 ± 3.860 | 0.039 |
| α1 | 1.11 ± 0.033 | 0.97 ± 0.061 | 0.053 |
| sd1 | 23.60 ± 2.260 | 33.80 ± 4.000 | 0.042 |
| sd2 | 64.50 ± 4.810 | 82.20 ± 8.020 | 0.048 |
| SampEn | 1.47 ± 0.057 | 1.50 ± 0.069 | 0.761 |
| PermEn | 1.71 ± 0.012 | 1.71 ± 0.011 | 0.825 |
© 2015 by the authors; licensee MDPI, Basel, Switzerland This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Graff, B.; Graff, G.; Makowiec, D.; Kaczkowska, A.; Wejer, D.; Budrejko, S.; Kozłowski, D.; Narkiewicz, K. Entropy Measures in the Assessment of Heart Rate Variability in Patients with Cardiodepressive Vasovagal Syncope. Entropy 2015, 17, 1007-1022. https://0-doi-org.brum.beds.ac.uk/10.3390/e17031007
Graff B, Graff G, Makowiec D, Kaczkowska A, Wejer D, Budrejko S, Kozłowski D, Narkiewicz K. Entropy Measures in the Assessment of Heart Rate Variability in Patients with Cardiodepressive Vasovagal Syncope. Entropy. 2015; 17(3):1007-1022. https://0-doi-org.brum.beds.ac.uk/10.3390/e17031007
Chicago/Turabian StyleGraff, Beata, Grzegorz Graff, Danuta Makowiec, Agnieszka Kaczkowska, Dorota Wejer, Szymon Budrejko, Dariusz Kozłowski, and Krzysztof Narkiewicz. 2015. "Entropy Measures in the Assessment of Heart Rate Variability in Patients with Cardiodepressive Vasovagal Syncope" Entropy 17, no. 3: 1007-1022. https://0-doi-org.brum.beds.ac.uk/10.3390/e17031007