Intelligent Fog-Enabled Smart Healthcare System for Wearable Physiological Parameter Detection



 , , and
, , and 
Abstract
:1. Introduction
1.1. Motivation and Inspiration
- Latency—High latency is introduced due to data processing in the cloud layer. In general, healthcare services need on-time data transmission. Latency in healthcare applications directly affects the patient’s or user’s health.
- Fault Data—Most wearable or biosensors are deployed in the open or mobile (on the human) environment. It makes the sensors to generate erroneous data. Analyzing the inaccurate data ultimately leads to incorrect prediction.
- Low Accuracy—Health status prediction accuracy is down due to improper algorithms and attributes. All research works considered only wearable sensor data, which are unable to provide accurate results. However, environmental data are also crucial for accurate prediction. As the wearable data consists of duplicate data, it also affects the data processing accuracy.
- Fog Overloading—One of the best solutions for minimizing latency is to use fog computing. However, when more users are connected in the same region, the fog will become overloaded. This overloading problem is the major research issue in smart healthcare.
- Design a family healthcare system by using wearable for monitoring physiological parameters.
- Accurately predict the user state through physiological parameters.
- Minimize latency and detect the user state promptly.
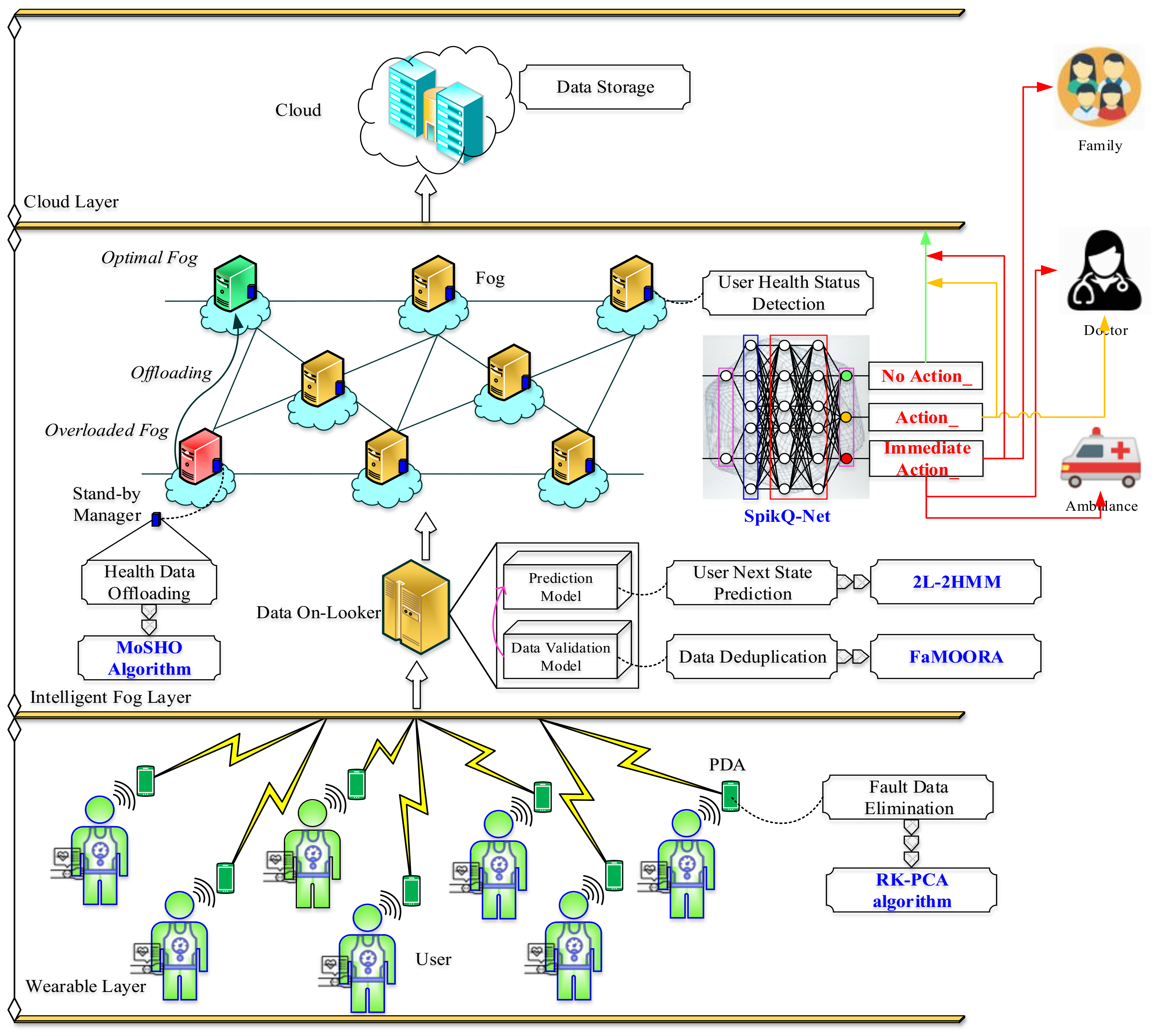
- Erroneous data from the wearable is diagnosed by using a rapid kernel principal component analysis (RK-PCA) algorithm. The RK-PCA algorithm is incorporated in a personal data assistant (PDA) (i.e.,) the faulty data is detected and eliminated in the wearable layer.
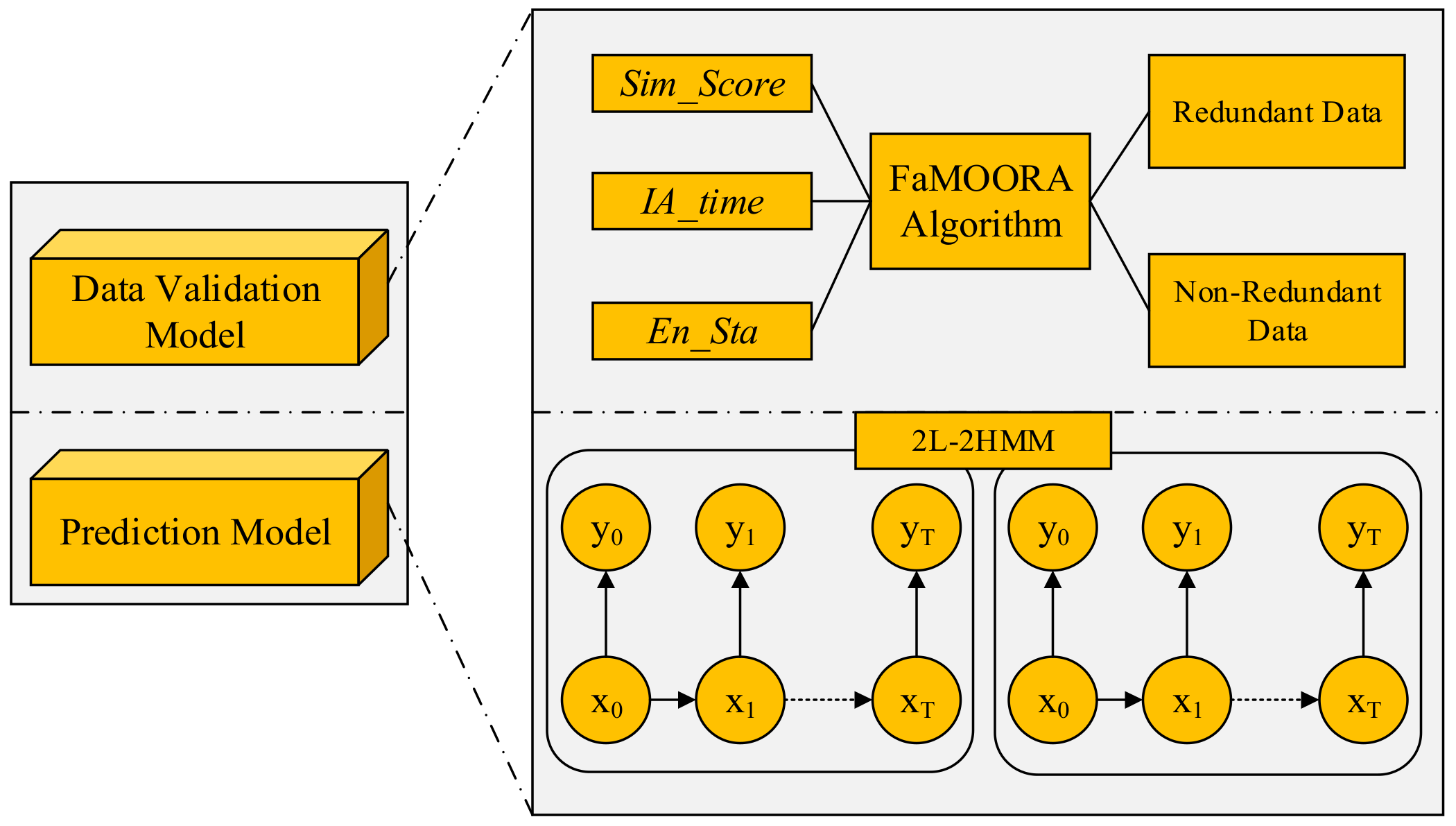
- From the faultless data, the data deduplication process is carried by the data on-looker node. To detect and eliminate duplicate data, we present a fuzzy assisted objective optimization by ratio analysis (FaMOORA) algorithm. If no duplicate data is found, then the fog node predicts the user’s health status through temporal features using the two-level health hidden Markov model (2L-2HMM). The 2L-2HMM appends the severity level of the user’s health status and provides apt action for severe cases.
- To prevent the fog layer from overloading the issue, we enable the health off procedure. The health of works upon two states. In the first stage, the offloading decision is made based on two rules. Then, an optimal node is selected for offloading by using the multi-objective spotted hyena optimization (MoSHO) algorithm.
- Then, the user’s current health status is detected in the cloud layer based on behavioral, biomedical, and environmental attributes. All these attributes are fed into the spiking quantum neural network (SpikQ-Net) that accurately classifies the user’s health status into normal action required, no action required, and immediate action required classes.
1.2. Paper Layout
2. Related Work
2.1. Research Works on Cloud-Based Smart Healthcare System
2.2. Research Works on Fog-Enabled Healthcare System
2.3. Research Works on Fog Offloading
3. Problem Overview
3.1. Overall Problem Statement
3.2. Background of the Problem
4. Proposed Tri-Fog Health System
4.1. System Overview
- All users have the same number of wearable devices to sense and generate health data;
- The number of fog nodes always equal or higher than the number of data on-looker nodes (i.e.,) ;
4.2. Fault Data Elimination in the Wearable Layer
| Algorithm 1: RK-PCA for Fault Data Detection. |
 |
4.3. Redundant Data Elimination by Data Validation
4.3.1. Redundant Data Elimination
4.3.2. User Health Status Prediction by Temporal Analysis
- When the user’s next status is emergency, and the location is not-frequent of the user, then the user is in a critical situation (C1).
- When the user’s next status is emergency, and the location is a frequent location of the user, then the user is in a near-critical situation (C2).
- When the user’s next status is normal, then the user is in the non-critical situation (C3).
| Algorithm 2: Process in Data On-Looker. |
 |
4.3.3. User’s Health Status Detection by Fog Nodes
- The set of input functions ( is fed into the input layer;
- Each neuron learns the input to produce output vectors in the hidden layers;
- The initial weight values () are initialized as the random numbers;
- Then the weight values are updated according to the update rule of quantum mechanics;
- Here o is the desired output provided for the training stage, is step size, and it is set as ;
- At last, the out layer learns the output based on the weights learned from hidden layers. The output of the quantum perceptron at the time t is,
4.3.4. Health Data Offloading
- Case1:
- When the fog node becomes overloaded
- Case2:
- When the environmental condition becomes worst
| Algorithm 3: Procedure of Health Off by MoSHO. |
 |
5. Experimental Evaluation
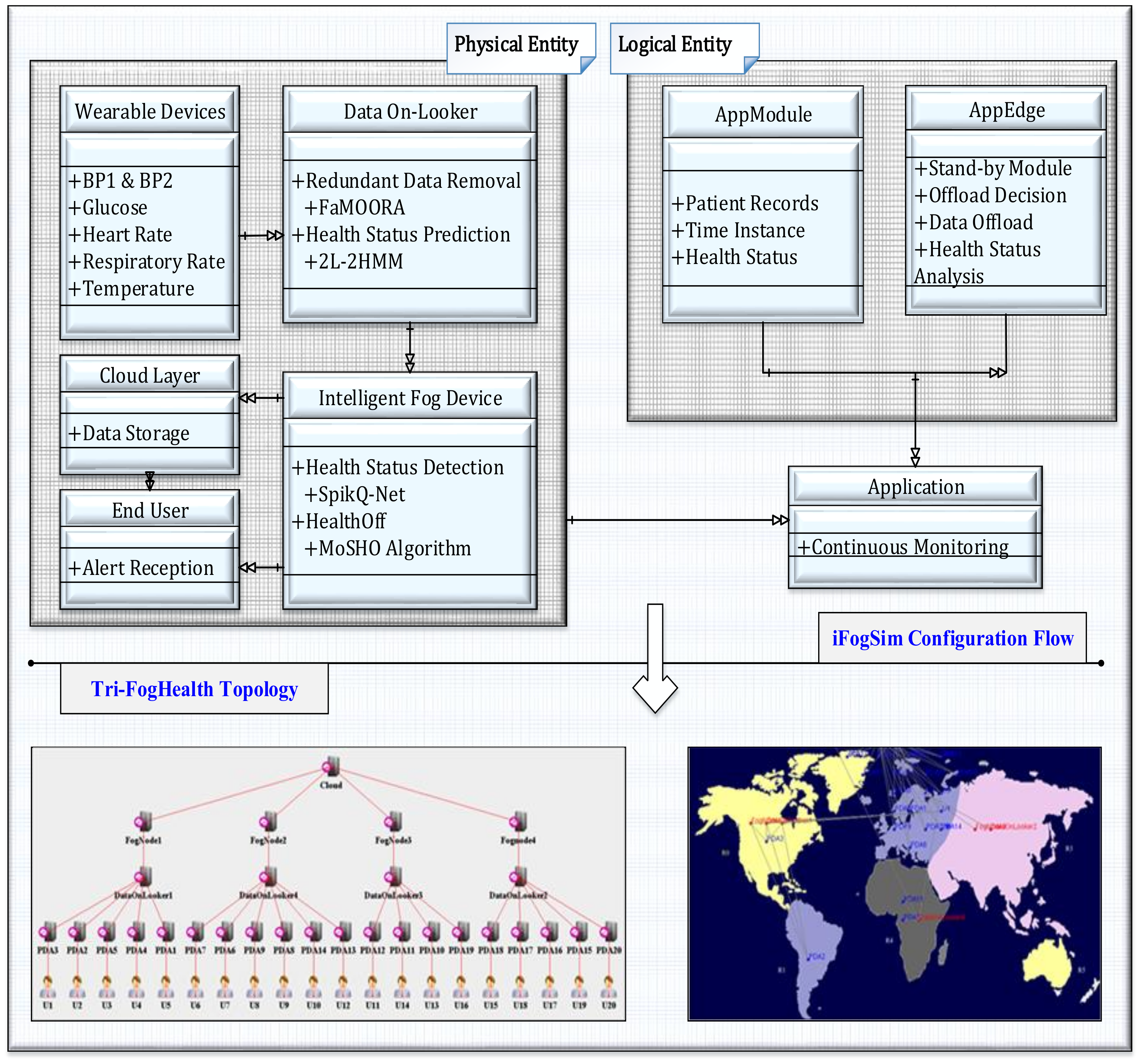
5.1. Experimental Setup
5.2. Application Scenario: Remote Quarantine Monitoring for Covid-19 Outbreak
5.3. Comparative Analysis
5.3.1. Analysis of Latency
5.3.2. Analysis of Execution Time
5.3.3. Analysis of Detection Accuracy
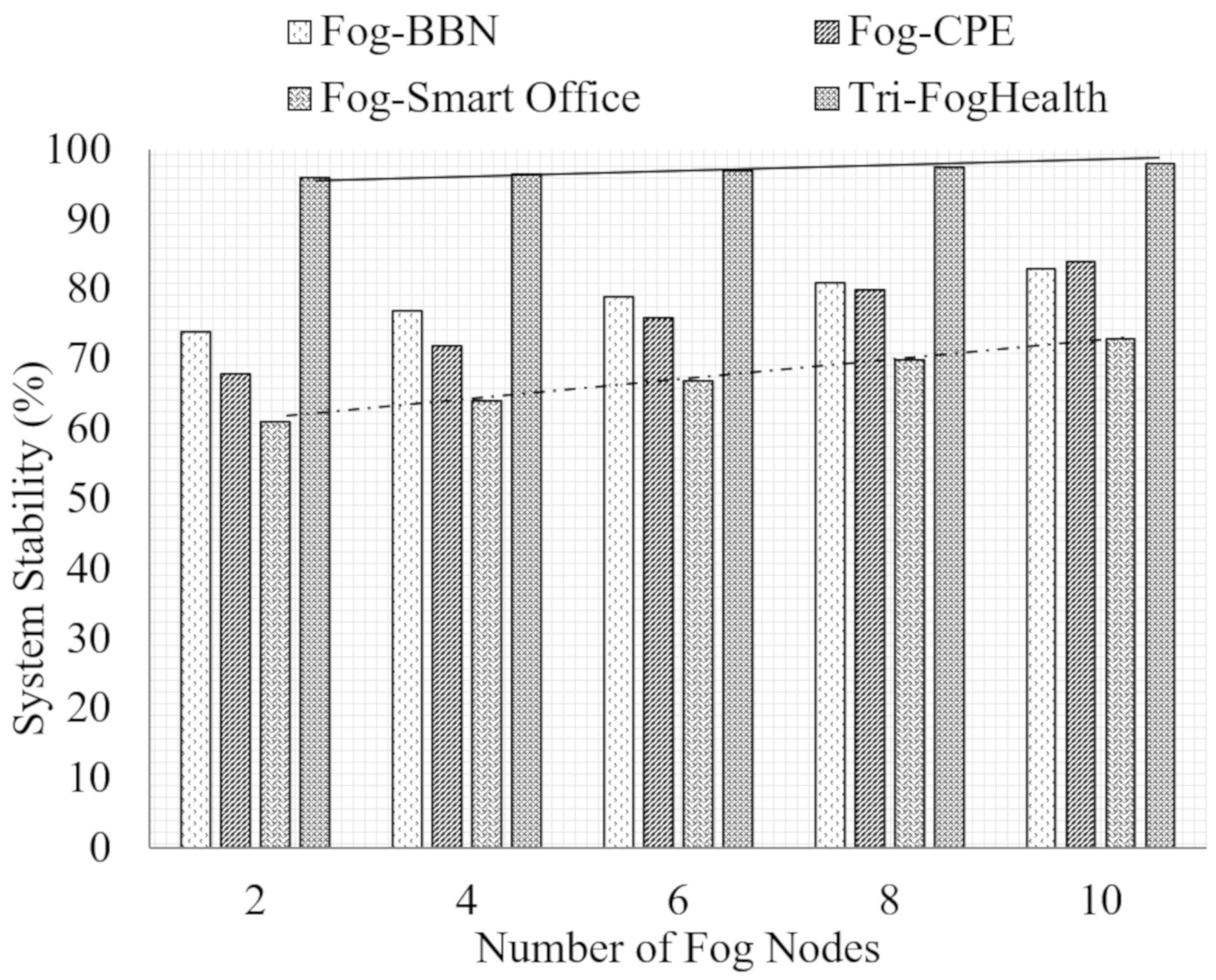
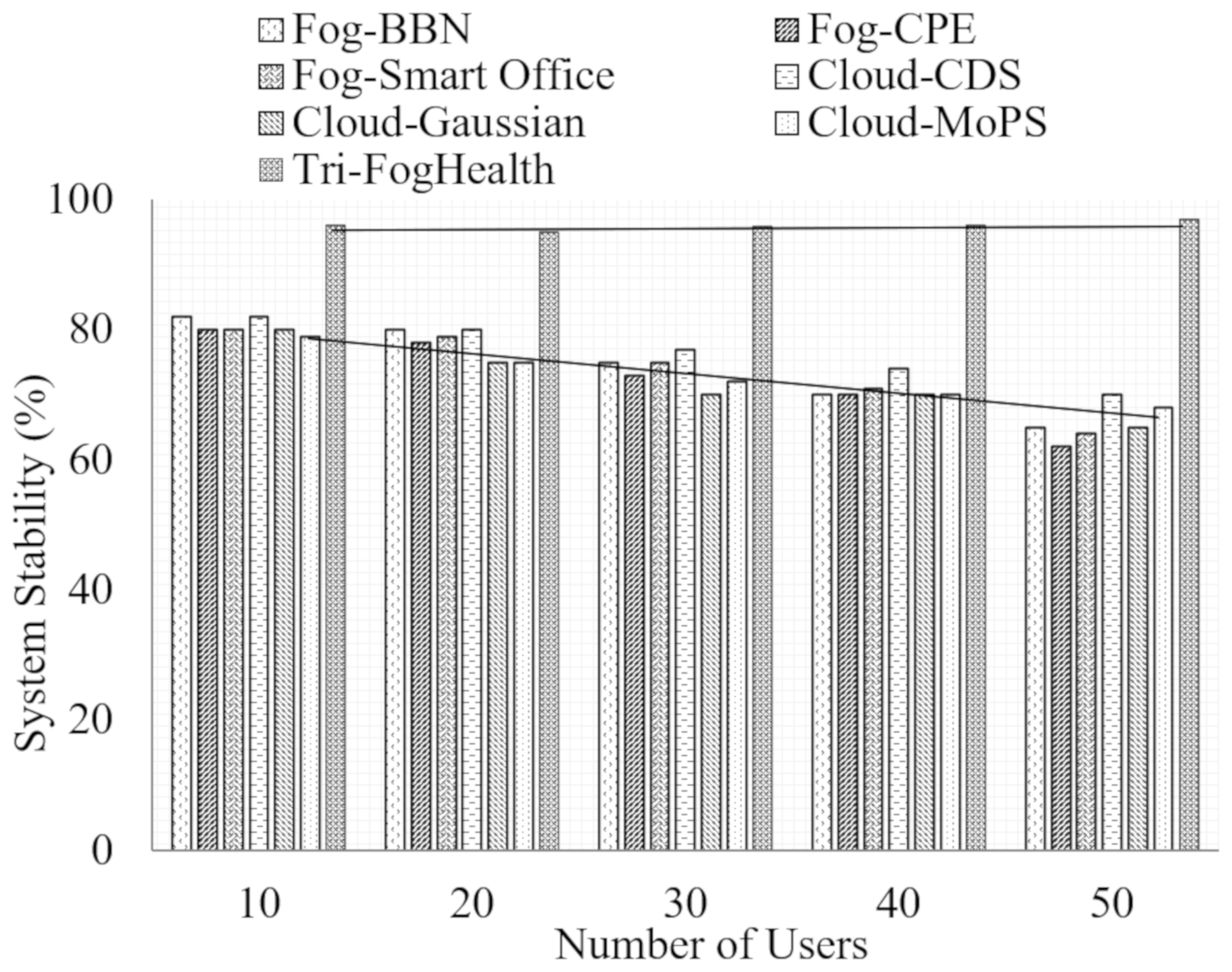
5.3.4. System Stability
5.3.5. Discussion on Results
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mohapatra, S.; Mohanty, S.; Mohanty, S. Smart healthcare: An approach for ubiquitous healthcare management using IoT. In Advances in Ubiquitous Sensing Applications for Healthcare; Academic Press: Cambridge, MA, USA, 2019. [Google Scholar]
- Ahad, A.; Tahir, M.A.; Yau, K.A. 5G-based smart healthcare network: Architecture, taxonomy, challenges, and future research directions. IEEE Access 2019, 7, 100747–100762. [Google Scholar] [CrossRef]
- Tian, S.; Yang, W.; Grange, J.M.; Wang, P.; Huang, W.; Ye, Z. Smart healthcare: Making medical care more intelligent. Glob. Health J. 2019, 3, 62–65. [Google Scholar] [CrossRef]
- Muzny, M.; Henriksen, A.; Giordanengo, A.; Mužík, J.; Grøttland, A.; Blixgård, H.; Hartvigsen, G.; Årsand, E. Wearable sensors with possibilities for data exchange: Analyzing status and needs of different actors in mobile health monitoring systems. Int. J. Med. Inform. 2019, 133, 104017. [Google Scholar] [CrossRef] [PubMed]
- Papa, A.; Mital, M.; Pisano, P.; Giudice, M.D. E-health and wellbeing monitoring using smart healthcare devices: An empirical investigation. Technol. Forecast. Soc. Chang. 2020, 153, 119226. [Google Scholar] [CrossRef]
- Mutlag, A.A.; Ghani, M.K.; Arunkumar, N.; Mohammed, M.A.; Mohd, O. Enabling technologies for fog computing in healthcare IoT systems. Future Gener. Comput. Syst. 2019, 90, 62–78. [Google Scholar] [CrossRef]
- Mahmud, R.; Ramamohanarao, K.; Buyya, R. Application management in fog computing environments: A taxonomy, review, and future directions. ACM Comput. Surv. 2020. [Google Scholar] [CrossRef]
- Zhao, R.; Yan, R.; Chen, Z.; Mao, K.; Wang, P.; Gao, R.X. Deep Learning and Its Applications to Machine Health Monitoring: A Survey. arXiv 2016, arXiv:abs/1612.07640. [Google Scholar] [CrossRef]
- Soualhi, M.; Nguyen, K.T.; Soualhi, A.; Medjaher, K.; Hemsas, K.E. Health monitoring of bearing and gear faults by using a new health indicator extracted from current signals. Measurement 2019, 141, 37–51. [Google Scholar] [CrossRef] [Green Version]
- Fu, Y.; Peng, C.; Gomez, F.; Narazaki, Y.; Spencer, B.F. Sensor fault management techniques for wireless smart sensor networks in structural health monitoring. Struct. Control Health Monit. 2019. [Google Scholar] [CrossRef]
- Petrovska, B.; Zdravevski, E.; Lameski, P.; Corizzo, R.; Štajduhar, I.; Lerga, J. Deep learning for feature extraction in remote sensing: A case-study of aerial scene classification. Sensors 2020, 20, 3906. [Google Scholar] [CrossRef]
- Munir, M.; Siddiqui, S.A.; Chattha, M.A.; Dengel, A.; Ahmed, S. FuseAD: Unsupervised anomaly detection in streaming sensors data by fusing statistical and deep learning models. Sensors 2019, 19, 2451. [Google Scholar] [CrossRef] [Green Version]
- Merrill, N.; Eskandarian, A. Modified autoencoder training and scoring for robust unsupervised anomaly detection in deep learning. IEEE Access 2020, 8, 101824–101833. [Google Scholar] [CrossRef]
- Ceci, M.; Corizzo, R.; Japkowicz, N.; Mignone, P.; Pio, G. ECHAD: Embedding-based change detection from multivariate time series in smart grids. IEEE Access 2020, 8, 156053–156066. [Google Scholar] [CrossRef]
- Hu, J.; Wu, K.; Liang, W. An IPv6-based framework for fog-assisted healthcare monitoring. Adv. Mech. Eng. 2019, 11. [Google Scholar] [CrossRef] [Green Version]
- Jeyaraj, P.R.; Rajan, S.E.; Martis, R.J.; Panigrahi, B.K. Fog computing employed computer aided cancer classification system using deep neural network in internet of things based healthcare system. J. Med. Syst. 2019, 44, 34. [Google Scholar]
- Nweke, H.F.; Wah, T.Y.; Mujtaba, G.; Al-garadi, M.A. Data fusion and multiple classifier systems for human activity detection and health monitoring: Review and open research directions. Inf. Fusion 2019, 46, 147–170. [Google Scholar] [CrossRef]
- Goschenhofer, J.; Pfister, F.M.; Yuksel, K.A.; Bischl, B.; Fietzek, U.; Thomas, J. Wearable-based Parkinson’s Disease Severity Monitoring using Deep Learning. arXiv 2019, arXiv:1904.10829. [Google Scholar]
- Mani, N.; Singh, A.; Nimmagadda, S.L. An IoT guided healthcare monitoring system for managing real-time notifications by fog computing services. Procedia Comput. Sci. 2020, 167, 850–859. [Google Scholar] [CrossRef]
- Zheng, H.; Xiong, K.; Fan, P.; Zhong, Z.; Letaief, K.B. Fog-assisted multiuser swipt networks: Local computing or offloading. IEEE Internet Things J. 2019, 6, 5246–5264. [Google Scholar] [CrossRef]
- Runkle, J.; Sugg, M.; Boase, D.; Galvin, S.L.; Coulson, C.C. Use of wearable sensors for pregnancy health and environmental monitoring: Descriptive findings from the perspective of patients and providers. Digit. Health 2019, 5. [Google Scholar] [CrossRef] [Green Version]
- Sangeetha, A.; Thangavel, A. Pervasive healthcare system based on environmental monitoring. Intell. Pervasive Comput. Syst. Smarter Healthc. 2019. [Google Scholar] [CrossRef]
- Aboudi, N.E.; Benhlima, L. Big data management for healthcare systems: Architecture, requirements, and implementation. Adv. Bioinform. 2018. [Google Scholar] [CrossRef]
- Sun, F.; Zang, W.; Gravina, R.; Fortino, G.; Li, Y. Gait-based identification for elderly users in wearable healthcare systems. Inf. Fusion 2020, 53, 134–144. [Google Scholar] [CrossRef]
- Albahri, A.S.; Albahri, O.S.; Zaidan, A.A.; Zaidan, B.B.; Hashim, M.; Alsalem, M.A.; Mohsin, A.H.; Mohammed, K.I.; Alamoodi, A.H.; Enaizan, O.; et al. Based on multiple heterogeneous wearable sensors: A smart real-time health monitoring structured for hospitals distributor. IEEE Access 2019, 7, 37269–37323. [Google Scholar] [CrossRef]
- Zhang, H.; Liu, J.; Kato, N. Threshold tuning-based wearable sensor fault detection for reliable medical monitoring using bayesian network model. IEEE Syst. J. 2018, 12, 1886–1896. [Google Scholar] [CrossRef]
- Colopy, G.W.; Roberts, S.J.; Clifton, D.A. Bayesian optimization of personalized models for patient vital-sign monitoring. IEEE J. Biomed. Health Inform. 2018, 22, 301–310. [Google Scholar] [CrossRef]
- Liu, Y.; Zhang, L.; Yang, Y.; Zhou, L.; Ren, L.; Wang, F.; Liu, R.; Pang, Z.; Deen, M.J. A novel cloud-based framework for the elderly healthcare services using digital twin. IEEE Access 2019, 7, 49088–49101. [Google Scholar] [CrossRef]
- Anagaw, A.; Chang, Y. A new complement naïve Bayesian approach for biomedical data classification. J. Ambient Intell. Humaniz. Comput. 2019, 10, 3889–3897. [Google Scholar] [CrossRef]
- Pathinarupothi, R.K.; Durga, P.; Rangan, E. IoT-based smart edge for global health: Remote monitoring with severity detection and alerts transmission. IEEE Internet Things J. 2018, 6, 2449–2462. [Google Scholar] [CrossRef]
- Rahmani, A.M.; Gia, T.N.; Negash, B.; Anzanpour, A.; Azimi, I.; Jiang, M.; Liljeberg, P. Exploiting smart e-Health gateways at the edge of healthcare Internet-of-Things: A fog computing approach. Future Gener. Comput. Syst. 2018, 78, 641–658. [Google Scholar] [CrossRef]
- Gai, K.; Lu, Z.; Qiu, M.; Zhu, L. Toward smart treatment management for personalized healthcare. IEEE Netw. 2019, 33, 30–36. [Google Scholar] [CrossRef]
- Hassan, M.K.; El-Desouky, A.I.; Badawy, M.M.; Sarhan, A.M.; Elhoseny, M.; Manogaran, G. EoT-driven hybrid ambient assisted living framework with naïve Bayes–firefly algorithm. Neural Comput. Appl. 2018, 31, 1275–1300. [Google Scholar] [CrossRef]
- Tuli, S.; Basumatary, N.; Gill, S.S.; Kahani, M.; Arya, R.C.; Wander, G.S.; Buyya, R. HealthFog: An ensemble deep learning based smart healthcare system for automatic diagnosis of heart diseases in integrated IoT and fog computing environments. Future Gener. Comput. Syst. 2020, 104, 187–200. [Google Scholar] [CrossRef] [Green Version]
- Muhammed, T.; Mehmood, R.; Albeshri, A.A.; Katib, I.A. UbeHealth: A personalized ubiquitous cloud and edge-enabled networked healthcare system for smart cities. IEEE Access 2018, 6, 32258–32285. [Google Scholar] [CrossRef]
- Khattak, H.A.; Arshad, H.; Islam, S.U.; Ahmed, G.; Jabbar, S.; Sharif, A.M.; Khalid, S. Utilization and load balancing in fog servers for health applications. Eurasip J. Wirel. Commun. Netw. 2019, 2019, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Mutlag, A.A.; Ghani, M.K.; Mohammed, M.A.; Maashi, M.S.; Mohd, O.; Mostafa, S.A.; Abdulkareem, K.H.; Marques, G.; Díez, I.D. MAFC: Multi-Agent fog computing model for healthcare critical tasks management. Sensors 2020, 20, 1853. [Google Scholar] [CrossRef] [Green Version]
- Sharma, S.; Saini, H. A novel four-tier architecture for delay aware scheduling and load balancing in fog environment. Sustain. Comput. Inform. Syst. 2019, 24, 100355. [Google Scholar] [CrossRef]
- Adhikari, M.; Gianey, H.K. Energy efficient offloading strategy in fog-cloud environment for IoT applications. Internet Things 2019, 6, 100053. [Google Scholar] [CrossRef]
- Naghshvarianjahromi, M.; Kumar, S.; Deen, M.J. Brain-inspired intelligence for real-time health situation understanding in smart e-health home applications. IEEE Access 2019, 7, 180106–180126. [Google Scholar] [CrossRef]
- Zhu, T.; Colopy, G.W.; MacEwen, C.; Niehaus, K.E.; Yang, Y.; Pugh, C.W.; Clifton, D.A. Patient-specific physiological monitoring and prediction using structured gaussian processes. IEEE Access 2019, 7, 58094–58103. [Google Scholar] [CrossRef]
- Leu, F.; Ko, C.; You, I.; Choo, K.R.; Ho, C. A smartphone-based wearable sensors for monitoring real-time physiological data. Comput. Electr. Eng. 2018, 65, 376–392. [Google Scholar]
- Verma, P.; Sood, S.K. Fog assisted-IoT enabled patient health monitoring in smart homes. IEEE Internet Things J. 2018, 5, 1789–1796. [Google Scholar] [CrossRef]
- Dautov, R.; Distefano, S.; Buyya, R. Hierarchical data fusion for smart healthcare. J. Big Data 2019, 6, 1–23. [Google Scholar] [CrossRef] [Green Version]
- Bhatia, M.; Sood, S.K. Exploring temporal analytics in fog-cloud architecture for smart office healthcare. Mob. Netw. Appl. 2019, 24, 1392–1410. [Google Scholar] [CrossRef]
- Brauers, W.K.; Zavadskas, E.K. The MOORA method and its application to privatization in a transition economy. Control Cybern. 2006, 35, 445–469. [Google Scholar]
- Xiang, S.; Zhang, Y.; Gong, J.; Guo, X.; Lin, L.; Hao, Y. STDP-based unsupervised spike pattern learning in a photonic spiking neural network With VCSELs and VCSOAs. IEEE J. Sel. Top. Quantum Electron. 2019, 25, 1–9. [Google Scholar] [CrossRef]
- Salahshour, E.; Malekzadeh, M.; Gholipour, R.; Khorashadizadeh, S. Designing multi-layer quantum neural network controller for chaos control of rod-type plasma torch system using improved particle swarm optimization. Evol. Syst. 2019, 1–15. [Google Scholar] [CrossRef]
- Dhiman, G.; Kumar, V. Spotted hyena optimizer: A novel bio-inspired based metaheuristic technique for engineering applications. Adv. Eng. Softw. 2017, 114, 48–70. [Google Scholar] [CrossRef]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Presented Works | Research Issues |
|---|---|---|
| Cloud-Smart Healthcare |
| |
| Fog-Smart Healthcare |
| |
| Fog Offloading |
|
| Layer | Entities Involved | Functions Incorporated |
|---|---|---|
| Wearable Layer |
|
|
| Intelligent Fog Layer |
|
|
| • Cloud Layer | • Cloud Servers | • Data Storage and Retrieval |
| Category | Attributes | Description |
|---|---|---|
| Behavior |
| Attributes are related to the user’s normal behavior. We consider the static information like smoke or not and dynamic information like location to monitor the user’s health status |
| Biomedical |
| We consider the data from wearable devices. All data related to the biomedical data that shows the user’s current health status |
| Environmental |
| These data are collected from the regional environmental sensors. |
| Software/Hardware | Description |
|---|---|
| Simulation Tool | iFogSim |
| Simulator Version | 3.0.3 |
| Operating System | Windows 7 Ultimate |
| Programming Language | Java |
| Development Kit | JDK 1.8 |
| IDE | NetBeans 8.2 |
| Database | MySQL-5.1.36 (Wamp Server 2.0) |
| Parameter | Value | |
|---|---|---|
| Number of users | 50 | |
| Number of biosensors in each user | 5 | |
| Number of data on-lookers | 10 | |
| Number of fog nodes | 10 | |
| Fog Node Configuration | Storage | 1 GB |
| Bandwidth | 1000 KBs | |
| Resource Cost | 3.0 | |
| Memory Cost | 0.5 | |
| Cloud Configuration | MIPS | 1000 |
| Memory | 10 MB | |
| Bandwidth | 1000 KBs | |
| SpikQ-Net | Number of neurons | 10 |
| Number of hidden layers | 3 | |
| Activation Function | Sigmoid | |
| Step Size | 0.2 | |
| MoSHO | Initial Population | 100 |
| 0.3 | ||
| Iteration | 100 | |
| Work | Architecture | Concept | Attributes Considered | Cons | Common Issues |
|---|---|---|---|---|---|
| Cloud-CDS [40] | Cloud-based Smart Healthcare System | CDS based Healthcare System Decision Tree-based classification | Biomedical |
| 1 Latency is high since the data processing is performed in the cloud layer |
| Cloud-Gaussian [41] | Cloud-based Physiological Sign Monitoring | Gaussian Model detects health level Patient’s Health Trajectory is extracted | Biomedical |
|
|
| Cloud-MoPS [42] | Cloud-based Mobile Healthcare System | A smart shirt and Wearable Technology is used for health monitoring | Biomedical |
| |
| Fog-BBN [43] | Cloud-Fog based Patient Health Monitoring | BBN Classifier is used in Fog Layer THI is computed in Cloud Layer | Biomedical Behavior Environmental |
|
|
| Fog-CPE [44] | Hierarchical Data Fusion Model with Sensor, Fog and Cloud Model | Biosensor Readings are Classified in each Level | Biomedical | Biosensor data alone is insufficient to analyze the health data accurately CPE works upon pre-defined rules which are not efficient for dynamic health data | |
| Fog-Smart Office [45] | Fog-Cloud Healthcare System for Smart Office | Severity Index is constructed to monitor the health status | Biomedical Behavior Environmental | Bayesian classifier which is used here is complex and has less accuracy Final health status is detected and a decision made in the cloud layer which increases latency |
| Parameter | Cloud-CDS [36] | Cloud-Gaussian [37] | Cloud-MoPS [38] | Fog-BBN [39] | Fog-CPE [40] | Fog-Smart Office [41] | Tri-FogHealth | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Latency (ms) | 18.52 | 17.4 | 16.4 | 7.8 | 6.96 | 9.98 | 7.92 | 11.2 | 9.02 | 3.44 | 2.9 |
| Execution Time (ms) | 11.2 | 11.2 | 12.5 | 7.8 | 5.02 | 9.98 | 8.6 | 11.2 | 11 | 2.52 | 1.74 |
| Detection Accuracy (%) | 61.6 | 58.6 | 50 | 72.4 | 75.3 | 68.8 | 68.4 | 64.6 | 66.7 | 95.44 | 97 |
| System Stability (%) | 76.6 | 72 | 72.8 | 78.8 | 74.4 | 76 | 72.6 | 67 | 73 | 97 | 96 |
| The Methodology Used in Tri-FogHealth | Contribution in Results |
|---|---|
| RK-PCA Fault Detection | Eliminates fault data generated by wearable devices Increases detection accuracy since it allows only proper data for analysis Minimizes execution time since a large amount of fault data is suppressed |
| FaMOORA Redundant Data Elimination | Eliminates redundant data generated by wearable devices Minimizes execution time since the repeated data has been removed |
| 2L-2HMM Health Status Prediction | Predicts user’s health status based on temporal variations Increases detection accuracy since it predicts the user’s next state Minimizes latency |
| SpikQ-Net Health Status Detection | Detect user’s current health status Minimizes latency since the response is generated in the fog layer Detection accuracy is high since it considers there categories of attributes Execution time is low as the SpikQ-Net which is a machine learning technique that works faster than statistical approaches |
| MoSHO Health Off | Enable offloading procedure when the fog becomes overloaded Minimizes latency by offloading data to optimal fog nodes Increases system stability by maintaining a balanced load among the fog |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ijaz, M.; Li, G.; Wang, H.; El-Sherbeeny, A.M.; Moro Awelisah, Y.; Lin, L.; Koubaa, A.; Noor, A. Intelligent Fog-Enabled Smart Healthcare System for Wearable Physiological Parameter Detection. Electronics 2020, 9, 2015. https://0-doi-org.brum.beds.ac.uk/10.3390/electronics9122015
Ijaz M, Li G, Wang H, El-Sherbeeny AM, Moro Awelisah Y, Lin L, Koubaa A, Noor A. Intelligent Fog-Enabled Smart Healthcare System for Wearable Physiological Parameter Detection. Electronics. 2020; 9(12):2015. https://0-doi-org.brum.beds.ac.uk/10.3390/electronics9122015
Chicago/Turabian StyleIjaz, Muhammad, Gang Li, Huiquan Wang, Ahmed M. El-Sherbeeny, Yussif Moro Awelisah, Ling Lin, Anis Koubaa, and Alam Noor. 2020. "Intelligent Fog-Enabled Smart Healthcare System for Wearable Physiological Parameter Detection" Electronics 9, no. 12: 2015. https://0-doi-org.brum.beds.ac.uk/10.3390/electronics9122015