
Parent-Reported Social-Communicative Skills of Children with 22q11.2 Copy Number Variants and Siblings
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Research Design
2.3. Measurements
2.4. Data Analysis
3. Results
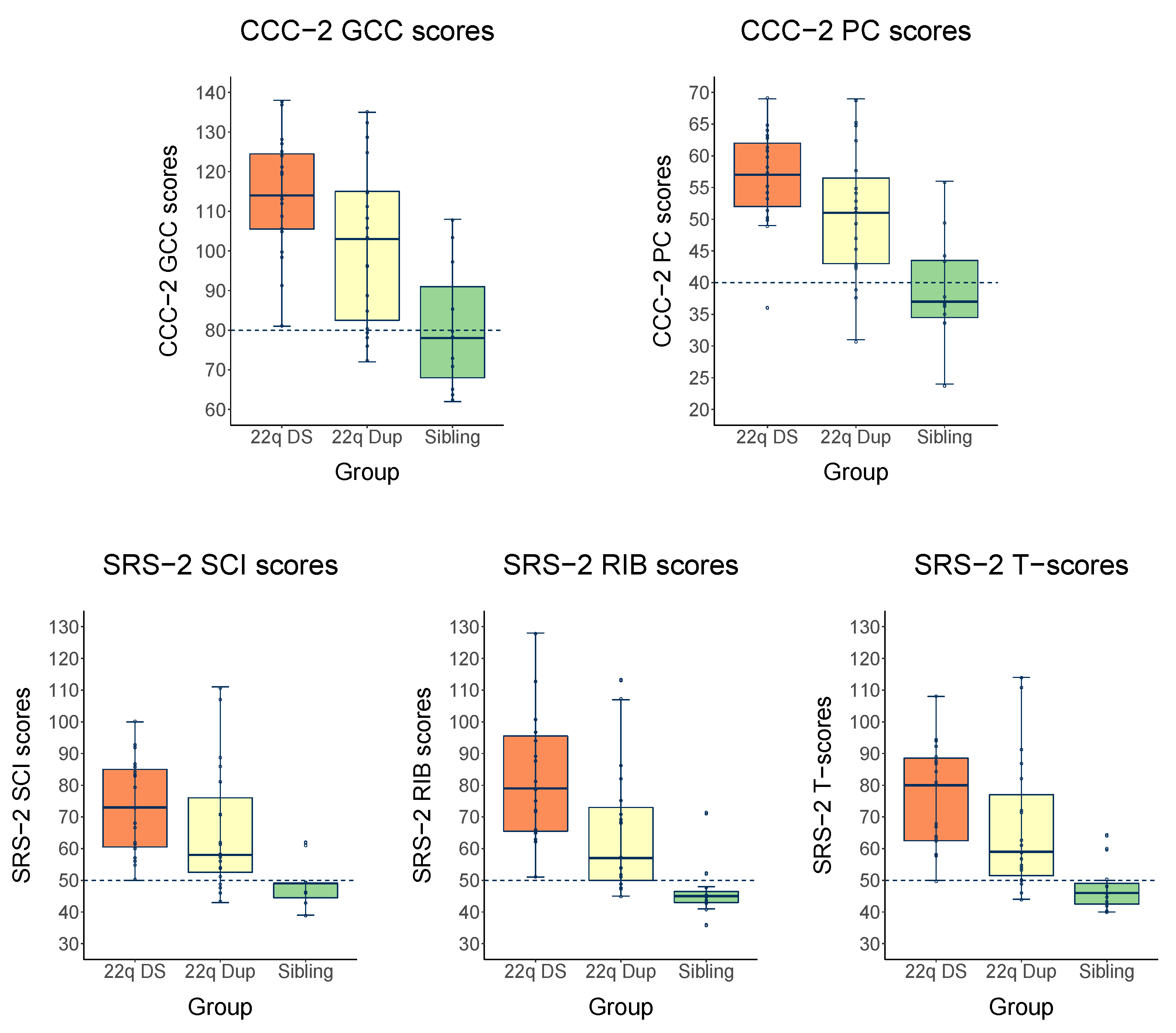
3.1. CNVs and Siblings Compared to Norm Group Scores
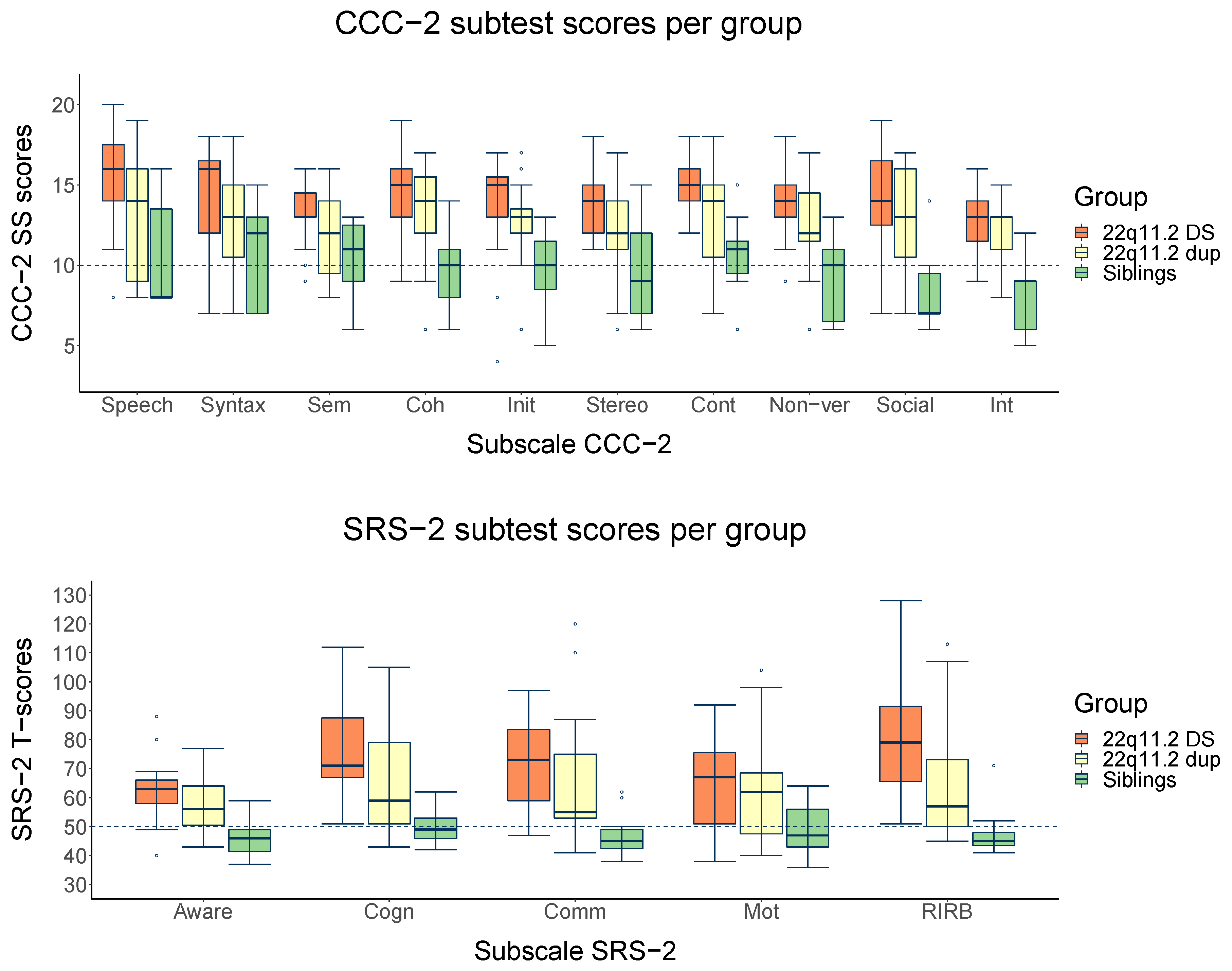
3.2. Cross-CNV and Intrafamilial Comparisons at Group Level: Mean Differences
3.3. Cross-CNV and Intrafamilial Comparisons at Subgroup Level: Proportion Differences
3.4. Within-Group Comparisons at Individual Level
4. Discussion
Strengths, Limitations, and Future
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Grayton, H.M.; Fernandes, C.; Rujescu, D.; Collier, D.A. Copy Number Variations in Neurodevelopmental Disorders. Prog. Neurobiol. 2012, 99, 81–91. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.A.; Lupski, J.R. Genomic Rearrangements and Gene Copy-Number Alterations as a Cause of Nervous System Disorders. Neuron 2006, 52, 103–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deshpande, A.; Weiss, L.A. Recurrent Reciprocal Copy Number Variants: Roles and Rules in Neurodevelopmental Disorders. Dev. Neurobiol. 2018, 78, 519–530. [Google Scholar] [CrossRef]
- Zarrei, M.; Burton, C.L.; Engchuan, W.; Young, E.J.; Higginbotham, E.J.; MacDonald, J.R.; Trost, B.; Chan, A.J.S.; Walker, S.; Lamoureux, S.; et al. A Large Data Resource of Genomic Copy Number Variation across Neurodevelopmental Disorders. NPJ Genom. Med. 2019, 4, 26. [Google Scholar] [CrossRef] [Green Version]
- Chawner, S.J.R.A.; Owen, M.J.; Holmans, P.; Raymond, F.L.; Skuse, D.; Hall, J.; van den Bree, M.B.M. Genotype–Phenotype Associations in Children with Copy Number Variants Associated with High Neuropsychiatric Risk in the UK (IMAGINE-ID): A Case-Control Cohort Study. Lancet Psychiatry 2019, 6, 493–505. [Google Scholar] [CrossRef]
- Van Agt, H.; Verhoeven, L.; Van Den Brink, G.; De Koning, H. The Impact on Socio-Emotional Development and Quality of Life of Language Impairment in 8-Year-Old Children. Dev. Med. Child. Neurol. 2011, 53, 81–88. [Google Scholar] [CrossRef]
- Vyshedskiy, A.; Mahapatra, S.; Dunn, R. Linguistically Deprived Children: Meta-Analysis of Published Research Underlines the Importance of Early Syntactic Language Use for Normal Brain Development. Res. Ideas Outcomes 2017, 3, e20696. [Google Scholar] [CrossRef] [Green Version]
- Carpenter, J.L.; Drabick, D.A.G. Co-Occurrence of Linguistic and Behavioural Difficulties in Early Childhood: A Developmental Psychopathology Perspective. Early Child. Dev. Care 2011, 181, 1021–1045. [Google Scholar] [CrossRef]
- Nudel, R.; Christiani, C.A.J.; Ohland, J.; Uddin, M.J.; Hemager, N.; Ellersgaard, D.V.; Spang, K.S.; Burton, B.K.; Greve, A.N.; Gantriis, D.L.; et al. Language Deficits in Specific Language Impairment, Attention Deficit/Hyperactivity Disorder, and Autism Spectrum Disorder: An Analysis of Polygenic Risk. Autism Res. 2020, 13, 369–381. [Google Scholar] [CrossRef]
- Geurts, H.M.; Embrechts, M. Language Profiles in ASD, SLI, and ADHD. J. Autism Dev. Disord. 2008, 38, 1931–1943. [Google Scholar] [CrossRef]
- Norbury, C.F.; Nash, M.; Baird, G.; Bishop, D.V.M. Using a Parental Checklist to Identify Diagnostic Groups in Children with Communication Impairment: A Validation of the Children’s Communication Checklist—2. Int. J. Lang. Commun. Disord. 2004, 39, 345–364. [Google Scholar] [CrossRef] [PubMed]
- Solot, C.B.; Sell, D.; Mayne, A.; Baylis, A.L.; Persson, C.; Jackson, O.; McDonald-McGinn, D.M. Speech-Language Disorders in 22q11.2 Deletion Syndrome: Best Practices for Diagnosis and Management. Am. J. Speech Lang. Pathol. 2019, 28, 984–999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Den Heuvel, E.; Manders, E.; Swillen, A.; Zink, I. Atypical Language Characteristics and Trajectories in Children with 22q11.2 Deletion Syndrome. J. Commun. Disord. 2018, 75, 37–56. [Google Scholar] [CrossRef] [PubMed]
- Antshel, K.M.; Aneja, A.; Strunge, L.; Peebles, J.; Fremont, W.P.; Stallone, K.; AbdulSabur, N.; Higgins, A.M.; Shprintzen, R.J.; Kates, W.R. Autistic Spectrum Disorders in Velo-Cardio Facial Syndrome (22q11.2 Deletion). J. Autism Dev. Disord. 2007, 37, 1776–1786. [Google Scholar] [CrossRef]
- Fine, S.E.; Weissman, A.; Gerdes, M.; Pinto-Martin, J.; Zackai, E.H.; McDonald-McGinn, D.M.; Emanuel, B.S. Autism Spectrum Disorders and Symptoms in Children with Molecularly Confirmed 22q11.2 Deletion Syndrome. J. Autism Dev. Disord. 2005, 35, 461–470. [Google Scholar] [CrossRef]
- Jalal, R.; Nair, A.; Lin, A.; Eckfeld, A.; Kushan, L.; Zinberg, J.; Karlsgodt, K.H.; Cannon, T.D.; Bearden, C.E. Social Cognition in 22q11.2 Deletion Syndrome and Idiopathic Developmental Neuropsychiatric Disorders. J. Neurodev. Disord. 2021, 13, 15. [Google Scholar] [CrossRef]
- Van Den Heuvel, E.; Jonkers, E.; Rombouts, E.; Manders, E.; Zink, I.; Swillen, A. Exploratory Study on Cognitive Abilities and Social Responsiveness in Children with 22q11.2 Deletion Syndrome (22q11DS) and Children with Idiopathic Intellectual Disability (IID). Res. Dev. Disabil. 2018, 81, 89–102. [Google Scholar] [CrossRef]
- Verbesselt, J.; Zink, I.; Breckpot, J.; Swillen, A. Cross-sectional and Longitudinal Findings in Patients with Proximal 22q11.2 Duplication: A Retrospective Chart Study. Am. J. Med. Genet. A 2022, 188, 46–57. [Google Scholar] [CrossRef]
- Van Campenhout, S.; Devriendt, K.; Breckpot, J.; Frijns, J.-P.; Peeters, H.; Van Buggenhout, G.; Van Esch, H.; Maes, B.; Swillen, A. Microduplication 22q11.2: A Description of the Clinical, Developmental and Behavioral Characteristics during Childhood. Genet. Couns. 2012, 23, 135–147. [Google Scholar]
- Yu, A.; Turbiville, D.; Xu, F.; Ray, J.W.; Britt, A.D.; Lupo, P.J.; Jain, S.K.; Shattuck, K.E.; Robinson, S.S.; Dong, J. Genotypic and Phenotypic Variability of 22q11.2 Microduplications: An Institutional Experience. Am. J. Med. Genet. A 2019, 179, 2178–2189. [Google Scholar] [CrossRef]
- Portnoï, M.-F. Microduplication 22q11.2: A New Chromosomal Syndrome. Eur. J. Med. Genet. 2009, 52, 88–93. [Google Scholar] [CrossRef] [PubMed]
- Woodward, K.J.; Stampalia, J.; Vanyai, H.; Rijhumal, H.; Potts, K.; Taylor, F.; Peverall, J.; Grumball, T.; Sivamoorthy, S.; Alinejad-Rokny, H.; et al. Atypical Nested 22q11.2 Duplications between LCR22B and LCR22D Are Associated with Neurodevelopmental Phenotypes Including Autism Spectrum Disorder with Incomplete Penetrance. Mol. Genet. Genom. Med. 2019, 7, e00507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wenger, T.L.; Miller, J.S.; DePolo, L.M.; de Marchena, A.B.; Clements, C.C.; Emanuel, B.S.; Zackai, E.H.; McDonald-McGinn, D.M.; Schultz, R.T. 22q11.2 Duplication Syndrome: Elevated Rate of Autism Spectrum Disorder and Need for Medical Screening. Mol. Autism 2016, 7, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Constantino, J.N.; Gruber, C.P. Social Responsiveness Scale (SRS); Western Psychological Services: Los Angeles, CA, USA, 2005. [Google Scholar]
- Clements, C.C.; Wenger, T.L.; Zoltowski, A.R.; Bertollo, J.R.; Miller, J.S.; De Marchena, A.B.; Mitteer, L.M.; Carey, J.C.; Yerys, B.E.; Zackai, E.H.; et al. Critical Region within 22q11.2 Linked to Higher Rate of Autism Spectrum Disorder. Mol. Autism 2017, 8, 58. [Google Scholar] [CrossRef] [Green Version]
- Drmic, I.E.; MacKinnon Modi, B.; McConnell, B.; Jilderda, S.; Hoang, N.; Noor, A.; Bassett, A.S.; Speevak, M.; Stavropoulos, D.J.; Carter, M.T. Neurodevelopmental Functioning in Probands and Non-proband Carriers of 22q11.2 Microduplication. Am. J. Med. Genet. A 2022, 188, 2999–3008. [Google Scholar] [CrossRef]
- Lin, A.; Vajdi, A.; Kushan-Wells, L.; Helleman, G.; Hansen, L.P.; Jonas, R.K.; Jalbrzikowski, M.; Kingsbury, L.; Raznahan, A.; Bearden, C.E. Reciprocal Copy Number Variations at 22q11.2 Produce Distinct and Convergent Neurobehavioral Impairments Relevant for Schizophrenia and Autism Spectrum Disorder. Biol. Psychiatry 2020, 88, 260–272. [Google Scholar] [CrossRef]
- Bennetts, S.K.; Mensah, F.K.; Westrupp, E.M.; Hackworth, N.J.; Reilly, S. The Agreement between Parent-Reported and Directly Measured Child Language and Parenting Behaviors. Front. Psychol. 2016, 7, 1710. [Google Scholar] [CrossRef] [Green Version]
- Garibaldi, A.; Venkatesh, L.; Bhat, J.S.; Boominathan, P. Relationship between Parental Report of Language Skills and Children’s Performance among 3-Year-Olds: Implications for Screening Language among Preschoolers. Int. J. Pediatr. Otorhinolaryngol. 2021, 151, 110943. [Google Scholar] [CrossRef]
- Bishop, D.V.M.; McDonald, D. Identifying Language Impairment in Children: Combining Language Test Scores with Parental Report. Int. J. Lang. Commun. Disord. 2009, 44, 600–615. [Google Scholar] [CrossRef] [Green Version]
- Van Roy, B.; Groholt, B.; Heyerdahl, S.; Clench-Aas, J. Understanding Discrepancies in Parent-Child Reporting of Emotional and Behavioural Problems: Effects of Relational and Socio-Demographic Factors. BMC Psychiatry 2010, 10, 56. [Google Scholar] [CrossRef] [Green Version]
- Bishop, D.V.M. Children’s Communication Checklist-2: CCC-2-NL; Geurts, H.M., Ed.; Pearson Assessment and Information B.V.: Amsterdam, The Netherlands, 2016. [Google Scholar]
- Constantino, J.N.; Gruber, C.P. Social Responsiveness Scale—Second Edition (SRS-2); Western Psychological Services: Torrance, CA, USA, 2012. [Google Scholar]
- Jacquemont, S.; Reymond, A.; Zufferey, F.; Harewood, L.; Walters, R.G.; Kutalik, Z.; Martinet, D.; Shen, Y.; Valsesia, A.; Beckmann, N.D.; et al. Mirror Extreme BMI Phenotypes Associated with Gene Dosage at the Chromosome 16p11.2 Locus. Nature 2011, 478, 97–102. [Google Scholar] [CrossRef]
- Mervis, C.B. Cross-Etiology Comparisons of Cognitive and Language Development. In Developmental Language Disorders—From Phenotypes to Etiologies; Lawrence Erlbaum Associates, Publishers: Mahwah, NJ, USA, 2004; pp. 153–186. ISBN 0-8058-4662-X. [Google Scholar]
- Cummins, J. Language, Power and Pedagogy—Bilingual Children in the Crossfire; Multilingual Matters Ltd.: Clevedon, UK, 2000; ISBN 1-85359-474-1. [Google Scholar]
- Kohnert, K.; Ebert, K.D.; Pham, G.T. Language Disorders in Bilingual Children; Plural Publishing Inc.: San Diego, CA, USA, 2021; ISBN 9781635501896. [Google Scholar]
- De Houwer, A. Bilingual Development in Childhood (Elements in Child Development); Cambridge University Press: Cambridge, UK, 2021; ISBN 978-1-108-79139-7. [Google Scholar]
- Crosbie, S.; Holm, A.; Wandschneider, S.; Hemsley, G. Narrative Skills of Children Born Preterm. Int. J. Lang. Commun. Disord. 2011, 46, 83–94. [Google Scholar] [CrossRef] [PubMed]
- Barre, N.; Morgan, A.; Doyle, L.W.; Anderson, P.J. Language Abilities in Children Who Were Very Preterm and/or Very Low Birth Weight: A Meta-Analysis. J. Pediatr. 2011, 158, 766–774.e1. [Google Scholar] [CrossRef] [PubMed]
- Bruining, H.; de Sonneville, L.; Swaab, H.; de Jonge, M.; Kas, M.; van Engeland, H.; Vorstman, J. Dissecting the Clinical Heterogeneity of Autism Spectrum Disorders through Defined Genotypes. PLoS ONE 2010, 5, e10887. [Google Scholar] [CrossRef] [Green Version]
- Van Den Heuvel, E.; Manders, E.; Swillen, A.; Zink, I. Parental Report on Socio-Communicative Behaviours in Children with 22q11.2 Deletion Syndrome. J. Intellect. Dev. Disabil. 2017, 42, 162–172. [Google Scholar] [CrossRef]
- Geurts, H. CCC-2-NL Children’s Communication Checklist—Second Edition—Nederlandse Versie [CCC-2- NL: Dutch Edition. Manual]; Pearson Assessment and Information B.V.: Amsterdam, The Netherlands, 2007. [Google Scholar]
- Bishop, D.V.M. The Children’s Communication Checklist-2; Psychological Corporation: London, UK, 2003. [Google Scholar]
- Bishop, D.V.M. Development of the Children’s Communication Checklist (CCC): A Method for Assessing Qualitative Aspects of Communicative Impairment in Children. J. Child. Psychol. Psychiatry 1998, 39, 879–891. [Google Scholar] [CrossRef]
- Roeyers, H.; Thys, M.; Druart, C.; De Schryver, M.; Schittekatte, M. Screeningslijst Voor Autismespectrumstoornissen (SRS-2); Hogrefe: Amsterdam, The Netherlands, 2015. [Google Scholar]
- Bruni, T.P. Test Review: Social Responsiveness Scale–Second Edition (SRS-2). J. Psychoeduc. Assess. 2014, 32, 365–369. [Google Scholar] [CrossRef]
- Roeyers, H.; Thys, M.; Druart, C.; De Schryver, M.; Schittekatte, M. SRS: Screeningslijst Voor Autismespectrumstoornissen; Hogrefe: Amsterdam, The Netherlands, 2011. [Google Scholar]
- American Psychiatric Association. DSM-5 and Diagnoses for Children. Am. Psychiatr. Assoc. 2013, 32, 91–93. [Google Scholar]
- Olsson, C. The Use of Communicative Functions among Pre-School Children with Multiple Disabilities in Two Different Setting Conditions: Group Versus Individual Patterns. Augment. Altern. Commun. 2005, 21, 3–18. [Google Scholar] [CrossRef]
- JASP Team JASP, Version 0.16.3; Jasp Team: Amsterdam, The Netherlands, 2022.
- R Core Team. R: A Language and Environment for Statistical Computing; R Core Team: Vienna, Austria, 2017. [Google Scholar]
- Wickham, H. Ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016; ISBN 978-3-319-24277-4. [Google Scholar]
- Pizzo, L.; Jensen, M.; Polyak, A.; Rosenfeld, J.A.; Mannik, K.; Krishnan, A.; McCready, E.; Pichon, O.; Le Caignec, C.; Van Dijck, A.; et al. Rare Variants in the Genetic Background Modulate Cognitive and Developmental Phenotypes in Individuals Carrying Disease-Associated Variants. Genet. Med. 2019, 21, 816–825. [Google Scholar] [CrossRef] [Green Version]
- De Smedt, B.; Devriendt, K.; Fryns, J.P.; Vogels, A.; Gewillig, M.; Swillen, A. Intellectual Abilities in a Large Sample of Children with Velo-Cardio-Facial Syndrome: An Update. J. Intellect. Disabil. Res. 2007, 51, 666–670. [Google Scholar] [CrossRef] [PubMed]
- Niklasson, L.; Rasmussen, P.; Óskarsdóttir, S.; Gillberg, C. Autism, ADHD, Mental Retardation and Behavior Problems in 100 Individuals with 22q11 Deletion Syndrome. Res. Dev. Disabil. 2009, 30, 763–773. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| 22q11.2DS | 22q11.2Dup | Siblings of Dup | |
|---|---|---|---|
| Sample Size (n) | 19 | 19 | 11 |
| Sex (n, %) | |||
| Male | 14 (74%) | 10 (53%) | 4 (36%) |
| Female | 5 (26%) | 9 (47%) | 7 (64%) |
| Chronological age (years·mo) | |||
| Average (SD) | 10.7 (2.5) | 10.7 (2.5) | 10.10 (2.10) |
| Median | 11.2 | 11 | 11 |
| Range | 6.7–14.4 | 6.8–14.9 | 6.3–16.1 |
| Country of residence (n, %) | |||
| Belgium | 15 (79%) | 10 (53%) | 5 (45%) |
| The Netherlands | 4 (21%) | 9 (47%) | 6 (55%) |
| Type of education (n, %) | |||
| Special education | 14 (74%) | 12 (63%) | 0 (0%) |
| Regular education | 5 (26%) | 7 (37%) | 11 (100%) |
| Speech-language delays (n, %) | 18 (95%) | 15 (79%) | 0 (0%) |
| Speech-language therapy (n, %) | 19 (100%) | 16 (84%) | 3 (27%) |
| Formal NDD diagnoses (n, %) | |||
| ASD | 8 (42%) | 2 (11%) | 0 (0%) |
| ADHD | 4 (21%) | 4 (21%) | 0 (0%) |
| SLD | 1 (5%) | 4 (21%) | 0 (0%) |
| DCD | 0 (0%) | 4 (21%) | 0 (0%) |
| DLD | 0 (0%) | 3 (16%) | 0 (0%) |
| CVI | 0 (0%) | 3 (16%) | 0 (0%) |
| Inheritance pattern (n, %) | |||
| De novo | 18 (95%) | 8 (42%) | |
| Inherited | 1 (5%) | 8 (42%) | / |
| Unknown | 0 (0%) | 3 (16%) |
| 22q11.2Dup (n = 19) | 22q11.2DS (n = 19) | t-Test t =, p = | 22q11.2Dup (n = 11) | Siblings Dup (n = 11) | t-Test t =, p = | |
|---|---|---|---|---|---|---|
| CCC-2 GCC Mean (SD) | 101.58 (20.29) | 114.12 (14.99) | t = −2.281 | 98.36 (19.67) | 80.55 (16.01) | t = 2.647 |
| Range | 72.00–135.00 | 81.00–138.00 | p = 0.035 * | 72.00–132.00 | 62.00–108.00 | p = 0.024 * |
| CCC-2 PC Mean (SD) | 50.58 (10.25) | 56.63 (7.59) | t = −2.190 | 49.27 (8.79) | 39.09 (8.57) | t = 3.136 |
| Range | 31.00–69.00 | 36.00–69.00 | p = 0.042 * | 38.00–65.00 | 24.00–56.00 | p = 0.011 * |
| SRS-2 SCI Mean (SD) | 66.05 (20.07) | 73.47 (15.09) | t = −1.313 | 58.18 (13.00) | 48.36 (7.50) | t = 2.276 |
| Range | 43.00–111.00 | 50.00–100.00 | p = 0.206 | 43.00–89.00 | 39.00–62.00 | p = 0.046 * |
| SRS-2 RIB Mean (SD) | 65.53 (19.94) | 82.05 (19.97) | t = −2.327 | 57.27 (12.33) | 46.64 (9.00) | t = 2.241 |
| Range | 45.00–113.00 | 51.00–128.00 | p = 0.032 * | 45.00–86.00 | 36.00–71.00 | p = 0.049 * |
| SRS-2 Total Mean (SD) | 66.79 (21.06) | 76.05 (16.28) | t = −1.508 | 58.46 (13.46) | 47.82 (7.79) | t = 2.292 |
| Range | 44.00–114.00 | 50.00–108.00 | p = 0.149 | 44.00–91.00 | 40.00–64.00 | p = 0.045 * |
| 22q11.2DS (n = 19) | 22q11.2Dup (n = 19) | Siblings of Dup (n = 11) | |
|---|---|---|---|
| CCC-2 GCC | 15/19 (79%) | 9/19 (47%) | 1/11 (9%) |
| CCC-2 PC | 13/19 (68%) | 7/19 (37%) | 1/11 (9%) |
| SRS-2 SCI | 14/19 (74%) | 9/19 (47%) | 2/11 (18%) |
| SRS-2 RIB | 18/19 (95%) | 9/19 (47%) | 1/11 (9%) |
| SRS-2 Total | 15/19 (79%) | 9/19 (47%) | 1/11 (9%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Verbesselt, J.; Van Den Heuvel, E.; Breckpot, J.; Zink, I.; Swillen, A. Parent-Reported Social-Communicative Skills of Children with 22q11.2 Copy Number Variants and Siblings. Genes 2022, 13, 1801. https://0-doi-org.brum.beds.ac.uk/10.3390/genes13101801
Verbesselt J, Van Den Heuvel E, Breckpot J, Zink I, Swillen A. Parent-Reported Social-Communicative Skills of Children with 22q11.2 Copy Number Variants and Siblings. Genes. 2022; 13(10):1801. https://0-doi-org.brum.beds.ac.uk/10.3390/genes13101801
Chicago/Turabian StyleVerbesselt, Jente, Ellen Van Den Heuvel, Jeroen Breckpot, Inge Zink, and Ann Swillen. 2022. "Parent-Reported Social-Communicative Skills of Children with 22q11.2 Copy Number Variants and Siblings" Genes 13, no. 10: 1801. https://0-doi-org.brum.beds.ac.uk/10.3390/genes13101801