
Postoperative Hypocalcemia following Non-Cardiac Surgical Procedures in Children with 22q11.2 Deletion Syndrome †
 , , and
, , and
Abstract
:1. Introduction
2. Methods
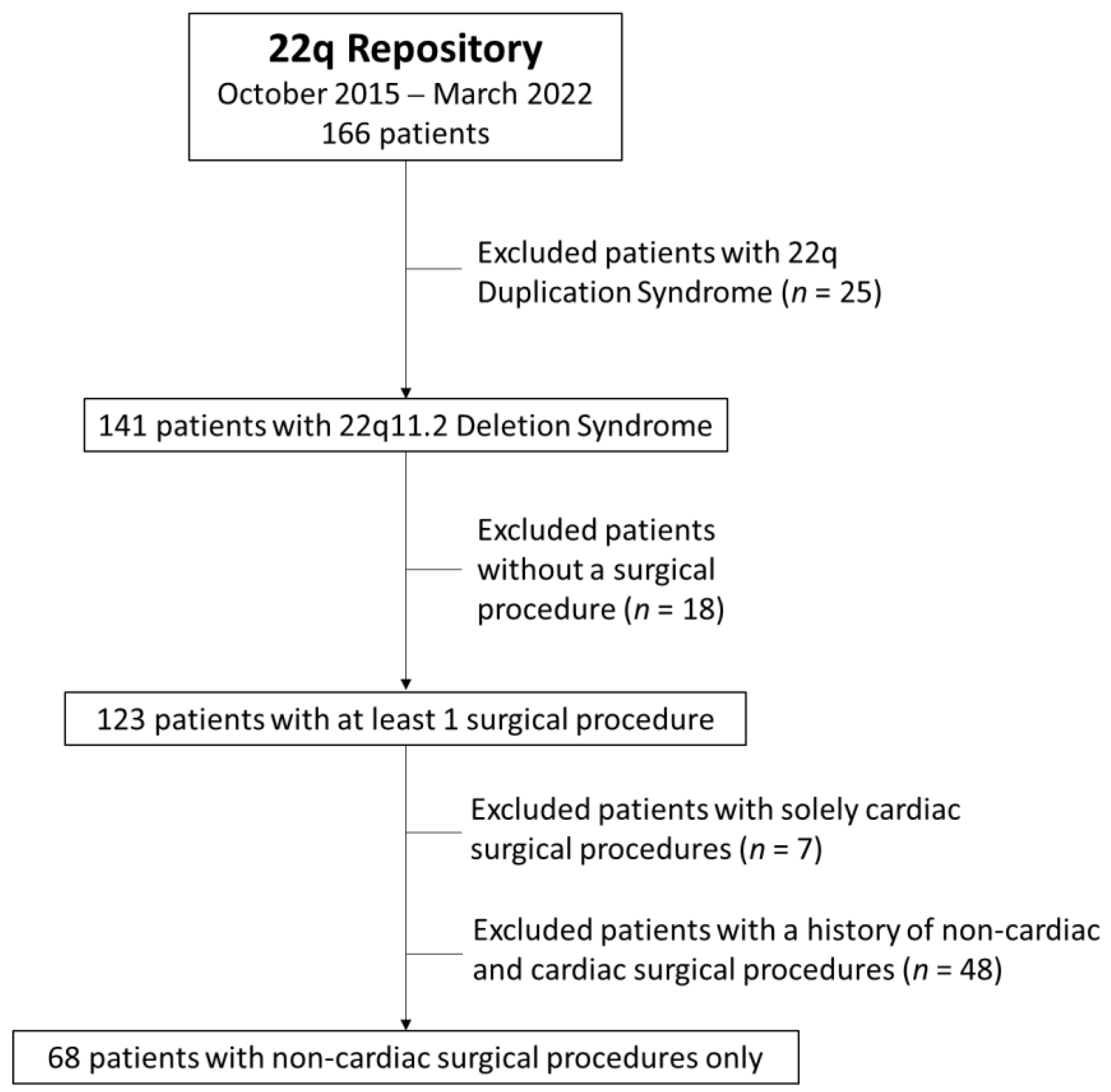
2.1. Study Design and Participants
2.2. Statistical Analysis
3. Results
3.1. Description of Study Participants
3.2. Calcium Testing
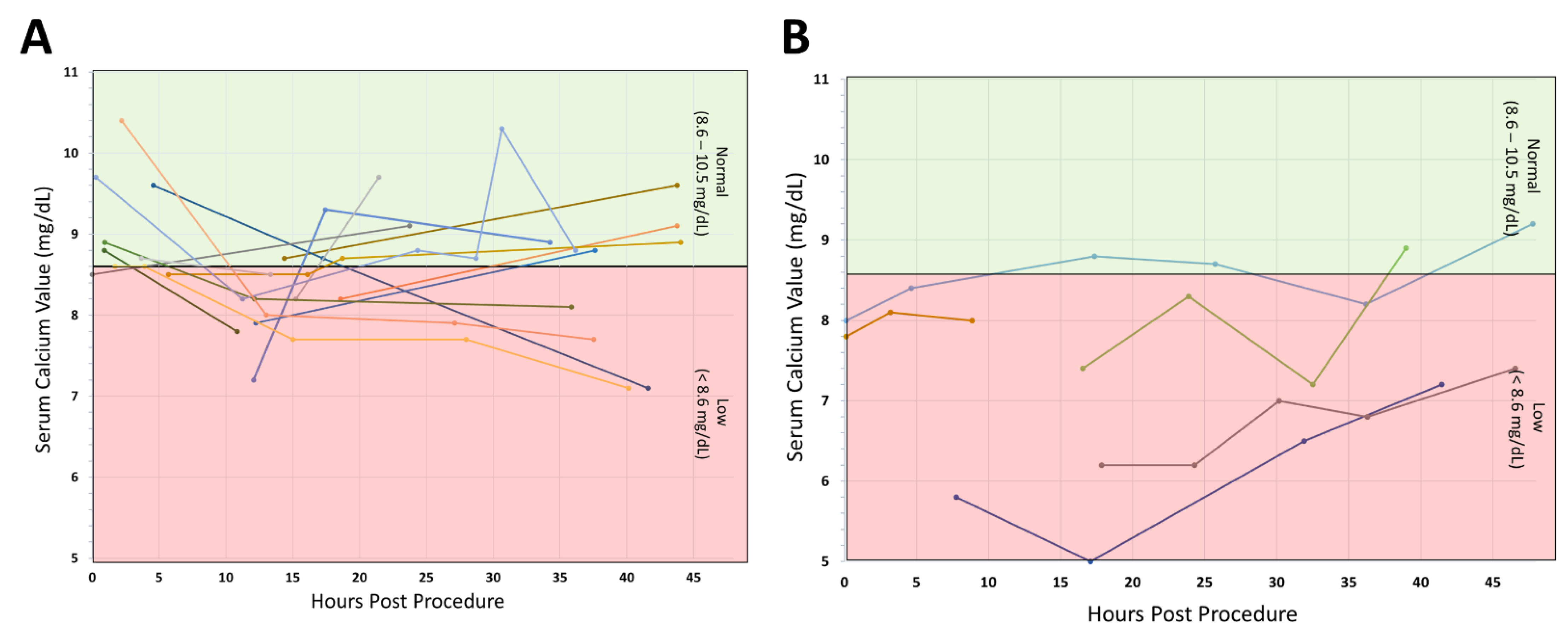
3.3. Postoperative Calcium Results and Hypocalcemia
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bassett, A.S.; McDonald-McGinn, D.M.; Devriendt, K.; Digilio, M.C.; Goldenberg, P.; Habel, A.; Marino, B.; Oskarsdottir, S.; Philip, N.; Sullivan, K.; et al. Practical guidelines for managing patients with 22q11.2 deletion syndrome. J. Pediatr. 2011, 159, 332–339.e1. [Google Scholar] [CrossRef] [PubMed]
- Mcdonald-Mcginn, D.M.; Tonnesen, M.K.; Laufer-Cahana, A.; Finucane, B.; A Driscoll, D.; Emanuel, B.S.; Zackai, E.H. Phenotype of the 22q11.2 deletion in individuals identified through an affected relative: Cast a wide FISHing net! Genet. Med. 2001, 3, 23–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oskarsdottir, S.; Persson, C.; Eriksson, B.O.; Fasth, A. Presenting phenotype in 100 children with the 22q11 deletion syndrome. Eur. J. Pediatr. 2005, 164, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Ryan, A.K.; Goodship, J.A.; Wilson, D.I.; Philip, N.; Levy, A.; Seidel, H.; Schuffenhauer, S.; Oechsler, H.; Belohradsky, B.; Prieur, M.; et al. Spectrum of clinical features associated with interstitial chromosome 22q11 deletions: A European collaborative study. J. Med. Genet. 1997, 34, 798–804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheung, E.N.M.; George, S.R.; Costain, G.A.; Andrade, D.; Chow, E.W.C.; Silversides, C.K.; Bassett, A.S. Prevalence of hypocalcaemia and its associated features in 22q11.2 deletion syndrome. Clin. Endocrinol. 2014, 81, 190–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brauner, R.; Gonneville, A.L.H.D.; Kindermans, C.; Le Bidois, J.; Prieur, M.; Lyonnet, S.; Souberbielle, J.-C. Parathyroid function and growth in 22q11.2 deletion syndrome. J. Pediatr. 2003, 142, 504–508. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.C.; Morris, G.; Wilson, D.; Davies, S.J.; Gregory, J.W. Hypoparathyroidism and 22q11 deletion syndrome. Arch. Dis. Child. 2003, 88, 520–522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kapadia, C.R.; Kim, Y.E.; McDonald-McGinn, D.M.; Zackai, E.H.; Katz, L.E.L. Parathyroid hormone reserve in 22q11.2 deletion syndrome. Genet. Med. 2008, 10, 224–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oikonomou, D.; Laina, A.; Xydaki, A.; Christopoulos, C. Steroid-induced hypocalcaemia with tetany in a patient with hypoparathyroidism. BMJ Case Rep. 2014, 2014, bcr2014207562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Onyema, M.C.; Kearney, J.; Dimitriadis, G.K. Glucocorticoid-Induced Hypocalcemia in a Patient with Established Hypoparathyroidism. Am. J. Med. 2021, 134, e321–e322. [Google Scholar] [CrossRef] [PubMed]
- Shen, L.; Gu, H.; Wang, D.; Yang, C.; Xu, Z.; Jing, H.; Jiang, Y.; Ding, Y.; Hou, H.; Ge, Z.; et al. Influence of chromosome 22q11.2 microdeletion on postoperative calcium level after cardiac-correction surgery. Pediatr. Cardiol. 2011, 32, 904–909. [Google Scholar] [CrossRef] [PubMed]
- Yeoh, T.Y.; Scavonetto, F.; Hamlin, R.J.; Burkhart, H.M.; Sprung, J.; Weingarten, T.N. Perioperative management of patients with DiGeorge syndrome undergoing cardiac surgery. J. Cardiothorac. Vasc. Anesth. 2014, 28, 983–989. [Google Scholar] [CrossRef]
- Yang, C.; Ge, J.; Zhang, R.; Chen, C.; Yi, L.; Shen, L. The Correlation Between Severity of Postoperative Hypocalcemia and Perioperative Mortality in Chromosome 22q11.2 Microdeletion (22q11DS) Patient After Cardiac-Correction Surgery: A Retrospective Analysis. Heart Surg. Forum. 2020, 23, E549–E554. [Google Scholar] [CrossRef]
- Cuturilo, G.; Drakulic, D.; Jovanovic, I.; Ilic, S.; Kalanj, J.; Vulicevic, I.; Raus, M.; Skoric, D.; Mijovic, M.; Medjo, B.; et al. The Impact of 22q11.2 Microdeletion on Cardiac Surgery Postoperative Outcome. Pediatr. Cardiol. 2017, 38, 1680–1685. [Google Scholar] [CrossRef] [PubMed]
- Putotto, C.; Pugnaloni, F.; Unolt, M.; Maiolo, S.; Trezzi, M.; Digilio, M.C.; Cirillo, A.; Limongelli, G.; Marino, B.; Calcagni, G.; et al. 22q11.2 Deletion Syndrome: Impact of Genetics in the Treatment of Conotruncal Heart Defects. Children 2022, 9, 772. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| All 22q11DS Patients (n = 141) | 22q11DS Patients with Only Non-Cardiac Surgeries (n = 68) | |
|---|---|---|
| Age at Surgery (years) mean (SD) | 3.6 (4.4) | 6.1 (4.2) |
| Male, n (%) | 82 (58) | 39 (57) |
| Race or ethnicity, n (%) | ||
| White | 117 (83) | 58 (85) |
| African American | 7 (5) | 3 (4) |
| Asian | 1 (1) | 1 (1) |
| American Indian/Alaska Native | 1 (1) | 1 (1) |
| Multiracial | 4 (3) | 1 (1) |
| Hispanic | 9 (6) | 4 (6) |
| Unknown | 1 (1) | 0 (0) |
| 22q11DS Breakpoints | ||
| A–B | 8 (6) | 5 (7) |
| A–C | 2 (1) | 0 (0) |
| A–D | 54 (38) | 30 (44) |
| B–D | 4 (3) | 3 (4) |
| C–D | 4 (3) | 2 (3) |
| Other | 2 (1) | 2 (3) |
| Unknown | 67 (48) | 26 (38) |
| Post-Op Ca * Testing (%) | Post-Op Hypocalcemia (%) | |
|---|---|---|
| History of Hypocalcemia ^ | 40 | 47 |
| No History of Hypocalcemia ^ | 60 | 53 |
| Subject ID | 22qDS Breakpoint | Any History of Hypocalcemia | Age at Procedure (Years) | Name of Surgery | Lowest Post-Op Ca † (mg/dL) | Lowest Post-Op Ionized Ca • (mmol/L) | Treatment |
|---|---|---|---|---|---|---|---|
| 1 | Unknown ◊ | − | 14.6 | Mammaplasty | 7.5 | ||
| 1 | 14.7 | Pharyngeal flap | 7.3 | 1.09 | |||
| 2 | A-D | + * | 0.1 | Ventriculoperitoneal shunt | 1.09 | ||
| 3 | Unknown ◊ | + * ^ | 0.5 | Gastrostomy tube | 8.2 | 1.05 | + a |
| 3 | 1.0 | Cleft palate repair | 7.9 | ||||
| 3 | 1.9 | ORIF | 5 | 0.73 | + ab | ||
| 3 | 15.1 | ORIF | 6.2 | 0.82 | + a | ||
| 4 | A-D | − | 0.2 | Gastrostomy tube | 8.2 | ||
| 4 | 1.3 | Superior adenoidectomy | 8.2 | ||||
| 5 | A-D | − | 3.5 | Cleft palate repair | 8.5 | ||
| 5 | 3.8 | Thoracotomy | 8.5 | ||||
| 6 | A-D | + * | 0.0 | Colostomy | 7.9 | ||
| 7 | Unknown ◊ | − | 12.8 | Spinal Fusion | 8.5 | ||
| 8 | A-D | + ^ | 10.7 | Spinal Fusion | 7 | ||
| 9 | A-D | + ^ | 6.7 | Pharyngeal flap | 8.1 | ||
| 10 | Unknown ◊ | − | 12.7 | Pharyngeal flap | 8 | 1.09 | |
| 11 | Unknown ◊ | + ^ | 5.4 | Adenotonsillectomy | 0.76 | ||
| 11 | 5.6 | Pharyngeal flap | 1.03 | ||||
| 12 | A-D | − | 6.6 | Spinal Fusion | 7.8 | ||
| 12 | 6.6 | Debridement of cervical wound | 7.9 | ||||
| 13 | Unknown ◊ | + * | 3.9 | Adenotonsillectomy | 8.4 | ||
| 13 | 9.1 | Debridement of scalp wound | 8.3 | ||||
| 14 | A-D | + ^ | 9.0 | Pharyngeal flap | 7.2 | 1.05 | + a |
| 15 | A-D | + ^ | 3.4 | Cleft palate repair | 8.2 | ||
| 15 | 5.3 | Adenotonsillectomy | 8.4 | ||||
| 15 | 5.5 | Pharyngeal flap | 8.4 | + a | |||
| 16 | A-B | + ^ | 5.5 | Pharyngeal flap | 8.2 | ||
| 17 | A-D | − | 8.3 | Pharyngeal flap | 7.8 | 1.04 | + a |
| 17 | 11.6 | Pharyngeal flap | 8 | + a | |||
| 18 | Unknown ◊ | + * | 5.7 | Pharyngeal flap | 7.4 | 0.98 | + a |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arganbright, J.M.; Tracy, M.; Feldt, M.; Narayanan, S.; Mahadev, A.; Noel-MacDonnell, J. Postoperative Hypocalcemia following Non-Cardiac Surgical Procedures in Children with 22q11.2 Deletion Syndrome. Genes 2022, 13, 1905. https://0-doi-org.brum.beds.ac.uk/10.3390/genes13101905
Arganbright JM, Tracy M, Feldt M, Narayanan S, Mahadev A, Noel-MacDonnell J. Postoperative Hypocalcemia following Non-Cardiac Surgical Procedures in Children with 22q11.2 Deletion Syndrome. Genes. 2022; 13(10):1905. https://0-doi-org.brum.beds.ac.uk/10.3390/genes13101905
Chicago/Turabian StyleArganbright, Jill M., Meghan Tracy, Max Feldt, Srivats Narayanan, Ashna Mahadev, and Janelle Noel-MacDonnell. 2022. "Postoperative Hypocalcemia following Non-Cardiac Surgical Procedures in Children with 22q11.2 Deletion Syndrome" Genes 13, no. 10: 1905. https://0-doi-org.brum.beds.ac.uk/10.3390/genes13101905