
Adult Height, 22q11.2 Deletion Extent, and Short Stature in 22q11.2 Deletion Syndrome
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Study Design
2.2. Analyses
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bassett, A.S.; McDonald-McGinn, D.M.; Devriendt, K.; Digilio, M.C.; Goldenberg, P.; Habel, A.; Marino, B.; Oskarsdottir, S.; Philip, N.; Sullivan, K.; et al. Practical guidelines for managing patients with 22q11.2 deletion syndrome. J. Pediatr. 2011, 159, 332–339.e1. [Google Scholar] [CrossRef] [PubMed]
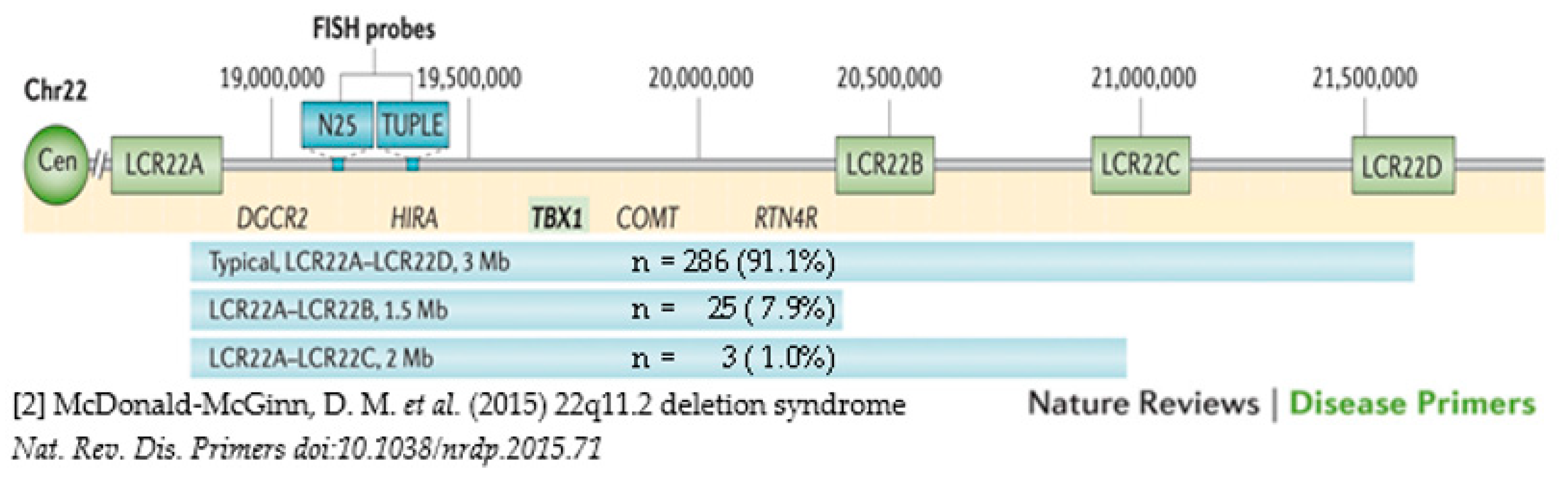
- McDonald-McGinn, D.M.; Sullivan, K.E.; Marino, B.; Philip, N.; Swillen, A.; Vorstman, J.A.; Zackai, E.H.; Emanuel, B.S.; Vermeesch, J.R.; Morrow, B.E.; et al. 22q11.2 deletion syndrome. Nat. Rev. Dis. Prim. 2015, 1, 15071. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blagojevic, C.; Heung, T.; Theriault, M.; Tomita-Mitchell, A.; Chakraborty, P.; Kernohan, K.; Bulman, D.E.; Bassett, A.S. Estimate of the contemporary live-birth prevalence of recurrent 22q11.2 deletions: A cross-sectional analysis from population-based newborn screening. Can. Med. Assoc. J. Open 2021, 9, E802–E809. [Google Scholar] [CrossRef] [PubMed]
- Habel, A.; McGinn, M.J., 2nd; Zackai, E.H.; Unanue, N.; McDonald-McGinn, D.M. Syndrome-specific growth charts for 22q11.2 deletion syndrome in Caucasian children. Am. J. Med. Genet. A 2012, 158, 2665–2671. [Google Scholar] [CrossRef]
- Digilio, M.C.; Marino, B.; Cappa, M.; Cambiaso, P.; Giannotti, A.; Dallapiccola, B. Auxological evaluation in patients with DiGeorge/velocardiofacial syndrome (deletion 22q11.2 syndrome). Genet. Med. 2001, 3, 30–33. [Google Scholar] [CrossRef] [Green Version]
- Fung, W.L.; Butcher, N.J.; Costain, G.; Andrade, D.M.; Boot, E.; Chow, E.W.; Chung, B.; Cytrynbaum, C.; Faghfoury, H.; Fishman, L.; et al. Practical guidelines for managing adults with 22q11.2 deletion syndrome. Genet. Med. 2015, 17, 599–609. [Google Scholar] [CrossRef] [Green Version]
- Dauber, A.; Yu, Y.; Turchin, M.C.; Chiang, C.W.; Meng, Y.A.; Demerath, E.W.; Patel, S.R.; Rich, S.S.; Rotter, J.I.; Schreiner, P.J.; et al. Genome-wide association of copy-number variation reveals an association between short stature and the presence of low-frequency genomic deletions. Am. J. Hum. Genet. 2011, 89, 751–759. [Google Scholar] [CrossRef] [Green Version]
- van Duyvenvoorde, H.A.; Lui, J.C.; Kant, S.G.; Oostdijk, W.; Gijsbers, A.C.; Hoffer, M.J.; Karperien, M.; Walenkamp, M.J.; Noordam, C.; Voorhoeve, P.G.; et al. Copy number variants in patients with short stature. Eur. J. Hum. Genet. 2014, 22, 602–609. [Google Scholar] [CrossRef] [Green Version]
- Zahnleiter, D.; Uebe, S.; Ekici, A.B.; Hoyer, J.; Wiesener, A.; Wieczorek, D.; Kunstmann, E.; Reis, A.; Doerr, H.G.; Rauch, A.; et al. Rare copy number variants are a common cause of short stature. PLoS Genet. 2013, 9, e1003365. [Google Scholar] [CrossRef] [Green Version]
- Macé, A.; Tuke, M.A.; Deelen, P.; Kristiansson, K.; Mattsson, H.; Noukas, M.; Sapkota, Y.; Schick, U.; Porcu, E.; Rueger, S.; et al. CNV-association meta-analysis in 191,161 European adults reveals new loci associated with anthropometric traits. Nat. Commun. 2017, 8, 744. [Google Scholar] [CrossRef]
- Owen, D.; Bracher-Smith, M.; Kendall, K.M.; Rees, E.; Einon, M.; Escott-Price, V.; Owen, M.J.; O’Donovan, M.C.; Kirov, G. Effects of pathogenic CNVs on physical traits in participants of the UK Biobank. BMC Genom. 2018, 19, 867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blagojevic, C.; Heung, T.; Malecki, S.; Ying, S.; Cancelliere, S.; Hegele, R.A.; Bassett, A.S. Hypertriglyceridemia in young adults with a 22q11.2 microdeletion. Eur. J. Endocrinol. 2022, 187, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Harris, M.A.; Brett, C.E.; Deary, I.J.; Starr, J.M. Associations among height, body mass index and intelligence from age 11 to age 78 years. BMC Geriatr. 2016, 16, 167. [Google Scholar] [CrossRef] [Green Version]
- Kanazawa, S.; Reyniers, D.J. The role of height in the sex difference in intelligence. Am. J. Psychol. 2009, 122, 527–536. [Google Scholar] [PubMed]
- Le Roy, C.; Larios, G.; Claveria, C.; Springmuller, D. Short stature among children undergoing cardiac surgery for congenital heart defects. Arch. Argent. Pediatr. 2019, 117, e211–e217. [Google Scholar] [CrossRef]
- Peres, M.B.; Croti, U.A.; Godoy, M.F.; De Marchi, C.H.; Hassem Sobrinho, S.; Beani, L.; Moscardini, A.C.; Braile, D.M. Evolution of weight and height of children with congenital heart disease undergoing surgical treatment. Rev. Bras. Cir. Cardiovasc. 2014, 29, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Billett, J.; Cowie, M.R.; Gatzoulis, M.A.; Vonder Muhll, I.F.; Majeed, A. Comorbidity, healthcare utilisation and process of care measures in patients with congenital heart disease in the UK: Cross-sectional, population-based study with case-control analysis. Heart 2008, 94, 1194–1199. [Google Scholar] [CrossRef] [Green Version]
- Van, L.; Heung, T.; Malecki, S.L.; Fenn, C.; Tyrer, A.; Sanches, M.; Chow, E.W.C.; Boot, E.; Corral, M.; Dash, S.; et al. 22q11.2 microdeletion and increased risk for type 2 diabetes. EClinicalMedicine 2020, 26, 100528. [Google Scholar] [CrossRef]
- Malecki, S.L.; Van Mil, S.; Graffi, J.; Breetvelt, E.; Corral, M.; Boot, E.; Chow, E.W.C.; Sanches, M.; Verma, A.A.; Bassett, A.S. A genetic model for multimorbidity in young adults. Genet. Med. 2020, 22, 132–141. [Google Scholar] [CrossRef]
- Rani, D.; Shrestha, R.; Kanchan, T.; Krishan, K. Short Stature; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Bassett, A.S.; Chow, E.W.; Husted, J.; Weksberg, R.; Caluseriu, O.; Webb, G.D.; Gatzoulis, M.A. Clinical features of 78 adults with 22q11 Deletion Syndrome. Am. J. Med. Genet. A 2005, 138, 307–313. [Google Scholar] [CrossRef]
- Humphreys, L.G.; Davey, T.C.; Park, R.K. Longitudinal correlation analysis of standing height and intelligence. Child. Dev. 1985, 56, 1465–1478. [Google Scholar] [CrossRef] [PubMed]
- Johnson, F.W. Biological factors and psychometric intelligence: A review. Genet. Soc. Gen. Psychol. Monogr. 1991, 117, 313–357. [Google Scholar] [PubMed]
- Lango Allen, H.; Estrada, K.; Lettre, G.; Berndt, S.I.; Weedon, M.N.; Rivadeneira, F.; Willer, C.J.; Jackson, A.U.; Vedantam, S.; Raychaudhuri, S.; et al. Hundreds of variants clustered in genomic loci and biological pathways affect human height. Nature 2010, 467, 832–838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marouli, E.; Graff, M.; Medina-Gomez, C.; Lo, K.S.; Wood, A.R.; Kjaer, T.R.; Fine, R.S.; Lu, Y.; Schurmann, C.; Highland, H.M.; et al. Rare and low-frequency coding variants alter human adult height. Nature 2017, 542, 186–190. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.; Guo, T.; Fiksinski, A.; Breetvelt, E.; McDonald-McGinn, D.M.; Crowley, T.B.; Diacou, A.; Schneider, M.; Eliez, S.; Swillen, A.; et al. Variance of IQ is partially dependent on deletion type among 1,427 22q11.2 deletion syndrome subjects. Am. J. Med. Genet. A 2018, 176, 2172–2181. [Google Scholar] [CrossRef]
- Mintz, C.S.; Seaver, L.H.; Irons, M.; Grimberg, A.; Lozano, R.; Practice, A.P.; Guidelines, C. Focused Revision: ACMG practice resource: Genetic evaluation of short stature. Genet. Med. 2021, 23, 813–815. [Google Scholar] [CrossRef]
- Fiksinski, A.M.; Heung, T.; Corral, M.; Breetvelt, E.J.; Costain, G.; Marshall, C.R.; Kahn, R.S.; Vorstman, J.A.S.; Bassett, A.S. Within-family influences on dimensional neurobehavioral traits in a high-risk genetic model. Psychol. Med. 2021, 1–9. [Google Scholar] [CrossRef]
- You, C.; Zhou, Z.; Wen, J.; Li, Y.; Pang, C.H.; Du, H.; Wang, Z.; Zhou, X.H.; King, D.A.; Liu, C.T.; et al. Polygenic Scores and Parental Predictors: An Adult Height Study Based on the United Kingdom Biobank and the Framingham Heart Study. Front. Genet. 2021, 12, 669441. [Google Scholar] [CrossRef]
- Yap, C.X.; Alvares, G.A.; Henders, A.K.; Lin, T.; Wallace, L.; Farrelly, A.; McLaren, T.; Berry, J.; Vinkhuyzen, A.A.E.; Trzaskowski, M.; et al. Analysis of common genetic variation and rare CNVs in the Australian Autism Biobank. Mol. Autism. 2021, 12, 12. [Google Scholar] [CrossRef]
- Yengo, L.; Vedantam, S.; Marouli, E.; Sidorenko, J.; Bartell, E.; Sakaue, S.; Graff, M.; Eliasen, A.U.; Jiang, Y.; Raghavan, S.; et al. A saturated map of common genetic variants associated with human height. Nature 2022, 610, 704–712. [Google Scholar] [CrossRef]
- Cleynen, I.; Engchuan, W.; Hestand, M.S.; Heung, T.; Holleman, A.M.; Johnston, H.R.; Monfeuga, T.; McDonald-McGinn, D.M.; Gur, R.E.; Morrow, B.E.; et al. Genetic contributors to risk of schizophrenia in the presence of a 22q11.2 deletion. Mol. Psychiatry 2021, 26, 4496–4510. [Google Scholar] [CrossRef] [PubMed]
- Guna, A.; Butcher, N.J.; Bassett, A.S. Comparative mapping of the 22q11.2 deletion region and the potential of simple model organisms. J. Neurodev. Disord. 2015, 7, 18. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Subgroup with Known Deletion Length (n = 314) | Short Stature | Statistics | ||
|---|---|---|---|---|---|
| Yes (n = 71) | No (n = 243) | ||||
| Categorical | n | % | n (%) | n (%) | p-value 2 |
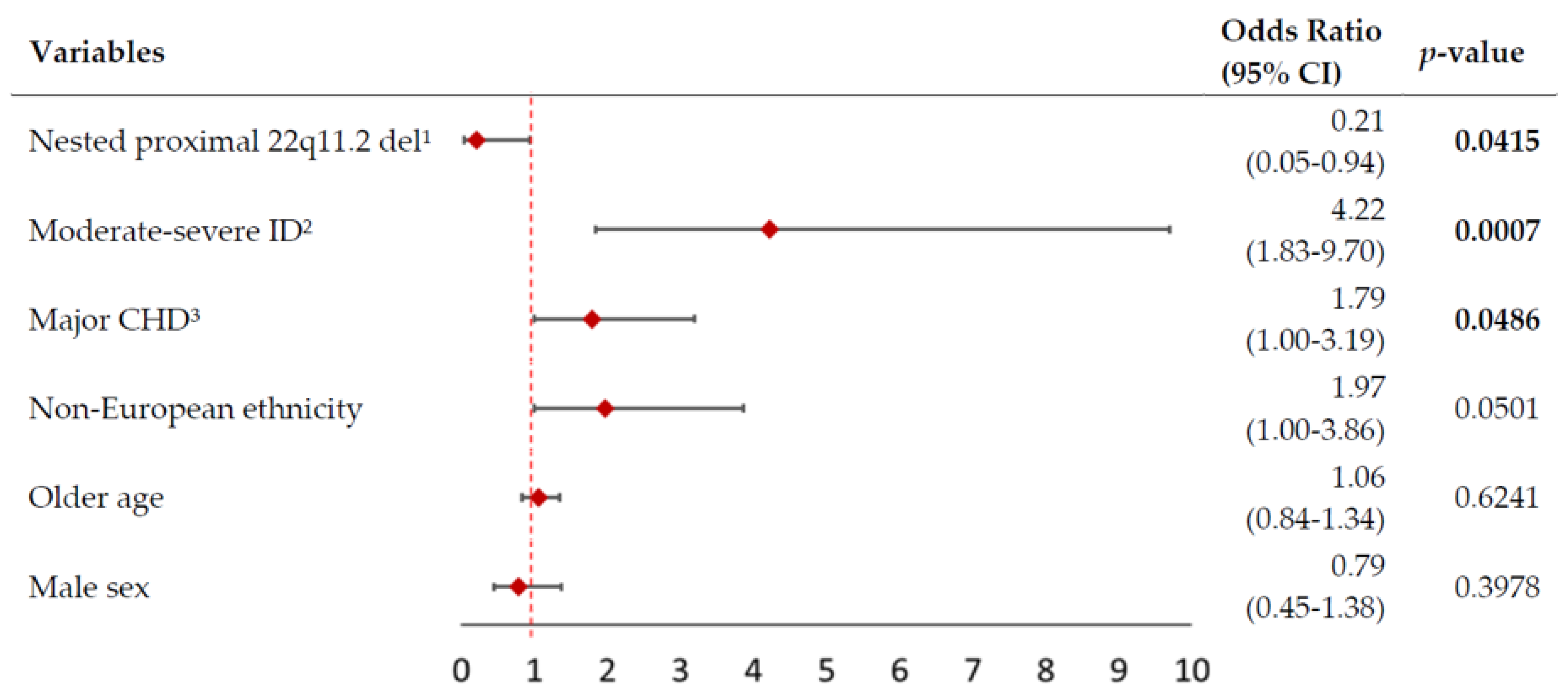
| Moderate–severe intellectual disability | 28 | 8.9 | 14 (19.7) | 14 (05.8) | 0.0003 |
| Major congenital cardiac disease | 104 | 33.1 | 31 (43.7) | 73 (30.0) | 0.0319 |
| Nested proximal 22q11.2 deletion 1 | 28 | 8.9 | 2 (02.8) | 26 (10.7) | 0.0403 |
| Non-European ancestry | 67 | 21.3 | 20 (28.2) | 47 (19.3) | 0.1102 |
| Male sex | 155 | 49.4 | 33 (46.5) | 122 (50.2) | 0.5806 |
| Continuous | Median (range) | ||||
| Median age (range) at height (years) | 314 | 100 | 34.0 (19.0–67.3) | 35.0 (18.0–76.3) | 0.5537 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heung, T.; Conroy, B.; Malecki, S.; Ha, J.; Boot, E.; Corral, M.; Bassett, A.S. Adult Height, 22q11.2 Deletion Extent, and Short Stature in 22q11.2 Deletion Syndrome. Genes 2022, 13, 2038. https://0-doi-org.brum.beds.ac.uk/10.3390/genes13112038
Heung T, Conroy B, Malecki S, Ha J, Boot E, Corral M, Bassett AS. Adult Height, 22q11.2 Deletion Extent, and Short Stature in 22q11.2 Deletion Syndrome. Genes. 2022; 13(11):2038. https://0-doi-org.brum.beds.ac.uk/10.3390/genes13112038
Chicago/Turabian StyleHeung, Tracy, Brigid Conroy, Sarah Malecki, Joanne Ha, Erik Boot, Maria Corral, and Anne S. Bassett. 2022. "Adult Height, 22q11.2 Deletion Extent, and Short Stature in 22q11.2 Deletion Syndrome" Genes 13, no. 11: 2038. https://0-doi-org.brum.beds.ac.uk/10.3390/genes13112038