Impact of CYP2C9 and VKORC1 Polymorphisms on Warfarin Sensitivity and Responsiveness in Jordanian Cardiovascular Patients during the Initiation Therapy


Abstract
:1. Introduction
2. Materials and Methods
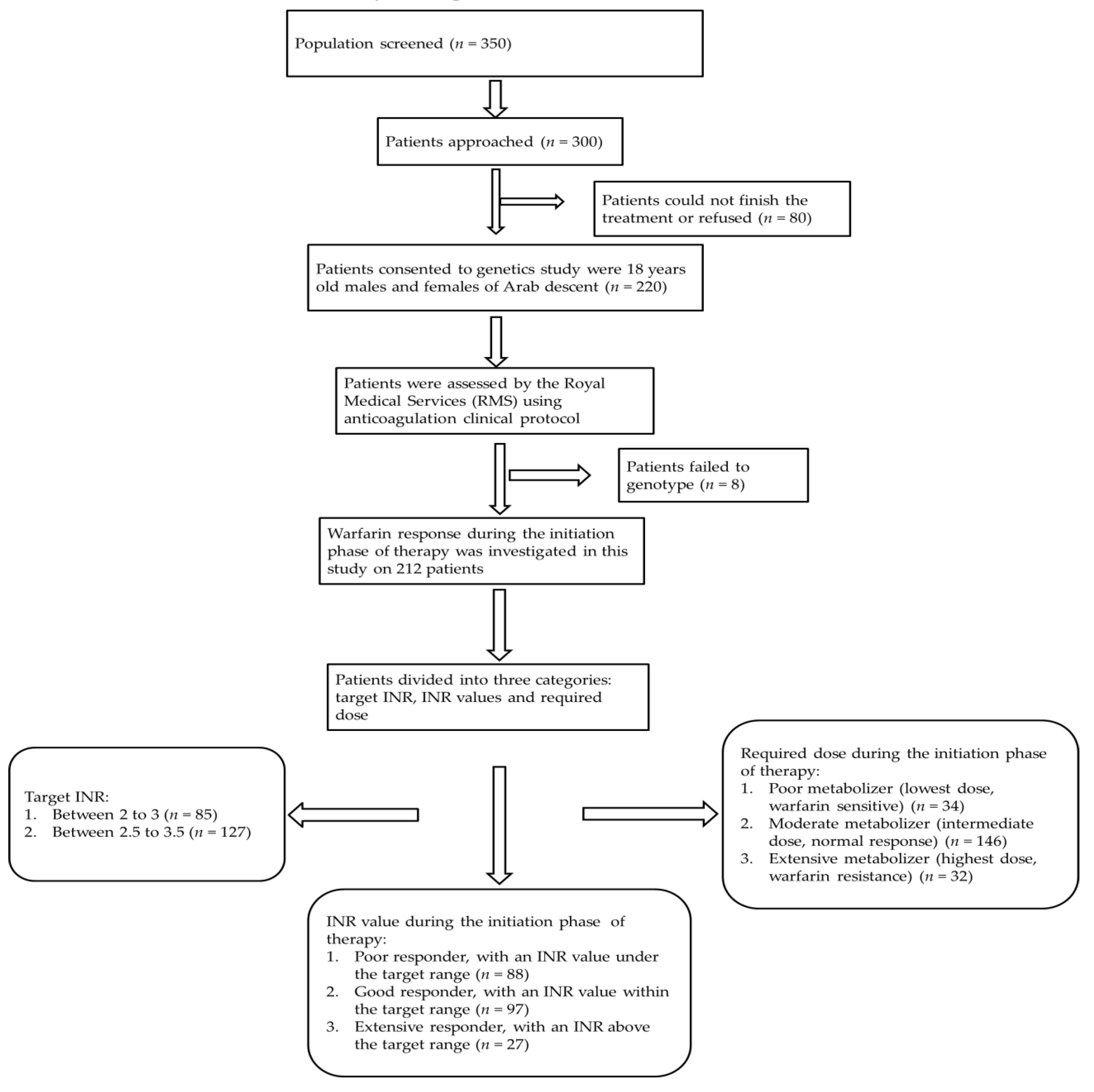
2.1. Patient Population and Study Design
2.2. Outcome Measurement
2.3. SNP Selection, DNA Extraction, and Genotyping
2.4. Statistical Analysis
3. Results
3.1. Study Group
3.2. Effect of CYP2C9 and VKORC1 Polymorphisms on Warfarin Sensitivity during Initiation Phase of Therapy
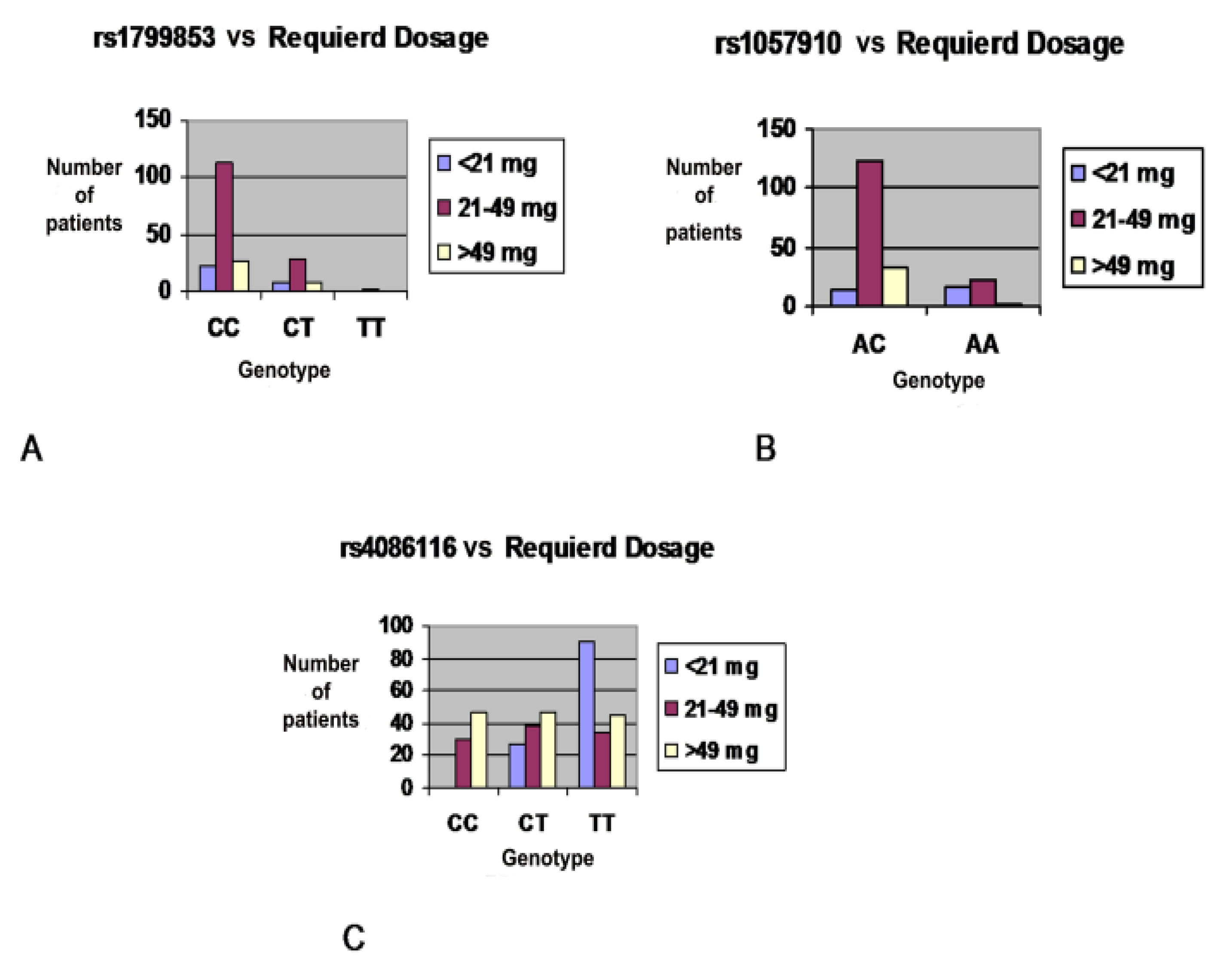
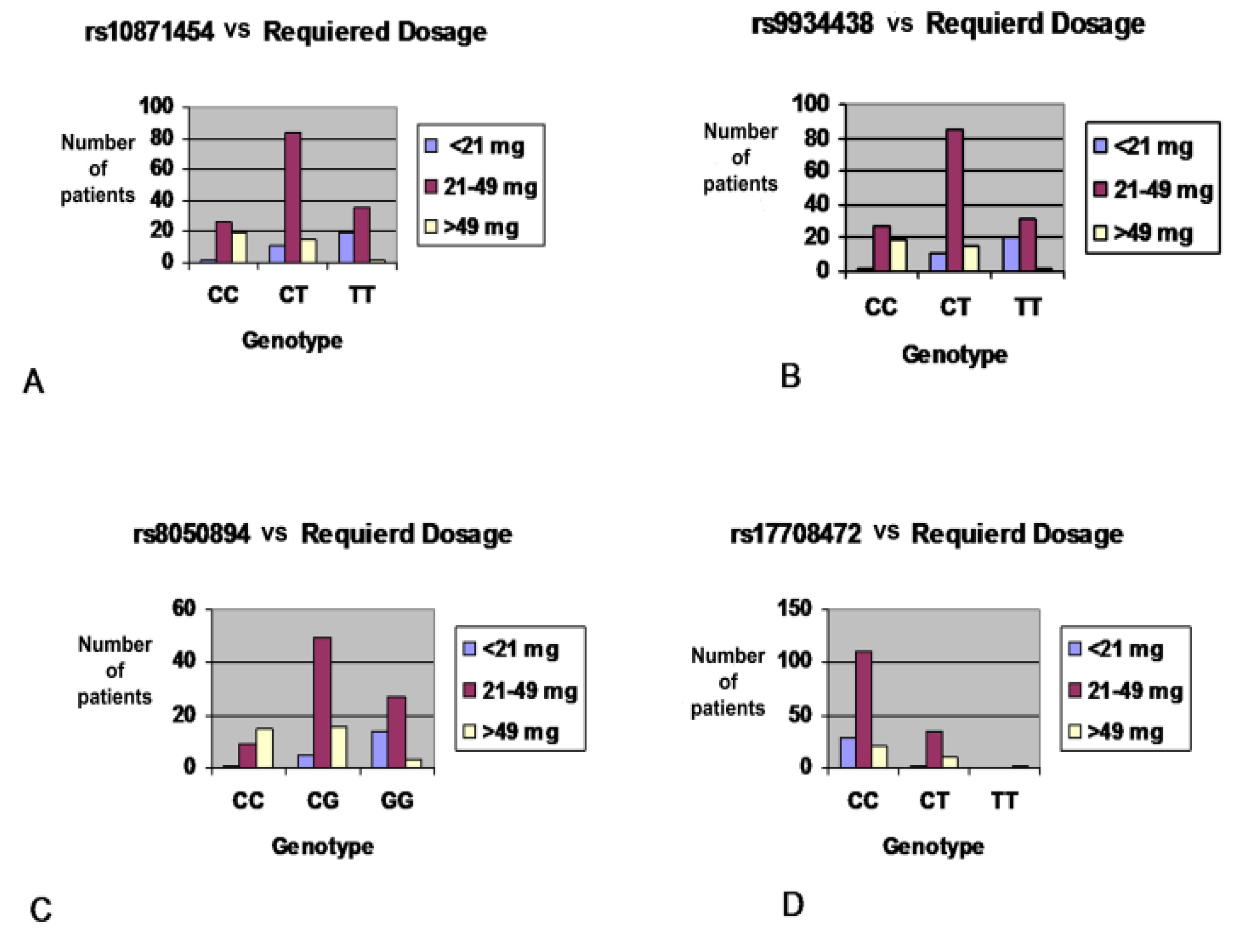
3.3. Effect of CYP2C9 and VKORC1 Polymorphisms on Warfarin Required Dose during Initiation Phase of Therapy
3.4. Effect of CYP2C9 and VKORC1 Polymorphisms on Warfarin Responsiveness during Initiation of Therapy
3.5. Effect of CYP2C9 and VKORC1 Polymorphisms on INR Treatment Outcome
3.6. Correlation Between Warfarin Dose and Clinical Data
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kim, Y.; Smith, A.; Wu, A. C3435T polymorphism of MDR1 gene with warfarin resistance. Clin. Chim. Acta 2013, 425, 34–36. [Google Scholar] [CrossRef] [PubMed]
- Motulsky, A.G.; Qi, M. Pharmacogenetics, pharmacogenomics and ecogenetics. J. Zhejiang Univ. Sci. B. 2006, 7, 169–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eriksson, N.; Wadelius, M. Prediction of warfarin dose: Why, when and how? Pharmacogenomics 2012, 13, 429–440. [Google Scholar] [CrossRef] [PubMed]
- Sconce, E.A.; Khan, T.I.; Wynne, H.A.; Avery, P.; Monkhouse, L.; King, B.P.; Wood, P.; Kesteven, P.; Daly, A.K.; Kamali, F. The impact of CYP2C9 and VKORC1 genetic polymorphism and patient characteristics upon warfarin dose requirements: Proposal for a new dosing regimen. Blood 2005, 106, 2329–2333. [Google Scholar] [CrossRef] [PubMed]
- Wadelius, M.; Chen, L.Y.; Downes, K.; Ghori, J.; Hunt, S.; Eriksson, N.; Wallerman, O.; Melhus, H.; Wadelius, C.; Bentley, D. Common VKORC1 and GGCX polymorphisms associated with warfarin dose. Pharmacogen. J. 2005, 5, 262–270. [Google Scholar] [CrossRef] [PubMed]
- Eichelbaum, M.; Ingelman-Sundberg, M.; Evans, W. Pharmacogenomics and individualized drug therapy. Annu. Rev. Med. 2006, 57, 119–137. [Google Scholar] [CrossRef] [PubMed]
- D’Andrea, G.; D’Ambrosio, R.L.; Di Perna, P.; Chetta, M.; Santacroce, R.; Brancaccio, V.; Grandone, E.; Margaglione, M. A polymorphism in the VKORC1 gene is associated with an interindividual variability in the dose-anticoagulant effect of warfarin. Blood 2005, 105, 645–649. [Google Scholar] [CrossRef] [PubMed]
- Muszkat, M.; Blotnik, S.; Elami, A.; Krasilnikov, I.; Caraco, Y. Warfarin metabolism and anticoagulant effect: A prospective, observational study of the impact of CYP2C9 genetic polymorphism in the presence of drug-disease and drug-drug interactions. Clin. Ther. 2007, 29, 427–437. [Google Scholar] [CrossRef]
- Rendic, S. Summary of information on human CYP enzymes: Human P450 metabolism data. Drug Metab. Rev. 2002, 34, 83–448. [Google Scholar] [CrossRef] [PubMed]
- Dean, L. Warfarin Therapy and VKORC1 and CYP Genotype; National Center for Biotechnology Information: Bethesda, MD, USA, 2012. [Google Scholar]
- Zhou, S.; Zhou, Z.; Yang, L.; Cai, J. Substrates, inducers, inhibitors and structure-activity relationships of human cytochrome P450 2C9 and implications in drug development. Curr. Med. Chem. 2009, 16, 3480–3675. [Google Scholar] [CrossRef] [PubMed]
- Kirchheiner, J.; Brockmoller, J. Clinical consequences of cytochrome P450 2C9 polymorphisms. Clin. Pharmacol. Ther. 2005, 77, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Ingelman-Sundberg, M.; Lauschke, V.M. Worldwide distribution of cytochrome P450 alleles: A meta-analysis of population-scale sequencing projects. Clin. Pharmacol. Ther. 2017, 102, 688–700. [Google Scholar] [CrossRef] [PubMed]
- Linder, M.W.; Homme, M.B.; Reynolds, K.K.; Gage, B.F.; Eby, C.; Silvestrov, N.; Valdes, R. Interactive modeling for ongoing utility of pharmacogenetic diagnostic testing: Application for warfarin therapy. Clin. Chem. 2009, 55, 1861–1868. [Google Scholar] [CrossRef] [PubMed]
- Tie, J.K.; Stafford, D.W. Structural and functional insights into enzymes of the vitamin K cycle. J. Thromb. Haemost. 2016, 14, 236–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loebstein, R.; Dvoskin, I.; Halkin, H.; Vecsler, M.; Lubetsky, A.; Rechavi, G.; Amariglio, N.; Cohen, Y.; Ken-Dror, G.; Almog, S.; et al. A coding VKORC1 Asp36Tyr polymorphism predisposes to warfarin resistance. Blood 2007, 109, 2477–2480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schalekamp, T.; De Boer, A. Pharmacogenetics of oral anticoagulant therapy. Curr. Pharm. Des. 2010, 16, 187–203. [Google Scholar] [CrossRef] [PubMed]
- Wadelius, M.; Chen, L.Y.; Lindh, J.D.; Eriksson, N.; Ghori, M.J.; Bumpstead, S.; Holm, L.; McGinnis, R.; Rane, A.; Deloukas, P. The largest prospective warfarin-treated cohort supports genetic forecasting. Blood 2009, 113, 784–792. [Google Scholar] [CrossRef] [PubMed]
- Lenzini, P.; Wadelius, M.; Kimmel, S.; Anderson, J.L.; Jorgensen, A.L.; Pirmohamed, M.; Caldwell, M.D.; Limdi, N.; Burmester, J.K.; Dowd, M.B.; et al. Integration of genetic, clinical, and INR data to refine warfarin dosing. Clin. Pharmacol. Ther. 2010, 87, 572–578. [Google Scholar] [CrossRef] [PubMed]
- Gage, B.; Lesko, L. Pharmacogenetics of warfarin: Regulatory, scientific, and clinical issues. J. Thromb. Thrombolysis 2007, 25, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Kuruvilla, M.; Gurk-Turner, C. A review of warfarin dosing and monitoring. Proc. Bayl. Univ. Med. Cent. 2001, 14, 305–306. [Google Scholar] [CrossRef] [PubMed]
- Hylek, E.; D’Antonio, J.; Evans-Molina, C.; Shea, C.; Henault, L.; Regan, S. Translating the results of randomized trials into clinical practice: The challenge of warfarin candidacy among hospitalized elderly patients with atrial fibrillation. Stroke 2006, 37, 1075–1080. [Google Scholar] [CrossRef] [PubMed]
- Wiedermann, C.J.; Stockner, I. Warfarin-induced bleeding complications—Clinical presentation and therapeutic options. Thromb. Res. 2008, 122, S13–S18. [Google Scholar] [CrossRef]
- Borgiani, P.; Ciccacci, C.; Forte, V.; Romano, S.; Federici, G.; Novelli, G. Allelic variants in the CYP2C9 and VKORC1 loci and interindividual variability in the anticoagulant dose effect of warfarin in Italians. Pharmacogenomics 2007, 8, 1545–1550. [Google Scholar] [CrossRef] [PubMed]
- Hamberg, A.; Dahl, M.L.; Barban, M.; Scordo, M.G.; Wadelius, M.; Pengo, V.; Padrini, R.; Jonsson, E.N. A PK-PD model for predicting the impact of age, CYP2C9, and VKORC1 genotype on individualization of warfarin therapy. Clin. Pharmacol. Ther. 2007, 81, 529–538. [Google Scholar] [CrossRef] [PubMed]
- Teichert, M.; Van Schaik, R.H.N.; Hofman, A.; Uitterlinden, A.G.; de Smet, P.A.G.M.; Stricker, B.; Visser, L.E. Genotypes associated with reduced activity of VKORC1 and CYP2C9 and their modification of acenocoumarol anticoagulation during the initial treatment period. Clin. Pharmacol. Ther. 2009, 85, 379–386. [Google Scholar] [CrossRef] [PubMed]
- 1000 Genomes Project Consortium. An integrated map of genetic variation from 1092 human genomes. Nature 2012, 491, 56–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahashi, H.; Echizen, H. Pharmacogenetics of warfarin elimination and its clinical implications. Clin. Pharmacokinet. 2001, 40, 587–603. [Google Scholar] [CrossRef] [PubMed]
- Kealey, C.; Chen, Z.; Christie, J.; Thorn, C.F.; Whitehead, A.S.; Price, M.; Samaha, F.F.; Kimmel, S.E. Warfarin and cytochrome P450 2C9 genotype: Possible ethnic variation in warfarin sensitivity. Pharmacogenomics 2008, 8, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Limdi, N.; McGwin, G.; Goldstein, J.; Beasley, T.; Arnett, D.; Adler, B.; Baird, M.; Acton, R. Influence of CYP2C9 and VKORC1 1173C/T genotype on the risk of hemorrhagic complications in African-American and European-American patients on warfarin. Clin. Pharmacol. Ther. 2007, 83, 312–321. [Google Scholar] [CrossRef] [PubMed]
- Ohno, M.; Yamamoto, A.; Ono, A.; Miura, G.; Funamoto, M.; Takemoto, Y.; Otsu, K.; Kouno, Y.; Tanabe, T.; Masunaga, Y.; et al. Influence of clinical and genetic factors on warfarin dose requirements among Japanese patients. Eur. J. Clin. Pharmacol. 2009, 65, 1097–1103. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.W.; Chen, H.S.; Wang, X.Q.; Huang, L.; Xu, D.L.; Hu, X.J.; Huang, Z.H.; He, Y.; Chen, K.M.; Xiang, D.K.; et al. Validation of VKORC1 and CYP2C9 genotypes on interindividual warfarin maintenance dose: A prospective study in Chinese patients. Pharmacogenet. Genomics 2009, 19, 226–234. [Google Scholar] [CrossRef] [PubMed]
- Gan, G.; Phipps, M.; Ku, C.; Teh, A.; Sangkar, V. Genetic polymorphism of the CYP2C9 subfamily of 3 different races in warfarin maintenance dose. Int. J. Hematol. 2004, 80, 295–296. [Google Scholar] [CrossRef] [PubMed]
- Tanira, M.; Al-Mukhaini, M.; Al-Hinai, A.; Al Balushi, K.; Ahmed, I. Frequency of CYP2C9 genotypes among Omani patients receiving warfarin and its correlation with warfarin dose. Community Genet. 2007, 10, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Schelleman, H.; Chen, Z.; Kealey, C.; Whitehead, A.S.; Christie, J.; Price, M.; Brensinger, C.M.; Newcomb, C.W.; Thorn, C.F.; Samaha, F.F.; et al. Warfarin response and vitamin K epoxide reductase complex 1 in African Americans and Caucasians. Clin. Pharmacol. Ther. 2007, 81, 742–747. [Google Scholar] [CrossRef] [PubMed]
- Limdi, N.A.; Arnett, D.K.; Goldstein, J.A.; Beasley, T.M.; McGwin, G.; Adler, B.K.; Acton, R.T. Influence of CYP2C9 and VKORC1 on warfarin dose, anticoagulation attainment and maintenance among European Americans and African Americans. Pharmacogenomics 2008, 9, 511–526. [Google Scholar] [CrossRef] [PubMed]
- Shrif, N.; Won, H.H.; Lee, S.T.; Park, J.H.; Kim, K.K.; Kim, M.J.; Kim, S.; Lee, S.Y.; Ki, C.S.; Osman, I.M.; et al. Evaluation of the effects of VKORC1 polymorphisms and haplotypes, CYP2C9 genotypes, and clinical factors on warfarin response in Sudanese patients. Eur. J. Clin. Pharmacol. 2011, 67, 1119–1130. [Google Scholar] [CrossRef] [PubMed]
- Haug, K.B.; Sharikabad, M.N.; Kringen, M.K.; Narum, S.; Sjaatil, S.T.; Johansen, P.W.; Kierulf, P.; Seljeflot, I.; Arnesen, H.; Brørs, O. Warfarin dose and INR related to genotypes of CYP2C9 and VKORC1 in patients with myocardial infarction. Thromb. J. 2008, 6, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kringen, M.K.; Haug, K.B.F.; Grimholt, R.M.; Stormo, C.; Narum, S.; Opdal, M.S.; Fosen, J.T.; Piehler, A.P.; Johansen, P.W.; Seljeflot, I.; et al. Genetic variation of VKORC1 and CYP4F2 genes related to warfarin maintenance dose in patients with myocardial infarction. J. Biomed. Biotechnol. 2011, 2011, 739–751. [Google Scholar] [CrossRef] [PubMed]
- Taube, J.; Halsall, D.; Baglin, T. Influence of cytochrome P-450 CYP2C9 polymorphisms on warfarin sensitivity and risk of over-anticoagulation in patients on long-term treatment. Blood 2000, 96, 1816–1819. [Google Scholar] [PubMed]
- Frymoyer, A. Effect of single-dose rifampin on the pharmacokinetics of warfarin in healthy volunteers. Clin. Pharmacol. Ther. 2010, 88, 540–547. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Category | Subcategory | Extensive Metabolizer | Good Metabolizers | Poor Metabolizers |
|---|---|---|---|---|
| Demographics | Patients (N, %) | (32/212) 15.1% | (146/212) 68.9% | (34/212) 16% |
| Age a (years) | 56.0 (17.68) | 55.0 (14.64) | 48.29 (15.09) | |
| BMI a | 27.87 (3.72) | 27.7 (4.85) | 27.42 (3.45) | |
| Smoking (N, %) | 31.25% | 18.6% | 41.2% | |
| Male | 59.4% | 51.4% | 67.6% | |
| Female | 40.6% | 48.6% | 32.4% | |
| Concomitant Disease | Co morbidity | 56.3% | 68.5% | 55.9% |
| Hypertension | 34.4% | 42.5% | 23.5% | |
| Diabetes mellitus | 18.8% | 21.9% | 26.5% | |
| CHD b | 28.1% | 25.3% | 29.4% | |
| Thyroid | 0% | 3.4% | 2.9% | |
| Lipid | 3.1% | 6.8% | 2.9% | |
| Medication | Aspirin | 62.5% | 65.8% | 76.5% |
| Indication of Treatment | MVR c | 18.8% | 10.3% | 20.6% |
| AVR d | 6.3% | 24.0% | 20.6% | |
| AF e | 34.4% | 19.2% | 20.6% | |
| DVR f | 9.4% | 15.8% | 11.8% | |
| Others | 9.4% | 7.5% | 0.0% | |
| Target INR | 2–3 | 43.8% | 39.7% | 38.2% |
| 2.5–3.5 | 56.3% | 60.3% | 61.8% | |
| Mean weakly dose a | 16.699 (2.79) | 35.896 (7.39) | 67.44 (42.48) | |
| Mean INR a | 2.82 (0.72) | 2.38 (0.75) | 2.44 (0.83) |
| Gene | SNP ID | Genotype | Sensitive | Moderate | Resistance | p-Value * |
|---|---|---|---|---|---|---|
| VKORC1 | rs10871454 | CC | 4.3% | 57.4% | 38.3% | <0.001 |
| CT | 10.0% | 76.4% | 13.6% | |||
| TT | 34.5% | 63.6% | 1.8% | |||
| rs8050894 | CC | 2.3% | 60.5% | 37.2% | <0.001 | |
| CG | 10.9% | 74.5% | 14.5% | |||
| GG | 32.2% | 64.4% | 3.4% | |||
| rs9934438 | CC | 4.2% | 58.3% | 37.5% | <0.001 | |
| CT | 9.9% | 76.6% | 13.5% | |||
| TT | 35.8% | 62.3% | 1.9% | |||
| rs17708472 | CC | 18.1% | 68.8% | 13.1% | <0.001 | |
| CT | 6.1% | 73.5% | 20.4% | |||
| TT | 0.0% | 0.0% | 100% | |||
| CYP2C9 | rs1799853 | CC | 14% | 70.1% | 15.9% | 0.744 |
| CT | 19.6% | 63% | 17.4% | |||
| TT | 0.0% | 100% | 0.0% | |||
| rs4086116 | CC | 8.1% | 73.2% | 18.7% | 0.012 | |
| CT | 24.1% | 62.0% | 13.9% | |||
| TT | 30.0% | 70.0% | 0.0% | |||
| rs1057910 | AA | 8.8% | 72.5% | 18.7% | <0.001 | |
| AC | 41.5% | 53.7% | 4.9% |
| Gene | Haplotypes | Frequency * (%) | Odds Ratio (95% CI) | p-Value ** |
|---|---|---|---|---|
| VKORC1 | TGAG | 0.512 | 0.00 | ------ |
| CCGG | 0.324 | 0.32 (0.2–0.43) | <0.0001 | |
| CCGA | 0.129 | 0.38 (0.23–0.54) | <0.0001 | |
| CGGG | 0.028 | 0.34 (0.03–0.66) | 0.034 | |
| TCGG | 0.007 | 0.21 (−0.38–0.8) | 0.48 | |
| CYP2C9 | CAC | 0.767 | 0.00 | ----- |
| TAT | 0.116 | −0.05 (−0.21–0.11) | 0.53 | |
| TCC | 0.094 | −0.45 (−0.64–−0.27) | <0.0001 | |
| TAC | 0.021 | 0.01 (−0.34–0.37) | 0.95 | |
| TCT | 0.002 | −1.11 (−2.14–−0.08) | 0.037 |
| SNP ID | Initiation Dose | p-Value * | Initiation INR | p-Value * |
|---|---|---|---|---|
| rs10871454 | 38.1 (23.02) | <0.001 | 2.46 (0.77) | 0.006 |
| rs8050894 | <0.001 | 0.008 | ||
| rs9934438 | <0.001 | 0.009 | ||
| rs17708472 | <0.001 | 0.511 | ||
| rs1799853 | 0.118 | 0.184 | ||
| rs4086116 | 0.001 | 0.08 | ||
| rs1057910 | 0.001 | 0.572 |
| Gene | SNP ID | Genotype | Poor Responder | Good Responder | Extensive Responder | p-Value * |
|---|---|---|---|---|---|---|
| VKORC1 | rs10871454 | CC | 55.3% | 36.2% | 8.5% | 0.171 |
| CT | 40.9% | 45.5% | 13.6% | |||
| TT | 30.9% | 54.5% | 14.5% | |||
| rs8050894 | CC | 53.5% | 39.5% | 7% | 0.235 | |
| CG | 41.8% | 43.6% | 14.5% | |||
| GG | 32.2% | 54.2% | 13.6% | |||
| rs9934438 | CC | 54.2% | 37.5% | 8.3% | 0.226 | |
| CT | 40.5% | 45% | 14.4% | |||
| TT | 32.1% | 54.7% | 13.2% | |||
| rs17708472 | CC | 38.1% | 50.6% | 11.3% | 0.042 | |
| CT | 55.1% | 28.6% | 16.3% | |||
| TT | 0.0% | 66.7% | 33.3% | |||
| CYP2C9 | rs1799853 | CC | 45.1% | 44.5% | 10.4% | 0.076 |
| CT | 28.3% | 52.5% | 19.6% | |||
| TT | 50.0% | 0.0% | 50.0% | |||
| rs4086116 | CC | 45.5% | 43.9% | 10.6% | 0.005 | |
| CT | 39.2% | 49.4% | 11.4% | |||
| TT | 10.0% | 40.0% | 50.0% | |||
| rs1057910 | AA | 42.1% | 45.0% | 12.9% | 0.910 | |
| AC | 39% | 48.8% | 12.2% |
| Gene | Haplotypes | Frequency * (%) | Odds Ratio (95% CI) | p-Value ** |
|---|---|---|---|---|
| VKORC1 | TGAG | 0.512 | 0.00 | ------ |
| CCGG | 0.326 | −0.18 (−0.33–−0.03) | 0.02 | |
| CCGA | 0.129 | −0.08 (−0.28–0.12) | 0.46 | |
| CGGG | 0.026 | −0.05 (−0.47–0.36) | 0.8 | |
| TCGG | 0.007 | 0.55 (−0.22–1.32) | 0.16 | |
| CYP2C9 | CAC | 0.767 | 0.00 | ------ |
| TAT | 0.115 | 0.25 (0.04–0.45) | 0.018 | |
| TCC | 0.094 | 0.06 (−0.17–0.3) | 0.59 | |
| TAC | 0.021 | 0.44 (−0.01–0.89) | 0.059 | |
| TCT | 0.003 | 0.4 (−0.9–1.71) | 0.55 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
AL-Eitan, L.N.; Almasri, A.Y.; Khasawneh, R.H. Impact of CYP2C9 and VKORC1 Polymorphisms on Warfarin Sensitivity and Responsiveness in Jordanian Cardiovascular Patients during the Initiation Therapy. Genes 2018, 9, 578. https://0-doi-org.brum.beds.ac.uk/10.3390/genes9120578
AL-Eitan LN, Almasri AY, Khasawneh RH. Impact of CYP2C9 and VKORC1 Polymorphisms on Warfarin Sensitivity and Responsiveness in Jordanian Cardiovascular Patients during the Initiation Therapy. Genes. 2018; 9(12):578. https://0-doi-org.brum.beds.ac.uk/10.3390/genes9120578
Chicago/Turabian StyleAL-Eitan, Laith N., Ayah Y. Almasri, and Rame H. Khasawneh. 2018. "Impact of CYP2C9 and VKORC1 Polymorphisms on Warfarin Sensitivity and Responsiveness in Jordanian Cardiovascular Patients during the Initiation Therapy" Genes 9, no. 12: 578. https://0-doi-org.brum.beds.ac.uk/10.3390/genes9120578