
Clinical Features, Inpatient Trajectories and Frailty in Older Inpatients with COVID-19: A Retrospective Observational Study

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Sample
2.3. Patient Characteristics
2.4. Patient Outcomes
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
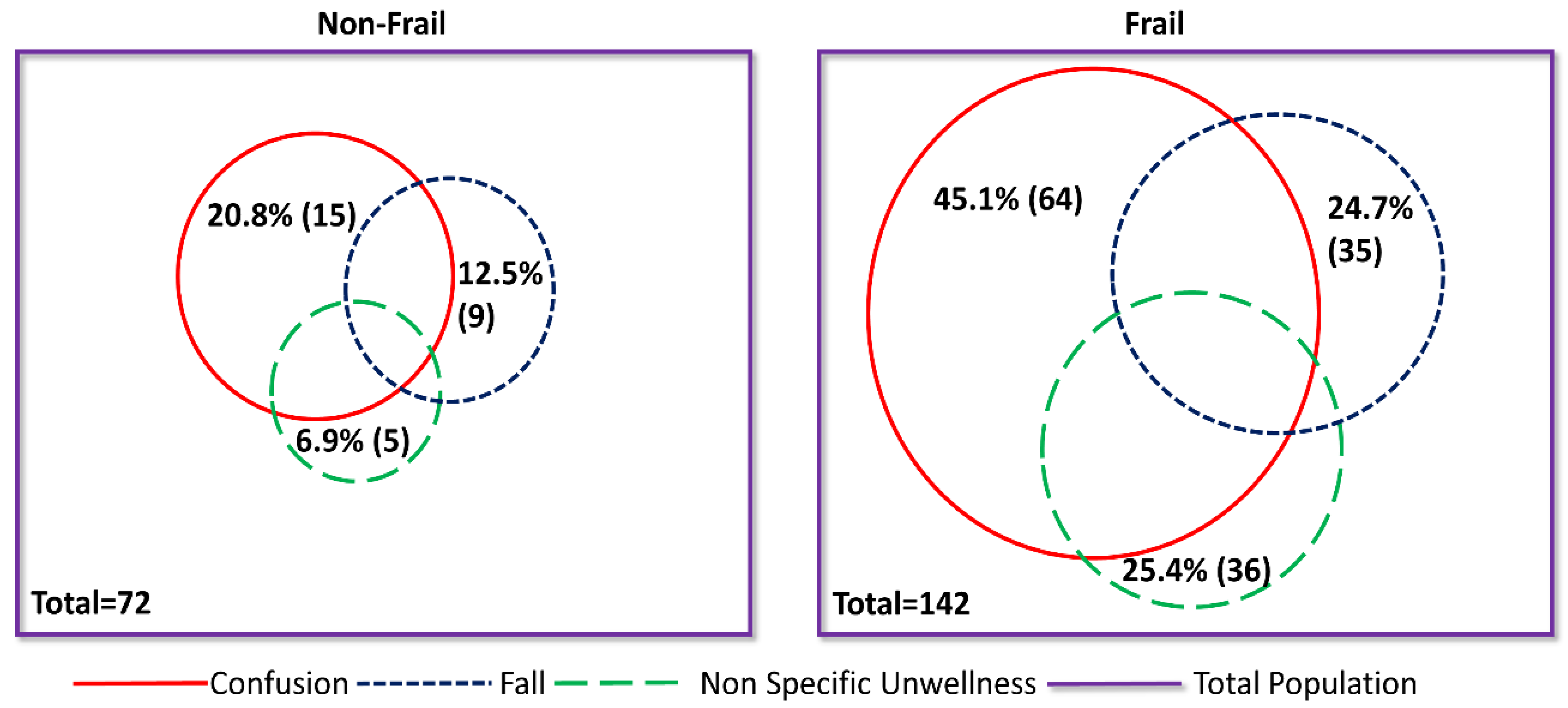
3.2. Relationship between Clinical Characteristics and Frailty
3.3. Relationship between Inpatient Trajectory and Frailty
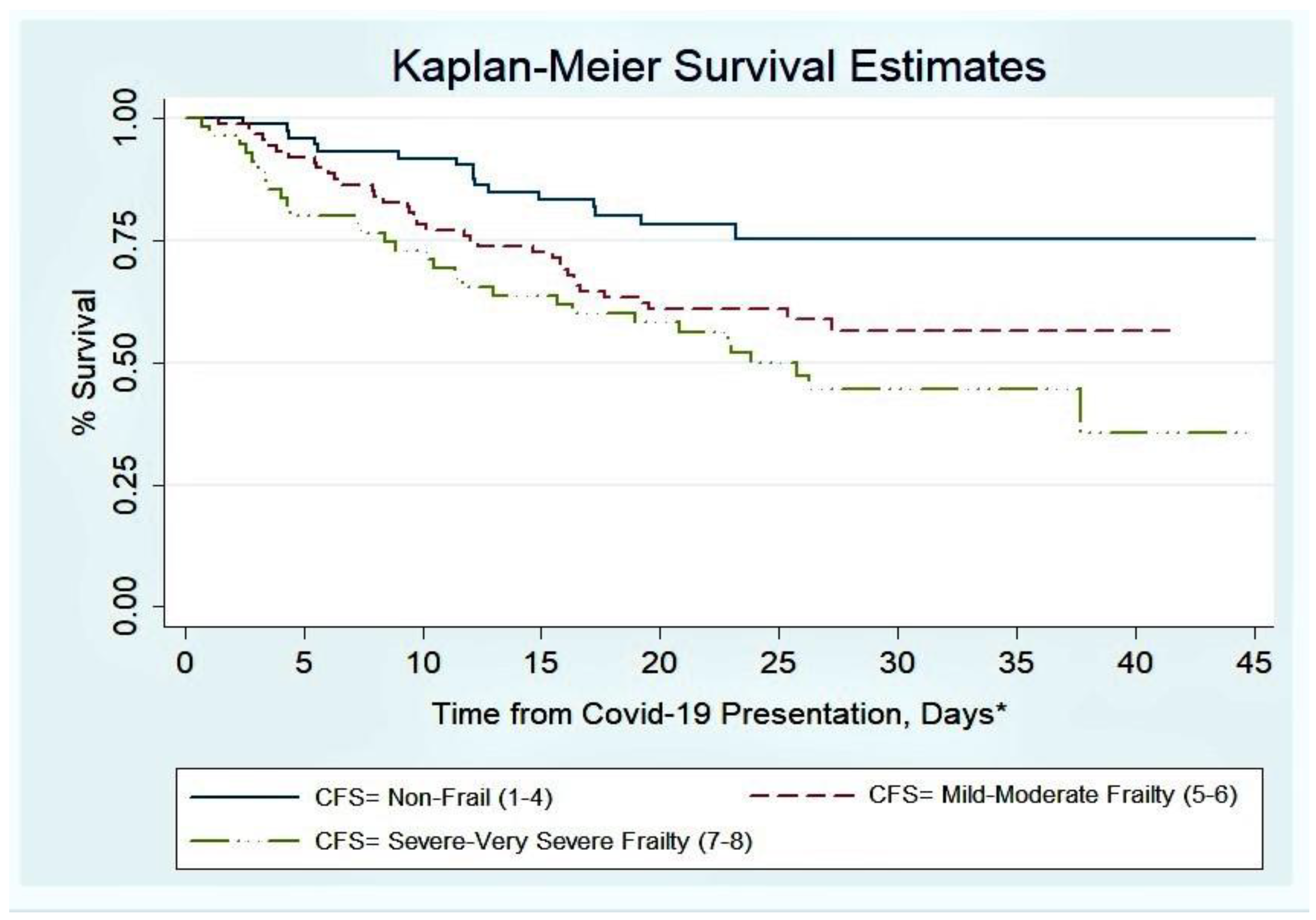
3.4. Relationship between Mortality and Frailty
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Coronavirus Disease (COVID-19)—Events as They Happen. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-as-they-happen (accessed on 10 April 2020).
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Lithander, F.E.; Neumann, S.; Tenison, E.; Lloyd, K.; Welsh, T.J.; Rodrigues, J.C.L.; Higgins, J.P.T.; Scourfield, L.; Christensen, H.; Haunton, V.J.; et al. COVID-19 in Older People: A Rapid Clinical Review. Age Ageing 2020, afaa093. [Google Scholar] [CrossRef]
- Mackett, A.; Keevil, V. COVID-19 and Gastrointestinal Symptoms—A Case Report. Geriatrics 2020, 5, 31. [Google Scholar] [CrossRef] [PubMed]
- Oxley, T.J.; Mocco, J.; Majidi, S.; Kellner, C.P.; Shoirah, H.; Singh, I.P.; De Leacy, R.A.; Shigematsu, T.; Ladner, T.R.; Yaeger, K.A.; et al. Large-Vessel Stroke as a Presenting Feature of Covid-19 in the Young. N. Engl. J. Med. 2020, 382, e60. [Google Scholar] [CrossRef] [PubMed]
- Beyrouti, R.; Adams, M.; Benjamin, L.; Cohen, H.; Farmer, S.F.; Goh, Y.Y.; Humphries, F.; Jäger, H.R.; Losseff, N.A.; Perry, R.J.; et al. Characteristics of ischaemic stroke associated with COVID-19. J. Neurol. Neurosurg. Psychiatry 2020, 2020, jnnp-2020-323586. [Google Scholar] [CrossRef]
- Fried, J.A.; Ramasubbu, K.; Bhatt, R.; Topkara, V.K.; Clerkin, K.J.; Horn, E.; Rabbani, L.; Brodie, D.; Jain, S.S.; Kirtane, A.J.; et al. The Variety of Cardiovascular Presentations of COVID-19. Circulation 2020, 141, 1930–1936. [Google Scholar] [CrossRef] [Green Version]
- Hendren, N.S.; Drazner, M.H.; Bozkurt, B.; Cooper, L.T., Jr. Description and Proposed Management of the Acute COVID-19 Cardiovascular Syndrome. Circulation 2020, 141, 1903–1914. [Google Scholar] [CrossRef]
- Menni, C.; Valdes, A.; Freydin, M.B.; Sudre, C.H.; Nguyen, L.H.; Drew, D.A.; Ganesh, S.; Varsavsky, T.; Cardoso, M.J.; El-Sayed Moustafa, J.S.; et al. Real-time tracking of self-reported symptoms to predict potential COVID-19. Nat. Med. 2020, 26, 1037–1040. [Google Scholar] [CrossRef]
- Xydakis, M.S.; Dehgani-Mobaraki, P.; Holbrook, E.H.; Xydakis, M.S.; Dehgani-Mobaraki, P.; Holbrook, E.H.; Geisthoff, U.W.; Bauer, C.; Hautefort, C.; Herman, P.; et al. Smell and taste dysfunction in patients with COVID-19. Lancet Infect Dis. 2020. [Google Scholar] [CrossRef]
- Tay, H.; Harwood, R. Atypical presentation of COVID-19 in a frail older person. Age Ageing 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zazzara, M.B.; Penfold, R.S.; Roberts, A.L.; Lee, K.A.; Dooley, H.; Sudre, C.H.; Welch, C.; Bowyer, R.C.E.; Visconti, A.; Mangino, M.; et al. Probable delirium is a presenting symptom of COVID-19 in frail, older adults: A cohort study of 322 hospitalised and 535 community-based older adults. Age Ageing 2020, afaa223. [Google Scholar] [CrossRef] [PubMed]
- Isaia, G.; Marinello, R.; Tibaldi, V.; Tamone, C.; Bo, M. Atypical Presentation of Covid-19 in an Older Adult with Severe Alzheimer Disease. Am. J. Geriatr. Psychiatry 2020, 28, 790–791. [Google Scholar] [CrossRef]
- Singhania, N.; Bansal, S.; Singhania, G. An Atypical Presentation of Novel Coronavirus Disease 2019 (COVID-19). Am. J. Med. 2020, 133, e365–e366. [Google Scholar] [CrossRef]
- Norman, R.E.; Stall, N.M.; Sinha, S.K. Typically Atypical: COVID-19 Presenting as a Fall in an Older Adult. J. Am. Geriatr. Soc. 2020, 68, E36–E37. [Google Scholar] [CrossRef]
- Andrew, M.K.; McElhaney, J.E.; McGeer, A.A.; Hatchette, T.F.; Leblanc, J.; Webster, D.; Bowie, W.; Poirier, A.; Nichols, M.K.; McNeil, S.A.; et al. Influenza surveillance case definitions miss a substantial proportion of older adults hospitalized with laboratory-confirmed influenza: A report from the Canadian Immunization Research Network (CIRN) Serious Outcomes Surveillance (SOS) Network. Infect Control Hosp. Epidemiol. 2020, 41, 499–504. [Google Scholar] [CrossRef]
- Falsey, A.; Baran, A.; Walsh, E. Should clinical case definitions of influenza in hospitalized older adults include fever? Influenza Other Respir. Viruses 2015, 9, 23–29. [Google Scholar] [CrossRef]
- Jarrett, P.G.; Rockwood, K.; Carver, D.; Stolee, P.; Cosway, S. Illness presentation in elderly patients. Arch. Intern. Med. 1995, 155, 1060–1064. [Google Scholar] [CrossRef]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [Green Version]
- Brill, S.; Jarvis, H.; Ozcan, E.; Burns, T.L.P.; Warraich, R.A.; Amani, L.J.; Jaffer, A.; Paget, S.; Sivaramakrishnan, A.; Creer, D.D. COVID-19: A retrospective cohort study with focus on the over-80s and hospital-onset disease. BMC Med. 2020, 18, 194. [Google Scholar] [CrossRef] [PubMed]
- Docherty, A.B.; Harrison, E.M.; Green, C.A.; Hardwick, H.E.; Pius, R.; Norman, L.; Holden, K.A.; Read, J.M.; Dondelinger, F.; Carson, G.; et al. Features of 20 133 UK patients in hospital with covid-19 using the ISARIC WHO Clinical Characterisation Protocol: Prospective observational cohort study. BMJ 2020, m1985. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef] [PubMed]
- Rockwood, K.; Song, X.; MacKnight, C.; Bergman, H.; Hogan, D.B.; McDowell, I.; Mitnitski, A. A global clinical measure of fitness and frailty in elderly people. CMAJ 2005, 173, 489–495. [Google Scholar] [CrossRef] [Green Version]
- Montero-Odasso, M.; Hogan, D.B.; Lam, R.; Madden, K.; MacKnight, C.; Molnar, F.; Rockwood, K. Age Alone is not Adequate to Determine Health-care Resource Allocation During the COVID-19 Pandemic. Can. Geriatr. J. 2020, 23, 152–154. [Google Scholar] [CrossRef]
- De Smet, R.; Mellaerts, B.; Vandewinckele, H.; Lybeert, P.; Frans, E.; Ombelet, S.; Lemahieu, W.; Symons, R.; Ho, E.; Frans, J.; et al. Frailty and mortality in hospitalized older adults with COVID-19: Retrospective observational study. J. Am. Med. Dir. Assoc. 2020, 21, 928–932.e1. [Google Scholar] [CrossRef] [PubMed]
- Miles, A.; Webb, T.E.; Mcloughlin, B.C.; Mannan, I.; Rather, A.; Knopp, P.; Davis, D. Outcomes from COVID-19 across the range of frailty: Excess mortality in fitter older people. Eur. Geriatr. Med. 2020, 1–5. [Google Scholar] [CrossRef]
- NEWS2 and Deterioration in COVID-19. Royal College of Physicians London. 2020. Available online: https://www.rcplondon.ac.uk/news/news2-and-deterioration-covid-19 (accessed on 20 July 2020).
- COVID-19 BSTI Reporting templates. The British Society of Thoracic Imaging. 2020. Available online: https://www.bsti.org.uk/covid-19-resources/covid-19-bsti-reporting-templates/ (accessed on 20 July 2020).
- Marincowitz, C.; Turner, V.; Allgar, V.; Bellwood, J.; Wheeler, A.; Hale, M.; Callaghan, H.; Clegg, A.; Sheldon, T.A. Can Patient Frailty Be Estimated from Inpatient Records? A Prospective Cohort Study. Adv. Geriatr. Med. Res. 2020, 2, e200004. [Google Scholar] [CrossRef]
- D’Adamo, H.; Yoshikawa, T.; Ouslander, J.G. Coronavirus Disease 2019 in Geriatrics and Long-Term Care: The ABCDs of COVID-19. J. Am. Geriatr. Soc. 2020, 68, 912–917. [Google Scholar] [CrossRef]
- O’Hanlon, S.; Inouye, S.K. Delirium: A missing piece in the COVID-19 pandemic puzzle. Age Ageing 2020, 49, 497–498. [Google Scholar] [CrossRef]
- Ellis, G.; Gardner, M.; Tsiachristas, A.; Langhorne, P.; Burke, O.; Harwood, R.H.; Conroy, S.P.; Kircher, T.; Somme, D.; Saltvedt, I.; et al. Comprehensive geriatric assessment for older adults admitted to hospital. Cochrane Database Syst. Rev. 2017, 9, CD006211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hewitt, J.; Carter, B.; Vilches-Moraga, A.; Quinn, T.J.; Braude, P.; Verduri, A.; Pearce, L.; Stechman, M.; Short, R.; Price, A.; et al. The effect of frailty on survival in patients with COVID-19 (COPE): A multicentre, European, observational cohort study. Lancet Public Health 2020. [Google Scholar] [CrossRef]
- Wong, H.Y.F.; Lam, H.Y.S.; Fong, A.H.; Leung, S.T.; Chin, T.W.; Lo, C.S.Y.; Lui, M.M.; Lee, J.C.Y.; Chiu, K.W.; Chung, T.W.; et al. Frequency and Distribution of Chest Radiographic Findings in COVID-19 Positive Patients. Radiology 2019, 201160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodrigues, J.C.L.; Hare, S.S.; Edey, A.; Devaraj, A.; Jacob, J.; Johnstone, A.; McStay, R.; Nair, A.; Robinson, G. An update on COVID-19 for the radiologist—A British society of Thoracic Imaging statement. Clin. Radiol. 2020, 75, 323–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fulop, T.; McElhaney, J.; Pawelec, G.; Cohen, A.A.; Morais, J.A.; Dupuis, G.; Baehl, S.; Camous, X.; Witkowski, J.M.; Larbi, A. Frailty, Inflammation and Immunosenescence. Interdiscip Top Gerontol. Geriatr. 2015, 41, 26–40. [Google Scholar] [CrossRef]
- Herold, T.; Jurinovic, V.; Arnreich, C.; Lipworth, B.J.; Hellmuth, J.C.; von Bergwelt-Baildon, M.; Klein, M.; Weinberger, T. Elevated levels of IL-6 and CRP predict the need for mechanical ventilation in COVID-19. J Allergy Clin. Immunol. 2020, 146, 128–136.e4. [Google Scholar] [CrossRef] [PubMed]
- RECOVERY Collaborative Group; Horby, P.; Lim, W.S.; Emberson, J.; Mafham, M.; Bell, J.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Effect of Dexamethasone in Hospitalized Patients with COVID-19: Preliminary Report. Dexamethasone in Hospitalized Patients with Covid-19—Preliminary Report. N. Engl. J. Med. 2020, 17. [Google Scholar] [CrossRef]
- Romero-Ortuno, R.; Forsyth, D.R.; Wilson, K.J.; Cameron, E.; Wallis, S.; Biram, R.; Keevil, V. The Association of Geriatric Syndromes with Hospital Outcomes. J. Hosp. Med. 2017, 12, 83–89. [Google Scholar] [CrossRef] [Green Version]
- NICE. COVID-19 Rapid Guideline: Critical Care (NICE Guideline NG159) 2020. Available online: https://www.nice.org.uk/guidance/ng159 (accessed on 20 July 2020).
- Coronavirus (COVID-19) Related Deaths by Ethnic Group, England and Wales. Office for National Statistics. 2020. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/articles/coronavirusrelateddeathsbyethnicgroupenglandandwales/2march2020to10april2020 (accessed on 16 June 2020).
- Are Some Ethnic Groups More Vulnerable to COVID-19 Than Others? Institute of Fiscal Studies. 2020. Available online: https://www.ifs.org.uk/inequality/chapter/are-some-ethnic-groups-more-vulnerable-to-covid-19-than-others/ (accessed on 16 June 2020).



{kind=link}
{kind=link}
| Characteristic, Median (IQR) | All (n = 214) | Non-Frail (n = 72) | Frail (n = 142) | p |
|---|---|---|---|---|
| Age, years | 80 (75, 87) | 75 (70, 77) | 84 (77, 89) | <0.001 |
| Sex, % (n) women | 43.9 (94) | 29.2 (21) | 51.4 (73) | 0.002 |
| CFS | 6 (4, 7) | 3 (2, 4) | 6 (6, 7) | <0.001 |
| BMI, Kg/m2 | 24.6 (21.2, 29.2) | 26.5 (23.3, 31.2) | 23.5 (20.1, 27.7) | 0.0015 |
| Known Dementia, % (n) | 27.1 (58) | 1.4 (1) | 40.1 (57) | <0.001 |
| Admission from care home, % (n) | 31.3 (67) | 0 (0) | 47.3 (67) | <0.001 |
| Pre-admission mobility, % (n) | <0.001 | |||
| Independent | 39.3 (84) | 84.7 (61) | 16.2 (23) | |
| Stick | 15.0 (32) | 9.7 (7) | 17.6 (25) | |
| Frame | 33.6 (72) | 5.6 (4) | 47.9 (68) | |
| Immobile | 12.2 (26) | 0 (0) | 18.3 (26) | |
| Symptoms, % (n) | ||||
| Fever | 73.4 (157) | 81.9 (59) | 69.0 (98) | 0.043 |
| Cough | 63.6 (136) | 76.4 (55) | 57.0 (81) | 0.005 |
| SOB | 59.8 (128) | 62.5 (45) | 58.5 (83) | 0.568 |
| Fatigue | 48.1 (103) | 62.5 (45) | 40.8 (58) | 0.003 |
| Myalgia | 14.5(31) | 26.4 (19) | 8.5 (12) | <0.001 |
| Confusion | 36.9 (79) | 20.8 (15) | 45.1 (64) | 0.001 |
| Fall | 20.6 (44) | 12.5 (9) | 24.7 (35) | 0.038 |
| N & V | 18.7 (40) | 25.0 (18) | 15.5 (22) | 0.092 |
| Diarrhoea | 16.4 (35) | 31.9 (23) | 8.5 (12) | <0.001 |
| Abdominal pain | 7.0 (15) | 12.5 (9) | 4.2 (6) | 0.025 |
| Taste/ smell | 4.7 (10) | 9.7 (7) | 2.1 (3) | 0.013 |
| Non-specifically unwell | 19.2 (41) | 6.9 (5) | 25.4 (36) | 0.001 |
| Multimorbidity, % (n) | <0.001 | |||
| <2 LTC | 7.5 (16) | 16.7 (12) | 2.8 (4) | |
| 2 LTC | 9.8 (21) | 16.7 (12) | 6.3 (9) | |
| ≥3 LTC | 82.7 (177) | 66.7 (48) | 90.8 (129) | |
| Polypharmacy, % (n) 0–4 medications 5–9 medications ≥10 medications | 21.0 (45) 51.9 (111) 27.1 (58) | 36.1 (26) 45.8 (33) 18.1 (13) | 13.4 (19) 54.9 (78) 31.7 (45) | <0.001 |
| CXR on COVID-19 presentation % (n) | ||||
| Classical/Probable COVID-19 | 34.6 (74) | 50.0 (36) | 26.8 (38) | |
| Indeterminate for COVID-19 | 17.8 (38) | 19.4 (14) | 16.9 (24) | |
| Non COVID-19 Features | 18.7 (40) | 9.7 (7) | 23.2 (33) | |
| Normal | 28.5 (61) | 20.8 (15) | 32.3 (46) | 0.002 |
| Hospital Acquired Disease, % (n) | 9.8 (21) | 11.1 (8) | 9.2 (13) | 0.649 |
| Time to first positive swab *, days | 0 (0, 1) | 0 (0, 1) | 0 (0, 1) | 0.290 |
| Acuity, % (n) yes | ||||
| Low (NEWS2 <5) | 45.3 (97) | 50.0 (36) | 43.0 (61) | |
| High (NEWS2 ≥5) | 54.7 (117) | 50.0 (36) | 57.0 (81) | 0.328 |
| Vital signs, % (n) | ||||
| Fever >38.0 °C | 28.5 (61) | 40.3 (29) | 22.5 (32) | 0.007 |
| Respiratory rate >24 bpm | 38.8 (83) | 36.1 (26) | 40.1 (57) | 0.568 |
| Systolic blood pressure ≤90 mmHg | 3.3 (7) | 0 (0) | 4.9 (7) | 0.060 |
| Pulse >130 bpm | 5.1 (11) | 5.6 (4) | 4.9 (7) | 0.845 |
| Laboratory Values | ||||
| White blood cells, 109/L | 6.9 (5.0, 9.6) | 6.3 (4.9, 8.6) | 7.4 (5.1, 10.0) | 0.094 |
| Neutrophils, 109/L | 5.4 (3.7, 7.8) | 4.8 (3.6, 7.2) | 5.8 (3.8, 8.2) | 0.19 |
| Lymphocytes, 109/L | 0.67 | 0.61 | 0.67 | 0.28 |
| (0.48, 1.01) | (0.46, 0.90) | (0.50, 1.04) | ||
| Creatinine, µmol/l | 89.0 | 87.5 | 89.5 | 0.32 |
| (71.1, 118.5) | (69.5, 111.0) | (71.6, 128.6) | ||
| C-Reactive Protein, % (n) | 0.007 | |||
| <40 mg/L | 30.3 (65) | 18.1 (13) | 36.7 (52) | |
| 40–100 mg/L | 31.3 (67) | 30.6 (22) | 31.7 (45) | |
| >100 mg/L | 37.4 (80) | 50.0 (36) | 31.0 (44) | |
| Interleukin-6, pg/mL | 19.6 (7.3, 50.8) | 26.8 (9.6, 71.1) | 17.6 (6.6, 39.2) | 0.04 |
| Troponin, % (n) ≤58.1 ng/L >58.1 ng/L | 50.9 (109) 23.8 (51) | 68.1 (49) 16.7 (12) | 42.3 (60) 27.5 (39) | 0.009 |
| D Dimer, % (n) | ||||
| ≤230 ng/mL | 15.6 (35) | 16.7 (12) | 16.2 (23) | |
| >230 ng/mL | 54.2 (116) | 54.1 (39) | 54.2 (77) | 0.942 |
| Hospital Trajectory and Outcome | All (n = 214) | Non-Frail (n = 72) | Frail (n = 142) | p |
|---|---|---|---|---|
| Ward moves, % (n) | 0.021 | |||
| Up to 1 | 42.1 (90) | 44.4 (32) | 40.8 (58) | |
| 2 | 33.2 (71) | 27.8 (20) | 35.9 (51) | |
| 3 | 15.4 (33) | 12.5 (9) | 16.9 (24) | |
| 4 or more | 9.4 (20) | 14.3 (11) | 6.4 (9) | |
| Admission to High Care, % (n) | 10.3 (22) | 29.2 (21) | 0.7 (1) | <0.001 |
| Delirium or new confusion during admission at any point, % (n) | 47.7 (102) | 29.2 (21) | 57.0 (81) | <0.001 |
| Mobility at discharge *, % (n) | <0.001 | |||
| Independent | 35.0 (49) | 75.4 (43) | 7.2 (6) | |
| Stick | 5.7 (8) | 3.5 (2) | 7.2 (6) | |
| Frame | 37.1 (52) | 17.5 (10) | 50.6 (42) | |
| Immobile | 20.0 (28) | 0 (0) | 33.7 (28) | |
| Length of stay, days # | 11 (6, 18) | 8 (4, 17) | 12 (7, 19) | 0.08 |
| Hospital outcomes, % (n) | ||||
| Inpatient Death | 34.6 (74) | 20.8 (15) | 41.6 (59) | 0.003 |
| Death as inpatient or within 14 days of discharge | 38.3 (82) | 22.2 (16) | 46.7 (66) | 0.001 |
| Prolonged length of stay (>10 days) | 53.5 (114) | 45.1 (32) | 57.8 (82) | 0.08 |
| New Institutionalisation * | 5.6 (12) | 3.5 (2) | 12.1 (10) | 0.08 |
| Readmission * | 19.3 (27) | 15.8 (9) | 21.7 (18) | 0.385 |
| Delayed transfer of care * | 46.4 (65) | 26.3 (15) | 60.2 (50) | <0.001 |
| Univariable Analysis | Multivariable Analysis | |||
|---|---|---|---|---|
| Characteristic | HR | 95% Confidence Interval | HR | 95% Confidence Interval |
| Age, years | 1.04 | 1.02, 1.07 | 1.04 | 1.01, 1.07 |
| Sex | ||||
| Women | Ref | Ref | ||
| Men | 1.47 | 0.94, 2.30 | 2.03 | 1.27, 3.24 |
| CFS | ||||
| 1–4 | Ref | Ref | ||
| 5–6 | 1.99 | 1.11, 3.59 | 1.78 | 0.90, 3.53 |
| 7–8 | 2.83 | 1.54, 5.19 | 2.57 | 1.26, 5.24 |
| Acuity, NEWS2 | ||||
| Low (<5) | Ref | Ref | ||
| High (≥5) | 2.30 | 1.42, 3.65 | 2.33 | 1.45, 3.74 |
| Multimorbidity | ||||
| 0–1 LTC | Ref | Ref | ||
| 2 LTC | 0.99 | 0.30, 3.28 | 0.89 | 0.22, 2.68 |
| ≥3 LTC | 1.44 | 0.58, 3.58 | 0.85 | 0.32, 2.30 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Osuafor, C.N.; Davidson, C.; Mackett, A.J.; Goujon, M.; Van Der Poel, L.; Taylor, V.; Preller, J.; Goudie, R.J.B.; Keevil, V.L. Clinical Features, Inpatient Trajectories and Frailty in Older Inpatients with COVID-19: A Retrospective Observational Study. Geriatrics 2021, 6, 11. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics6010011
Osuafor CN, Davidson C, Mackett AJ, Goujon M, Van Der Poel L, Taylor V, Preller J, Goudie RJB, Keevil VL. Clinical Features, Inpatient Trajectories and Frailty in Older Inpatients with COVID-19: A Retrospective Observational Study. Geriatrics. 2021; 6(1):11. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics6010011
Chicago/Turabian StyleOsuafor, Christopher N., Catriona Davidson, Alistair J. Mackett, Marie Goujon, Lelane Van Der Poel, Vince Taylor, Jacobus Preller, Robert J. B. Goudie, and Victoria L. Keevil. 2021. "Clinical Features, Inpatient Trajectories and Frailty in Older Inpatients with COVID-19: A Retrospective Observational Study" Geriatrics 6, no. 1: 11. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics6010011