
Relationship between Measured Aerobic Capacity and Total Energy Expenditure Obtained by the Doubly Labeled Water Method in Community-Dwelling, Healthy Adults Aged 81–94 Years

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Aerobic Capacity
2.3. TEE Using DLW Methods
2.4. International Physical Activity Questionnaire
2.5. Statistical Analysis
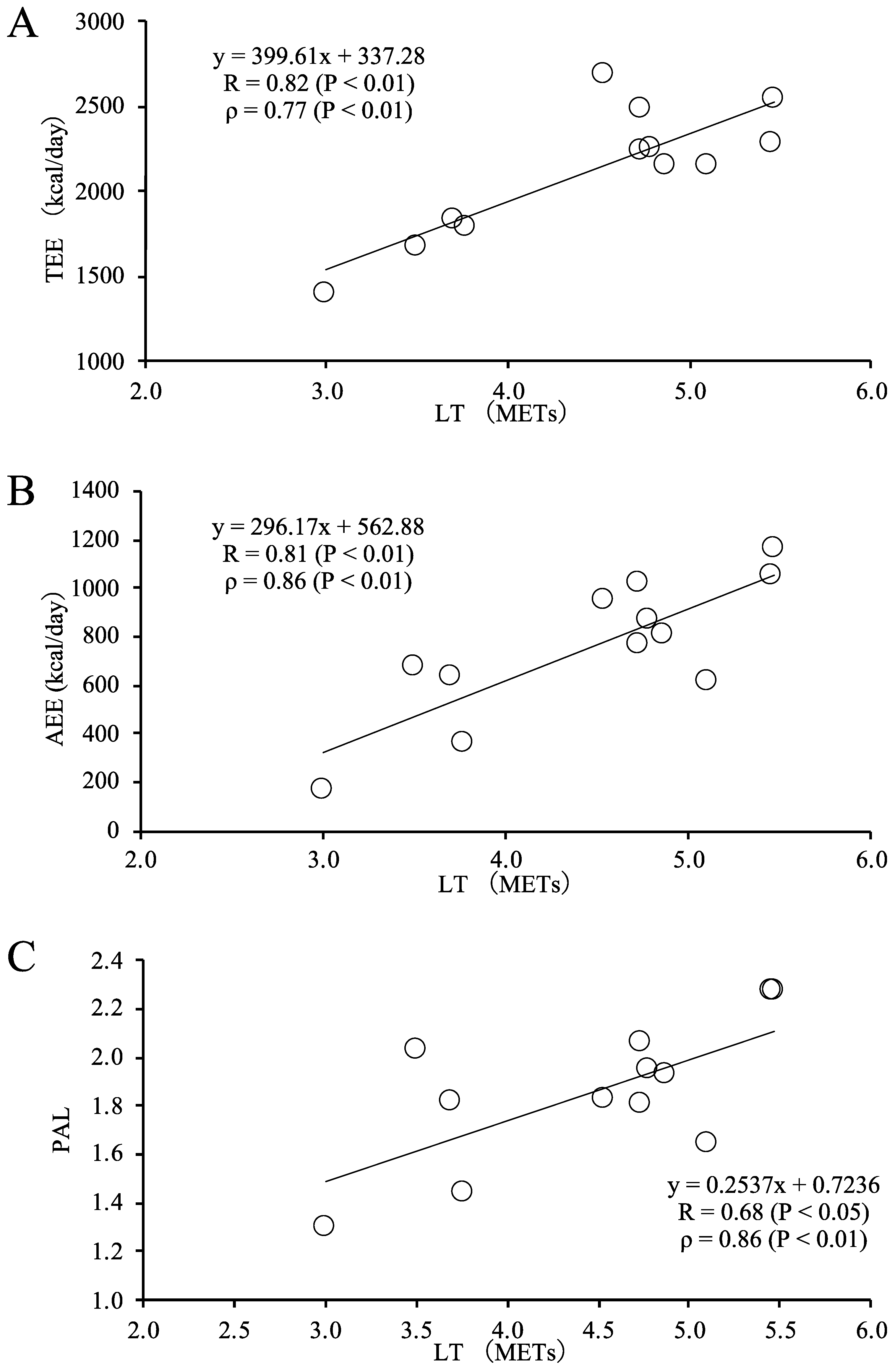
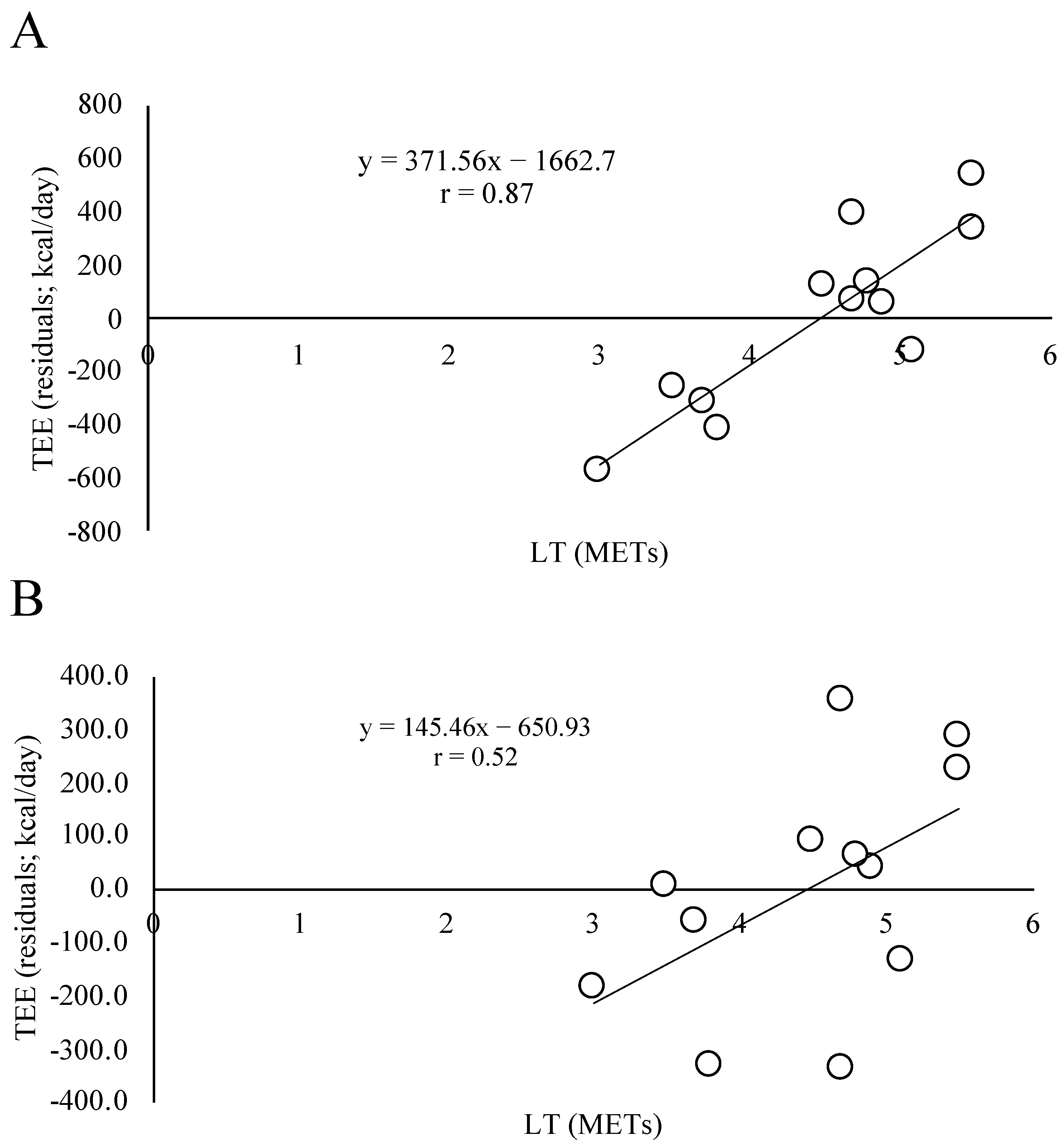
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Walston, J. Frailty and failure to thrive. In Principles of Geriatric Medicine and Gerontology, 4th ed.; Hazzard, W.R., Blass, J.P., Ettinger, W.H., Jr., Halter, J.B., Ouslander, J., Eds.; McGraw Hill: New York, NY, USA, 1998; Volume 1387–1402. [Google Scholar]
- Westerterp, K.R. Physical activity and physical activity induced energy expenditure in humans: Measurement, determinants, and effects. Front. Physiol. 2013, 4, 90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Speakman, J.R.; Yamada, Y.; Ainslie, P.N.; Andersen, L.F.; Anderson, L.J.; Arab, L.; Baddou, I.; Bedu-Addo, K.; Blaak, E.E.; Blanc, S.; et al. A standard calculation methodology for human doubly labeled water studies. Cell. Rep. Med. 2021, 2, 100203. [Google Scholar] [CrossRef] [PubMed]
- Xue, Q.L.; Bandeen-Roche, K.; Varadhan, R.; Zhou, J.; Fried, L.P. Initial manifestations of frailty criteria and the development of frailty phenotype in the Women’s Health and Aging Study II. J. Gerontol. A Biol. Sci. Med. Sci. 2008, 63, 984–990. [Google Scholar] [CrossRef] [Green Version]
- Yamada, Y.; Nanri, H.; Watanabe, Y.; Yoshida, T.; Yokoyama, K.; Itoi, A.; Date, H.; Yamaguchi, M.; Miyake, M.; Yamagata, E.; et al. Prevalence of frailty assessed by Fried and Kihon checklist indices in a prospective cohort study: Design and demographics of the Kyoto-Kameoka longitudinal study. J. Am. Med. Dir. Assoc. 2017, 18, 733.e7–733.e15. [Google Scholar] [CrossRef]
- Watanabe, D.; Yoshida, T.; Nanri, H.; Watanabe, Y.; Date, H.; Itoi, A.; Goto, C.; Ishikawa-Takata, K.; Sagayama, H.; Ebine, N.; et al. Association between the prevalence of frailty and doubly labeled water-calibrated energy intake among community-dwelling older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 76, 876–884. [Google Scholar] [CrossRef]
- Watanabe, D.; Yoshida, T.; Watanabe, Y.; Yamada, Y.; Kimura, M.; Group, K.S. Objectively Measured Daily Step Counts and Prevalence of Frailty in 3,616 Older Adults. J. Am. Geriatr. Soc. 2020, 68, 2310–2318. [Google Scholar] [CrossRef]
- Sasai, H.; Nakata, Y.; Murakami, H.; Kawakami, R.; Nakae, S.; Tanaka, S.; Ishikawa-Takata, K.; Yamada, Y.; Miyachi, M. Simultaneous Validation of Seven Physical Activity Questionnaires Used in Japanese Cohorts for Estimating Energy Expenditure: A Doubly Labeled Water Study. J. Epidemiol. 2018, 28, 437–442. [Google Scholar] [CrossRef] [Green Version]
- Frisard, M.I.; Fabre, J.M.; Russell, R.D.; King, C.M.; DeLany, J.P.; Wood, R.H.; Ravussin, E. Physical activity level and physical functionality in nonagenarians compared to individuals aged 60–74 years. J. Gerontol. A Biol. Sci. Med. Sci. 2007, 62, 783–788. [Google Scholar] [CrossRef]
- Yamada, Y.; Hashii-Arishima, Y.; Yokoyama, K.; Itoi, A.; Adachi, T.; Kimura, M. Validity of a triaxial accelerometer and simplified physical activity record in older adults aged 64–96 years: A doubly labeled water study. Eur. J. Appl. Physiol. 2018, 118, 2133–2146. [Google Scholar] [CrossRef]
- Nishida, Y.; Nakae, S.; Yamada, Y.; Kondo, E.; Yamaguchi, M.; Shirato, H.; Hirano, H.; Sasaki, S.; Tanaka, S.; Katsukawa, F. Validity of One-Day Physical Activity Recall for Estimating Total Energy Expenditure in Elderly Residents at Long-Term Care Facilities: CLinical EValuation of Energy Requirements Study (CLEVER Study). J. Nutr. Sci. Vitaminol. 2019, 65, 148–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takae, R.; Hatamoto, Y.; Yasukata, J.; Kose, Y.; Komiyama, T.; Ikenaga, M.; Yoshimura, E.; Yamada, Y.; Ebine, N.; Higaki, Y.; et al. Physical Activity and/or High Protein Intake Maintains Fat-Free Mass in Older People with Mild Disability; the Fukuoka Island City Study: A Cross-Sectional Study. Nutrients 2019, 11, 2595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mori, Y.; Ayabe, M.; Yahiro, T.; Tobina, T.; Kiyonaga, A.; Shindo, M.; Yamada, T.; Tanaka, H. The effects of home-based bench step exercise on aerobic capacity, lower extremity power and static balance in older adults. Int. J. Sport Health Sci. 2006, 4, 570–576. [Google Scholar] [CrossRef] [Green Version]
- Nishida, Y.; Tanaka, K.; Hara, M.; Hirao, N.; Tanaka, H.; Tobina, T.; Ikeda, M.; Yamato, H.; Ohta, M. Effects of home-based bench step exercise on inflammatory cytokines and lipid profiles in elderly Japanese females: A randomized controlled trial. Arch. Gerontol. Geriatr. 2015, 61, 443–451. [Google Scholar] [CrossRef] [PubMed]
- Borg, G. Psychophysical scaling with applications in physical work and the perception of exertion. Scand. J. Work Environ. Health 1990, 16 (Suppl. 1), 55–58. [Google Scholar] [CrossRef]
- Martin, S.B.; Morrow, J.R., Jr.; Jackson, A.W.; Dunn, A.L. Variables related to meeting the CDC/ACSM physical activity guidelines. Med. Sci. Sports Exerc. 2000, 32, 2087–2092. [Google Scholar] [CrossRef] [Green Version]
- Coward, W.A. Calculation of pool sizes and flux rates. In The Doubly-Labelled Water Method for the Measurement of Energy Expenditure; Prentice, A.M., Ed.; International Atomic Energy Agency: Vienna, Austria, 1990; pp. 48–65. [Google Scholar]
- Blanc, S.; Colligan, A.S.; Trabulsi, J.; Harris, T.; Everhart, J.E.; Bauer, D.; Schoeller, D.A. Influence of delayed isotopic equilibration in urine on the accuracy of the H-2(2) O-18 method in the elderly. J. Appl. Physiol. 2002, 92, 1036–1044. [Google Scholar] [CrossRef] [Green Version]
- Blanc, S.; Schoeller, D.A.; Bauer, D.; Danielson, M.E.; Tylavsky, F.; Simonsick, E.M.; Harris, T.B.; Kritchevsky, S.B.; Everhart, J.E. Energy requirements in the eighth decade of life. Am. J. Clin. Nutr. 2004, 79, 303–310. [Google Scholar] [CrossRef] [Green Version]
- Racette, S.B.; Schoeller, D.A.; Luke, A.H.; Shay, K.; Hnilicka, J.; Kushner, R.F. Relative dilution spaces of 2H- and 18O-labeled water in humans. Am. J. Physiol. Endocrinol. Metab. 1994, 267, E585–E590. [Google Scholar] [CrossRef]
- Sagayama, H.; Yamada, Y.; Racine, N.M.; Shriver, T.C.; Schoeller, D.A. Dilution space ratio of 2H and 18O of doubly labeled water method in humans. J. Appl. Physiol. 2016, 120, 1349–1354. [Google Scholar] [CrossRef] [Green Version]
- Schoeller, D.A.; Ravussin, E.; Schutz, Y.; Acheson, K.J.; Baertschi, P.; Jequier, E. Energy expenditure by doubly labeled water: Validation in humans and proposed calculation. Am. J. Physiol. Regul. Integr. Comp. Physiol. 1986, 250, R823–R830. [Google Scholar] [CrossRef] [PubMed]
- Weir, J.B. New methods for calculating metabolic rate with special reference to protein metabolism. J. Physiol. 1949, 109, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Black, A.E.; Prentice, A.M.; Coward, W.A. Use of food quotients to predict respiratory quotients for the doubly-labelled water method of measuring energy expenditure. Hum. Nutr. Clin. Nutr. 1986, 40, 381–391. [Google Scholar]
- Ishikawa-Takata, K.; Tabata, I.; Sasaki, S.; Rafamantanantsoa, H.H.; Okazaki, H.; Okubo, H.; Tanaka, S.; Yamamoto, S.; Shirota, T.; Uchida, K.; et al. Physical activity level in healthy free-living Japanese estimated by doubly labelled water method and International Physical Activity Questionnaire. Eur. J. Clin. Nutr. 2007, 62, 885–891. [Google Scholar] [CrossRef] [Green Version]
- Yamada, Y.; Yokoyama, K.; Noriyasu, R.; Osaki, T.; Adachi, T.; Itoi, A.; Naito, Y.; Morimoto, T.; Kimura, M.; Oda, S. Light-intensity activities are important for estimating physical activity energy expenditure using uniaxial and triaxial accelerometers. Eur. J. Appl. Physiol. 2009, 105, 141–152, Erratum in Eur. J. Appl. Physiol. 2016, 116, 1279–1280. [Google Scholar] [CrossRef]
- Ganpule, A.A.; Tanaka, S.; Ishikawa-Takata, K.; Tabata, I. Interindividual variability in sleeping metabolic rate in Japanese subjects. Eur. J. Clin. Nutr. 2007, 61, 1256–1261. [Google Scholar] [CrossRef] [Green Version]
- Itoi, A.; Yamada, Y.; Yokoyama, K.; Adachi, T.; Kimura, M. Validity of predictive equations for resting metabolic rate in healthy older adults. Clin. Nutr. ESPEN 2017, 22, 64–70. [Google Scholar] [CrossRef]
- Wang, Z. Hydration of fat-free body mass: Review and critique of a classic. Am. J. Clin. Nutr. 1999, 69, 833–841. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- Tomioka, K.; Iwamoto, J.; Saeki, K.; Okamoto, N. Reliability and validity of the International Physical Activity Questionnaire (IPAQ) in elderly adults: The Fujiwara-kyo Study. J. Epidemiol. 2011, 21, 459–465. [Google Scholar] [CrossRef] [Green Version]
- Inui, T.; Hanley, B.; Tee, E.S.; Nishihira, J.; Tontisirin, K.; Van Dael, P.; Eggersdorfer, M. The Role of Micronutrients in Ageing Asia: What Can Be Implemented with the Existing Insights. Nutrients 2021, 13, 2222. [Google Scholar] [CrossRef] [PubMed]
- Takae, R.; Hatamoto, Y.; Yasukata, J.; Kose, Y.; Komiyama, T.; Ikenaga, M.; Yoshimura, E.; Yamada, Y.; Ebine, N.; Higaki, Y.; et al. Association of Lower-Extremity Muscle Performance and Physical Activity Level and Intensity in Middle-Aged and Older Adults: A Doubly Labeled Water and Accelerometer Study. J. Nutr. Health Aging 2020, 24, 1023–1030. [Google Scholar] [CrossRef] [PubMed]
- Huggett, D.L.; Connelly, D.M.; Overend, T.J. Maximal aerobic capacity testing of older adults: A critical review. J. Gerontol. A Biol. Sci. Med. Sci. 2005, 60, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Tokmakidis, S.P.; Léger, L.A.; Pilianidis, T.C. Failure to obtain a unique threshold on the blood lactate concentration curve during exercise. Eur. J. Appl. Physiol. Occup. Physiol. 1998, 77, 333–342. [Google Scholar] [CrossRef]
- Yoshida, T.; Chida, M.; Ichioka, M.; Suda, Y. Blood lactate parameters related to aerobic capacity and endurance performance. Eur. J. Appl. Physiol. Occup. Physiol. 1987, 56, 7–11. [Google Scholar] [CrossRef]
- Svedahl, K.; MacIntosh, B.R. Anaerobic threshold: The concept and methods of measurement. Can. J. Appl. Physiol. 2003, 28, 299–323. [Google Scholar] [CrossRef] [Green Version]
- Ikenaga, M.; Yamada, Y.; Kose, Y.; Morimura, K.; Higaki, Y.; Kiyonaga, A.; Tanaka, H. Effects of a 12-week, short-interval, intermittent, low-intensity, slow-jogging program on skeletal muscle, fat infiltration, and fitness in older adults: Randomized controlled trial. Eur. J. Appl. Physiol. 2017, 117, 7–15. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Mean ± SD | |
|---|---|
| Age (yrs) | 84.5 ± 3.5 |
| Height (cm) | 158.1 ± 6.9 |
| Body mass (kg) | 58.1 ± 10.2 |
| TBW (kg) | 30.4 ± 5.3 |
| FFM | 41.5 ± 6.9 |
| FM | 16.6 ± 6.9 |
| FFMI | 16.6 ± 2.4 |
| FMI | 6.7 ± 2.8 |
| TEE (kcal/day) | 2123 ± 383 |
| eBMR (kcal/day) | 1150 ± 383 |
| PAL | 1.86 ± 0.30 |
| AEE (kcal/day) | 761 ± 288 |
| LT (METs) | 4.5 ± 0.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yasukata, J.; Yamada, Y.; Sagayama, H.; Higaki, Y.; Tanaka, H. Relationship between Measured Aerobic Capacity and Total Energy Expenditure Obtained by the Doubly Labeled Water Method in Community-Dwelling, Healthy Adults Aged 81–94 Years. Geriatrics 2022, 7, 48. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics7020048
Yasukata J, Yamada Y, Sagayama H, Higaki Y, Tanaka H. Relationship between Measured Aerobic Capacity and Total Energy Expenditure Obtained by the Doubly Labeled Water Method in Community-Dwelling, Healthy Adults Aged 81–94 Years. Geriatrics. 2022; 7(2):48. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics7020048
Chicago/Turabian StyleYasukata, Jun, Yosuke Yamada, Hiroyuki Sagayama, Yasuki Higaki, and Hiroaki Tanaka. 2022. "Relationship between Measured Aerobic Capacity and Total Energy Expenditure Obtained by the Doubly Labeled Water Method in Community-Dwelling, Healthy Adults Aged 81–94 Years" Geriatrics 7, no. 2: 48. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics7020048