
The Artificial Intelligence in Digital Radiology: Part 2: Towards an Investigation of acceptance and consensus on the Insiders

Abstract
:1. Introduction
Artificial Intelligence and Digital Radiology
- A first point of view is that DR includes different imaging sectors where it can potentially be applied. If we exclude imaging processes that do not involve ionizing radiation, we can identify the following sectors, both with reference to organ and total body diagnostics:
- Interventional radiology
- Diagnostic radiology (radiology, CT)
- Nuclear magnetic resonance
- Positron emission tomography
- amma chamber
- A second point of view is represented by the transversal sectors that embrace these disciplines in which AI can play an important role:
- Therapy
- Prevention
- Quality control
- Risk assessment
- A third point of view is represented by the AI app distribution methods. In fact, we must not forget that AI, in the context of DR, has a future of standardization related to software for medical devices [29]. This software has different implications if it is used standalone or on the network, and if it is networked through eHealth or mHealth solutions. The implications also concern important aspects of cybersecurity [30].
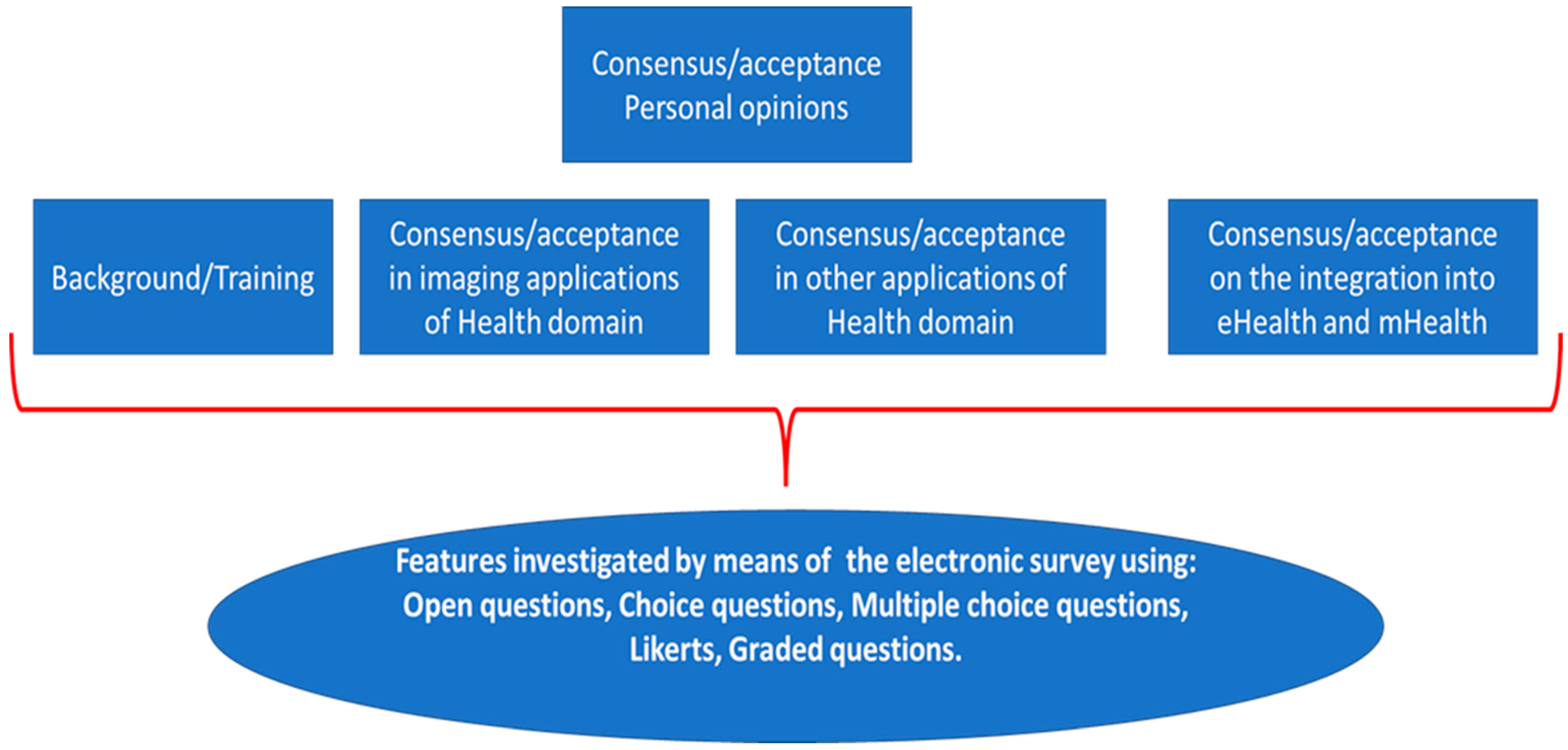
- A fourth point of view is represented by the specific training that must include AI and also the related disciplines such as informatics, medical imaging and the technologies for biomedical app.
- must consider the above-listed (1–4) points of views, not limited to imaging and including the integration into eHealth and mHealth [49];
- must consider all the involved professionals who have different training and a different work-flow and therefore different expectations from AI.
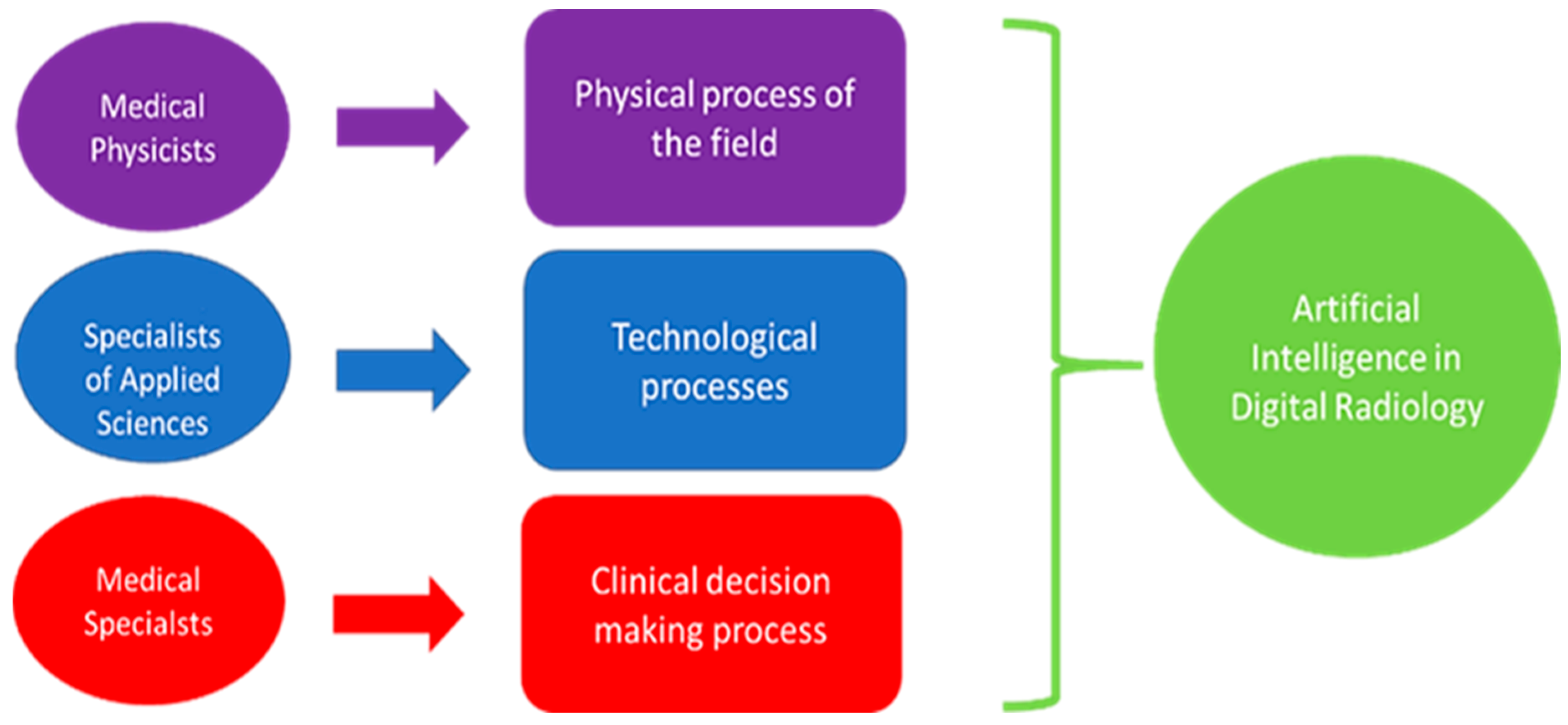
- the medical physics;
- the medical specialist;
- the specialist in applied sciences.
2. Methods
- Verification of data normality;
- Application of the ANOVA with a P lower than 0.01 for the significance of differences.
- FEDERATION OF ITALIAN MEDICAL-SCIENTIFIC SOCIETIES [53] (includes associations such as the Italian association of medical and health physics and other relevant scientific societies and other societies operating in the Medical Diagnostics and in related fields) mainly for the first two professionals MPs and MSs but also for the SASs.
- FEDERATION OF SCIENTIFIC AND TECHNICAL ASSOCIATIONS [54] (contains the National Group of Bioengineering and other relevant scientific societies) and FEDERATION OF SCIENTIFIC ASSOCIATIONS OF RADIOLOGY TECHNICIANS [55] (contains for example the Italian association of system administrators and telemedicine, association of interventional radiology technicians, Health Imaging Sciences Association, and other relevant societies) mainly for the SASs but also for the other professionals.
3. Results
3.1. Outcome of the Closed Questions from the Survey
3.2. Key Considerations from the Submission Process and Suggestions from the Open Questions
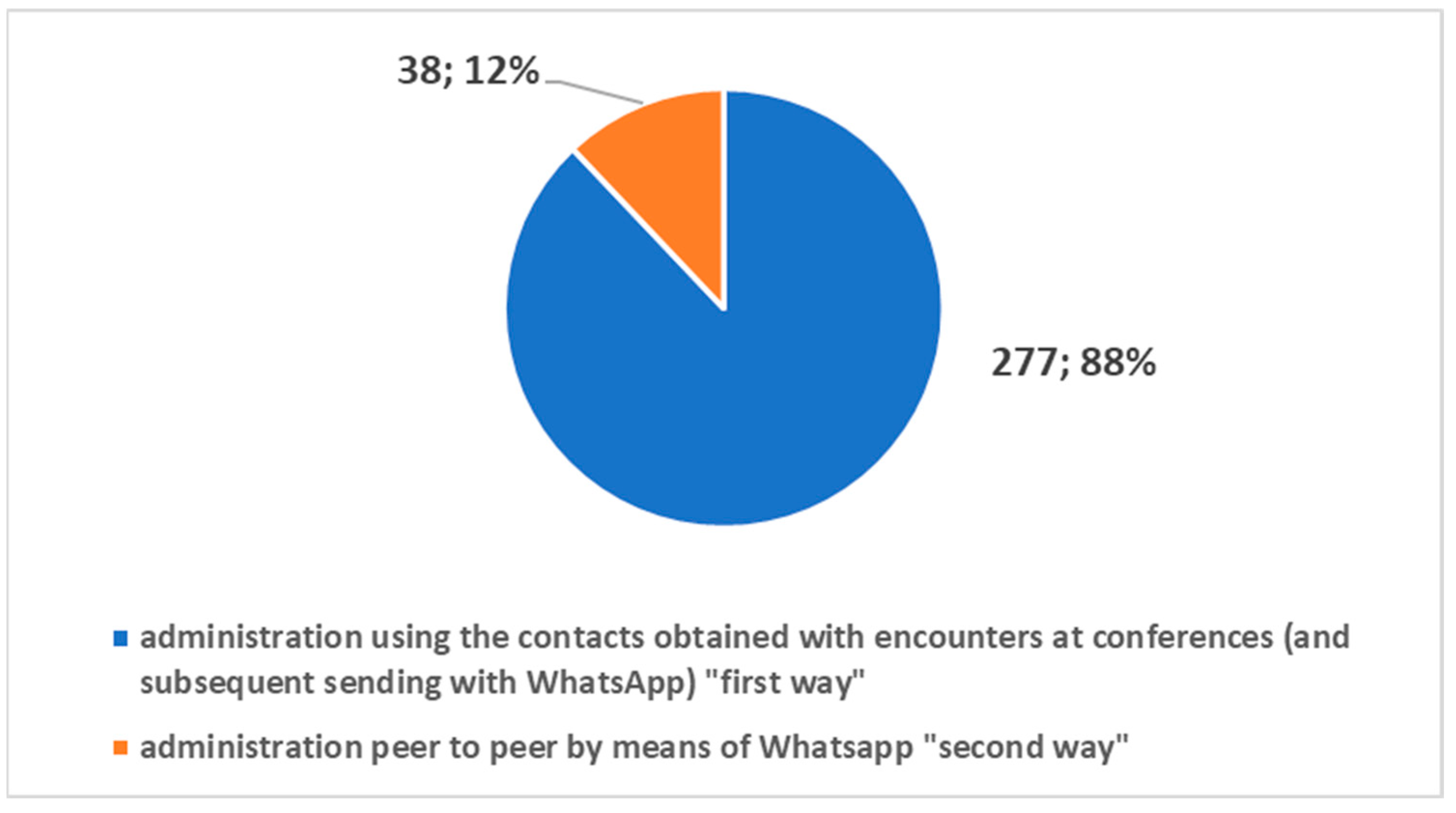
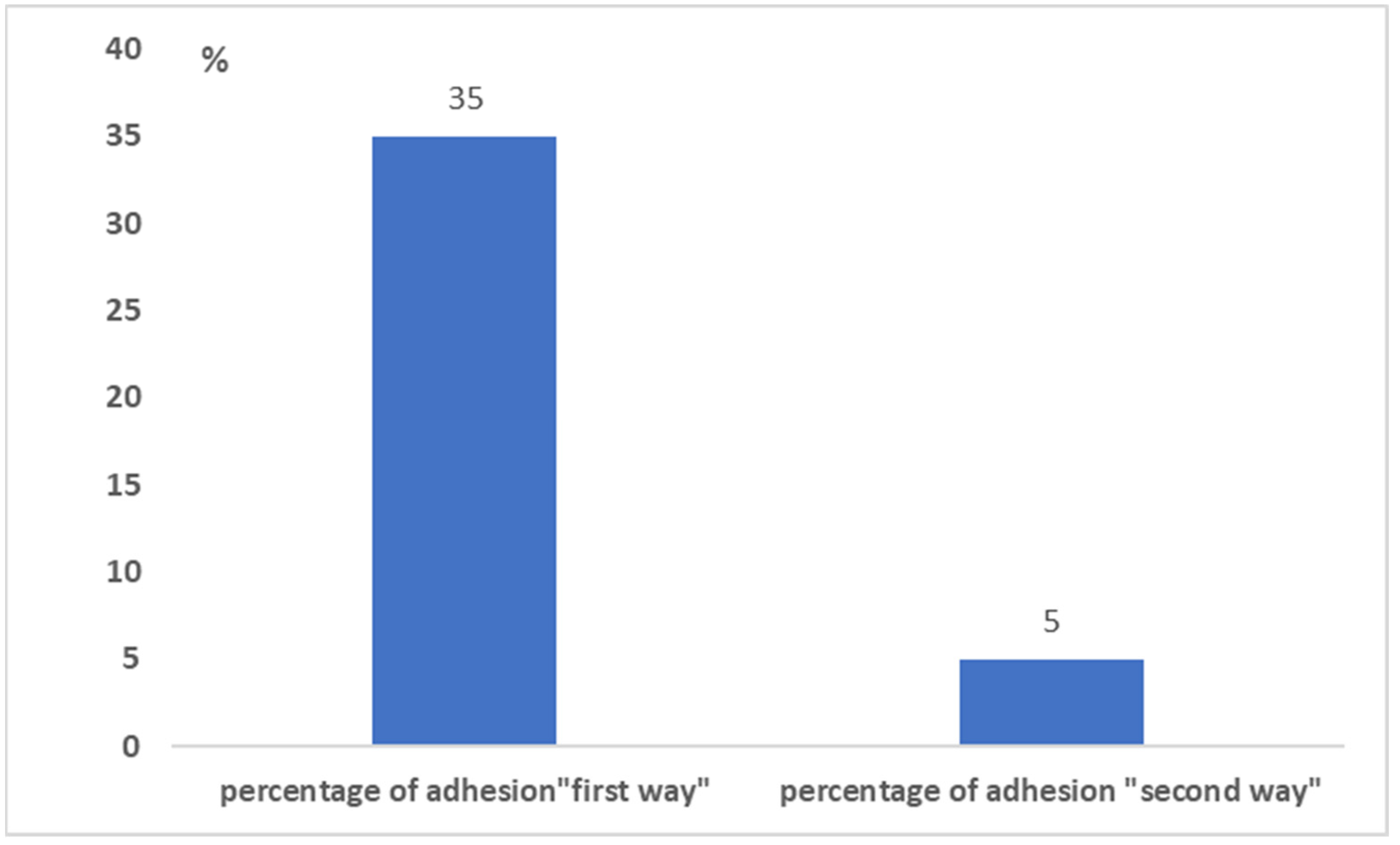
3.2.1. Adhesion to the Survey
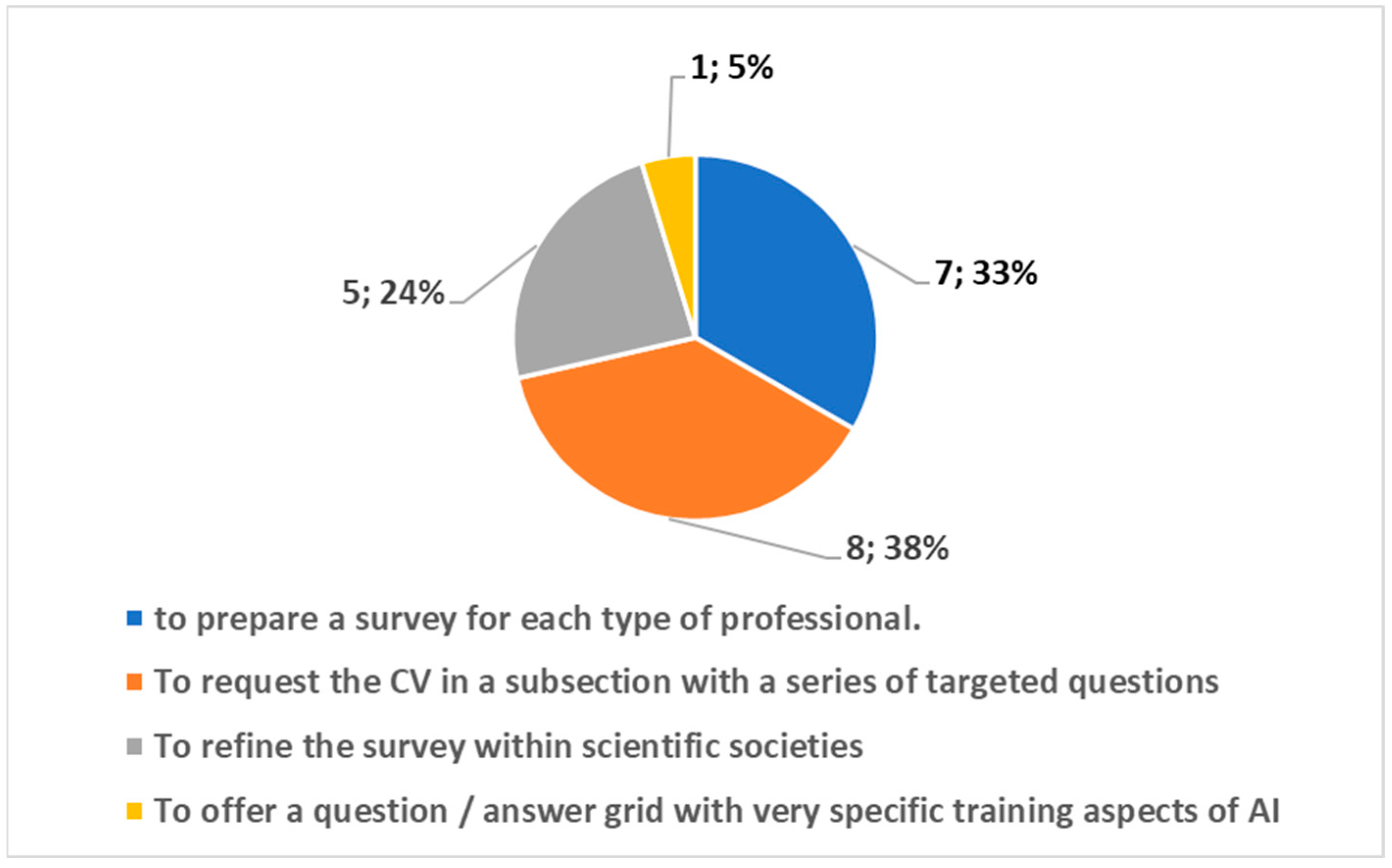
3.2.2. Outcome from the Open Question
- o to request the CV in a subsection with a series of targeted questions;
- o to prepare a survey for each type of professional;
- o to refine the survey within scientific societies;
- o to offer a question/answer grid with very specific training aspects of AI.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| Acronym | Description |
| AI | Artificial intelligence |
| CT | Computerized tomography |
| MP | Medical physicist |
| SAS | Specialists of applied sciences |
| MS | Medical specialist |
| DICOM | Digital imaging and communications in medicine |
| DR | Digital radiology |
| TA | Technology assessment |
| HTA | Health technology assessment |
| CER | Comparative effectiveness research |
| PCP | Primary care provider |
| TP | Technological process |
| TMV | Theorical mean value |
| PP | Physical process |
| DP | Decision-making process |
| ANOVA | Analysis of variance |
| eHealth | Electronic health |
| mHealth | Mobile health |
Appendix A


References
- Thrall, J.H. Teleradiology. Part I. History and clinical applications. Radiology 2007, 243, 613–617. [Google Scholar] [CrossRef] [PubMed]
- Thrall, J.H. Teleradiology. Part II. Limitations, risks, and opportunities. Radiology 2007, 244, 325–328. [Google Scholar] [CrossRef] [PubMed]
- Reponen, J. Teleradiology—Changing Radiological Service Processes from Local to Regional, International and Mobile Environment; University of Oulu: Oulu, Finland, 2010. [Google Scholar]
- Wootton, R. Telemedicine: A cautious welcome. BMJ 1996, 313, 1375–1377. [Google Scholar] [CrossRef] [Green Version]
- Giansanti, D. Teleradiology Today: The Quality Concept and the Italian Point of View. Telemed. E-Health 2017, 23, 453–455. [Google Scholar] [CrossRef] [PubMed]
- Orlacchio, A.; Romeo, P.; Inserra, M.C.; Grigioni, M.; Giansanti, D. Guidelines for Quality Assurance and Technical Requirements in Teleradiology; English Translation and Revision of Rapporti ISTISAN 10/44, Rapporti ISTISAN 13/38; Istituto Superiore di Sanità: Roma, Italy, 2013; pp. 1–33. [Google Scholar]
- Ruotsalainen, P. Privacy and security in teleradiology. Eur. J. Radiol. 2010, 73, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Giansanti, D. Diagnostic Imaging and E-Health: Standardization, Experiences and New Opportunities; Rapporti ISTISAN 17/10; Istituto Superiore di Sanità: Roma, Italy, 2017; pp. 1–60. [Google Scholar]
- Giansanti, D. Diagnostics Imaging and M-Health: Investigations on the Prospects of Integration in Cytological and Organ Diagnostics; Rapporti ISTISAN 20/1; Istituto Superiore di Sanità: Roma, Italy, 2019; pp. 1–66. [Google Scholar]
- Canadian Association of Radiologists. CAR Standards for Teleradiology; Canadian Association of Radiologists: Ottawa, ON, Canada, 2008. [Google Scholar]
- American College of Radiology. ACR Standard for Teleradiology; ACR: Reston, VA, USA, 2002. [Google Scholar]
- Teleradiology. Merrian-Webster Medical Dictionary Online. Available online: www.merriamwebster.com/medical/teleradiology (accessed on 30 September 2013).
- Dicom, Digital Imaging and Communication in Medicine. Available online: https://www.dicomstandard.org/ (accessed on 9 January 2022).
- Giansanti, D. The Artificial Intelligence in Digital Pathology and Digital Radiology: Where Are We? Healthcare 2020, 9, 30. [Google Scholar] [CrossRef]
- Alsharif, M.H.; Alsharif, Y.H.; Yahya, K.; Alomari, O.A.; Albreem, M.A.; Jahid, A. Deep learning applications to combat the dissemination of COVID-19 disease: A review. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 11455–11460. [Google Scholar]
- Ozsahin, I.; Sekeroglu, B.; Musa, M.S.; Mustapha, M.T.; Uzun Ozsahin, D. Review on Diagnosis of COVID-19 from Chest CT Images Using Artificial Intelligence. Comput. Math. Methods Med. 2020, 2020, 9756518. [Google Scholar] [CrossRef]
- Pham, T.D. Classification of COVID-19 chest X-rays with deep learning: New models or fine tuning? Health Inf. Sci. Syst. 2020, 9, 2. [Google Scholar] [CrossRef]
- Liang, H.; Guo, Y.; Chen, X.; Ang, K.L.; He, Y.; Jiang, N.; Du, Q.; Zeng, Q.; Lu, L.; Gao, Z.; et al. Artificial intelligence for stepwise diagnosis and monitoring of COVID-19. Eur. Radiol. 2022, 1–11, Epub ahead of print. [Google Scholar] [CrossRef]
- Stevenson, A. Oxford Dictionary of English, 3rd ed.; Oxford University Press: Oxford, UK, 2010. [Google Scholar]
- Hsiang, C.W.; Lin, C.; Liu, W.C.; Lin, C.S.; Chang, W.C.; Hsu, H.H.; Huang, G.S.; Lou, Y.S.; Lee, C.C.; Wang, C.H.; et al. Detection of left ventricular systolic dysfunction using an artificial intelligence-enabled chest X-ray. Can. J. Cardiol. 2022. Epub ahead of print. [Google Scholar] [CrossRef]
- Tajik, A.J. Machine Learning for Echocardiographic imaging: Embarking on another incredible journey. J. Am. Coll. Cardiol. 2016, 68, 2296–2298. [Google Scholar] [CrossRef]
- Krittanawong, C.; Zhang, H.; Wang, Z.; Aydar, M.; Kitai, T. Artificial intelligence in precision cardiovascular medicine. J. Am. Coll. Cardiol. 2017, 69, 2657–2664. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Gajjala, S.; Agrawal, P.; Tison, G.H.; Hallock, L.A.; Beussink-Nelson, L.; Deo, R.C. Fully automated echocardiogram interpretation in clinical practice. Circulation 2018, 138, 1623–1635. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Ruiz, A.; Lång, K.; Gubern-Merida, A.; Broeders, M.; Gennaro, G.; Clauser, P.; Helbich, T.H.; Chevalier, M.; Tan, T.; Mertelmeier, T.; et al. Stand-Alone Artificial Intelligence for Breast Cancer Detection in Mammography: Comparison With 101 Radiologists. J. Natl. Cancer Inst. 2019, 111, 916–922. [Google Scholar] [CrossRef] [PubMed]
- Bertini, F.; Allevi, D.; Lutero, G.; Montesi, D.; Calzà, L. Automatic Speech Classifier for Mild Cognitive Impairment and Early Dementia. ACM Trans. Comput. Healthc. 2022, 3, 1–11. [Google Scholar] [CrossRef]
- Mak, K.K.; Pichika, M.R. Artificial intelligence in drug development: Present status and future prospects. Drug Discov. Today 2019, 24, 773–780. [Google Scholar] [CrossRef]
- Jalal, S.; Nicolaou, S.; Parker, W. Artificial Intelligence, Radiology, and the Way Forward. Can. Assoc. Radiol. J. 2019, 70, 10–12. [Google Scholar] [CrossRef] [Green Version]
- European Society of Radiology (ESR). What the radiologist should know about artificial intelligence—An ESR white paper. Insights Imaging 2019, 10, 44. [Google Scholar] [CrossRef] [Green Version]
- Regulation (EU) 2017/745 of the European Parliament and of the Council of 5 April 2017 on Medical Devices, Amending Directive 2001/83/EC, Regulation (EC) No 178/2002 and Regulation (EC) No 1223/2009 and Repealing Council Directives 90/385/EEC and 93/42/EEC.2017. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/HTML/?uri=CELEX:32017R0745&from=IT (accessed on 25 November 2021).
- Giansanti, D. Cybersecurity and the Digital-Health: The Challenge of This Millennium. Healthcare 2021, 9, 62. [Google Scholar] [CrossRef]
- Evidence-Based Medicine Guidelines. Available online: https://www.ebm-guidelines.com/dtk/ebmg/home (accessed on 9 January 2022).
- Luce, B.R.; Drummond, M.; Jönsson, B.; Neumann, P.J.; Schwartz, J.S.; Siebert, U.; Sullivan, S.D. EBM, HTA, and CER: Clearing the confusion. Milbank Q. 2010, 88, 256–276. [Google Scholar] [CrossRef] [Green Version]
- McGlynn, E.A.; Kosecoff, J.; Brook, R.H. Format and conduct of consensus development conferences. Multi-nation comparison. Int. J. Technol. Assess. Health Care 1990, 6, 450–469. [Google Scholar] [CrossRef]
- Eddy, D.M. Evidence-Based Medicine: A Unified Approach. Health Affairs 2005, 24, 9–17. [Google Scholar] [CrossRef] [PubMed]
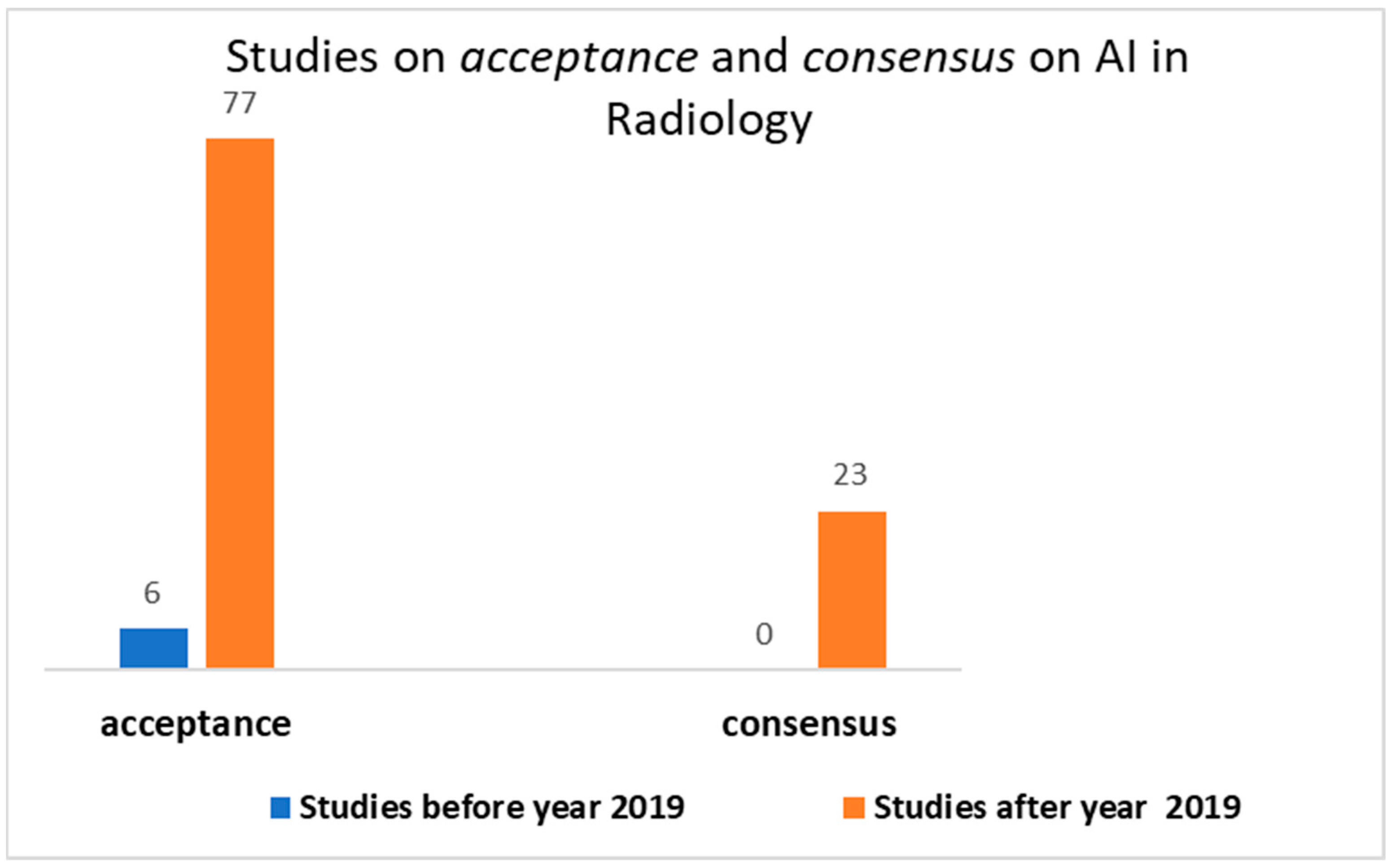
- National Library of Medicine. Available online: https://pubmed.ncbi.nlm.nih.gov/?term=%28acceptance%29+AND+%28artificial+intelligence%5BTitle%2FAbstract%5D%29+AND+Radiology&sort=date&size=200 (accessed on 9 January 2022).
- National Library of Medicine. Available online: https://pubmed.ncbi.nlm.nih.gov/?term=%28%28consensus%29+AND+%28artificial+intelligence%5BTitle%2FAbstract%5D%29%29+AND+%28radiology%5BTitle%2FAbstract%5D%29&sort=date&size=200 (accessed on 9 January 2022).
- Lennartz, S.; Dratsch, T.; Zopfs, D.; Persigehl, T.; Maintz, D.; Hokamp, N.G.; Dos Santos, D.P. Use and Control of Artificial Intelligence in Patients Across the Medical Workflow: Single-Center Questionnaire Study of Patient Perspectives. J. Med. Internet Res. 2021, 23, e24221. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Citardi, D.; Wang, D.; Genc, Y.; Shan, J.; Fan, X. Patients’ perceptions of using artificial intelligence (AI)-based technology to comprehend radiology imaging data. Health Inform. J. 2021, 27, 14604582211011215. [Google Scholar] [CrossRef]
- Ongena, Y.P.; Haan, M.; Yakar, D.; Kwee, T.C. Patients’ views on the implementation of artificial intelligence in radiology: Development and validation of a standardized questionnaire. Eur. Radiol. 2020, 30, 1033–1040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hendrix, N.; Hauber, B.; Lee, C.I.; Bansal, A.; Veenstra, D.L. Artificial intelligence in breast cancer screening: Primary care provider preferences. J. Am. Med. Inform. Assoc. 2021, 28, 1117–1124. [Google Scholar] [CrossRef]
- Abuzaid, M.M.; Elshami, W.; McConnell, J.; Tekin, H.O. An extensive survey on radiographers from the Middle East and India on artificial intelligence integration in radiology practice. Health Technol. 2021, 11, 1045–1050. [Google Scholar] [CrossRef]
- Abuzaid, M.M.; Tekin, H.O.; Reza, M.; Elhag, I.R.; Elshami, W. Assessment of MRI technologists in acceptance and willingness to integrate artificial intelligence into practice. Radiography 2021, 27, S83–S87. [Google Scholar] [CrossRef]
- Giansanti, D.; Rossi, I.; Monoscalco, L. Lessons from the COVID-19 Pandemic on the Use of Artificial Intelligence in Digital Radiology: The Submission of a Survey to Investigate the Opinion of Insiders. Healthcare 2021, 9, 331. [Google Scholar] [CrossRef] [PubMed]
- Abuzaid, M.M.; Elshami, W.; Tekin, H.; Issa, B. Assessment of the Willingness of Radiologists and Radiographers to Accept the Integration of Artificial Intelligence into Radiology Practice. Acad. Radiol. 2020, 29, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Alelyani, M.; Alamri, S.; Alqahtani, M.S.; Musa, A.; Almater, H.; Alqahtani, N.; Alshahrani, F.; Alelyani, S. Radiology Community Attitude in Saudi Arabia about the Applications of Artificial Intelligence in Radiology. Healthcare 2021, 9, 834. [Google Scholar] [CrossRef] [PubMed]
- European Society of Radiology (ESR). Impact of artificial intelligence on radiology: A EuroAIM survey among members of the European Society of Radiology. Insights Imaging 2019, 10, 105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galán, G.C.; Portero, F.S. Medical students’ perceptions of the impact of artificial intelligence in Radiology. Radiologia 2021, in press. [Google Scholar] [CrossRef]
- Aldosari, B. User acceptance of a picture archiving and communication system (PACS) in a Saudi Arabian hospital radiology department. BMC Med. Inform. Decis. Mak. 2012, 12, 44. [Google Scholar] [CrossRef] [Green Version]
- Moss, R.J.; Süle, A.; Kohl, S. eHealth and mHealth. Eur. J. Hosp. Pharm. 2019, 26, 57–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shan, H.; Padole, A.; Homayounieh, F.; Kruger, U.; Khera, R.D.; Nitiwarangkul, C.; Kalra, M.K.; Wang, G. Competitive performance of a modularized deep neural network compared to commercial algorithms for low-dose CT image reconstruction. Nat. Mach. Intell. 2019, 1, 269–276. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Altman, D.G.; Schulz, K.F.; Simera, I.; Wager, E. (Eds.) Guidelines for Reporting Health Research: A User’s Manual. Available online: https://0-onlinelibrary-wiley-com.brum.beds.ac.uk/doi/abs/10.1002/9781118715598.ch20 (accessed on 9 January 2022).
- Ministero Della Salute Rivede Elenco Società Scientifiche per Stesura Linee Guida. 41 Società in Più. Available online: http://www.aiponet.it/news/104-ufficio-stampa/2149-ministero-della-salute-rivede-elenco-societa-scientifiche-per-stesura-linee-guida-41-societa-in-piu.html (accessed on 9 January 2022).
- Federazione Delle Società Medico-Scientifiche Italiane. Available online: https://portale.fism.it/ (accessed on 9 January 2022).
- Federazione Delle Associazioni Scientifiche dei Tecnici di Radiologia. Available online: https://www.associazionefaster.org/ (accessed on 9 January 2022).
- Federazione Delle Associazioni Scientifiche e Tecniche. Available online: https://fast.mi.it/chi-siamo/ (accessed on 9 January 2022).
- Thomassin-Naggara, I.; Balleyguier, C.; Ceugnart, L.; Heid, P.; Lenczner, G.; Maire, A.; Séradour, B.; Verzaux, L.; Taourel, P. Conseil National Professionnel de la Radiologie et Imagerie Médicale (G4). Artificial intelligence and breast screening: French Radiology Community position paper. Diagn. Interv. Imaging 2019, 100, 553–566. [Google Scholar] [CrossRef]
- Avanzo, M.; Trianni, A.; Botta, F.; Talamonti, C.; Stasi, M.; Iori, M. Artificial Intelligence and the Medical Physicist: Welcome to the Machine. Appl. Sci. 2021, 11, 1691. [Google Scholar] [CrossRef]
- Coppola, F.; Faggioni, L.; Regge, D.; Giovagnoni, A.; Golfieri, R.; Bibbolino, C.; Miele, V.; Neri, E.; Grassi, R. Artificial intelligence: Radiologists’ expectations and opinions gleaned from a nationwide online survey. Radiol. Med. 2021, 126, 63–71. [Google Scholar] [CrossRef]
- Diaz, O.; Guidi, G.; Ivashchenko, O.; Colgan, N.; Zanca, F. Artificial intelligence in the medical physics community: An international survey. Phys. Med. 2021, 81, 141–146. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participants | Participants Agreeing to Continue/Passing the Requirement | Males/Females | Min Age/Max Age | Mean Age | |
|---|---|---|---|---|---|
| MSs | 111 | 108/92 | 48/44 | 32/43 | 37.9 |
| MPs | 105 | 97/91 | 43/48 | 31/41 | 36.1 |
| SASs | 99 | 93/90 | 47/43 | 33/40 | 37.3 |
| Knowledge | MSs Score | MPs Score | SASs Score | ANOVA p |
|---|---|---|---|---|
| AI (general) | 4.56 | 4.38 | 4.51 | p > 0.1 |
| AI (informatics) | 4.33 | 4.24 | 5.22 | p < 0.01 |
| AI (medical imaging) | 4.98 | 5.07 | 5.02 | p > 0.1 |
| Technologies for biomedical Apps | 4.32 | 5.03 | 5.11 | p < 0.01 |
| Application of AI in: | MSs Score | MPs Score | SASs Score | ANOVA p |
|---|---|---|---|---|
| 4.26 | 4.18 | 4.11 | p > 0.1 | |
| Interventional radiology | 4.54 | 4.39 | 4.41 | p > 0.1 |
| Diagnostic radiology (radiology, CT, etc.) | 4.26 | 4.28 | 4.31 | p > 0.1 |
| Nuclear magnetic resonance | 4.61 | 4.69 | 4.72 | p > 0.1 |
| Positron emission tomography | 4.53 | 4.38 | 4.52 | p > 0.1 |
| Gamma chamber | 4.44 | 4.39 | 4.43 | p > 0.1 |
| Application of AI (Non Imaging) | MSs Score | MPs Score | SASs Score | ANOVA p |
|---|---|---|---|---|
| Risk assessment | 4.82 | 4.21 | 4.13 | p < 0.01 |
| Therapy | 5.21 | 4.65 | 4.52 | p < 0.01 |
| Prevention | 5.11 | 4.02 | 4.11 | p < 0.01 |
| Quality Control | 4.12 | 5.07 | 5.12 | p < 0.01 |
| Scheme | MSs Score | MPs Score | SASs Score | ANOVA p |
|---|---|---|---|---|
| eHealth | 4.72 | 4.66 | 3.93 | p < 0.01 |
| mHealth | 4.55 | 4.62 | 3.89 | p < 0.01 |
| Both eHealth and mHealth | 4.58 | 4.62 | 3.86 | p < 0.01 |
| Standalone | 5.33 | 5,24 | 5.17 | p > 0.1 |
| Optimism | MSs Score | MPs Score | SASs Score | ANOVA p |
|---|---|---|---|---|
| AI (All) | 4.58 | 4.57 | 4.53 | p > 0.1 |
| AI (people dealing with AI in the workplace) | 4.98 | 4.96 | 4.93 | p > 0.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Basilio, F.; Esposisto, G.; Monoscalco, L.; Giansanti, D. The Artificial Intelligence in Digital Radiology: Part 2: Towards an Investigation of acceptance and consensus on the Insiders. Healthcare 2022, 10, 153. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10010153
Di Basilio F, Esposisto G, Monoscalco L, Giansanti D. The Artificial Intelligence in Digital Radiology: Part 2: Towards an Investigation of acceptance and consensus on the Insiders. Healthcare. 2022; 10(1):153. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10010153
Chicago/Turabian StyleDi Basilio, Francesco, Gianluca Esposisto, Lisa Monoscalco, and Daniele Giansanti. 2022. "The Artificial Intelligence in Digital Radiology: Part 2: Towards an Investigation of acceptance and consensus on the Insiders" Healthcare 10, no. 1: 153. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10010153