
A Noninvasive Risk Stratification Tool Build Using an Artificial Intelligence Approach for Colorectal Polyps Based on Annual Checkup Data

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Colonoscopy Procedure and Abdominal Ultrasonography
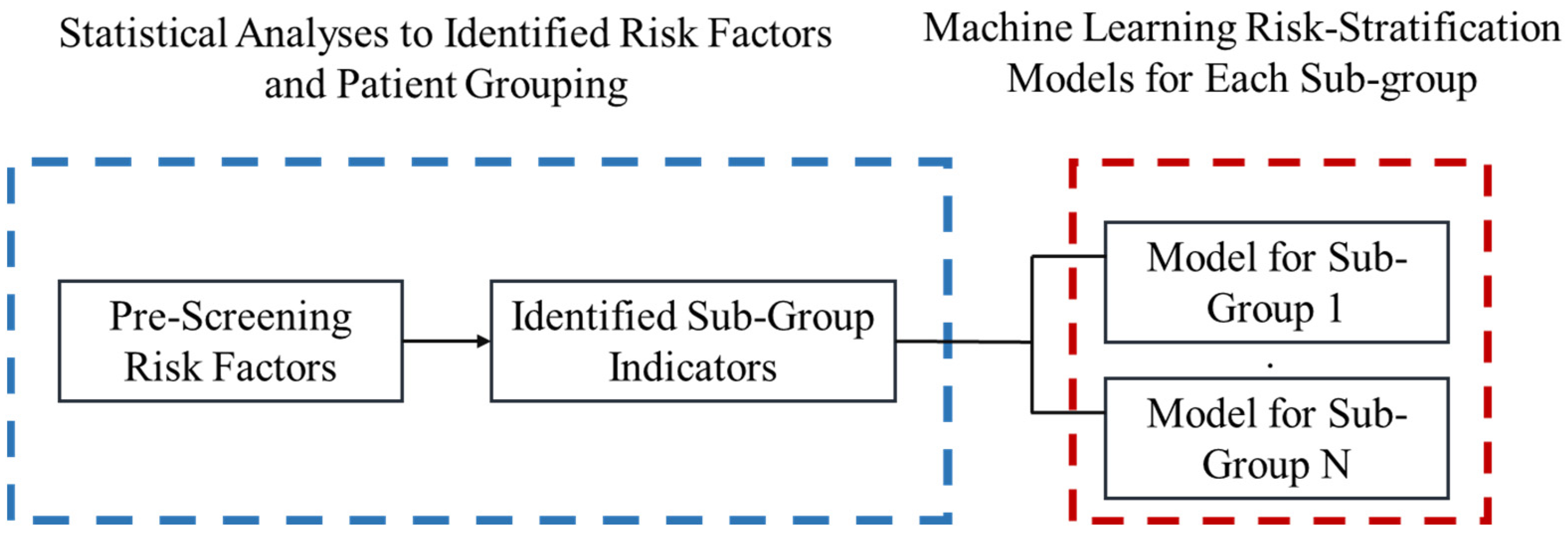
2.3. Risk Stratification Tool Building
- Step 1:
- Collect data from annual health check-ups. All risk factors are indexed from i = 1…N, the value of the risk factor is xi, where there are N risk factors in total.
- Step 2:
- Pre-screen with a z-test for two sample proportions with a significance level equal to 0.05 is applied to select potential risk factors. Where the two sample proportions are calculated asFor all risk factor i,
- phi = the proportion of patients who has colorectal polyps for patients with risk factor xi = h − 1.
That is,- p1i = the proportion of patients who has colorectal polyps for patients with risk factor xi = 0.
- p2i = the proportion of patients who has colorectal polyps for patients with risk factor xi = 1.
- Step 3:
- The null and alternative hypothesis is stated as below:Null Hypothesis: p1i = p2i = …. phi
- We record all risk factors which has a significantly different sample proportion between patients with and without colorectal polyps.
- Step 4:
- Logistics regression is applied for each risk factor to calculate the discriminability for each risk factor. Based on the logistic regression, we identified the demographic risk factors which can segregate patients into different sub-groups for the machine learning process.
- Step 5:
- Machine learning is applied to each sub-group to construct the risk stratification tool.
- Step 6:
- We output the system of models which consisted of multiple random forest models.
- Step 7:
- Output our four-fold-cross validation.
2.4. Statistical Analyses
2.5. Machine Learning Algorithm
- Step 1:
- Input all risk factors as vector X = <x1……xh> and the y = 1 if a patient is diagnosed with colorectal polyps, and zero otherwise. Moreover, input the demographic factors for aggregating patients into subgroups. Go to Step 2.
- Step 2:
- Segregate all patients into subgroups. Index subgroups as k = 1…N for N groups in total. Let k =1 and go to Step 3.
- Step 3:
- Input all risk factors X and y in the kth sub-group. Go to Step 4.
- Step 4:
- Input all data in with path_name = group k, with the following specification of random foreackage in python. We selected the four-fold validation, thus 75% of data will be randomly selected for modeling building and 25% will be reserved for validation. For each run, the random forest will repeat four times for validation. Output the model and go to Step 5.Branch criterion: gini indexNumber of estimators (number of decision trees): 1000Min_samples_leaf = 5Class weight: balancedValidation: Four-foldCalculate the following statistics:Specificity = True negative/(true negative + false positive)Sensitivity = True positive/(true positive + false negative)Area Under Curve (AUC)
- Step 5:
- Collected the outputted model and check if k = N, if not let k = k + 1 and go to Step 3, otherwise end the algorithm.
3. Results
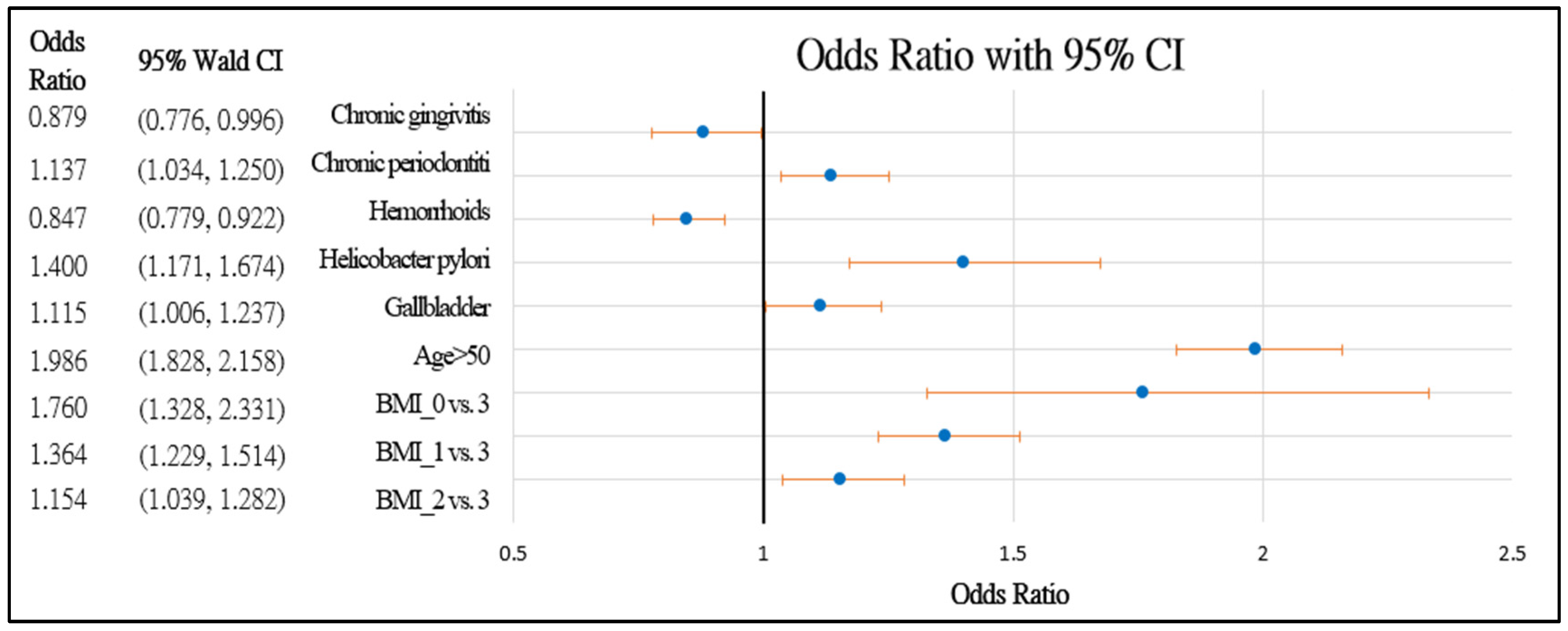
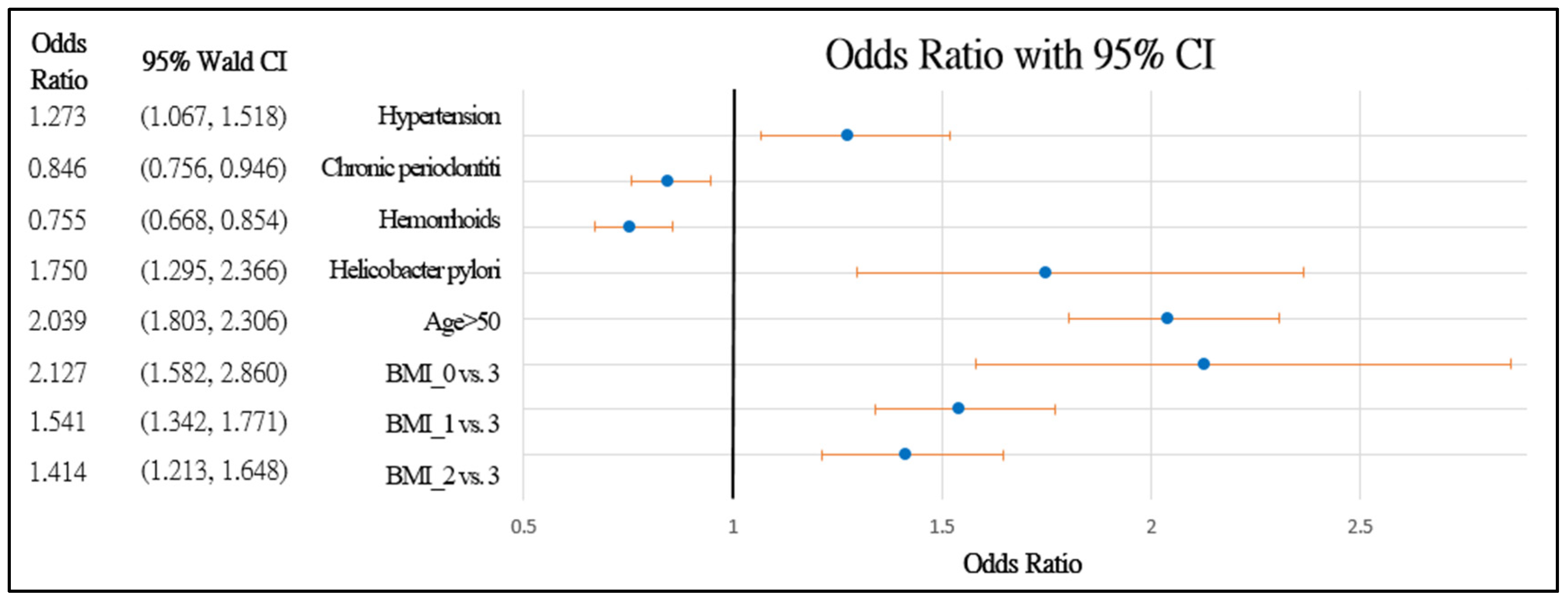
3.1. Statistical Analysis
3.2. Noninvasive Diagnostics Tool with Random Forests
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer Incidence and Mortality Worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Calderwood, A.H.; Lasser, K.E.; Roy, H.K. Colon adenoma features and their impact on risk of future advanced adenomas and colorectal cancer. World J. Gastrointest. Oncol. 2016, 8, 826–834. [Google Scholar] [CrossRef] [PubMed]
- Schmitz, J.M.; Stolte, M. Gastric Polyps as Precancerous Lesions. Gastrointest. Endosc. Clin. N. Am. 1997, 7, 29–46. [Google Scholar] [CrossRef]
- Zheng, E.; Ni, S.; Yu, Y.; Wang, Y.; Weng, X.; Zheng, L. Impact of gender and age on the occurrence of gastric polyps: Data analysis of 69575 southeastern Chinese patients. Turk. J. Gastroenterol. 2015, 26, 474–479. [Google Scholar] [CrossRef]
- Islam, R.S.; Patel, N.C.; Lam-Himlin, D.; Nguyen, C.C. Gastric Polyps: A Review of Clinical, Endoscopic, and Histopathologic Features and Management Decisions. Gastroenterol. Hepatol. 2013, 9, 640–651. [Google Scholar]
- Citarda, F.; Tomaselli, G.; Capocaccia, R.; Barcherini, S.; Crespi, M. The Italian Multicentre Study Group Efficacy in standard clinical practice of colonoscopic polypectomy in reducing colorectal cancer incidence. Gut 2001, 48, 812–815. [Google Scholar] [CrossRef] [Green Version]
- Carmack, S.W.; Genta, R.M.; Graham, D.Y.; Lauwers, G.Y. Management of gastric polyps: A pathology-based guide for gastroenterologists. Nat. Rev. Gastroenterol. Hepatol. 2009, 6, 331–341. [Google Scholar] [CrossRef]
- Kim, S.Y.; Kim, H.-S.; Park, H.J. Adverse events related to colonoscopy: Global trends and future challenges. World J. Gastroenterol. 2019, 25, 190–204. [Google Scholar] [CrossRef]
- Greenspan, M.; Prickett, E.; Melson, J. High Clinical Patient Workload Leads to Increased Premature Adenomatous Polyp Surveillance Colonoscopy. Am. J. Gastroenterol. 2015, 110, S601. [Google Scholar] [CrossRef]
- Almadi, M.; Sewitch, M.; Barkun, A.N.; Martel, M.; Joseph, L. Adenoma Detection Rates Decline with Increasing Procedural Hours in an Endoscopist’s Workload. Can. J. Gastroenterol. Hepatol. 2015, 29, 304–308. [Google Scholar] [CrossRef]
- Sey, M.S.L.; Gregor, J.; Adams, P.; Khanna, N.; Vinden, C.; Driman, D.; Chande, N. Wait Times for Diagnostic Colonoscopy among Outpatients with Colorectal Cancer: A Comparison with Canadian Association of Gastroenterology Targets. Can. J. Gastroenterol. 2012, 26, 894–896. [Google Scholar] [CrossRef] [Green Version]
- Cappell, M.S. The pathophysiology, clinical presentation, and diagnosis of colon cancer and adenomatous polyps. Med Clin. N. Am. 2005, 89, 1–42. [Google Scholar] [CrossRef]
- Ren, H.G.; Luu, H.N.; Cai, H.; Xiang, Y.B.; Steinwandel, M.; Gao, Y.T.; Hargreaves, M.; Zheng, W.; Blot, W.J.; Long, J.R.; et al. Oral health and risk of colorectal cancer: Results from three cohort studies and a meta-analysis. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2016, 27, 1329–1336. [Google Scholar] [CrossRef]
- Momen-Heravi, F.; Babic, A.; Tworoger, S.S.; Zhang, L.; Wu, K.; Smith-Warner, S.A.; Ogino, S.; Chan, A.T.; Meyerhardt, J.; Giovannucci, E.; et al. Periodontal disease, tooth loss and colorectal cancer risk: Results from the Nurses’ Health Study. Int. J. Cancer 2017, 140, 646–652. [Google Scholar] [CrossRef]
- Brim, H.; Zahaf, M.; Laiyemo, A.O.; Nouraie, M.; Pérez-Pérez, G.I.; Smoot, D.T.; Lee, E.; Razjouyan, H.; Ashktorab, H. Gastric Helicobacter pylori infection associates with an increased risk of colorectal polyps in African Americans. BMC Cancer 2014, 14, 296. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.L.; Wu, J.S.; Yang, Y.C.; Lu, F.H.; Lee, C.T.; Lin, W.J.; Chang, C.J. Gallbladder stones and gallbladder polyps associated with increased risk of colorectal adenoma in men. J. Gastroenterol. Hepatol. 2018, 33, 800–806. [Google Scholar] [CrossRef]
- Xiao, S.; Zhou, L. Gastric cancer: Metabolic and metabolomics perspectives (Review). Int. J. Oncol. 2017, 51, 5–17. [Google Scholar] [CrossRef] [Green Version]
- Ford, I.; Robertson, M.; Komajda, M.; Böhm, M.; Borer, J.S.; Tavazzi, L.; Swedberg, K. Top ten risk factors for morbidity and mortality in patients with chronic systolic heart failure and elevated heart rate: The SHIFT Risk Model. Int. J. Cardiol. 2015, 184, 163–169. [Google Scholar] [CrossRef] [Green Version]
- Okada, H.; Fukui, M.; Tanaka, M.; Matsumoto, S.; Mineoka, Y.; Nakanishi, N.; Asano, M.; Yamazaki, M.; Hasegawa, G.; Nakamura, N. Visit-to-Visit Blood Pressure Variability Is a Novel Risk Factor for the Development and Progression of Diabetic Nephropathy in Patients with Type 2 Diabetes. Diabetes Care 2013, 36, 1908–1912. [Google Scholar] [CrossRef] [Green Version]
- Khalilia, M.; Chakraborty, S.; Popescu, M. Predicting disease risks from highly imbalanced data using random forest. BMC Med Inform. Decis. Mak. 2011, 11, 51. [Google Scholar] [CrossRef] [Green Version]
- Graham, D.Y.; Miftahussurur, M. Helicobacter pylori urease for diagnosis of Helicobacter pylori infection: A mini review. J. Adv. Res. 2018, 13, 51–57. [Google Scholar] [CrossRef]
- Andren-Sandberg, A. Diagnosis and management of gallbladder polyps. N. Am. J. Med. Sci. 2012, 4, 203–211. [Google Scholar] [CrossRef] [Green Version]
- Abdulqader, D.M.; Abdulazeez, A.M.; Zeebaree, D.Q. Machine learning supervised algorithms of gene selection: A review. Mach. Learn. 2020, 62, 233–244. [Google Scholar]
- Goldman, O.; Ben-Assuli, O.; Rogowski, O.; Zeltser, D.; Shapira, I.; Berliner, S.; Zelber-Sagi, S.; Shenhar-Tsarfaty, S. Non-alcoholic Fatty Liver and Liver Fibrosis Predictive Analytics: Risk Prediction and Machine Learning Techniques for Improved Preventive Medicine. J. Med. Syst. 2021, 45, 22. [Google Scholar] [CrossRef]
- Fialoke, S.; Malarstig, A.; Miller, M.R.; Dumitriu, A. Application of Machine Learning Methods to Predict Non-Alcoholic Steatohepatitis (NASH) in Non-Alcoholic Fatty Liver (NAFL) Patients. AMIA Annu. Symp. Proc. 2018, 2018, 430–439. [Google Scholar]
- Wan, Y.; Yuan, J.; Li, J.; Li, H.; Yin, K.; Wang, F.; Li, D. Overweight and underweight status are linked to specific gut microbiota and intestinal tricarboxylic acid cycle intermediates. Clin. Nutr. 2020, 39, 3189–3198. [Google Scholar] [CrossRef]
- Jain, R.; Pickens, C.A.; Fenton, J.I. The role of the lipidome in obesity-mediated colon cancer risk. J. Nutr. Biochem. 2018, 59, 1–9. [Google Scholar] [CrossRef]
- Cao, W.; Hou, G.; Zhang, X.; San, H.; Zheng, J. Potential risk factors related to the development of gastric polyps. Immunopharmacol. Immunotoxicol. 2018, 40, 338–343. [Google Scholar] [CrossRef]
- Chen, H.; Li, N.; Ren, J.; Feng, X.; Lyu, Z.; Wei, L.; Li, X.; Guo, L.; Zheng, Z.; Zou, S.; et al. Participation and yield of a population-based colorectal cancer screening programme in China. Gut 2018, 68, 1450–1457. [Google Scholar] [CrossRef] [PubMed]
- Hussein Kamareddine, M.; Ghosn, Y.; Karam, K.; Nader, A.A.; El-Mahmoud, A.; Bou-Ayash, N.; El-Khoury, M.; Farhat, S. Adenoma Detection before and after the age of 50: A retrospective analysis of Lebanese outpatients. BMJ Open Gastroenterol. 2018, 5, 000253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolf, A.M.D.; Fontham, E.T.H.; Church, T.R.; Flowers, C.R.; Guerra, C.E.; LaMonte, S.J.; Etzioni, R.; McKenna, M.T.; Oeffinger, K.C.; Shih, Y.-C.T.; et al. Colorectal cancer screening for average-risk adults: 2018 guideline update from the American Cancer Society. CA Cancer J. Clin. 2018, 68, 250–281. [Google Scholar] [CrossRef] [PubMed]
- Schreuders, E.H.; Ruco, A.; Rabeneck, L.; Schoen, R.E.; Sung, J.J.Y.; Young, G.; Kuipers, E.J. Colorectal cancer screening: A global overview of existing programmes. Gut 2015, 64, 1637–1649. [Google Scholar] [CrossRef] [PubMed]
- Bevan, R.; Rutter, M.D. Colorectal Cancer Screening-Who, How, and When? Clin. Endosc. 2018, 51, 37–49. [Google Scholar] [CrossRef] [Green Version]
- Kang, K.H.; Hwang, S.H.; Kim, N.; Kim, D.-H.; Kim, S.Y.; Hyun, J.J.; Jung, S.W.; Koo, J.S.; Jung, Y.K.; Yim, H.J.; et al. The Effect of Helicobacter pylori Infection on Recurrence of Gastric Hyperplastic Polyp after Endoscopic Removal. Korean J. Gastroenterol. 2018, 71, 213–218. [Google Scholar] [CrossRef] [Green Version]
- Anjiki, H.; Mukaisho, K.-I.; Kadomoto, Y.; Doi, H.; Yoshikawa, K.; Nakayama, T.; Vo, D.T.-N.; Hattori, T.; Sugihara, H. Adenocarcinoma arising in multiple hyperplastic polyps in a patient with Helicobacter pylori infection and hypergastrinemia during long-term proton pump inhibitor therapy. Clin. J. Gastroenterol. 2017, 10, 128–136. [Google Scholar] [CrossRef]
- Markowski, A.R.; Markowska, A.; Guzinska-Ustymowicz, K. Pathophysiological and clinical aspects of gastric hyperplastic polyps. World J. Gastroenterol. 2016, 22, 8883–8891. [Google Scholar] [CrossRef]
- Togo, K.; Ueo, T.; Yonemasu, H.; Honda, H.; Ishida, T.; Tanabe, H.; Yao, K.; Iwashita, A.; Murakami, K. Two cases of adenocarcinoma occurring in sporadic fundic gland polyps observed by magnifying endoscopy with narrow band imaging. World J. Gastroenterol. 2016, 22, 9028–9034. [Google Scholar] [CrossRef]
- Tongtawee, T.; Simawaranon, T.; Wattanawongdon, W. Role of screening colonoscopy for colorectal tumors in Helicobacter pylori-related chronic gastritis with MDM2 SNP309 G/G homozygous: A prospective cross-sectional study in Thailand. Turk. J. Gastroenterol. 2018, 29, 555–560. [Google Scholar] [CrossRef]
- Kumar, A.; Kim, M.; Lukin, D.J. Helicobacter pylori is associated with increased risk of serrated colonic polyps: Analysis of serrated polyp risk factors. Indian J. Gastroenterol. 2018, 37, 235–242. [Google Scholar] [CrossRef]
- Nam, J.H.; Hong, C.W.; Kim, B.C.; Shin, A.; Ryu, K.H.; Park, B.J.; Kim, B.; Sohn, D.K.; Han, K.S.; Kim, J.; et al. Helicobacter pylori infection is an independent risk factor for colonic adenomatous neoplasms. Cancer Causes Control. 2017, 28, 107–115. [Google Scholar] [CrossRef]
- Meira, L.B.; Bugni, J.M.; Green, S.L.; Lee, C.-W.; Pang, B.; Borenshtein, D.; Rickman, B.H.; Rogers, A.B.; Moroski-Erkul, C.A.; McFaline, J.L.; et al. DNA damage induced by chronic inflammation contributes to colon carcinogenesis in mice. J. Clin. Investig. 2008, 118, 2516–2525. [Google Scholar] [CrossRef] [Green Version]
- Thorburn, C.M.; Friedman, G.D.; Dickinson, C.J.; Vogelman, J.H.; Orentreich, N.; Parsonnet, J. Gastrin and colorectal cancer: A prospective study. Gastroenterology 1998, 115, 275–280. [Google Scholar] [CrossRef]
- Georgopoulos, S.D.; Polymeros, D.; Triantafyllou, K.; Spiliadi, C.; Mentis, A.; Karamanolis, D.G.; Ladas, S.D. Hypergastrinemia Is Associated with Increased Risk of Distal Colon Adenomas. Digestion 2006, 74, 42–46. [Google Scholar] [CrossRef]
- Epplein, M.; Pawlita, M.; Michel, A.; Peek, R.M.; Cai, Q.; Blot, W.J. Helicobacter pylori Protein–Specific Antibodies and Risk of Colorectal Cancer. Cancer Epidemiol. Biomark. Prev. 2013, 22, 1964–1974. [Google Scholar] [CrossRef] [Green Version]
- Shmuely, H.; Passaro, D.; Figer, A.; Niv, Y.; Pitlik, S.; Samra, Z.; Koren, R.; Yahav, J. Relationship between Helicobacter pylori CagA status and colorectal cancer. Am. J. Gastroenterol. 2001, 96, 3406–3410. [Google Scholar] [CrossRef]
- Grundy, S.M.; Brewer, H.B.; Cleeman, J.I., Jr.; Smith, S.C., Jr.; Lenfant, C. Definition of metabolic syndrome: Report of the National Heart, Lung, and Blood Institute/American Heart Association conference on scientific issues related to definition. Circulation 2004, 109, 433–438. [Google Scholar] [CrossRef] [Green Version]
- Park, W.; Lee, H.; Kim, E.H.; Yoon, J.Y.; Park, J.C.; Shin, S.K.; Kil Lee, S.; Lee, Y.C.; Kim, W.H.; Noh, S.H. Metabolic syndrome is an independent risk factor for synchronous colorectal neoplasm in patients with gastric neoplasm. J. Gastroenterol. Hepatol. 2012, 27, 1490–1497. [Google Scholar] [CrossRef]
- Chou, S.H.; Tung, Y.C.; Wu, L.S.; Chang, C.J.; Kung, S.; Chu, P.H. Severity of chronic periodontitis and risk of gastrointestinal cancers: A population-based follow-up study from Taiwan. Medicine 2018, 97, e11386. [Google Scholar] [CrossRef]
- Lauritano, D.; Sbordone, L.; Nardone, M.; Iapichino, A.; Scapoli, L.; Carinci, F. Focus on periodontal disease and colorectal carcinoma. Oral Implant. 2017, 10, 229–233. [Google Scholar] [CrossRef]
- Gao, Z.; Guo, B.; Gao, R.; Zhu, Q.; Qin, H. Microbiota disbiosis is associated with colorectal cancer. Front. Microbiol. 2015, 6, 20. [Google Scholar] [CrossRef] [PubMed]
- Moutsopoulos, N.M.; Madianos, P.N. Low-Grade Inflammation in Chronic Infectious Diseases: Paradigm of Periodontal Infections. Ann. N. Y. Acad. Sci. 2006, 1088, 251–264. [Google Scholar] [CrossRef] [PubMed]
- Stergios, K.; Damaskos, C.; Frountzas, M.; Nikiteas, N.; Lalude, O. Can gallbladder polyps predict colorectal adenoma or even neoplasia? A systematic review. Int. J. Surg. 2016, 33, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.H.; Kim, D.H.; Park, M.J.; Kim, Y.S.; Kim, C.H.; Yim, J.Y.; Cho, K.R.; Kim, S.S.; Choi, S.H.; Kim, N.; et al. Is Metabolic Syndrome One of the Risk Factors for Gallbladder Polyps Found by Ultrasonography during Health Screening? Gut Liver 2007, 1, 138–144. [Google Scholar] [CrossRef]
- Tanwar, S.; Vijayalakshmi, S. Comparative Analysis and Proposal of Deep Learning Based Colorectal Cancer Polyps Classification Technique. J. Comput. Theor. Nanosci. 2020, 17, 2354–2362. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total Number | n, % | 20,129 |
|---|---|---|
| Gender | Ratio of male to female (n/n) | 11,570:8559 |
| Polyp | ||
| Colorectal polyp (n, %) | 5450, 27.08% | |
| Gallbladder polyps (n, %) | 2188, 10.87% | |
| Gallbladder stone (n, %) | 1106, 5.49% | |
| Gallbladder problem | 3191, 15.85% | |
| Hypertension | (n, %) | 1684, 8.37% |
| Helicobacter pylori infection | (n, %) | 751, 3.73% |
| Tooth disease | 15,346, 76.24% | |
| Periodontal disease (n, %) | 8917, 44.30% | |
| Chronic gingivitis (n, %) | 4168, 20.71% | |
| Chronic periodontitis (n, %) | 11,655, 57.90% | |
| BMI | ||
| Underweight (n, %) | 805, 4% | |
| Normal (n, %) | 9090, 45.16% | |
| Overweight (n, %) | 6046, 30.04% | |
| Obesity (n, %) | 4188, 20.81% | |
| Age | Median (range) | 50 (18–96) years |
| Total cholesterol | 2818, 14% | |
| HDL | 2617, 13% | |
| Triglycerides | 3452, 17% |
| Regardless of Gender | Male | Female | |||||
|---|---|---|---|---|---|---|---|
| Parameters | p-Value | AUC | p-Value | AUC | p-Value | AUC | |
| Age | (>50 years = 1) | <0.0001 | 0.5847 | <0.0001 | 0.5906 | <0.0001 | 0.5900 |
| Helicobacter pylori | (Yes = 1) | <0.0001 | 0.5113 | <0.0001 | 0.5104 | <0.0001 | 0.5092 |
| Hypertension | (Yes = 1) | <0.0001 | 0.5142 | 0.0029 | 0.5084 | <0.0001 | 0.5240 |
| Tooth disease | Total | 0.3734 | 0.503 | 0.0053 | 0.5118 | 0.1041 | 0.5086 |
| Gallbladder | (Yes = 1) | <0.0001 | 0.514 | 0.002 | 0.5119 | 0.0185 | 0.5105 |
| BMI | |||||||
| Underweight = 0 | <0.0001 | 0.5604 | 0.0012 | 0.5389 | <0.0001 | 0.5709 | |
| Normal = 1 | 0.0055 | 0.1301 | 0.0341 | ||||
| Overweight = 2 | <0.0001 | 0.0017 | 0.008 | ||||
| Obesity = 3 | |||||||
| Gender | Age | BMI | Sensitivity | Specificity | AUC |
|---|---|---|---|---|---|
| Female | <50 years old | Normal | 0.22 | 0.74 | 0.61 |
| Overweight | 0.09 | 0.83 | 0.76 | ||
| Obese | 0.14 | 0.79 | 0.91 | ||
| Underweight | 0.55 | 0.50 | 0.66 | ||
| ≥50 years old | Normal | 0.35 | 0.66 | 0.68 | |
| Overweight | 0.27 | 0.74 | 0.68 | ||
| Obese | 0.34 | 0.74 | 0.85 | ||
| Underweight | 0.05 | 0.67 | 0.79 | ||
| Male | <50 years old | Normal | 0.38 | 0.68 | 0.63 |
| Overweight | 0.39 | 0.59 | 0.68 | ||
| Obese | 0.29 | 0.67 | 0.83 | ||
| Underweight | 0.11 | 0.72 | 0.75 | ||
| ≥50 years old | Normal | 0.56 | 0.47 | 0.67 | |
| Overweight | 0.47 | 0.52 | 0.70 | ||
| Obese | 0.43 | 0.57 | 0.87 | ||
| Underweight | 0.28 | 0.65 | 0.80 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, C.; Lin, T.-H.; Lin, C.-J.; Kuo, C.-F.; Pai, B.C.-J.; Cheng, H.-T.; Lai, C.-C.; Chen, T.-H. A Noninvasive Risk Stratification Tool Build Using an Artificial Intelligence Approach for Colorectal Polyps Based on Annual Checkup Data. Healthcare 2022, 10, 169. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10010169
Lee C, Lin T-H, Lin C-J, Kuo C-F, Pai BC-J, Cheng H-T, Lai C-C, Chen T-H. A Noninvasive Risk Stratification Tool Build Using an Artificial Intelligence Approach for Colorectal Polyps Based on Annual Checkup Data. Healthcare. 2022; 10(1):169. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10010169
Chicago/Turabian StyleLee, Chieh, Tsung-Hsing Lin, Chen-Ju Lin, Chang-Fu Kuo, Betty Chien-Jung Pai, Hao-Tsai Cheng, Cheng-Chou Lai, and Tsung-Hsing Chen. 2022. "A Noninvasive Risk Stratification Tool Build Using an Artificial Intelligence Approach for Colorectal Polyps Based on Annual Checkup Data" Healthcare 10, no. 1: 169. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10010169