
Identification of Determinants of Biofeedback Treatment’s Efficacy in Treating Migraine and Oxidative Stress by ARIANNA (ARtificial Intelligent Assistant for Neural Network Analysis)

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants, Biomarkers, and Migraine Assessment
2.2. Biofeedback Treatment
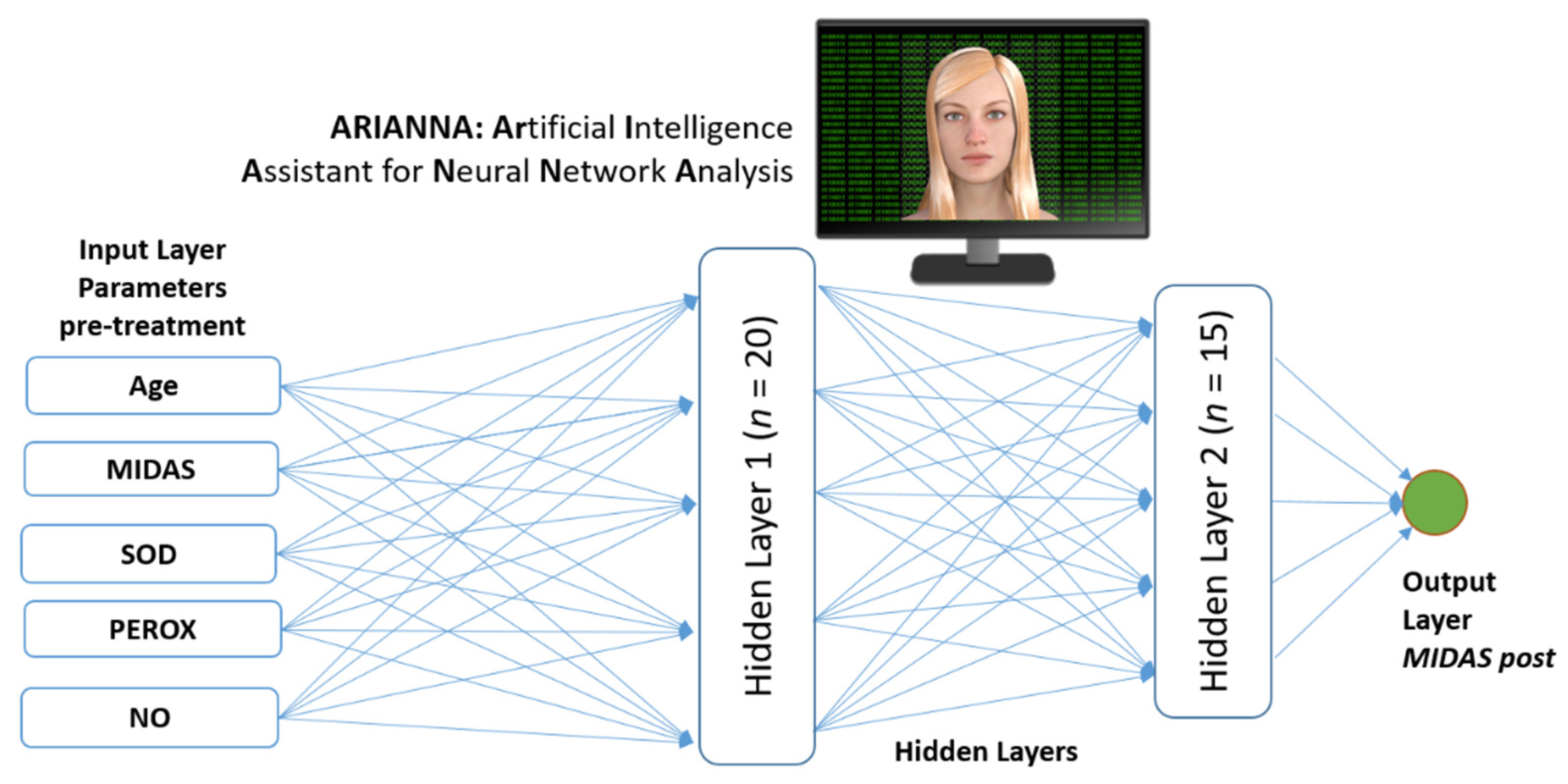
2.3. Artificial Neural Network
2.4. Statistical Analysis
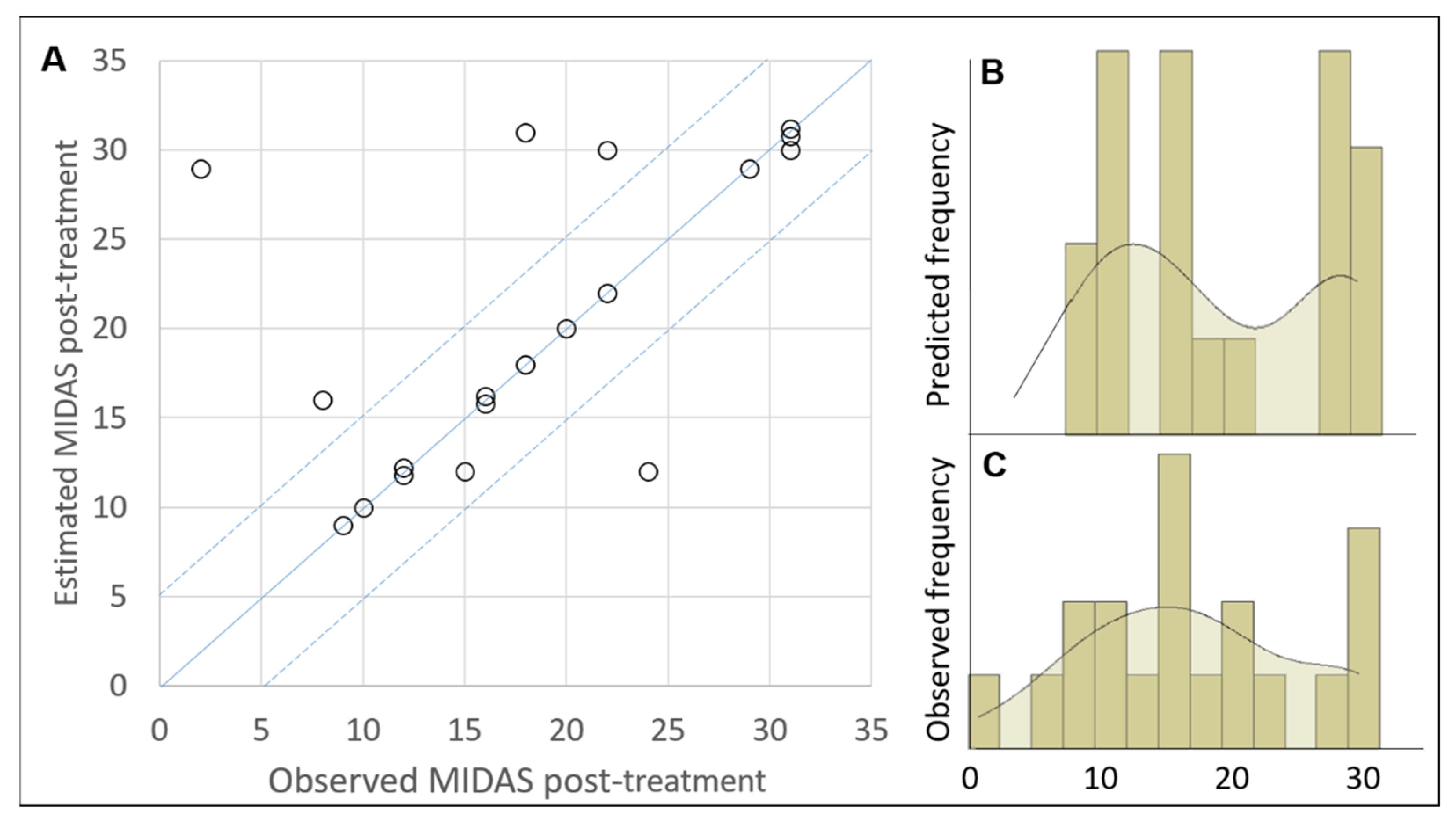
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Agosti, R. Migraine Burden of Disease: From the Patient’s Experience to a Socio-Economic View. Headache 2018, 58, 17–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buse, D.C.; Greisman, J.D.; Baigi, K.; Lipton, R.B. Migraine progression: A systematic review. Headache 2019, 59, 306–338. [Google Scholar] [CrossRef] [PubMed]
- Stovner, L.J.; Nichols, E.; Steiner, T.J.; Abd-Allah, F.; Abdelalim, A.; Al-Raddadi, R.M.; Ansha, M.G.; Barac, A.; Bensenor, I.M.; Doan, L.P.; et al. Global, regional, and national burden of migraine and tension-type headache, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018, 17, 954–976. [Google Scholar] [CrossRef] [Green Version]
- Andrasik, F. Behavioral treatment of migraine: Current status and future directions. Expert Rev. Neurother. 2004, 4, 403–413. [Google Scholar] [CrossRef]
- Ciancarelli, I.; Tozzi-Ciancarelli, M.G.; Spacca, G.; Di Massimo, C.; Carolei, A. Relationship between biofeedback and oxidative stress in patients with chronic migraine. Cephalalgia 2007, 27, 1136–1141. [Google Scholar] [CrossRef]
- Andrasik, F.; Grazzi, L.; Sansone, E.; D’Amico, D.; Raggi, A.; Grignani, E. Non-pharmacological Approaches for Headaches in Young Age: An Updated Review. Front Neurol. 2018, 9, 1009. [Google Scholar] [CrossRef] [Green Version]
- National Clinical Guideline C National institute of Health and Clinical Excellence: Guidance. Headaches: Diagnosis and Management of Headaches in Young People and Adults. Available online: http://www.nice.org.uk/CG150 (accessed on 4 April 2022).
- Kroop, P.; Meyer, B.; Meyer, W.; Dresler, T. An update on behavioural treatments in migraine—Current knowledge and future options. Expert Rev. Neurother. 2017, 17, 1059–1068. [Google Scholar] [CrossRef]
- Ailani, J.; Burch, R.C.; Robbins, M.S.; On behalf of the Board of Directors of the American Headache Society. The American Headache Society Consensus statement: Update on integrating new migraine treatments into clinical practice. Headache 2021, 61, 1021–1039. [Google Scholar] [CrossRef]
- Halliwell, B. Reactive oxygen species and the central nervous system. J. Neurochem. 1992, 59, 1609–1623. [Google Scholar] [CrossRef]
- Guzik, T.J.; Korbut, R.; Adamek-Guzik, T. Nitric oxide and superoxide in inflammation and immune regulation. J. Ohysiology Pharmacol. 2003, 54, 469–487. [Google Scholar]
- Olesen, J.; Jansen-Olesen, I. Nitric oxide mechanisms in migraine. Pathol. Biol. 2000, 48, 648–657. [Google Scholar] [PubMed]
- Noor, R.; Mittal, S.; Iqbal, J. Superoxide dismutase applications and relevance to human diseases. Med. Sci. Monit. 2002, 8, RA210-5. [Google Scholar] [PubMed]
- Mauskop, A. Nonmedication, alternative, and complementary treatments for migraine. Headache 2021, 18, 796–806. [Google Scholar] [CrossRef] [PubMed]
- Nestoriuc, Y.; Martin, A. Efficacy of biofeedback for migraine: A meta-analysis. Pain 2007, 128, 111–127. [Google Scholar] [CrossRef]
- Baxt, W.G. Application of artificial neural networks to clinical medicine. Lancet 2018, 1995, 1135–1138. [Google Scholar] [CrossRef]
- Iosa, M.; Capodaglio, E.; Pelà, S.; Persechino, B.; Morone, G.; Antonucci, G.; Paolucci, S.; Panigazzi, M. Artificial Neural Network Analyzing Wearable Device Gait Data for Identifying Patients with Stroke Unable to Return to Work. Front. Neurol. 2021, 12, 650542. [Google Scholar] [CrossRef]
- Iosa, M.; Benedetti, M.G.; Antonucci, G.; Paolucci, S.; Morone, G. Artificial Neural Network Detects Hip Muscle Forces as Determinant for Harmonic Walking in People after Stroke. Sensors 2022, 22, 1374. [Google Scholar] [CrossRef]
- Iosa, M.; Morone, G.; Antonucci, G.; Paolucci, S. Prognostic Factors in Neurorehabilitation of Stroke: A Comparison among Regression, Neural Network, and Cluster Analyses. Brain Sci. 2021, 11, 1147. [Google Scholar] [CrossRef]
- The Headache Classification Subcommittee of the International Headache Society. The International Classification of Headache Disorders, 2nd ed. Cephalalgia 2004, 24 (Suppl. 1), 1–160. [Google Scholar]
- Stewart, W.F.; Lipton, R.B.; Kolodner, K. Migraine disability assessment (MIDAS) score: Relation to headache frequency, pain intensity, and headache symptoms. Headache 2003, 43, 258–265. [Google Scholar] [CrossRef]
- Togha, M.; Razeghi Jahromi, S.; Ghorbani, Z.; Ghaemi, A.; Rafiee, P. An investigation of oxidant/antioxidant balance in patients with migraine: A case-control study. BMC Neurol. 2019, 19, 323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuncel, D.; Tolun, F.I.; Gokce, M.; Imrek, S.; Ekerbicer, H. Oxidative Stress in Migraine with and Without Aura. Biol. Trace Elem. Res. 2008, 126, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, A.; Hyde, E.; Sangwan, N.; Gilbert, J.A.; Viirre, E.; Knight, R. Migraines Are Correlated with Higher Levels of Nitrate-, Nitrite-, and Nitric Oxide-Reducing Oral Microbes in the American Gut Project Cohort. mSystems 2017, 2, e00023-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vekhter, D.; Robbins, M.S.; Minen, M.; Buse, D.C. Efficacy and feasibility of behavioral treatments for migraine, headache, and pain in the acute care setting. Curr. Pain Headache Rep. 2020, 24, 66. [Google Scholar] [CrossRef]
- Esch, T.; Fricchione, G.L.; Stefano, G.B. The therapeutic use of the relaxation response in stress-related diseases. Med. Sci. Monit. 2003, 9, RA23-34. [Google Scholar]



{kind=link}
{kind=link}
| Assessment of Variables | Pre-Treatment | Post-Treatment | Paired Comparison T-Test, p-Value | Normality Shapiro–Wilk Test, p-Value |
|---|---|---|---|---|
| SOD (μM) | 6.5 ± 1.0 | 8.0 ± 0.7 | <0.001 | 0.372 |
| NOx (μM) | 23.7 ± 4.2 | 31.4 ± 3.0 | <0.001 | 0.612 |
| Peroxides (U/mL) | 145.8 ± 40.3 | 82.5 ± 21.3 | <0.001 | 0.199 |
| MIDAS | 37.0 ± 13.2 | 18.8 ± 8.6 | <0.001 | 0.102 |
| Pre-Treatment Variable | Importance in the ANN | Normalized Importance |
|---|---|---|
| Age (years) | 0.184 | 83.4% |
| SOD (μM) | 0.189 | 85.6% |
| NOx (μM) | 0.221 | 100% |
| Peroxides (U/mL) | 0.216 | 97.9% |
| MIDAS | 0.191 | 86.5% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ciancarelli, I.; Morone, G.; Tozzi Ciancarelli, M.G.; Paolucci, S.; Tonin, P.; Cerasa, A.; Iosa, M. Identification of Determinants of Biofeedback Treatment’s Efficacy in Treating Migraine and Oxidative Stress by ARIANNA (ARtificial Intelligent Assistant for Neural Network Analysis). Healthcare 2022, 10, 941. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10050941
Ciancarelli I, Morone G, Tozzi Ciancarelli MG, Paolucci S, Tonin P, Cerasa A, Iosa M. Identification of Determinants of Biofeedback Treatment’s Efficacy in Treating Migraine and Oxidative Stress by ARIANNA (ARtificial Intelligent Assistant for Neural Network Analysis). Healthcare. 2022; 10(5):941. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10050941
Chicago/Turabian StyleCiancarelli, Irene, Giovanni Morone, Maria Giuliana Tozzi Ciancarelli, Stefano Paolucci, Paolo Tonin, Antonio Cerasa, and Marco Iosa. 2022. "Identification of Determinants of Biofeedback Treatment’s Efficacy in Treating Migraine and Oxidative Stress by ARIANNA (ARtificial Intelligent Assistant for Neural Network Analysis)" Healthcare 10, no. 5: 941. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10050941