
Impact of an Educational Program on Improving Nurses’ Management of Fever: An Experimental Study


Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Ethical Consideration
2.3. Study Setting
2.4. Study Participants
2.5. Sample Size
2.6. Intervention
2.7. Instruments
2.7.1. KAFMQ
2.7.2. MRFMC
2.8. Data Collection
2.9. Data Analysis
3. Results
3.1. Basic Participant Characteristics
3.2. Changes in Knowledge Post-Education
3.3. Changes in Attitudes Post-Education
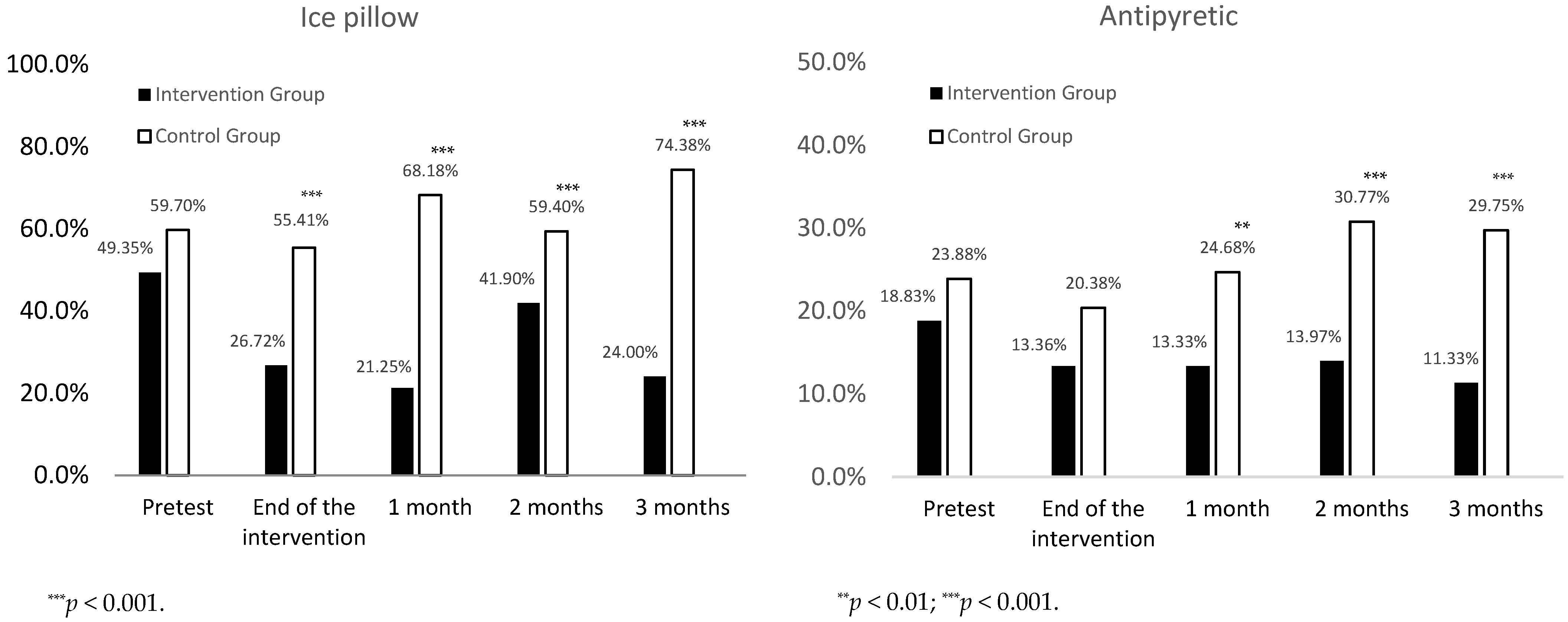
3.4. Changes in Behaviors Post-Education
4. Discussion
4.1. The Effects of Education on Nurses’ Knowledge in Fever Management
4.2. Effects of Education on Nurses’ Attitudes in Fever Management
4.3. Effects of Education on Nurses’ Behaviors in Fever Management
4.4. Study Strengths and Limitations
5. Conclusions and Recommendations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bor, D.H.; Makadon, H.J.; Friedland, G.; Dasse, P.; Komaroff, A.L.; Aronson, M.D. Fever in hospitalized medical patients: Characteristics and significance. J. Gen. Intern. Med. 1988, 3, 119–125. [Google Scholar] [CrossRef] [PubMed]
- McGowan, J.E.; Rose, R.C.; Jacobs, N.F.; Schaberg, D.R.; Haley, R.W. Fever in hospitalized patients: With special reference to the medical service. Am. J. Med. 1987, 82, 580–586. [Google Scholar] [CrossRef]
- Cannon, J.G. Perspective on fever: The basic science and conventional medicine. Complement. Ther. Med. 2013, 21 (Suppl. S1), S54–S60. [Google Scholar] [CrossRef] [PubMed]
- Drewry, A.M.; Ablordeppey, E.; Murray, E.T.; Stoll, C.R.T.; Izadi, S.R.; Dalton, C.M.; Hardi, A.; Fowler, S.A.; Fuller, B.M.; Colditz, G. Antipyretic Therapy in Critically Ill Septic Patients: A Systematic Review and Meta-Analysis. Crit. Care Med. 2017, 45, 806–813. [Google Scholar] [CrossRef]
- Kiekkas, P.; Aretha, D.; Bakalis, N.; Karpouhtsi, I.; Marneras, C.; Baltopoulos, G.I. Fever effects and treatment in critical care: Literature review. Aust. Crit. Care 2013, 26, 130–135. [Google Scholar] [CrossRef]
- Roth, J. Endogenous antipyretics. Clin. Chim. Acta 2006, 371, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Rice, P.; Martin, E.; He, J.R.; Frank, M.; DeTolla, L.; Hester, L.; O’Neill, T.; Manka, C.; Benjamin, I.; Nagarsekar, A.; et al. Febrile-range hyperthermia augments neutrophil accumulation and enhances lung injury in experimental gram-negative bacterial pneumonia. J. Immunol. 2005, 174, 3676–3685. [Google Scholar] [CrossRef] [Green Version]
- Beard, R.M.; Day, M.W. Fever and Hyperthermia: Learn to beat the heat. Nursing 2008, 38, 28–31. [Google Scholar] [CrossRef]
- Mizushima, Y.; Ueno, M.; Idoguchi, K.; Ishikawa, K.; Matsuoka, T. Fever in Trauma Patients: Friend or Foe? J. Trauma Acute Care Surg. 2009, 67, 1062–1065. [Google Scholar] [CrossRef]
- Scrase, W.; Tranter, S. Improving evidence-based care for patients with pyrexia. Nurs. Stand. 2011, 25, 37–41. [Google Scholar] [CrossRef]
- Laupland, K.B.; Shahpori, R.; Kirkpatrick, A.W.; Ross, T.; Gregson, D.B.; Stelfox, H.T. Occurrence and outcome of fever in critically ill adults. Crit. Care Med. 2008, 36, 1531–1535. [Google Scholar] [CrossRef] [PubMed]
- Broom, M. Physiology of fever. Nurs. Child. Young People 2007, 19, 40–44. [Google Scholar]
- Laupland, K.B. Fever in the critically ill medical patient. Crit. Care Med. 2009, 37 (Suppl. S7), S273–S278. [Google Scholar] [CrossRef] [PubMed]
- Dalal, S.; Zhukovsky, D.S. Pathophysiology and management of fever. J. Support. Oncol. 2006, 4, 9–16. [Google Scholar]
- Young, P.J.; Bellomo, R.; Bernard, G.R.; Niven, D.J.; Schortgen, F.; Saxena, M.; Beasley, R.; Weatherall, M. Fever control in critically ill adults. An individual patient data meta-analysis of randomised controlled trials. Intensiv. Care Med. 2019, 45, 468–476. [Google Scholar] [CrossRef]
- Carey, J.V. Literature review: Should antipyretic therapies routinely be administered to patient fever? J. Clin. Nurs. 2010, 19, 2377–2393. [Google Scholar] [CrossRef]
- Swenson, B.R.; Hedrick, T.L.; Popovsky, K.; Pruett, T.L.; Sawyer, R.G. Is Fever Protective in Surgical Patients with Bloodstream Infection? J. Am. Coll. Surg. 2007, 204, 815–821. [Google Scholar] [CrossRef]
- Thompson, H.J. Fever: A concept analysis. J. Adv. Nurs. 2005, 51, 484–492. [Google Scholar] [CrossRef]
- Ludwig, J.; McWhinnie, H. Antipyretic drugs in patients with fever and infection: Literature review. Br. J. Nurs. 2019, 28, 610–618. [Google Scholar] [CrossRef]
- Launey, Y.; Nesseler, N.; Mallédant, Y.; Seguin, P. Clinical review: Fever in septic ICU patients-friend or foe? Crit. Care 2011, 15, 222–227. [Google Scholar] [CrossRef] [Green Version]
- Lenhardt, R.; Negishi, C.; Sessler, D.I.; Vuong, K.; Bastanmehr, H.; Kim, J.-S.; Bjorksten, A.R. The effects of physical treatment on induced fever in humans. Am. J. Med. 1999, 106, 550–555. [Google Scholar] [CrossRef]
- High, K.P.; Bradley, S.F.; Gravenstein, S.; Mehr, D.R.; Quagliarello, V.J.; Richards, C.; Yoshikawa, T.T. Clinical Practice Guideline for the Evaluation of Fever and Infection in Older Adult Residents of Long-Term Care Facilities: 2008 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2009, 48, 149–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulman, C.I.; Namias, N.; Doherty, J.; Manning, R.J.; Li, P.; Elhaddad, A.; Lasko, D.; Amortegui, J.; Dy, C.J.; Dlugasch, L.; et al. The Effect of Antipyretic Therapy upon Outcomes in Critically Ill Patients: A Randomized, Prospective Study. Surg. Infect. 2005, 6, 369–375. [Google Scholar] [CrossRef]
- Egi, M.; Morita, K. Fever in non-neurological critically ill patients: A systematic review of observational studies. J. Crit. Care 2012, 27, 428–433. [Google Scholar] [CrossRef] [PubMed]
- Thompson, H.J.; Kagan, S.H. Clinical management of fever by nurses: Doing what works. J. Adv. Nurs. 2010, 67, 359–370. [Google Scholar] [CrossRef] [Green Version]
- Khalifa, M.I. Impact of an educational program based on evidence related to Fever management. J. Egypt. Public Health Assoc. 2007, 82, 419–435. [Google Scholar]
- Young, P.J.; Saxena, M.; Beasley, R.; Bellomo, R.; Bailey, M.; Pilcher, D.; Finfer, S.; Harrison, D.; Myburgh, J.; Rowan, K. Early peak temperature and mortality in critically ill patients with or without infection. Intensiv. Care Med. 2012, 38, 437–444. [Google Scholar] [CrossRef] [Green Version]
- Lee, B.H.; Inui, D.; Suh, G.Y.; Kim, J.Y.; Kwon, J.Y.; Park, J.; Tada, K.; Tanaka, K.; Ietsugu, K.; Uehara, K.; et al. Association of body temperature and antipyretic treatments with mortality of critically ill patients with and without sepsis: Multi-centered prospective observational study. Crit. Care 2012, 16, R33. [Google Scholar] [CrossRef]
- Kiekkas, P.; Konstantinou, E.; Psychogiou, K.-S.; Tsampoula, I.; Stefanopoulos, N.; Bakalis, N. Nursing personnel’s attitudes towards fever and antipyresis of adult patients: Cross-sectional survey. J. Clin. Nurs. 2014, 23, 2949–2957. [Google Scholar] [CrossRef]
- Considine, J.; Brennan, D. Emergency nurses’ opinions regarding paediatric fever: The effect of an evidence-based education program. Australas. Emerg. Nurs. J. 2006, 9, 101–111. [Google Scholar] [CrossRef]
- Walsh, A.M.; Edwards, H.E.; Courtney, M.D.; Wilson, J.E.; Monaghan, S.J. Fever management: Paediatric nurses’ knowledge, attitudes and influencing factors. J. Adv. Nurs. 2005, 49, 453–464. [Google Scholar] [CrossRef] [PubMed]
- Sarrell, M.; Cohen, H.A.; Kahan, E. Physicians’, nurses’, and parents’ attitudes to and knowledge about fever in early childhood. Patient education and counseling. Patient Educ. Couns. 2002, 46, 61–65. [Google Scholar] [CrossRef]
- Considine, J.; Brennan, D. Effect of an evidence-based education programme on ED discharge advice for febrile children. J. Clin. Nurs. 2007, 16, 1687–1694. [Google Scholar] [CrossRef] [PubMed]
- Considine, J.; Brennan, D. Effect of an evidence-based paediatric fever education program on emergency nurses’ knowledge. Accid. Emerg. Nurs. 2007, 15, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Edwards, H.; Walsh, A.; Courtney, M.; Monaghan, S.; Wilson, J.; Young, J. Improving paediatric nurses’ knowledge and attitudes in childhood fever management. J. Adv. Nurs. 2007, 57, 257–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edwards, H.; Walsh, A.; Courtney, M.; Monaghan, S.; Wilson, J.; Young, J. Promoting evidence-based childhood fever management through a peer education programme based on the theory of planned behaviour. J. Clin. Nurs. 2007, 16, 1966–1979. [Google Scholar] [CrossRef] [Green Version]
- Altun, I.; Zencirci, A.D. Management of fever and hyperthermia: Impact of lecture-based interactive workshops on training of nurses. Libyan J. Med. 2010, 5, 5140. [Google Scholar] [CrossRef] [Green Version]
- Sutherland, S. Quantitative Methodology: Interventional Designs and Methods. In Burns and Grove’s the Practice of Nursing Research, 8th ed.; Gray, J.R., Grove, S.K., Sutherland, S., Eds.; Elsevier: St. Louis, MO, USA, 2017; pp. 217–238. [Google Scholar]
- Weng, Y.; Chen, C.; Kuo, K.N.; Yang, C.; Lo, H.; Chen, K.-H.; Chiu, Y. Implementation of Evidence-Based Practice in Relation to a Clinical Nursing Ladder System: A National Survey in Taiwan. Worldviews Evid.-Based Nurs. 2015, 12, 22–30. [Google Scholar] [CrossRef] [Green Version]
- Dai, Y.-T.; Lu, S.-H. What’s missing for evidence-based fever management? Is fever beneficial or harmful to humans? Int. J. Nurs. Stud. 2012, 49, 505–507. [Google Scholar] [CrossRef]
- Sund-Levander, M.; Grodzinsky, E. Time for a change to assess and evaluate body temperature in clinical practice. Int. J. Nurs. Pract. 2009, 15, 241–249. [Google Scholar] [CrossRef]
- O’Grady, N.P.; Barie, P.S.; Bartlett, J.G.; Bleck, T.; Carroll, K.; Kalil, A.C.; Linden, P.; Maki, D.G.; Nierman, D.; Pasculle, W.; et al. Guidelines for evaluation of new fever in critically ill adult patients: 2008 update from the American College of Critical Care Medicine and the Infectious Diseases Society of America. Crit. Care Med. 2008, 36, 1330–1349. [Google Scholar] [CrossRef] [PubMed]
- Kiekkas, P.; Velissaris, D.; Karanikolas, M.; Aretha, D.; Samios, A.; Skartsani, C.; Baltopoulos, G.I.; Filos, K.S. Peak body temperature predicts mortality in critically ill patients without cerebral damage. Heart Lung 2010, 39, 208–216. [Google Scholar] [CrossRef]
- El-Radhi, A.S.M. Why is the evidence not affecting the practice of fever management? Arch. Dis. Child. 2008, 93, 918–920. [Google Scholar] [CrossRef] [PubMed]
- Gozzoli, V.; Schöttker, P.; Suter, P.M.; Ricou, B. Is It Worth Treating Fever in Intensive Care Unit Patients? Preliminary results from a randomized trial of the effect of external cooling. Arch. Intern. Med. 2001, 161, 121–123. [Google Scholar] [CrossRef]
- Polit, D.F.; Beck, C.T. Developing and Testing Self-Report Scales. In Nursing Research: Generating and Asessing Evidence for Nursing Practice, 10th ed.; Polit, D.F., Beck, C.T., Eds.; Wolters Kluwer: Philadelphia, PA, USA, 2017; pp. 331–355. [Google Scholar]
- Chiu, L.Y.; Dai, Y.T.; Sheng, W.H.; Ko, W.J. Association between Professional Readiness and Fever and Antipyretic Management in Physicians and Nurses. J. Nurs. Healthc. Res. 2013, 9, 74–82. [Google Scholar] [CrossRef]
- Caruso, C.C.; Hadley, B.J.; Shukla, R.; Frame, P.; Khoury, J. Cooling effects and comfort of four cooling blanket temperatures in humans with fever. Nurs. Res. 1992, 41, 68–72. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Intervention Group (n = 29) | Control Group (n = 29) | p | ||
|---|---|---|---|---|---|
| n (%) | M ± SD | n (%) | M ± SD | ||
| Gender | |||||
| Female | 28 (96.55) | 28 (96.55) | >0.999 a | ||
| Male | 1 (03.44) | 1 (03.44) | |||
| Age (years) | 27.58 ± 6.77 | 30.39 ± 8.05 | 0.143 b | ||
| 20–24 | 10 (34.48) | 8 (27.58) | 0.404 a | ||
| 25–29 | 14 (48.27) | 11 (37.93) | |||
| 30–34 | 2 (06.89) | 2 (06.89) | |||
| ≥35 | 3 (10.34) | 8 (27.58) | |||
| Education | |||||
| Associate | 5 (17.24) | 4 (13.79) | 0.731 a | ||
| College | 23 (79.31) | 25 (86.20) | |||
| Graduate (or above) | 1 (03.44) | 0 (00.00) | |||
| Nursing Ladder | |||||
| N | 7 (24.13) | 7 (24.13) | 0.241 a | ||
| N1 | 8 (27.58) | 3 (10.34) | |||
| N2 | 12 (41.37) | 14 (48.27) | |||
| N3 | 2 (06.89) | 3 (10.34) | |||
| N4 | 0 (00.00) | 2 (06.89) | |||
| Clinical Experience (months) | 67.48 ± 89.15 | 96.48 ± 98.74 | 0.230 b | ||
| 0–12 | 3 (10.34) | 4 (13.79) | 0.344 a | ||
| 13–60 | 17 (58.62) | 13 (44.82) | |||
| 61–120 | 6 (20.68) | 6 (20.68) | |||
| 121–360 | 3 (10.34) | 6 (20.68) | |||
| Variable | Intervention Group (n = 29) | Control Group (n = 29) | t | p | ||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| Knowledge | ||||||
| Pretest | 27.26 | 3.89 | 26.35 | 5.78 | 0.722 | 0.473 |
| End of the intervention | 36.93 | 3.09 | 25.32 | 5.61 | 10.015 | <0.001 *** |
| 1 month | 34.55 | 3.47 | 29.19 | 4.92 | 4.847 | <0.001 *** |
| 2 months | 34.03 | 2.99 | 28.03 | 4.00 | 6.502 | <0.001 *** |
| 3 months | 32.62 | 4.00 | 29.00 | 3.63 | 3.610 | 0.001 ** |
| Attitude | ||||||
| Pretest | 21.77 | 3.28 | 20.77 | 4.91 | 0.943 | 0.350 |
| End of the intervention | 25.48 | 3.44 | 20.13 | 3.60 | 5.879 | <0.001 *** |
| 1 month | 24.21 | 3.90 | 21.35 | 3.03 | 3.174 | 0.002 ** |
| 2 months | 22.48 | 5.40 | 20.90 | 3.03 | 1.381 | 0.174 |
| 3 months | 22.66 | 4.46 | 21.52 | 2.63 | 1.184 | 0.243 |
| Variable | Knowledge Score | Attitude Score |
|---|---|---|
| (β and 95% CI) | (β and 95% CI) | |
| Intercept | 26.35 (24.85, 27.86) *** | 20.77 (19.42, 21.13) *** |
| Group a (Experimental vs. Control) | 0.90 (−1.22, 3.03) | 1.00 (−0.92, 2.92) |
| Time a | ||
| End of the intervention vs. Pretest | −1.03 (−2.84, 0.77) | −0.65 (−2.10, 0.81) |
| 1 month vs. Pretest | 2.84 (1.03, 4.64) ** | 0.58 (−0.88, 2.04) |
| 2 months vs. Pretest | 1.71 (−0.11, 3.54) | 0.15 (−1.32, 1.63) |
| 3 months vs. Pretest | 2.59 (0.75, 4.43) ** | 0.67 (−0.81, 2.16) |
| Group × Time a | ||
| End of the intervention | 10.68 (8.10, 13.26) *** | 4.33 (2.24, 6.42) *** |
| 1 month | 4.43 (1.85, 7.01) ** | 1.83 (−0.26, 3.92) |
| 2 months | 5.04 (2.44, 7.63) *** | 0.53 (−1.57, 2.63) |
| 3 months | 2.75 (0.14, 5.36) * | 0.18 (−1.92, 2.29) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsiao, B.-H.; Tzeng, Y.-L.; Lee, K.-C.; Lu, S.-H.; Lin, Y.-P. Impact of an Educational Program on Improving Nurses’ Management of Fever: An Experimental Study. Healthcare 2022, 10, 1135. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10061135
Hsiao B-H, Tzeng Y-L, Lee K-C, Lu S-H, Lin Y-P. Impact of an Educational Program on Improving Nurses’ Management of Fever: An Experimental Study. Healthcare. 2022; 10(6):1135. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10061135
Chicago/Turabian StyleHsiao, Bi-Hung, Ya-Ling Tzeng, Kwo-Chen Lee, Shu-Hua Lu, and Yun-Ping Lin. 2022. "Impact of an Educational Program on Improving Nurses’ Management of Fever: An Experimental Study" Healthcare 10, no. 6: 1135. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10061135